
Abstract
Objective
We aimed to present the radiographic and functional outcomes of anatomical reduction and fixation of anterior inferior tibiofibular ligament (AITFL) avulsion fracture without syndesmotic screw fixation in rotational ankle fracture.
Methods
We retrospectively reviewed 66 consecutive patients with displaced malleolar fracture combined with AITFL avulsion fracture. We performed reduction and fixation for the AITFL avulsion fracture when syndesmotic instability was present after malleolar fracture fixation. A syndesmotic screw was inserted only when residual syndesmotic instability was present even after AITFL avulsion fracture fixation. The radiographic parameters were compared with those of the contralateral uninjured ankles. The American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot scores were assessed 1 year postoperatively.
Results
Fifty-four patients showed syndesmotic instability after malleolar fracture fixation and underwent reduction and fixation for AITFL avulsion fracture. Among them, 45 (83.3%) patients achieved syndesmotic stability, while 9 (16.7%) patients with residual syndesmotic instability needed additional syndesmotic screw fixation. The postoperative radiographic parameters were not significantly different from those of the uninjured ankles. The mean AOFAS score was 94.
Conclusion
Reduction and fixation of AITFL avulsion fracture obviated the need for syndesmotic screw fixation in more than 80% of patients with AITFL avulsion fracture and syndesmotic instability.
Keywords
Background
Distal tibiofibular syndesmotic injury is often associated with ankle fracture and is estimated to accompany 10% of all ankle fractures and 20% to 40% of operatively treated rotational ankle fractures.1–5 Distal tibiofibular syndesmosis is crucial for integrity of the ankle joint and thus for weight bearing. 6 Therefore, in the presence of an associated syndesmotic instability following anatomical reduction and fixation of ankle fracture, stabilization of the syndesmosis is essential for improving functional outcomes and avoiding posttraumatic ankle arthritis.5,7–9
Fixation of the ankle syndesmosis using a screw has been the most widely used treatment method for syndesmotic injury. However, detailed methods of syndesmotic screw fixation remain quite controversial.10–18 Furthermore, several drawbacks of syndesmotic screw fixation have been reported, such as malreduction, screw breakage, and the need for screw removal.2,19–28 To overcome the disadvantages of syndesmotic screw fixation, some authors have suggested alternative fixation methods, such as Kirschner wire fixation, suture button fixation, and bioabsorbable screw fixation.29–35
The anterior inferior tibiofibular ligament (AITFL) is one of the four ligaments of the distal tibiofibular syndesmosis. The AITFL provides the most stability against lateral displacement of the distal fibula and is the first ligament subjected to stress upon the application of external rotational force to the fibula.36,37 In syndesmotic injury, disruption of the AITFL may occur through the ligament itself, or bone may be avulsed from the ligament’s insertion to the distal tibia (Chaput tubercle) or fibula (Wagstaffe tubercle). AITFL avulsion fracture reportedly accompanies approximately 10% of surgically treated rotational ankle fractures.38,39 AITFL avulsion fracture was first described by Wagstaffe in 1875, who originally presented three fracture patterns. In 2002, Park et al. 39 suggested the modified Wagstaffe classification for AITFL avulsion fracture. According to the modified Wagstaffe classification, type I is an isolated AITFL avulsion fracture from the fibula without lateral malleolar fracture, type II is an AITFL avulsion fracture from the fibula with lateral malleolar fracture, type III is an AITFL avulsion fracture from the tibia, and type IV is an AITFL avulsion fracture from both the tibia and fibula (Figure 1).
