
Abstract
Objective
To assess the effect and complications of tibial cortex transverse distraction (TCTD) in treating diabetic foot ulcers and draw attention to the concerning issues of this procedure.
Methods
This case series included 30 patients with diabetic foot ulcers from four centers. The ulcers had not healed after >6 months. The patients then underwent TCTD combined with other procedures (debridement, vacuum sealing drainage, and others). All patients were followed up for >12 months postoperatively.
Results
Three patients underwent amputation because of aggravated infections. Tibial fractures occurred in two patients after surgery, and the fractures healed after 3 months of plaster fixation. Pin-site infections occurred in five patients, and the infected pin site healed after the patients underwent pin removal and dressing changes for 3.3 ± 2.1 weeks. The ulcers of the other 27 patients healed by 13.5 ± 8.2 weeks postoperatively, and the postoperative visual analog scale score was significantly lower than the preoperative score.
Conclusions
Although TCTD can be performed as an adjuvant treatment for diabetic foot ulcers, the effect should not be exaggerated and the complications should not be ignored. Further research is needed to propose a standard operative procedure and avoid postoperative complications such as tibial fractures.
Keywords
Introduction
Diabetic foot is a neuropathy associated with long-term diabetes, It is characterized by vascular disease of the lower extremity combined with foot wounds, foot ulcers, and gangrene caused by local bacterial infection of the toes. 1 , 2 Diabetic foot can lead to disability and death in patients with diabetes. Because of the combined effect of vascular ischemia, injury to nerve endings, and infection, a small wound usually does not heal for a long time, finally leading to the need for amputation and causing great psychological trauma to patients and their families. 2 , 3 Therefore, the key points of treatment are restoration of the blood flow of the affected limb and improvement of the microcirculation and oxygen metabolism of the ulcer and its adjacent tissues. Although the treatment of diabetic foot is diverse, the final effect is very limited, and some patients inevitably undergo eventual amputation.
Tibial cortex transverse distraction (TCTD) is a new method for treating diabetic foot based on the tension-stress rule. TCTD technology is reportedly able to stimulate the microvascular circulation of the affected limb, provide the necessary blood nutrients for wound healing of diabetic foot, and therefore produce good results. 4 However, most previous reports described single-center results, and the studies focused on the efficacy of the operation; the complications of the operation were not reported in detail. To verify the effect of this operation, the clinical results of patients from multiple research centers were evaluated in the present study with a focus on the effect and complications of the operation. This report also presents surgeons’ concerns regarding the treatment of diabetic foot ulcer and provides a reference for further clinical treatments.
Materials and methods
Patients
This study was conducted in accordance with the guidelines of the Declaration of Helsinki for Human Research. Informed consent was obtained from all participants, and their rights to privacy were preserved. This retrospective review involved patients with diabetic foot ulcers who underwent TCTD combined with other procedures such as debridement, vacuum sealing drainage, and dressing changes from March 2015 to March 2018 at Jiangxi Provincial People’s Hospital Affiliated to Nanchang University, The First Affiliated Hospital of Nanchang University, Yichun People’s Hospital, and Nanchang Shuguang Hand and Foot Surgery Hospital, China. According to our clinical experience, the indications for surgery were as follows: (1) Wagner grade ≥3 diabetic foot or treatment of diabetic foot by debridement, dressing changes or vacuum sealing drainage, and standard medical treatment for >2 months; (2) little effect of endovascular intervention or surgical vascular bypass graft revascularization alone; and (3) the ability to tolerate surgery and anesthesia. The inability to tolerate surgery and anesthesia was an absolute contraindication. The inclusion criteria were the presence of diabetic foot ulcers and treatment by TCTD. The exclusion criteria were an incomplete medical history, loss to follow-up, and the presence of combined trauma.
Preoperative management
After admission to the hospital, the patients underwent a routine preoperative examination. A consultation with the Department of Endocrinology was arranged, and regular monitoring of blood glucose fluctuations was conducted, with glucose control targets of <8 mmol/L before a meal and <12 mmol/L at 2 hours after a meal. In 22 patients who had foot ulcers with obvious infection, bacterial culture and drug sensitivity testing were performed on the wound exudate, and appropriate antibiotics were selected according to the drug sensitivity results. All patients with Wagner grade 3 and 4 diabetic foot ulcers underwent radical debridement and removal of the infected necrotic tissue, and 12 of these patients were treated with continuous closed negative-pressure drainage.
