
Abstract
Cancellous bone grafts from the calcaneus have been used for the foot and ankle as well as iliac bone graft; however, there is a sparse report for calcaneal bone transplantation in the field of rheumatoid foot surgery. In this study, safety and usefulness of calcaneal bone grafts, and combination with interconnected porous hydroxyapatite ceramic, was evaluated in rheumatoid arthritis foot surgeries. Of six rheumatoid arthritis cases, three (talo-navicular joint fusion) used a calcaneal bone graft alone, and the remaining three cases (subtalar joint and talo-navicular joint fusion) used a combination of calcaneal bone graft and interconnected porous hydroxyapatite ceramic augmented with dense calcium hydroxyapatite for subtalar bony defect (1.5–2.0 cm) after the correction. Pre- and postoperative Japanese Society for Surgery of the Foot rheumatoid arthritis foot ankle scale scores were obtained for the clinical assessment. As radiographic assessment, tibio-calcaneal angle, calcaneal pitch, talo-1st metatarsal angle, and pronated foot index were also evaluated. After starting weight-bearing or walking, there was no pain and skin trouble at the fusion and harvesting sites. All cases achieved bony fusion within 6–10 weeks. Japanese Society for Surgery of the Foot rheumatoid arthritis foot ankle score was improved in all six cases. Furthermore, tibio-calcaneal angle, talo-1st metatarsal angle, and pronated foot index were also improved at latest follow-up in all cases. In conclusion, autologous bone grafting from the calcaneus was safe and convenient even in rheumatoid foot surgeries. For larger bony defects (1.5–2.0 cm), combination use with interconnected porous hydroxyapatite ceramic augmented with dense calcium hydroxyapatite was also useful.
Keywords
Introduction
Rheumatoid foot deformity often causes severe pain, disability walking, and infected callosities. In such situations, surgical intervention is required and then corrective osteotomy and corrective arthrodesis are often performed. In these surgeries, bone transplantation is needed for bony fusion and bony defect filling. For such cases, autologous bone grafts from the iliac crest have been classically used in many orthopedic surgery procedures, including the fore-mid-hind foot and ankle.1–7 However, harvesting bone grafts from the iliac crest has some issues, including pain, fracture at the harvesting site, deep/superficial infection, hematoma, and sensory loss.1–7 Furthermore, if possible, iliac bone should be preserved for larger joint and spine surgeries in patients with rheumatoid arthritis (RA). Thus, cancellous bone from the calcaneus has been used for autologous bone grafting 8 for RA foot and ankle surgeries in our group hospitals. Furthermore, harvesting of calcaneal bone grafts can be done in the same surgical site of the foot. In cases that require more volume of bone graft (correction of severe subtalar joint deformity), combination use of calcaneal bone graft and interconnected porous hydroxyapatite ceramic (IP-CHA; NEOBONE®, Aimedic MMT, Tokyo, Japan) has been used. NEOBONE® has a three-dimensional and abundant interconnected pore structure that has the advantage of inducing bone tissue and local bone repair.9,10 Taken together, the concept of using autologous grafts from the calcaneus and the combination with IP-CHA should have some advantages not only for bone formation/fusion but also for convenience in rheumatoid foot surgery. However, there is a sparse information in the field of rheumatic foot surgery about calcaneal bone grafting, or combined use with artificial bone substitute. In this study, the usefulness of these procedures in rheumatoid foot surgery was evaluated.
Cases
Autologous bone transplantation as part of surgery for painful foot deformity/destruction was performed in six RA cases. Of these six cases, three (talo-navicular joint fusion against destruction of the longitudinal arch and/or abduction deformity/destruction of talo-navicular joint without valgus hindfoot) used calcaneal bone grafts alone. The other three cases (subtalar joint and talo-navicular joint fusion against pes planovalgus deformity (valgus hindfoot, destruction of longitudinal arch, and abduction deformity)) used a combination of calcaneal bone grafts and IP-CHA (NEOBONE®) for the subtalar bony defect after correction. All of these three cases (cases 3–5 in Table 1) showed severe reduction of talo-1st metatarsal angle (destruction of longitudinal arch) and pronated foot index (abduction deformity of the foot), so correction/fusion was done not only in subtalar but also in talo-navicular joint. The patients’ demographics are shown in Table 1. The reporting of this research was approved by the Institutional Ethical Review Board at the Osaka University Hospital (approval number: 14219) and the Osaka Minami Medical Center (approval number: 28–12), and informed consent was obtained from the patients.
