
Abstract
Diabetes (DM) increases fracture risk, and bone quality depends on type diabetes type, duration, and other comorbidities. Diabetes is associated with a 32% increased relative risk (RR) of total fractures and 24% increased RR of ankle fractures compared with patients without DM. Type 2 DM is associated with a 37% increased RR of foot fractures compared with patients without DM. The incidence of ankle fractures in the general population is 169/100,000 per year, while foot fractures occur less frequently, with an incidence of 142/100,000 per year. Biomechanical properties of bone are negatively impacted by stiff collagen, contributing to the increased risk of fragility fractures in patients with DM. Systemic elevation of proinflammatory cytokines, such as tumor necrosis factor-alpha (TNFα), interleukin-1β (IL-1β), and interleukin 6 (IL-6), impact bone healing in patients with DM. Fractures in patients with DM, can be associated with poorly regulated levels of RANKL (receptor activator of nuclear transcription factor kappa-b ligand) leading to prolonged osteoclastogenesis, and net bone resorption. One of the most salient factors in treating fractures and dislocations of the foot and ankle is to recognize the difference between patients with uncomplicated and complicated DM. Complicated diabetes is defined as ‘end organ damage’, and for the purposes of this review, includes patients with neuropathy, peripheral artery disease (PAD) and/or chronic renal disease. Uncomplicated diabetes is not associated with ‘end organ damage’. Foot and ankle fractures in patients with complicated DM pose challenges, and surgery is associated with increased risks of impaired wound healing, delayed fracture healing, malunion, infection, surgical site infection, and revision surgery. While patients with uncomplicated DM can be treated like patients without DM, patients with complicated DM require close follow-up and robust fixation methods should be considered to withstand the anticipated prolonged healing period. The aims of this review are as follows: (1) to review pertinent aspects of DM bone physiology and fracture healing, (2) to review the recent literature on treatment of foot and ankle fractures in patients with complicated DM, and (3) to provide treatment protocols based on the recent published evidence.
Introduction
An estimated 537 million adults were living with diabetes mellitus (DM) in 2021, with an estimated prevalence of 1 in 10 people. 1 Diabetes is associated with increased fracture risk and impaired bone health, and fragility fractures can affect various age groups with different disease burden depending on type of diabetes, disease duration, and the presence of other comorbidities. 2 Patients with DM have a 32% increased relative risk of total fractures (vertebral, upper extremity, and lower extremity) and 24% increased relative risk of ankle fractures compared with patients without DM. 3 In a recent descriptive study of 250,000 patients, the incidence rate of foot, ankle, and tibia/fibula fracture were higher in patients with newly treated DM compared with a matched control group. 4 Although both type 1 DM and type 2 DM are associated with increased risk of ankle fracture, patients with type 1 DM are at a greater risk of ankle fractures than patients with type 2 DM. A meta-analysis from 2021 confirmed the findings that type 1 DM was associated with a higher risk of fracture than type 2 DM, and both type 1 and type 2 DM increased the risk of ankle fractures. 5 Moayeri et al. 6 specifically looked at type 2 DM and found a 37% increased relative risk of foot fractures compared with patients without DM. The incidence of ankle fractures in the general population is among the highest of all anatomic locations at 169/100,000 per year, 7 while foot fractures occur less frequently, with an incidence of 142/100,000 per year. 8 The most common location of foot fractures is the forefoot (123.9/100,000/year), followed by the hind foot (13.7/100,000/ year), and midfoot (6.5/100,000/year) (Figure 1). Patients on oral anti-diabetic medications, such as thiazolidinediones, have also shown to have increased risk of fractures in another meta-analysis of 22 randomized controlled trials. 9

Incidence of location of fractures per 100,000 persons annually.