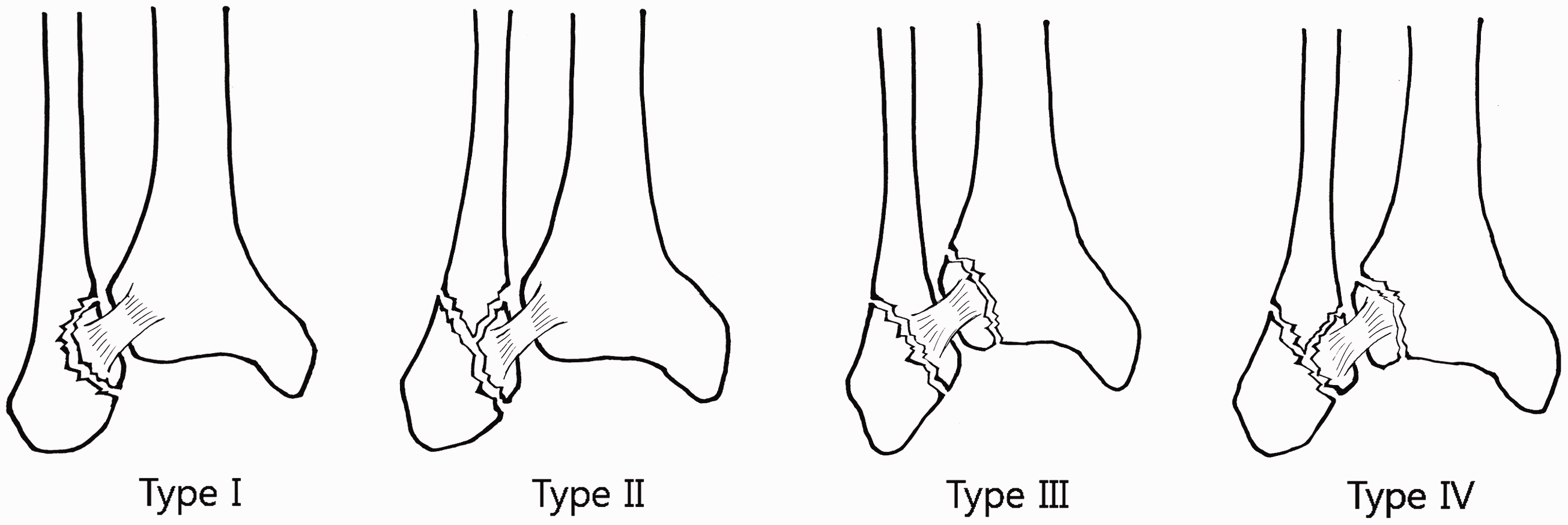
Modified Wagstaffe classification of anterior inferior tibiofibular ligament (AITFL) avulsion fractures.
Although a few reports have described good clinical results of reduction and fixation of AITFL avulsion fracture, there is insufficient evidence that the reduction and fixation of AITFL avulsion fracture without syndesmotic screw fixation can effectively stabilize syndesmotic injuries.38,39 Therefore, in this study, we retrospectively reviewed cases of displaced rotational ankle fracture combined with AITFL avulsion fracture and investigated whether the reduction and fixation of AITFL avulsion fractures without syndesmotic screw fixation can yield satisfactory radiographic and functional outcomes. We hypothesized that anatomical reduction and fixation of AITFL avulsion fracture can be an alternative treatment option for syndesmotic instability following anatomical reduction and fixation of ankle fracture, obviating the need for syndesmotic screw fixation and thereby preventing potential complications.
Materials and methods
Patients
We retrospectively reviewed patients who underwent surgery for displaced rotational ankle fracture at our hospital from 2010 to 2017. The inclusion criteria for this study were as follows: (1) the presence of AITFL avulsion fracture combined with displaced malleolar fracture, (2) the performance of open reduction and internal fixation (ORIF) for the displaced malleolar fracture, and (3) a follow-up period longer than 1 year. The exclusion criteria for this study were as follows: (1) open ankle fracture, (2) comminuted articular fracture of the distal tibia plafond and/or fracture line extension into the metaphysis, (3) a history of trauma or surgery around either ankle, and (4) a history of arthritis in either ankle.
Patient management
The fractures were diagnosed based on simple radiographs (anteroposterior, lateral, and mortise views) and three-dimensional computed tomography (3 D-CT). The average time to the operation was 3.4 days from trauma (range, 2–7 days). All operations were conducted by a single orthopedic surgeon. First, we performed anatomical reduction and internal fixation of displaced lateral malleolar, medial malleolar, and/or posterior malleolar fractures. When a deltoid ligament injury was suspected without medial malleolar fracture (observed as increased medial clear space on simple radiographs), we did not routinely repair the deltoid ligament. Deltoid ligament repair was indicated only when increased medial clear space was observed under fluoroscopy even after syndesmotic stabilization by AITFL avulsion fracture fixation and/or syndesmotic screw fixation. Following the fixation of malleolar fractures, we exposed the anterior syndesmosis under direct vision through a lateral malleolar incision by releasing the superior extensor retinaculum at its fibular insertion. We then checked the gross syndesmotic stability using the hook test. In the hook test, we applied a laterally translating force to the distal fibula using a bone hook in one hand while stabilizing the distal tibia with the other hand. 40 We measured the lateral translation of the distal fibula using a sterilized micrometer ruler. We defined syndesmotic instability as more than 2 mm of lateral translation of the distal fibula, as previously suggested by many authors.40–42 Two surgeons performed the hook test consecutively with a time interval of a few minutes between tests. If there was a discrepancy in the determination of instability between the two surgeons, we regarded the syndesmosis as unstable rather than stable to avoid overlooking any subtle instability. If the syndesmosis was determined to be unstable, we attempted to reduce and fix the AITFL avulsion fracture to stabilize the syndesmotic instability. We used Kirschner wires and 1.7-mm mini screws (Stryker Leibinger GmbH & Co., Freiburg, Germany) or 4.0-mm cannulated screws (OT medical Corp., Seoul, Korea) to fix the AITFL avulsion fragments according to the size of each avulsion fragment (Figures 2 and 3). Following the fixation of the avulsed fragment, the two surgeons repeated the hook test as previously performed to re-evaluate the syndesmotic stability. If the syndesmosis was unstable even after AITFL fixation, we inserted one 3.5-mm cortical screw (OT Medical Corp.) into the syndesmosis under fluoroscopy. After surgery, a short leg cast was applied, and the patients were instructed not to bear weight on the operated limb for 6 weeks. At 6 weeks after surgery, the patients started range-of-motion exercises and gradual partial weight bearing. Full weight bearing was allowed at 8 weeks after surgery. In cases of syndesmotic screw fixation, the screws were removed at 3 months after surgery.