Patients’ demographics.

DMARDs: disease-modifying anti-rheumatic drugs; MTX: methotrexate; IFX: infliximab; TCZ: tocilizumab; talo-navi: talo-navicular joint; subtalar: subtalar joint; calcaneus: cancellous bone graft from the calcaneus; IP-CHA: interconnected porous hydroxyapatite ceramic.
Each parameter at surgery is reported for each case individually.
Surgical technique for harvesting calcaneal bone grafts
As described previously, a skin incision was centered 2 cm anterior to the posterior aspect of the calcaneus and 2 cm superior to the plantar aspect of the foot over the lateral aspect of the calcaneus. 8 After approaching the lateral calcaneal wall with care to avoid injury to the terminal branches of the sural nerve, insertion of Achilles tendon and plantar fascia was retracted by elevatoriums. Then, periosteum was elevated, and a 7-mm square fenestration was made on the lateral calcaneal wall. Then, cancellous bone was harvested using a curette while taking care to prevent penetration of the medial cortex. After removal of the bone graft, the harvested site was filled with porous β-tricalcium phosphate (β-TCP; OSferion 60®, Olympus Co., Tokyo, Japan). Finally, a 7-mm square area of retracted cortical bone was returned to its original place and stabilized by suture of the periosteum and subcutaneous soft tissue (Figure 1(a)–(c)).
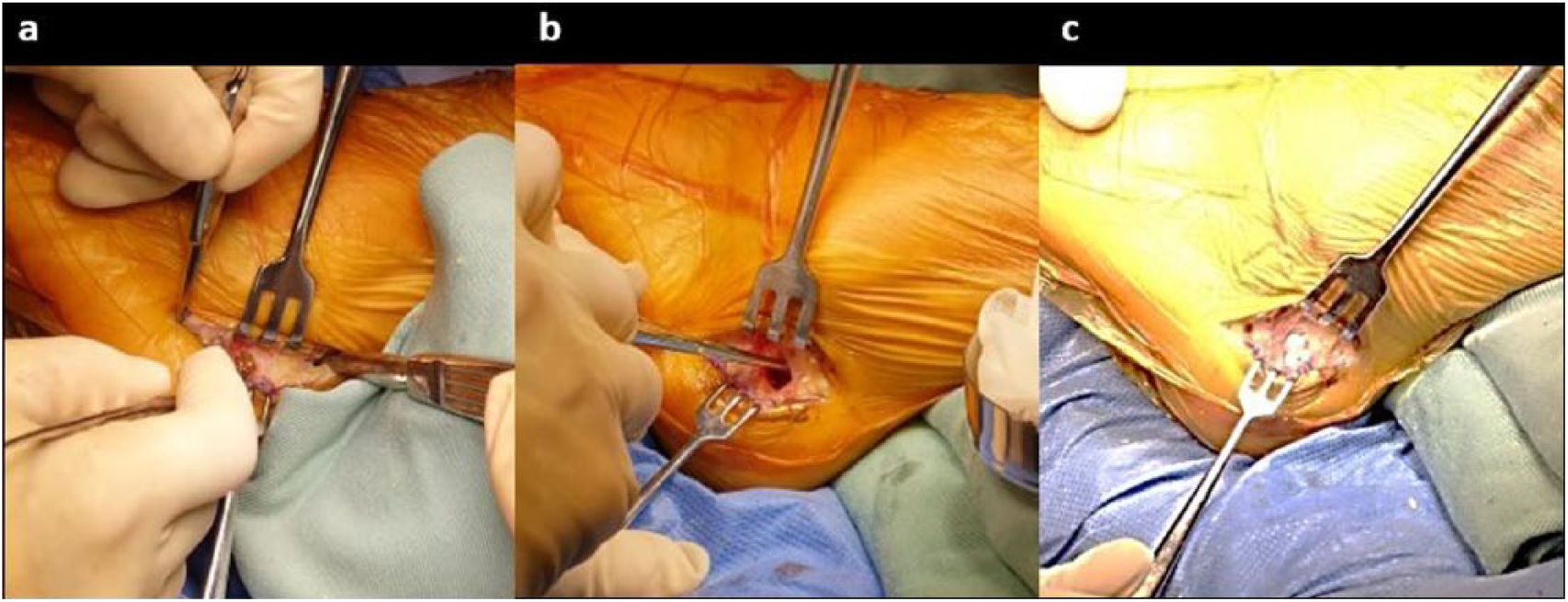
A series of pictures showing harvesting of a calcaneal bone graft: (a) skin incision and approaching the lateral calcaneal wall. The insertion of the Achilles tendon and plantar fascia are retracted by the elevatorium. (b) A 7-mm square fenestration is made on the lateral calcaneal wall, and a cancellous bone graft is harvested using the curette. (c) After removal of the bone graft, the harvested site is filled with porous β-TCP.