In addition to the increased risk of fracture, patients with DM have an increased risk of falls due to poor vision, peripheral neuropathy, and renal function.10–12 The Health, Aging, and Body Composition cohort study of 446 well-functioning older adults with DM (mean age 73.6 years) reported that 23% of patients acknowledged falling in the first year of the study and 22%, 26%, 30%, and 31% fell in the subsequent 4 years. 10 Impaired renal function has been shown to have a linear relationship to fall risk, as those with chronic kidney disease and increased cystatin-C have an increased risk for falls.10,13–15 Higher levels of cystatin-C and creatinine, both indicators of reduced renal function, have been studied in ratio to one another as a biomarker for muscle mass and indirectly, fall risk. 15 Chronic hyperglycemia impacts bone metabolism by decreasing bone mineral density (BMD), further jeopardizing a cohort of patients who are at increased risk of falls and fractures.6,16–19
Foot and ankle fractures in patients with DM, particularly in those who suffer from the complications of diabetes, can lead to devastating outcomes. 20 The risk of amputation after ankle fracture surgery is 7.4 times higher in patients with DM compared with patients without DM. 21 The aims of this review are as follows: (1) to review the pertinent aspects of DM bone physiology and fracture healing, (2) to review the recent literature on the treatment of foot and ankle fractures in patients with complicated DM, and (3) to provide diagnosis and treatment protocols in this population based on the recent published evidence.
Bone health in DM and fracture healing physiology
Approximately one-third of patients with DM experience macrovascular (32%) and microvascular disease (35%).22,23 Macrovascular disease results in coronary, cerebrovascular, and lower extremity peripheral artery disease, while microvascular disease is associated with nephropathy, retinopathy, and neuropathy.24,25 Complications after foot and ankle surgery are generally due to the associated comorbidities which result from macrovascular and microvascular disease.
Chronic hyperglycemia leads to alterations in normal physiology at the cellular level that results in higher levels of proinflammatory cytokines and adipokines, formation of advanced glycation end-products (AGEs), and disturbances to the Wnt (Wingless-related integration site) signaling pathway. These alterations impair function of osteoblasts, osteoclasts, and osteocytes. 26 When the receptor for AGEs is activated (RAGE), reactive oxygen species (ROS) production is increased, leading to cycles of chronic inflammation and bone resorption, a state that is unfavorable to bone health in DM patients. Unlike normal bone homeostasis, osteoclastic bone resorption is not balanced by osteoblastic bone formation, leading to net bone loss. 27 Non-enzymatic glycation end-products accumulate in bone, resulting in stiffness of type 1 collagen. Biomechanical properties of bone, such as yield and final fracture, are negatively impacted by stiff collagen. Increased inflammation and biomechanical changes in bone of patients with DM contributes to the increased risk of fragility fractures. 28
Soft tissue and osseous injury (fractures and dislocations) result in hyperemia and upregulation of proinflammatory cytokines. From a clinical perspective, systemic elevation of proinflammatory cytokines, such as tumor necrosis factor-alpha (TNFα), interleukin-1β (IL-1β), and interleukin 6 (IL-6), impact bone healing in patients with diabetes. These proinflammatory cytokines cause further upregulation of receptor activator of nuclear transcription factor kappa-b ligand (RANKL). In healthy patients, this proinflammatory state is necessary for normal bone healing by enhancing extracellular matrix (ECM) synthesis, angiogenesis and recruiting mesenchymal stem cells (MSCs) to form bone.29,30 Patients with DM and neuropathy may have a prolonged and unabated proinflammatory state due to continued trauma from weight-bearing on an injured limb. The normal orderly sequence of bone healing may be disrupted due to alteration in perfusion, chondrocyte imbalances, RAGEs, and increased osteoclast activity.31,32 After fractures in patients with DM, poorly regulated levels of RANKL may stimulate prolonged osteoclastogenesis, resulting in imbalance in bone homeostasis, net bone resorption, and impaired fracture healing. 33 RANKL is also implicated in the pathophysiology of Charcot neuroarthropathy. 34
Contributions from basic science to the understanding of fracture healing in diabetes