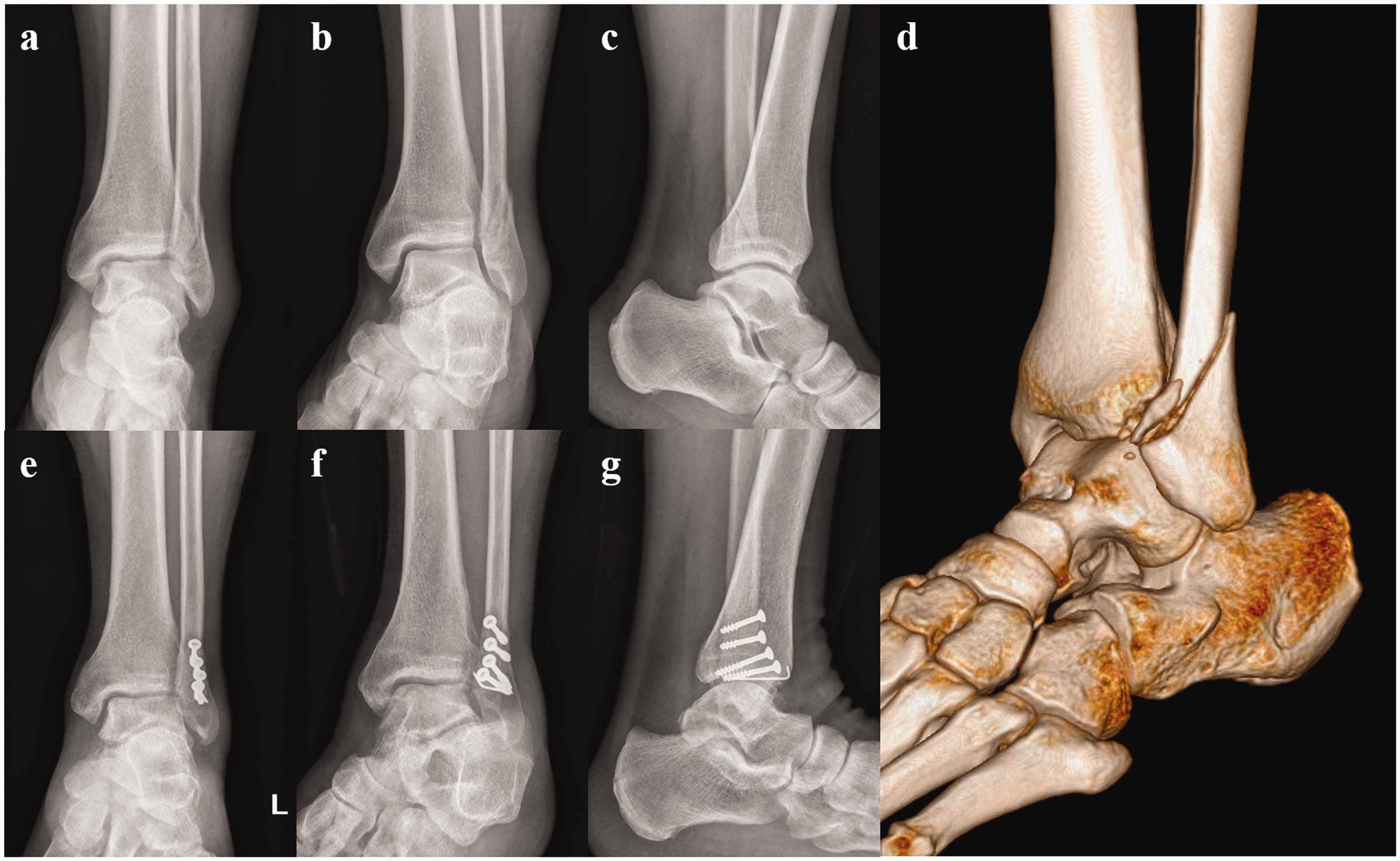
(a–c) Anteroposterior, mortise, and lateral radiographs of the left ankle of a 51-year-old man with a long oblique fracture of the distal fibula. The anterior inferior tibiofibular ligament (AITFL) fibular avulsion fracture is not visible on the simple radiographs. (d) Ankle three-dimensional computed tomography image showing an AITFL fibular avulsion fracture. (e–g) Anteroposterior, mortise, and lateral radiographs of the left ankle at 2 months postoperatively. The lateral malleolar fracture was fixed with three 4.0-mm cannulated screws, and the AITFL fibular avulsion fracture was fixed with a 4.0-mm cannulated screw and a Kirschner wire.

