
Abstract
We present a case of calcaneal reconstruction after both an improvised explosive device injury and subsequent salvage procedures left the patient with a large calcaneal defect and damaged hindfoot soft tissue. A subtalar arthrodesis was performed with a femoral head allograft, where it was fused to the remaining calcaneus and superiorly through the talus, to successfully reconstruct this defect. Demineralized bone matrix, bone morphogenetic protein, and concentrated bone marrow aspirate were also added as adjuncts to promote bone remodeling. At final follow-up, the patient denied pain, was fully weight-bearing, and had resumed an active lifestyle.
Keywords
Introduction
Fractures of the calcaneus represent 1%–2% of all fractures and are typically sustained in a high-energy fashion from falls from a height or motor vehicle accidents. 1 Injuries of the calcaneus can significantly restrict global foot function due to hindered subtalar motion, as the joint is crucial in load transmission and accommodating uneven surfaces. 2 In addition, as the calcaneus bears approximately 80% of the body’s weight, calcaneal fractures compromise weight-bearing and normal ambulation. 3
Calcaneal fractures can present as either open or closed, though open is more rare.4,5 Outcomes of open fractures of the calcaneus are more unpredictable than closed injuries, with higher rates of infection and an incidence of osteomyelitis as high as 19% compared to 1%–4% in closed cases.4,5
In this case report, the patient presented with a large calcaneal defect after multiple foot salvage surgeries for a high-energy open calcaneal injury. There is no consensus regarding the treatment of these types of injuries.6–8 This case report aims to discuss complex calcaneal reconstruction with a femoral head allograft and the impact of biologic adjuncts, including demineralized bone matrix (DBM), bone morphogenetic protein (BMP), and concentrated bone marrow aspirate (cBMA). The patient has given us written consent to publish data from their case.
Case report
A 29-year-old male presented with persistent hindfoot pain at the level of the ankle over the last 14 months and the inability to ambulate without the use of an assistive device and ankle-foot orthoses (AFO). He had sustained a lower limb injury several years prior from an improvised explosive device (IED) explosion while serving in the armed forces in Saudi Arabia. The explosion caused severe damage to his right leg, including a fractured calcaneus with extensive hindfoot soft tissue injury. At the military hospital, he had undergone 15 operations over a period of 3 months to manage his hindfoot injuries, including multiple irrigations and debridement surgeries and open reduction and internal fixation of a complex calcaneal fracture. The patient subsequently developed osteomyelitis of the calcaneus and required a partial calcanectomy, split skin grafts, and several wound debridement surgeries.
On examination, the patient displayed 20° of dorsiflexion and 5° of plantarflexion with 3/5 muscle strength for both, and poorly healed skin over the hindfoot (Figure 1). The patient exhibited an antalgic gait and was unable to perform a unilateral heel raise. Upon ambulating, the patient reported pain on the anterior joint line and from deep within his ankle. Preoperative X-ray images suggested post-surgical changes related to his previous subtotal resection of the posterior aspect of the calcaneus to the level of the middle subtalar joint with abnormality of the overlying soft tissues related to scarring (Figure 2).

A preoperative image of the medial aspect of the right foot displays scars from previous procedures.
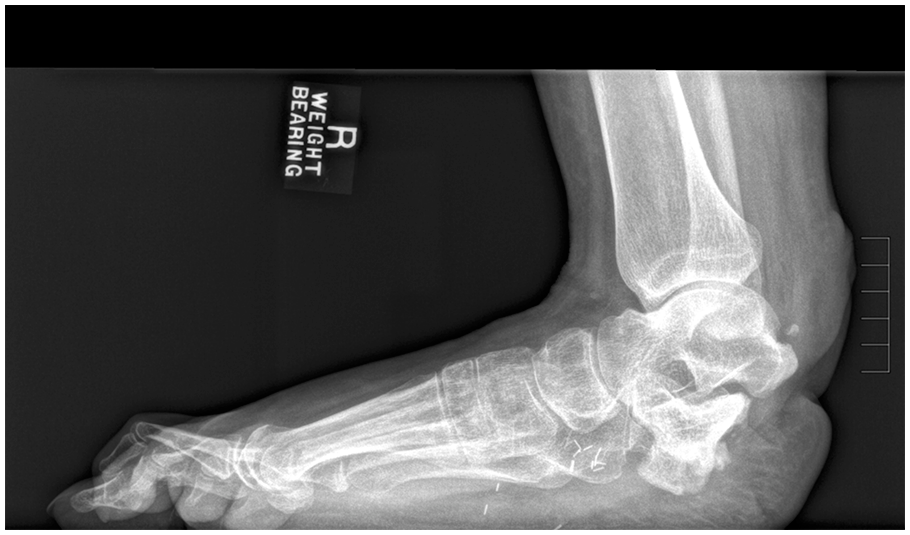
A preoperative lateral weight-bearing radiograph of the right foot demonstrates a partial calcanectomy.