Several animal studies have investigated the effects of DM on bone healing. Gandhi et al. 35 studied an intramedullary insulin delivery system in a diabetic BB Wistar rat femur fracture model to assess the direct effects of insulin on bone healing. They studied three groups: nondiabetic rats, untreated diabetic rats, and diabetic rats treated with local intramedullary insulin. Local insulin at the site of the fracture resulted in increased cellular proliferation, chondrogenesis, mineralized tissue, cartilage content, and improved mechanical strength compared with the untreated diabetic rats. In another mouse fracture model, diabetes significantly increased TNFα levels and reduced mesenchymal stem cells numbers in new bone area. 36 It has been hypothesized that increased TNFα expression during fracture healing in diabetes may predispose patients to delayed bone fracture healing by reducing chondrogenesis in the collagenous callus phase, and by promoting osteoclastogenesis in the endochondral bone formation phase of fracture healing. 37 MicroRNAs have been also been identified as regulators of fracture healing, and altered microRNA profiles have been observed during fracture healing in diabetic rats. 38
Another recent study in a streptozotocin-induced diabetes mouse model found that DM impairs fracture healing through disruption of cilia formation in osteoblasts. 39 Cilia are hair-like cellular organelles that project from the cell membrane and serve to regulate the development of many organs including bone. Diabetes-inhibited ciliary gene expression and primary cilia formation in osteoblasts resulted in delayed fracture healing, significantly reduced bone density, and significantly reduced mechanical strength. Furthermore, the authors found decreased expression of osteoblast markers, decreased angiogenesis, and decreased proliferation of bone lining cells at the fracture sites.
Importance of distinguishing between complicated versus uncomplicated diabetes
One of the most important factors in treating fractures and dislocations of the foot and ankle is to recognize the difference between patients with uncomplicated and complicated diabetes.20,33,34 Complicated diabetes is defined as ‘end organ damage’, and for the purposes of this review, includes patients with neuropathy, peripheral artery disease (PAD), and/or chronic renal disease. The management of foot and ankle fractures in patients with complicated DM can be challenging, and surgical intervention is associated with an increased risk of impaired wound healing, delayed fracture healing, malunion, infection, and need for revision surgery.25,40–43 Surgical repair of diabetes-related ankle fracture in patients with complicated DM is associated with higher rates of in-hospital postoperative complications, longer hospital stay, higher total costs, higher rates of non-routine discharges, higher in-hospital mortality rates, and prolonged opioid use.44–46 Because peripheral neuropathy may be associated with absent or diminished pain, patients often ambulate on the surgically repaired foot or ankle unknowingly. Increased stress from premature weight-bearing can lead to early failure of the construct. Peripheral artery disease increases the risk of wound healing problems, and this can be problematic, especially in the peroneal artery angiosomal distribution. Routine palpation of pulses and measurement of ankle and toe pressures do not assess the peroneal artery. The peroneal artery supplies the tissue of the lateral ankle and hindfoot, a common anatomic area for incision placement (Figure 2). 47 Finally, renal disease may be associated with metabolic bone disease because of vitamin D deficiency and secondary hyperparathyroidism. Another important factor for reducing complications is glycemic control, as both long-term and perioperative control impacts outcomes after foot and ankle surgery. 35

Distribution of the foot and ankle angiosomes.
To further complicate the healing process, patients with sensory neuropathy have a significantly higher risk of developing postoperative infections and nonunions of their fracture site.48,49 In a prospective cohort study of 2060 patients, Wukich et al. 47 demonstrated that patients with neuropathy had a significantly higher rate of postoperative infection in foot and ankle surgery. This study included four groups of patients: a group without diabetes or neuropathy, a group with neuropathy and no diabetes, a group with uncomplicated diabetes, and a group with complicated diabetes. Patients with complicated diabetes had a 3.7-fold increased risk of infection compared with people with uncomplicated diabetes and 7.3 increased risk of infection compared with patients without diabetes and without sensory neuropathy. In a retrospective cohort study of 439 ankle fractures, Lavery et al. 48 reported the risk of infection and nonunion was 2.8 and 6.5 times higher in people with diabetes.