Surgical technique
After administration of general anesthesia or lumbar anesthesia, the osteotomy area was selected as the medial tibial cortex about 10 to 20 cm below the knee joint. After appropriate positioning, the external fixation frame was fixed at the far and near ends of the tibial osteotomy area with two half nails. Two half nails were then placed in the osteotomy area. An approximately 6-cm-long incision was made at the far and near ends of the osteotomy area of the inner tibia, the subcutaneous tissue was separated, and the inner tibia side was exposed. The bone flap was then separated from the tibial backbone with a bone knife after drilling, the external fixation device was assembled, and the complete free bone flap was determined. Finally, the incision was sutured (Figure 1).

The procedure of tibial cortex transverse distraction. (a) Schematic diagram of tibial cortex transverse distraction. (b) Intraoperative photograph of tibial cortex transverse distraction.
For large areas of infection or large areas of tissue necrosis over the wound, intraoperative debridement was also performed; pure dry gangrene was not prescribed special treatment. Twelve patients were also treated with continuous closed negative-pressure drainage.
Postoperative management
After the surgery, the patients’ blood glucose fluctuations were regularly monitored, with glucose control targets of <8 mmol/L before a meal and <12 mmol/L at 2 hours after a meal (consistent with the targets of preoperative management). Appropriate antibiotics were selected according to the drug sensitivity results of the preoperative wound exudate and deep tissue culture. The wound dressings were changed and the pin sites were disinfected regularly. The nail sites were strapped with wet diluted povidone iodine gauze. TCTD began 3 to 5 days after the operation and was carried out 1 mm every day for 14 days (Figure 2(a)). The daily 1-mm distraction was divided into three time points (morning, noon, and night). The bone mass was then moved 1 mm in the reverse direction every day; this treatment was