In a multidisciplinary effort, we proposed to the patient a two-component procedure. To address the structural loss due to the partial calcanectomy, we decided upon a femoral head allograft to provide greater hindfoot support while weight-bearing. To achieve adequate soft tissue coverage following the placement of the allograft, a tissue expander was proposed and a secondary plastics closure was considered.
During the procedure, an approach was made over the previous incision, which was cicatrized, avoiding injury to the neurovasculature. A tenosynovectomy of the Achilles was performed. The distal aspect of the Achilles was liberated and advanced to the most distal aspect of the talus and to the femoral allograft, where it was secured with suture anchors. A calcaneal exostectomy was then performed to remove any compromised bone followed by a gram stain and culture to rule out any source of sequestrum. A 44-mm femoral head allograft was osteotomized and shaped to incorporate with the remaining calcaneus and to mimic the contralateral calcaneus’s anatomy. The soft tissue envelope reshaped the size of the allograft, and fluoroscopy was used to confirm that primary closure could be obtained with insertion of the allograft. Once the articular surface was prepared, DBM, BMP-2, cBMA, and the femoral head allograft were placed in the interface of the reconstructed calcaneus to provide both an osteoconductive and osteoinductive environment, along with growth factors and anti-inflammatory proteins.9–11 Once the final position was achieved, the subtalar joint was prepared and then fused with two 6.5 mm screws. The screws engaged both the endogenous calcaneus and the allograft (Figure 3).
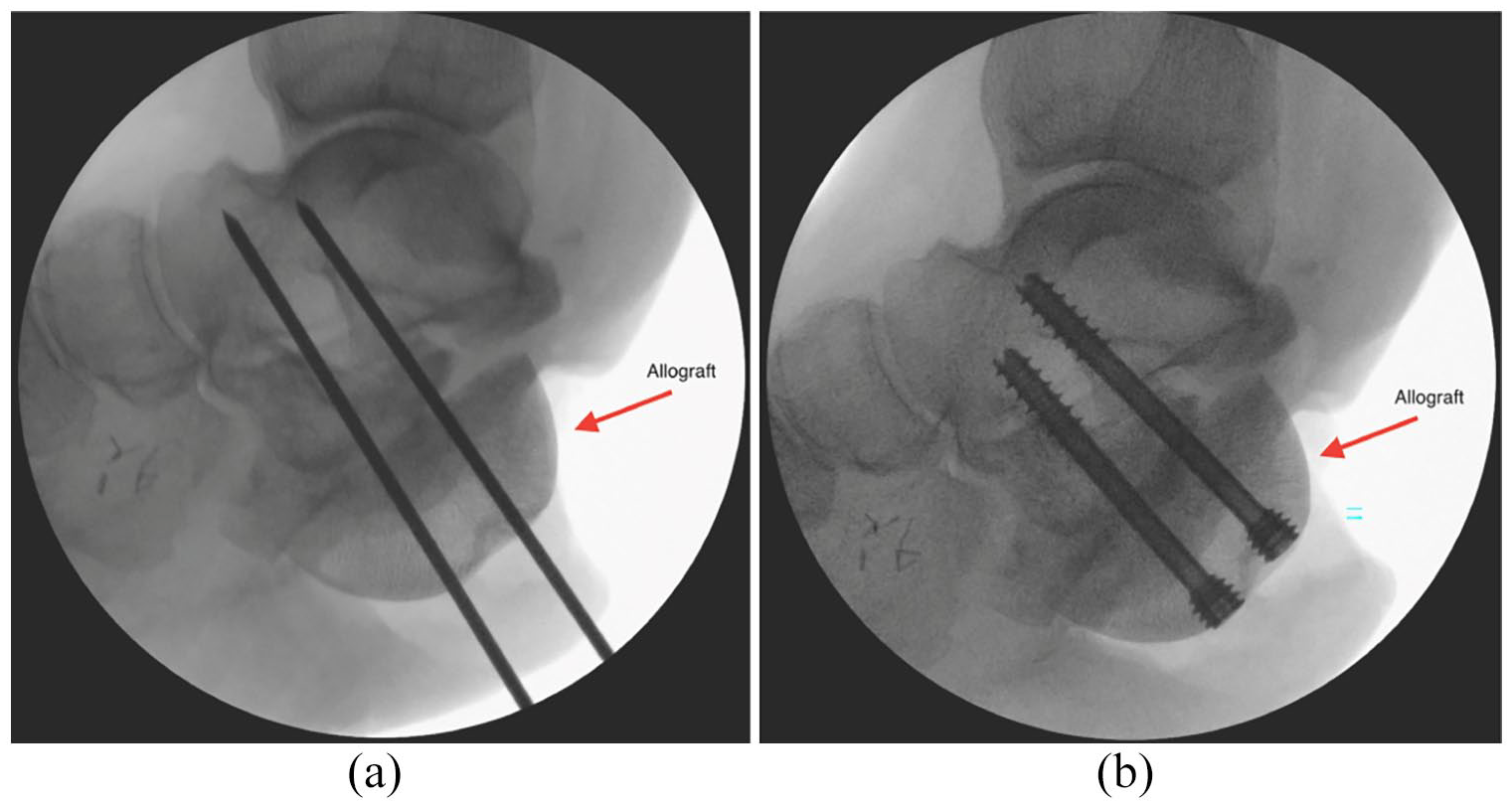
Intraoperative radiographs display (a) K-wire placement and (b) cannulated screw placement for the subtalar arthrodesis involving the femoral head allograft and remaining calcaneus.
After the successful calcaneal reconstruction, the plastic surgery team used a right gracilis muscle flap to close the defect and provide healthy vascularized tissue to the area. Then a split-thickness skin graft was harvested from the upper right thigh and transferred to the vascularized muscle base.