Evaluation and assessment
Initial evaluation of a foot and ankle fracture in a patient with DM begins with a comprehensive history to include the mechanism of injury, time elapsed since the injury, and any medical comorbidities. Pertinent medical history includes the presence or absence of nephropathy, neuropathy, and history of prior ulceration/amputation, (PAD), active tobacco use, obesity, as well as duration of DM and glycemic control. 50 Poorly controlled and longer duration of DM are more likely to be associated with complications of DM (neuropathy, nephropathy, and PAD). 51 The absence of pain and ability to ambulate on a fractured foot or ankle indicates the presence of peripheral neuropathy, which can lead to a delay in presentation and appropriate treatment. Due to lack of protective sensation, patients may continue to ambulate on the injured limb, creating further trauma. This prolongs the inflammatory response, which may lead to net bone loss due to upregulation of osteoclastogenesis. Patients often seek medical treatment once they notice a red, warm, and edematous foot that no longer fits into a shoe.
Physical examination should include a detailed dermatological, vascular, neurological, and musculoskeletal assessment. The skin is evaluated for any wounds, swelling, fracture blisters or impending skin compromise (tenting of the skin or fracture blisters). 50 The vascular exam includes palpation of the dorsalis pedis, posterior tibial and popliteal arteries, presence of edema, and the presence of hair growth. Pulses should be evaluated with a handheld Doppler ultrasound if pulses are not palpable. In patients with an abnormal vascular findings, further diagnostic testing should be performed, but should not delay the treatment of unstable fractures that require urgent reduction of fractures and dislocations. Further testing may include advanced diagnostic vascular studies and consultation with an experienced vascular consultant. Depending on geography, vascular consultants may include vascular surgeons, cardiologists, or interventional radiologists. Palpable pedal pulses do not exclude the presence of PAD in patients with DM and neuropathy, and these patients may not manifest the typical symptoms of PAD such as claudication. 52 In addition, ankle brachial index (ABI) may be falsely elevated due to stiffening of the arterial wall from medial artery calcinosis which is common in patients with DM. In the presence of non-compressible arteries (ABI > 1.3), transcutaneous oximetry (TcPO2) may also be performed to assess tissue perfusion. Measurement of the ABI, toe brachial index (TBI), absolute toe pressure, and the assessment of arterial wave forms may not be feasible or practical in patients with acute fractures. 53 It is not uncommon for patients with displaced foot and ankle fractures with dislocation to have absent or diminished pulses. Immediate closed reduction should be performed, and reassessment of the pulses undertaken. This usually results in improvement of perfusion.
Neurologic history and examination of the foot and ankle should be performed to assess for peripheral neuropathy. Simply asking patients if they have numbness, tingling, sensation of insects crawling on their skin, or burning is an effective way to identify sensory neuropathy. 54 Examination using a 5.07/10 g Semmes-Weinstein monofilament (SWMF) is performed to the plantar feet while the patient’s eyes are closed (Figure 3).55,56 The ability to sense vibratory sensation is examined by placement of a 128-Hz tuning fork directly on bone on the dorsal hallux interphalangeal joint. 57 Assessing the Achilles tendon reflex on the contralateral normal foot can be done as well. The inability to detect the SWMF, decreased vibration sense with the tuning fork, or absent ankle reflexes demonstrates the presence of peripheral neuropathy, and are critical to the provider’s assessment in addition to patient’s neuropathy symptoms. 55 If these instruments are not available to help detect the presence of neuropathy, the Ipswich Touch Test can be used to detect loss of sensation. 58

Illustration of 5.07/10 g Semmes-Weinstein monofilament examination (left) and suggested testing locations of the foot (right).