Talo-navicular joint arthrodesis
Four centimeters of skin incision was made between tibialis anterior tendon and tibialis posterior tendon on navicular bone for approaching to talo-navicular joint. After approaching to talo-navicular joint, decortication and drilling using 2-mm Kirscner wire (K-wire) was done. After that, bony defect after the correction (adduction and plantar flexion) was filled with harvested autologous calcaneal bone (Figure 2(a) and (b)). After the correction, increased calcaneal pitch, re-formation of longitudinal arch, and adduction correction of the foot were confirmed using fluoroscopy. Then, internal fixation was performed with cannulated screws and staples (Figure 2(b)).
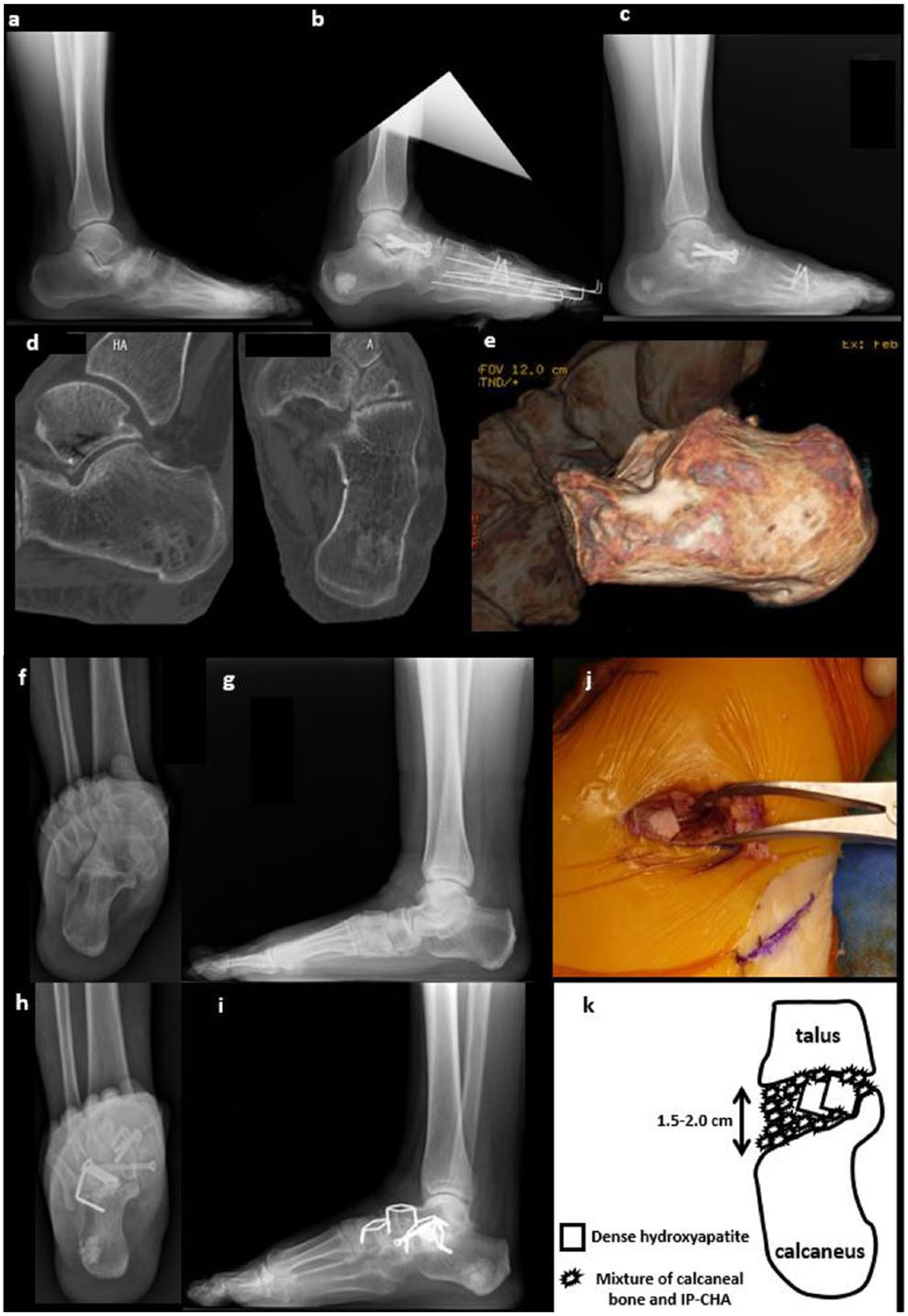
Radiographic and CT analysis of a representative case that underwent talo-navicular and subtalar joint arthrodesis: (a) lateral preoperative radiograph of the foot in the standing position (weight-bearing). The talar bone shows plantar flexion deformity against the navicular bone. (b) Lateral postoperative radiograph just after talo-navicular joint arthrodesis. Autologous bone grafting from the calcaneus was used, and the position of the talar bone is dorsally corrected. Surgery for the forefoot deformity was also performed simultaneously. (c) Lateral postoperative radiograph of the foot 3 months after surgery. Bony fusion between the talus and navicular bone has been completed. In addition, the size of the transplanted β-TCP area in