The patient was initially made non-weight-bearing and was placed in a splint. All cultures resulted negative. The soft tissue was stable, with a viable flap and split-thickness graft at 4 weeks post-operation (Figure 4). At approximately 8 weeks post-operation, the patient began weight-bearing at 10% of his weight with wedges in the controlled ankle movement (CAM) boot to offload the Achilles tendon. Radiographs taken at this point showed signs of bone healing (Figure 5). At approximately 12 weeks post-operation, radiographs and the clinical evaluation of increased callus formation allowed a further increase in weight-bearing in the CAM boot with wedges, and the patient was advised to begin physical therapy. At 4 months, radiographs displayed bony consolidation at the host–graft interface and the patient was advised to increase weight-bearing from 60% to 100% in the following weeks.

A 4-week postoperative image of the medial aspect of the right foot which displays soft tissue healing.

An 8-week postoperative lateral non-weight-bearing radiograph showing signs of bone healing.
At approximately 9 months post-operation, the patient presented to the emergency room for heel pain upon weight-bearing, and subsequent images displayed a loose screw (Figure 6). However, 1 month later, he underwent surgery to remove and replace that screw and DBM injected into the screw tract to promote osteoconduction (Figure 7).

A 9-month postoperative lateral non-weight-bearing radiograph demonstrating screw loosening.

Intraoperative radiograph of the hardware replacement: removal of 6.5 mm screw and replacement with an 8.0 mm screw (shown above).
The patient continued to do well but with dorsiflexion restriction and pain, and so he subsequently underwent an in-office nano-arthroscopy procedure to remove anterior scar tissue. He felt immediate relief and normal dorsiflexion was obtained. Radiographs taken at 15 months display osseous bridging across the osseous margins (Figure 8). At a final follow-up of 17 months from the initial procedure, the patient denied any pain and was fully weight-bearing without AFO or other assistive devices. The patient had progressed to an arc of motion of 25° and 4/5 muscle strength for both dorsiflexion and plantarflexion, and was able to perform a unilateral heel raise.