For diagnostic imaging, three view radiographs of both feet and ankles should be performed, and in most cases, are satisfactory for guiding treatment. Computed tomography (CT) scans can provide additional guidance when suspected injury is not obvious on radiographs. CT is also useful for surgical planning in more extensive fracture patterns/injuries, especially those with intra-articular and periarticular injury. Magnetic resonance imaging (MRI)is also beneficial in the setting of normal radiographs with clinical concern for injury, as well as imaging ligamentous injuries. MRI can identify bone marrow edema and stress injury that could be a precursor to Charcot neuroarthropathy. 59
Ankle fracture treatment and complications
Regardless of nonoperative or operative treatment for ankle fractures, the goal of treatment is to attain a stable foot and ankle, reestablish function, and minimize complications. As a general guideline, patients with uncomplicated diabetes who sustain an ankle fracture may be treated like patients without diabetes. In those patients with uncomplicated DM who require surgery, they can be treated with the same fixation techniques as patients without diabetes.25,49,60 Weight-bearing status during recovery is dependent on the type of fracture, however there is no substantial evidence to support or refute weight-bearing restrictions in neurologically intact patients. Nondisplaced, stable unimalalleolar fractures in patients with complicated DM can be managed nonsurgically using casting or controlled ankle motion boots with cautious observation. Stability of ankle injuries can be assessed by stress radiographs, weight-bearing radiographs and close follow-up to evaluate for displacements. 61 In patients with neuropathy (i.e. complicated DM) and stable, nondisplaced fractures, non-weight-bearing should be considered until fracture healing occurs, although the evidence supporting this is not of high quality. 62 Recommended duration of immobilization and non-weight-bearing in patients with complicated DM is to double the amount of time as compared with patients with uncomplicated DM. Patients should be monitored for reduction of inflammation (edema, warmth and erythema) of the injured limb. After fracture healing is achieved in patients with neuropathy, protected weight-bearing immobilization in a brace is often utilized for an additional 2–3 months. To the best of our knowledge, no study has directly evaluated the ideal time of casting or bracing necessary beyond initial fracture healing, but prolonged protection potentially can avoid the development of Charcot neuroarthropathy. Complicated DM adversely impacts outcomes of ankle fractures with overall rates of complications and aggregate noninfectious complications significantly higher than seen in uncomplicated DM.25,41,43,63 It is prudent to treat all neuropathic patients with ankle injuries, either soft tissue or bone, as if they are at risk for developing Charcot neuroarthropathy.