the calcaneus is reduced. (d): Sagittal and transverse views of CT analysis 12 months after surgery. Transplanted β-TCP at the harvesting site is almost completely transposed to bone trabecula of host bone. (e) Three-dimensional (3D) CT data show that cortical bone in the lateral wall of the calcaneus (site of the fenestration) is completely restored 12 months after surgery. (f) Preoperative radiograph showing the subtalar joint view. The hindfoot shows severe valgus deformity. (g) Lateral preoperative radiograph of the foot in the standing position (weight-bearing). The talar bone shows plantar flexion deformity against the navicular bone. (h) Postoperative radiograph showing the subtalar joint view. The valgus hindfoot was corrected to normal alignment. (i) Lateral postoperative radiograph of the foot 3 months after surgery. Bony fusion at the talo-navicular and subtalar joints is completed (joint between navicular and medial cuneiform was also fused in this case). Surrounding transplanted β-TCP has been resorbed, but most β-TCP has remained in this case. (j) Intraoperative picture from lateral view. After the refreshment of subtalar joint, the joint was spread (2.0 cm of width) by spreader, subsequently varus correction was completed. Dense hydroxyapatite (APACERAM®) was implanted to support and augment corrected subtalar joint. After that, calcaneal bone grafting combined with the IP-CHA (NEOBONE®) was filled. (k) The scheme of filling the spread subtalar joint using calcaneal bone graft combined with IP-CHA with the augmentation by dense hydroxyapatite. This schematic diagram was designed and illustrated by the first author (M.H.)