also divided into three time points (Figure 2(b)). If the patient felt intolerable pain, the 1-mm movements were performed every 2 days. After the pain had been obviously relieved, the movements were increased to 1 mm per day. The total distraction time ranged from 28 to 30 days in most patients. An X-ray examination was performed every month to evaluate the bone healing, and the external fixation frame was removed after initial healing of the bone window.
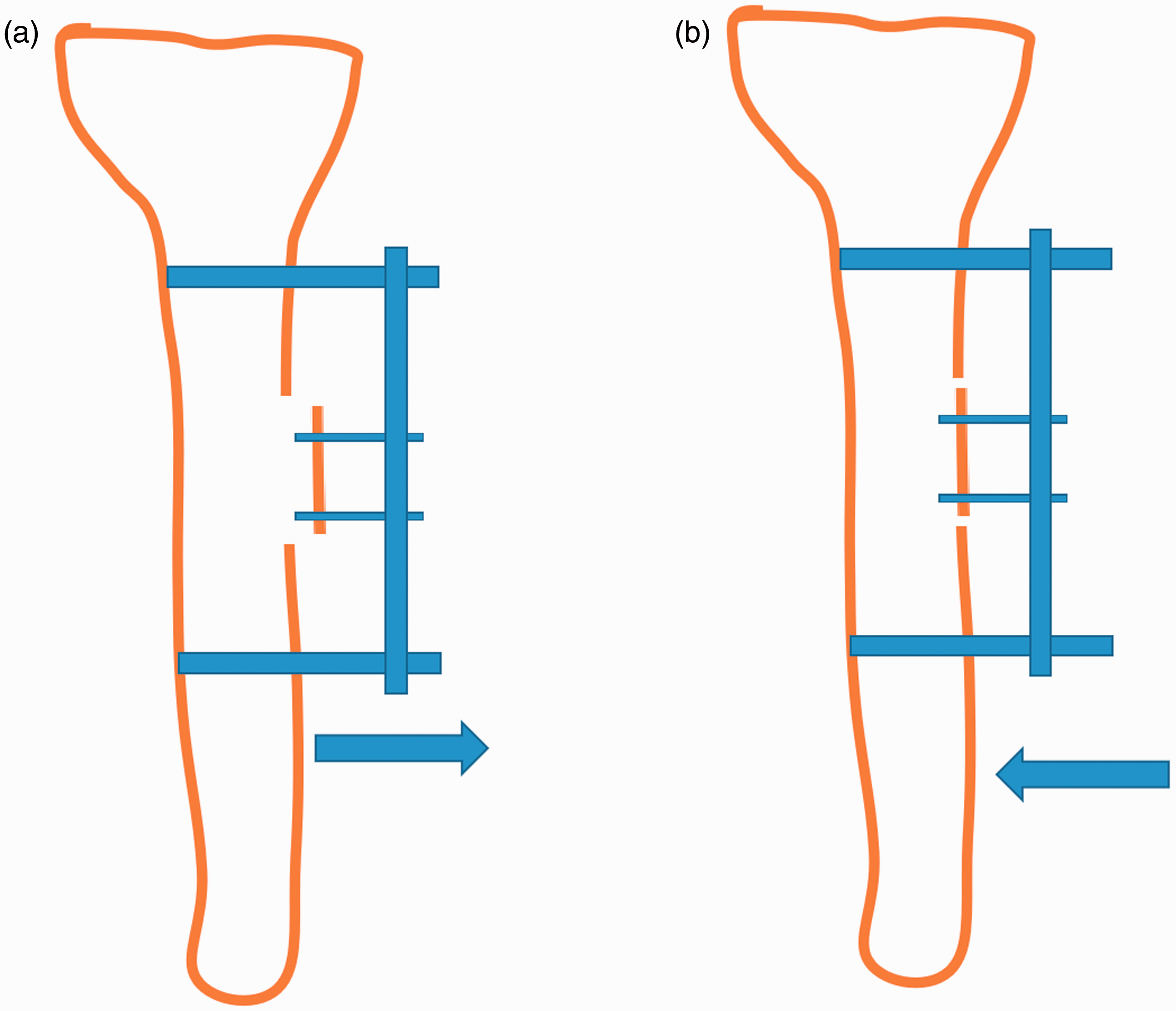
Schematic diagram of postoperative distraction. (a) Schematic diagram of forward distraction. (b) Schematic diagram of reverse distraction.
Postoperative assessment indicators
The patients’ skin temperature, visual analog scale (VAS) pain score, ankle-brachial index (ABI), and wound healing were closely monitored during treatment. Computed tomography angiography (CTA) examination was conducted to check for vascular hyperplasia.
Statistical analyses
IBM SPSS Statistics for Windows, Version 19.0 (IBM Corp., Armonk, NY, USA) was used to calculate the mean ± standard deviation of continuous data. A t test was used to compare preoperative and postoperative data. Statistical significance was set at P < 0.05.
Results
Thirty consecutive patients (21 men and 9 women) with diabetic foot ulcers were included in this study. Their median age was 56 years (range, 42–71 years). Their median duration of time from diagnosis of diabetes to diagnosis of diabetic foot was 17.5 years (range, 2.5–68 years). The left foot was affected in 17 patients, and the right foot was affected in 13 patients. According to the Wagner grading system, 8 patients had grade 2 ulcers, 16 patients had grade 3 ulcers, and 6 patients had grade 4 ulcers. During treatment of Wagner grade 2 and 3 ulcers, the foot exhibited different degrees of redness, exudation, and other signs of infection, and stage 4 ulcers contained dry gangrene at the end of the foot. Lower extremity CTA showed that 30 patients had sub-knee artery occlusion or varying degrees of stenosis with exclusion of other causes of arterial lesions.