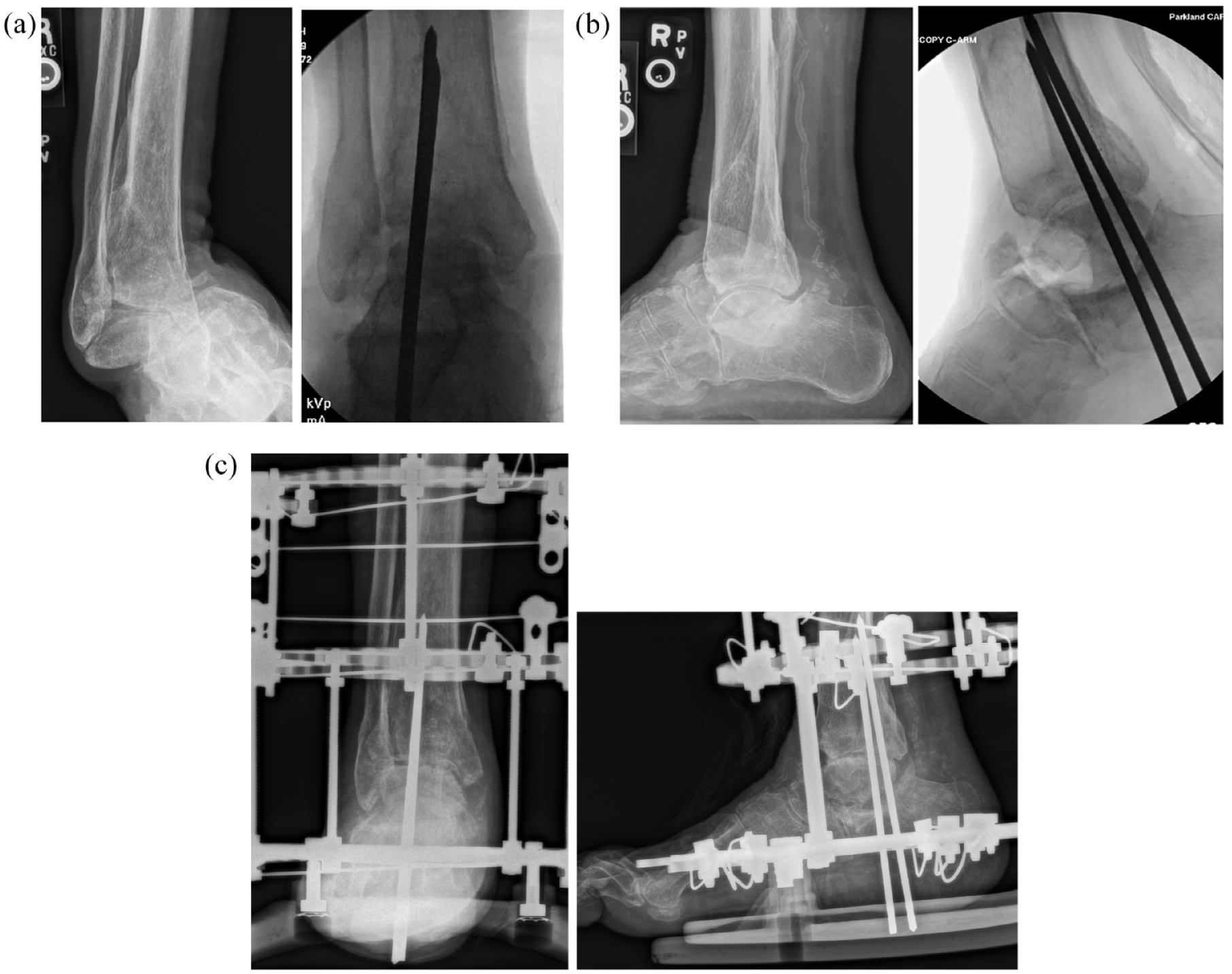
For closed, displaced ankle fractures, immediate closed reduction and splinting is performed. If osseous stability cannot be achieved and maintained with splinting, or the skin is at risk of compromise, a spanning external fixator can be applied as a first stage reduction, as seen in Figure 4. Definitive operative management is performed when the soft tissue envelope is clear of fractures blisters, and when the edema is sufficiently resolved that skin wrinkling in present. 64 Immediate open reduction and internal fixation (ORIF) is sometimes possible if performed before the onset of acute swelling; otherwise, optimization of skin may require a delay in surgery ranging from several days to several weeks. Displaced, unstable ankle fractures are best treated with ORIF. In cases of severe intra-articular injury or delayed presentation in patients with complicated DM, primary fusion may be a consideration (Figure 5). Patients with complicated DM require enhanced/supplemental fixation for unstable ankle fractures to maintain fracture reduction for anticipated prolonged healing period. This fixation may include multiple tetracortical trans-syndesmotic screw fixation (Figure 6), robust locking plates, trans-articular pinning (Figures 6 and 7), or a combination of internal and external fixation (Figure 7).

(a) spanning external fixator in place temporarily until the soft tissue is appropriate for surgery (b) lateral radiographs of ankle fracture dislocation (c) postoperative lateral radiograph demonstrating reduction of the fracture and external fixator in place.

Primary hindfoot and ankle fusion in a patient with complicated DM (neuropathy), severe intra-articular injury and delayed presentation.

multiple tetracortical syndesmotic screws, additional robust plates, and trans-articular pinning in a patient with complicated DM (neuropathy) who sustained ankle fracture dislocation.
(a) Preoperative and infra-operative radiograph (anterior–posterior view) of a patient with complicated DM, with subtalar dislocation. (b) Preoperative and intraoperative radiographs (lateral view) of the same patient (c) Postoperative radiographs combination of internal and external fixation.