Subtalar joint arthrodesis
Four centimeters of skin incision was made on sinus tarsi for approaching to subtalar joint. After approaching to subtalar joint, decortication and drilling using 2-mm K-wire was done. After that, bony defect after the correction (varus) was filled with the mixture of harvested autologous calcaneal bone and IP-CHA with augmentation using dense calcium hydroxyapatite (APACERAM®, HOYA Technosurgical Co., Tokyo, Japan) was done at subtalar joint. Between 2 and 5 g of IP-CHA (NEOBONE®) was mixed with harvested calcaneal bone before transplantation. Mixed volume of NEOBONE® was arranged according to size of the bony defect. Half of the mixture was covered in the medial end of subtalar joint, then APACERAM® was placed to sustain talus and calcaneus, finally the other half of mixture was covered in the lateral side of subtalar joint. After the correction, increased calcaneal pitch, re-formation of longitudinal arch, and adduction correction of the foot were confirmed using fluoroscopy. Then, internal fixation was performed with cannulated screws and staples (Figure 2(f)–(j)). The schematic diagram is shown in Figure 2(k).
Medication during surgery
Methotrexate (MTX) treatment was continued during surgery. Infliximab (IFX) treatment was also continued. Because IFX was administered bimonthly, surgery was performed 1 month after the last administration, and re-administrated 1 month after the surgery. Tocilizumab (TCZ) treatment (subcutaneous injection) was skipped before surgery and re-started after wound healing was completed (normally 2–3 weeks after the surgery).
Postoperative procedures
After surgery, the affected feet were fixed with below-knee (BK) casting for 4–6 weeks, at which time, range of motion (ROM) exercises of the ankle joint were started. Between 6 and 10 weeks after surgery, bony fusion at the surgical site was checked by radiography and computed tomography (CT), and partial-weight bearing was gradually allowed.
Evaluation
Preoperative and postoperative scores for the RA foot ankle scale11,12 using the Japanese Society for Surgery of the Foot (JSSF) standard rating system was obtained11,12 for the clinical assessment. The period of time (minutes) spent harvesting the calcaneal bone grafts (from the time of skin incision to completion of periosteum/subcutaneous soft tissue suture) was checked. Radiographic changes at the sites of bony fusion and bone graft harvesting were also checked over time. Finally, postoperative issue of harvesting site was also evaluated. Pre- and postoperative tibio-calcaneal angle (TC angle) was measured with subtalar view radiographs using the modified Cobey’s method 13 to evaluate hindfoot alignment. Furthermore, calcaneal pitch, talo-1st metatarsal angle, and pronated foot index (normal > 65°) 14 were also evaluated.
Results
No patients complained of pain at the bony fusion site or the harvesting site after surgery. No skin trouble or numbness was seen at the harvesting site. After starting weight-bearing and walking, no pain and no fracture was reported at the fusion site and the harvesting site. All cases achieved bony fusion within 6–10 weeks (Figure 2 and Table 1). The size of the bony defect at the harvesting site of the calcaneus decreased gradually (Figure 2(c)). Within 12 months, almost all of the transplanted β-TCP apatite was absorbed and transposed to host bone (Figure 2(d)), and the fenestrated lateral wall of the calcaneus was completely restored (Figure 2(e)). As clinical outcomes, JSSF RA foot ankle scale was improved in all of six cases. As radiographic outcomes, TC angle, talo-1st metatarsal angle, and pronated foot index were also improved after surgery in all cases (Table 2).
Clinical and radiological assessment.

Pre: at preoperative; Latest: at latest follow-up; JSSF RA foot and ankle scale: scores for the rheumatoid arthritis foot ankle scale using the Japanese Society for Surgery of the Foot (JSSF) standard rating system; TC: tibio-calcaneal.