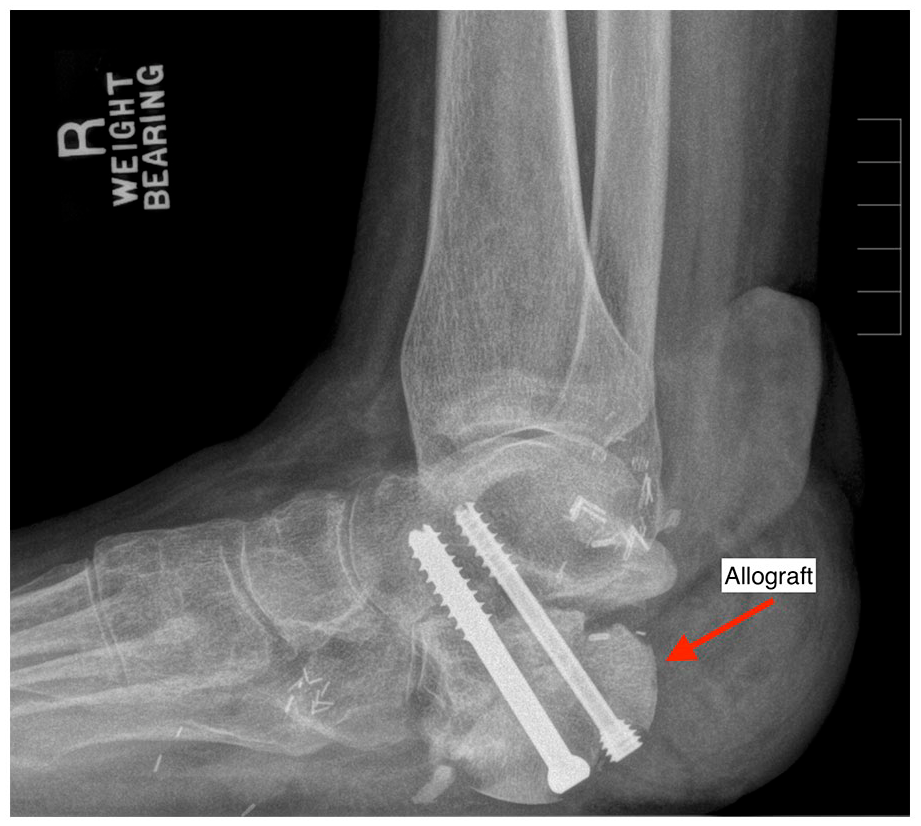
A 15-month standing weight-bearing radiograph displaying subtalar arthrodesis with the presence of osseous bridging across the osseous margins.
Discussion
This patient sustained a significant injury from an IED explosion consisting of extensive calcaneus fracture with soft tissue damage to the lower extremity. Initially, amputation was considered, but as the patient was young and wanted to maintain an active lifestyle, he instead wished to pursue reconstructive options. Thus, we explored a range of treatment options to reconstruct what was remaining of the calcaneus, which had been osteotomized after a number of salvage surgeries, including arthrodesis with several types of bone grafts. To provide greater hindfoot structural support, we needed to augment the patient’s remaining calcaneus. Allografts, autografts, and custom synthetic implants have been shown to provide sufficient support as bone replacement tools for foot and ankle injuries. 12 The possibility of donor site morbidity increases as the size of the autograft increases, and considering the defect spanned approximately 50 mm autografting was ruled out. 12 As there remained a small amount of structurally stable calcaneus and we wanted to preserve native anatomy, an implant to replace the calcaneus was ruled out. As the calcaneus bears 80% of the body’s weight, it is important that the allograft provides sufficient structural support under such large forces. 3
Various types of allografts have been used in calcaneal reconstruction, including femoral heads,6–8 fibulas,3,13–15 portions of the ileum,16,17 portions of the anterolateral ribs, 18 and a proximal tibia. 19 To fit the shape of the posteroinferior defect of the calcaneus, the hemi-spherical shape of the femoral head was the best option in this case. Case reports from Loder and Dunn 7 and Mehta et al. 8 using femoral heads for calcaneal reconstruction after calcaneus fracture and subsequent osteomyelitis have shown good outcomes with increased ankle stability and ambulation with follow-ups of 24 and 18 months, respectively. The long-term outcomes of using a femoral head allograft have been studied in total hip arthroplasty (THA) as well. When looking at the use of femoral head allografts to augment acetabular bone loss post-THA, Butscheidt et al. 20 found that the allograft showed intact structure, significantly higher mineralization than the host bone, and an average of 7.2 mm of ingrowth with a mean follow-up of 12.9 years. Subtalar, 19 calcaneocuboid,19,21 and fusions to the remaining calcaneus7,8 have been used to help manage large defects of the calcaneus. We decided upon a subtalar fusion through the allograft and remaining calcaneus as it would preserve ankle joint range of motion and inversion/eversion ability while providing strong hindfoot structural support.