Multiple studies have shown that diabetic patients with ankle fractures have an increased risk of complications in comparison to non-diabetic patients.25,41–43,65–67 Lovy et al. 68 reported that nonoperative treatment (closed reduction and casting) of displaced ankle fractures was associated with 21-fold increased odds of complications compared with operative treatment (ORIF). Flynn et al. 65 demonstrated that diabetic patients treated nonoperatively experienced higher rates of infection compared with those treated surgically. McCormack and Leith 40 also found nonoperative treatment of displaced ankle fractures were associated with a high rate of loss of reduction and malunion.
Blotter et al. 42 compared the outcomes of operative treatment for ankle fractures in patients with and without DM, and demonstrated that the relative risk for complications is 2.76 times greater in the patients with DM compared with those without DM. Haddix et al. 66 compared outcomes of ankle fractures with type 1 and type 2 DM; patients with type 1 DM had higher rates of amputation, postoperative infection, and total complications than patients with type 2 DM.
Neuropathy and poorly controlled diabetes are associated with significantly higher rates of surgical site infection after foot and ankle surgery. 49 Costigan et al. 43 evaluated 84 patients with DM who underwent ORIF and noted that 14% of patients developed complications; the study further revealed that patients with complicated DM experienced the highest risk of complications. Jones et al. 41 compared 21 patients with complicated DM with 21 patients with uncomplicated DM and found that patients with comorbidities had significantly higher rates of complications than patients without complications. (47% versus 14%, respectively). Higher body mass index (BMI) has been associated with delayed wound healing and increased complications in young adult patients surgically treated for bimalleolar fractures. 67 Moreover, higher complication rates are also observed in patients with a hemoglobin A1c (HbA1c) level greater than 6.5%; therefore, optimizing glucose levels prior to surgical intervention can help improve patient outcomes. 69 We recognize that long-term glycemic control, as measured by HbA1c, is not modifiable in acute fracture management; however, perioperative glycemic control is paramount to reduce complications. 70
Foot fractures and treatment
In contrast to ankle fractures, little has been published on foot fractures in patients with uncomplicated and complicated DM. As previously discussed, foot fractures of the hindfoot and midfoot fractures are relatively uncommon compared with ankle fractures. Through our literature search, we found five case reports of foot fractures in which the primary subjects were patients with DM: fifth metatarsal base (Jones), calcaneal body, calcaneal tuberosity avulsion, and two case reports of Lisfranc fracture-dislocation. The Jones and calcaneus fractures were treated with surgery in the acute setting without complications, whereas the Lisfranc cases were reported to develop Charcot neuroarthropathy after nonoperative immobilization and casting treatment.71–75
The overwhelming majority of case series reporting on outcomes in foot fractures do not include diabetes as a comorbidity. A study of the American College of Surgeons National Trauma Data Bank reported on calcaneus fractures from 700 trauma centers over a 2-year period. 76 A total of 14,516 calcaneus fractures were treated, and 96% of them were in patients aged 18 years or older. Diabetes was present in 7% of patients, although outcomes were not reported. Wallace et al. 77 reported on the sinus tarsi approach for treating fractures of the calcaneus in 100 patients, and only four patients (4%) had diabetes. Kline et al. 78 reported on the outcomes of 112 calcaneus fractures treated surgically. Only three of these 112 patients (2.7%) had diabetes, and the numbers were too few to identify any association with outcomes. A large single center study by Folk et al. 79 reported on 190 fractures in 179 patients who underwent operative treatment of calcaneal fractures, nine of whom had DM (5.0%). Wound complications occurred in seven of nine fractures (78%) associated with DM compared with 41 of 181 fractures (22.7%) (p = 0.02) in patients without DM. A recent long-term series on the outcomes of surgically treated talus fractures included only two patients with DM in their series of 84 patients (2.4%). 80 Case series of other tarsal and metatarsal injuries rarely report on diabetes as a comorbidity. The prevalence of DM as a comorbidity in these series is lower than the prevalence in the general population, suggesting a selection bias against operative treatment of hindfoot, midfoot and forefoot fractures in patients with DM. Consequently, treatments for the foot are generally extrapolated from the principles of managing ankle fractures in patients with DM.