Discussion
Calcaneal bone grafts also had been used in foot and ankle surgery, 8 as well as iliac bone graft. Furthermore, recently calcaneal bone grafts are also utilized in autologous matrix-induced chondrogenesis technique for the treatment of osteochondral talar lesion. 15 However, their usefulness and safety in rheumatoid foot surgery has not yet been reported. In our limited experience, autologous bone grafting from the calcaneus was very useful and safe even in RA patients. The mean time spent for harvesting was 15 min (Table 1), which was not long, so it was also considered to be a useful point for the surgery. Furthermore, it is convenient that calcaneal bone grafts can be harvested in the same surgical site of the foot. As shown in Figure 2(d), transplanted β-TCP at the harvesting site was almost completely transposed to bone trabecula of host bone, and cortical bone in the lateral wall of the calcaneus was completely restored (Figure 2(e)). If additional foot surgery is required in the future, autologous bone grafts could be harvested again from the same site, because the rheumatoid foot often shows a comprehensive deformity in the hind-mid-forefoot. Recently, allografts have also been used as a novel form of bone transplantation that has been described as useful and safe.16,17 Furthermore, other orthobiologics and other synthetic bone grafts including cellular bone allograft containing mesenchymal stem cells, bone marrow aspirate, platelet-derived growth factor, platelet-rich plasma, bone morphogenetic protein, fatal tissue, and demineralized bone matrix are also recommended for foot and ankle surgery.18–20 However, at present, there are many actual cases for which allografts and other orthobiologics are not available in Japanese hospitals or Japanese health insurance systems. In such situations, combination of calcaneal bone with IP-CHA (NEOBONE®) was also useful for relatively larger bony defects (1.5–2.0 cm) in subtalar joint. Using IP-CHA alone has previously been reported to be useful for large bony defects in correction and fusion of the subtalar joint and the treatment of juxta-articular intraosseous cystic lesions in RA cases.21,22 However, the combination with autologous bone grafting is considered to have more advantages with respect to accelerating bone formation and induction, because autologous bone grafts contain living osteogenic cells, type I collagen, and bone morphogenetic protein. Although there was a concern that skin trouble after the correction would be occurred by stretching the lateral skin, there was no trouble in the process of wound healing. Because of valgus deformity of the hindfoot, lateral skin in the hindfoot was loose in these three cases (cases 3–5). Thus, suturing the lateral skin was easily completed even after spreading of lateral side of subtalar joint (varus correction).
In cases that require cortical bone grafts, this system is not recommended. Combination with dense calcium hydroxyapatite is recommended. Indeed, in this study although maximum bony defect was 1.5–2.0 cm at subtalar joint, combination use of calcaneal bone and IP-CHA augmented with dense calcium hydroxyapatite was useful (Figure 2(f)–(i)). In the present series, bony fusion at the surgical site was achieved in all cases within 6–10 weeks. However, if tight control of RA is not achieved, there might be cases that could not achieve bony fusion, because the transplanted bone graft and/or hydroxyapatite could be absorbed aggressively by activated osteoclasts before sufficient bone formation. In the present series, all cases were tightly controlled by MTX and/or biologics (Table 1). Furthermore, steroid administration must also be considered, because steroid therapy has a suppressive effect on bone formation by osteoblasts. 23 Fortunately, cases in this study with steroid administration also achieved bony fusion and had no problems at the bone harvest site (Table 1).
In conclusion, although this study included a small number of case series, autologous bone grafting from the calcaneus was safe and convenient in rheumatoid foot surgeries. For larger bony defects (1.5–2.0 cm), combination use with IP-CHA and augmentation by dense calcium hydroxyapatite was also useful. If there is a situation that iliac bone or allografts and other orthobiologics were not available, such combination use was also recommended for talo-navicular and/or subtalar joint fusion surgery in RA patients.
Footnotes
Acknowledgements
The authors thank all of medical staffs, rheumatologist, and physical therapists in Osaka University Hospital and National Hospital Organization, Osaka Minami Medical Center.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from Osaka University Hospital (approval number: 14219) and the Osaka Minami Medical Center (approval number: 28–12).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.