In this case, three biologics were used to enhance the bone graft through osteoinduction, osteoconduction, and osteogenesis. To provide structural support, a DBM gel was added to the articular surfaces of the joints that were being arthrodesed. DBM is a decalcified form of allograft bone that contains collagen and other proteins, and osteoinductive growth factors such as BMP-2 and BMP-4.22,23 As it is mainly osteoconductive, it creates a matrix for endogenous bone infiltration but lacks the ability to induce infiltration and subsequent differentiation. 10 Therefore, to further promote osteogenesis, BMP-2 was added to the DBM. BMP-2 is a member of the transforming growth factor-beta (TGF-β) superfamily of cytokine signaling molecules, which exhibit osteoinductive properties. 9 BMP-2 induces differentiation of mesenchymal stem cells (MSCs) into both osteoblasts and chondroblasts, leading to bone and cartilage restoration. 23 James et al. 24 showed that recombinant human BMP-2 (rhBMP-2) significantly improved rates of union for both acute trauma and posttraumatic reconstruction of the extremities. The senior surgeon used both DBM and BMP-2 to provide a scaffold for future bone growth and osteoinductive media to induce infiltration and differentiation in the scaffold itself, respectively. The combination of DBM and BMP-2 has been suggested by Campana et al. 25 and has been shown to have applications in cranial, maxillofacial, spinal, and ankle procedures.26–30 Specifically, in a 2013 study of craniofacial reconstruction by Francis et al., 26 DBM and rhBMP-2 had a 97.2% success rate compared to 84.2% with iliac crest bone grafting.
Another biologic adjunct, cBMA, was added to the DBM and BMP-2 mixture to augment bone regeneration. cBMA is a concentrated form of bone marrow aspirate, which is harvested from the patient’s iliac crest, and then centrifugated to separate the leukocytes, MSCs, and platelets from the erythrocytes. 11 Besides these main cellular components, cBMA is enriched in various growth factors, such as platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), and TGF-β 1, 2, 3. 31 As PDGF and VEGF both promote angiogenesis, the increased perfusion can accelerate the bone healing process. 32 VEGF has also been found to play a role in bone formation and bone homeostasis, with direct signaling effects on bone cells themselves. 33 In addition, members of the TGF-β superfamily have been shown to be important in osteoblast differentiation.9,34 This cBMA also contains anti-inflammatory cytokines, such as interleukin-1 receptor antagonist protein (IL-1Ra), which is a competitive inhibitor of IL-1’s pro-inflammatory and catabolic effects.11,31 There is also a small population of MSCs found in cBMA, which has immunomodulatory effects and the potential to differentiate into osteoblasts, and can be stimulated by the PDGF present in the cBMA.11,35 Literature about the use of cBMA with allografts for foot and ankle surgery is limited, but there are examples in lumbar36,37 and cervical spinal fusions,38,39 and for long bone nonunions. 40 Specifically, the 2018 paper by Barber et al. 38 looking at 92 patients with 122 cervical levels undergoing anterior cervical discectomy and fusion showed in their Kaplan–Meier analysis that their BMA cohort had a higher probability of fusion at all time points. 38
Conclusion
At the final follow-up of 17 months, the patient had made significant improvements in the range of motion of the ankle and denied pain in the right lower extremity. The patient displayed good hindfoot alignment when weight-bearing and was able to perform a unilateral heel raise without difficulty. This case report highlights the need for structural allografts in large bone defects. It also demonstrates that a combination of biologic agents can affect positively the incorporation of the graft–host bone interface in a previously biologically compromised location.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John G Kennedy has consulting fees from Arthrex Inc., In2Bones, and Isto Biologics.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: John G. Kennedy would like to acknowledge Mr and Mrs Michael J Levitt for their research support.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.