Our treatment protocol for foot fractures in patients with DM follow the established recommendations for treating ankle fractures in patients with DM. The key is identifying patients with and without complicated DM. Foot fractures in patients with uncomplicated DM can be treated like patients without DM. Patients with complicated DM require a more intensive management protocol to prevent or identify complications. For closed, nondisplaced, or mildly displaced foot fractures, splinting is performed. For closed, moderate-to-severely displaced fractures or joint dislocations that cannot be reduced and splinted, a spanning external fixator or percutaneous pinning can be performed. External fixation is particularly useful in patients with skin compromise.
Definitive stabilization is performed when the soft tissue envelope has recovered. 51 Immediate open reduction is rarely indicated, and optimization of skin may require a delay in surgery ranging from several days to several weeks. Similar treatment for doubling the amount of fixation, doubling the amount of non-weight-bearing and doubling the number of office visits are appropriate for foot fractures in patients with complicated DM. In patients with complicated DM and comminuted intra-articular foot fractures, our preference is ORIF and primary arthrodesis.
Some of the available literature discusses the correlation of DM foot fractures and its relationship to Charcot neuroarthropathy. Establishing an association between foot fractures as a precursor to Charcot neuroarthropathy may be challenging in the setting of delayed presentation for medical care due to peripheral neuropathy. Nearly 50% of patients with DM-related peripheral neuropathy with Charcot neuroarthropathy may not even recall a specific injury. Seemingly trivial injuries in patients with complicated DM (minor fractures, sprains, strains, and contusions) and normal radiographs can develop Charcot neuroarthropathy several weeks later, as seen in Figure 8. In patients with complicated DM, immobilization, offloading and non-weight-bearing precautions is prudent, as normal plain film radiographic findings of foot injuries often precede a diagnosis of Charcot neuroarthropathy. In a series of DM patients with 14-foot fractures, seven developed Charcot neuroarthropathy of the foot: forefoot (n = 1), midfoot (n = 5) and hindfoot (n = 1). All the patients who developed Charcot neuroarthropathy had a delayed diagnosis or inadequate initial treatment. The patients in this series who did not develop Charcot neuroarthropathy were treated on average at 1 week from onset of symptoms, compared with 8 weeks in the group that developed Charcot neuroarthropathy. 81 In some cases, radiographs may not show obvious foot fracture, but increased soft tissue swelling is an early sign of Charcot neuroarthropathy. 82 In addition, further evaluation of stability of the foot may be warranted with weight-bearing radiographs. Advanced imaging with MRI or CT is also beneficial in high-risk patients with normal radiographs.

(a) normal radiographs in a patient with complicated DM who presented after minor sprain (b) several weeks later the patient developed CNA of the midfoot.
Perioperative management
Pathways should be in place for perioperative management of patients with DM who fracture their foot and ankle. Glycemic targets for hospitalized patients should follow national standards depending on whether or not the patient in is the intensive care unit or on the medical surgical post care unit. The goal is to optimize glycemic management without increasing the risk of hypoglycemia. Early mobilization is important for several reasons. First, it reduces the risk of soft tissue pressure injury (decubitus ulcers). Second, it decreases the risk of thromboembolism. Third, it improves pulmonary function. Perioperatively, diabetic patients are at risk for acute kidney injury, and judicious hydration is important. Comorbid conditions beyond those directly related to DM, such as malignancy, may influence healing as well. In addition, low energy falls in patients with DM indicate bone fragility, and further evaluation may be warranted to prevent future fragility fractures. The ideal perioperative program should be multidisciplinary in nature. 2
Conclusion
Health care providers will see more foot and ankle fractures as the prevalence of DM rises globally. The presence of neuropathy, nephropathy, PAD, and retinopathy (complicated DM) increases the complication rate of fracture treatment compared with patients without these complications. Prompt treatment and referral to an experienced foot and ankle specialist can improve outcomes in this vulnerable cohort of patients.