All patients were regularly followed up for a mean of 16.5 months (range, 12–26 months). Three patients underwent amputation because of aggravated infections. Tibial fractures occurred in two patients after surgery, and the fractures healed after 3 months of plaster fixation (Figure 3). Pin-site infections occurred in five patients, and the infected pin sites healed after pin removal and dressing changes for 3.3 ± 2.1 weeks. The ulcers of the other 27 patients healed by 13.5 ± 8.2 weeks postoperatively. At the last follow-up, the postoperative VAS score was significantly lower than the preoperative VAS score (3.52 ± 0.45 vs. 6.35 ± 0.54, respectively; P < 0.05), the postoperative skin temperature was significantly higher than the preoperative temperature (36.12 ± 0.19 vs. 35.31 ± 0.34, respectively; P < 0.05), and the postoperative ABI was significantly better than the preoperative ABI (0.43 ± 0.06 vs. 0.56 ± 0.09, respectively; P < 0.05). Postoperative CTA examination showed the formation of collateral circulation, and the superficial artery of the lower extremity had become thicker than that before the operation and was interweaved into a net. No other complications such as bone nonunion or osteomyelitis occurred in any patients. A representative case is shown in Figure 4.

Postoperative tibial fractures.

Representative patient diagnosed with diabetic foot ulcers and treated with tibial cortex transverse distraction. (a, b) Preoperative wound. (c, d) Wound condition 1 year postoperatively.
Discussion
Distraction regeneration is a biological theory proposed by Professor Ilizarov in the 1960s. According to this theory, when biological tissue is slowly and continuously stretched to produce a certain tension, tissue regeneration and active growth can be stimulated. 5 , 6 Professor Ilizarov used this theory to design corresponding external fixation equipment and develop a series of operative techniques. 5 , 6 The concept of “in situ tissue regeneration, natural repair and reconstruction” is regarded as the fourth milestone in the field of modern orthopedic surgery and has the advantages of minimal trauma, a good curative effect, a short operation time, and low cost.5,6 Previous studies have shown that blood flow can be redistributed by promoting angiogenesis in calluses and surrounding soft tissues, thus increasing the number of functional capillaries and promoting an increase in the local blood supply with a corresponding increase in venous reflux. 7 , 8 Transverse bone transfer of the tibia has been used to treat diabetic foot and lower limb ischemic diseases, and good clinical results have been reported. 4 However, large-sample clinical data are currently lacking, and the above conclusions need to be further verified.
In the treatment of nonunion and osteomyelitis, the main complications of tibial longitudinal bone transport are pin-site infection, local skin necrosis, and nonunion. 4 ,9–11 In the present study, four cases of pin-site infection occurred during the use of TCTD; this may have been related to the heat produced by the high-speed electric drill during nail grafting. Additionally, three patients underwent amputation because of aggravated infections. Therefore, the effect of TCTD should not be exaggerated and the complications should not be ignored. Tibial fractures occurred in two patients after surgery, and the fractures healed after 3 months of plaster fixation. Such tibial fractures might be avoided if standard tibial osteotomy criteria are developed for this procedure and postoperative education in fall prevention is conducted. For patients of short stature, the bone window can also be narrowed to avoid tibial fractures. The duration of time that the bone mass is pulled can be further shortened from 3 weeks to 2 weeks, helping to avoid the necrosis caused by excessive bulging of the local bone mass, which presses against the skin overlying the anterior tibia. The pathophysiological process of diabetic foot is complicated, and the curative effect of transverse tibial bone transfer is closely associated with the fields of endocrinology, vascular surgery, and nursing.6–8 High patient compliance is required because of the long duration of bone handling and the effects of the external fixation frame on the patients’ daily life. If necessary, patients can be referred to the mental health department for psychological counseling intervention to improve their mental state. It is also important that patients avoid falling during bone handling and return to the hospital regularly for follow-up.
Diabetic foot is a multifactorial disease. Although TCTD can serve as an adjuvant treatment for diabetic foot ulcers, the effect should not be exaggerated and the complications should not be ignored. Transverse bone transport of the tibia cannot be expected to completely resolve the lesion. Complete debridement, professional wound care, systemic or local anti-infection measures, and control of blood glucose are essential for patients with soft tissue infection, suppuration, and osteomyelitis while conducting TCTD. Further research is needed to establish a standard operative procedure and avoid postoperative complications such as tibial fractures.
Footnotes
Acknowledgement
We would like to thank all participants for their involvement in this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.