(a–c) Anteroposterior, mortise, and lateral radiographs of the left ankle of a 70-year-old man with ankle dislocation and a medial malleolar fracture, high fibular fracture, and anterior inferior tibiofibular ligament (AITFL) tibial avulsion fracture. Diastasis was present in the distal tibiofibular syndesmosis. (d) Ankle three-dimensional computed tomography image showing the AITFL tibial avulsion fracture. (e–g) Anteroposterior, mortise, and lateral radiographs of the left ankle at 2 months postoperatively. The lateral malleolar fracture was fixed with a one-third tubular plate and screws, and the medial malleolar fracture was fixed with two 4.0-mm cannulated screws and a Kirschner wire. The AITFL tibial avulsion fracture was fixed with two 4.0-mm cannulated screws and a Kirschner wire. Because the distal tibiofibular syndesmosis was stable after fixation of the avulsed fragments, we did not insert any syndesmotic screws.
Radiographic and functional assessment
Radiographic parameters, such as the talocrural angle, medial clear space, and tibiofibular clear space, were measured using mortise images of both ankles at the time of injury and mortise images of the injured ankles at 6 weeks and 1 year after surgery using a picture archiving and communication system (INFINITT PACS; INFINITT Healthcare Co., Seoul, Korea). All radiographs were assessed by two of the authors, both of whom were orthopedic surgeons and were blinded to all other patient information. The interobserver reliability was assessed using the intraclass correlation coefficient. Among patients who underwent AITFL avulsion fracture fixation without syndesmotic screw fixation, we compared the radiographic parameters of the injured ankles at baseline and at 6 weeks and 1 year after surgery with those of the uninjured ankles using paired-sample t-tests. Functional results were assessed using the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot score at 1 year after surgery. All statistical analyses were performed using SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA).
Ethics statements
The Institutional Review Board of the Seoul National University Boramae Medical Center reviewed and approved this study (approval number 20130715/16-2013-102/081). Informed consent was obtained from all patients.
Results
Of 1,404 patients with surgically treated rotational ankle fractures during the study period, 81 patients (5.8%) had an AITFL avulsion fracture. Finally, after exclusion, 66 patients (34 men, 32 women) were eligible for the study. The average age at the time of surgery was 50.6 years (range, 18–72 years), and the median follow-up duration was 28.9 months. The causes of injury were as follows: slipping and falling down (76%), traffic accident (18%), sports injury (3%), and falling down (3%). According to the Lauge-Hansen classification, 50 (75.8%) patients were classified as having a supination-external rotation injury, 14 (21.2%) patients were classified as having a pronation-external rotation injury, and 2 (3%) patients were classified as having a pronation-abduction injury. According to the modified Wagstaffe classification suggested by Park et al., 39 30 (45.5%), 28 (42.4%), and 8 (12.1%) patients were classified as having type II, III, and IV injuries, respectively. Some patients had modified Wagstaffe type II, III, and IV injuries combined with Lauge-Hansen supination-external rotation injuries, whereas only patients with type III injuries also showed pronation-external rotation and pronation-abduction injuries (Table 1).
Number of patients who exhibited syndesmotic instability according to the Lauge-Hansen and modified Wagstaffe classification systems.

AITFL: anterior inferior tibiofibular ligament, ORIF: open reduction and internal fixation, SER: supination-external rotation, PER: pronation-external rotation, PAB: pronation-abduction.
Interobserver reliability for radiographic parameters.

Intraclass correlation coefficient is presented as median (range).
TCA: talocrural angle, MCS: medial clear space, TFCS: tibiofibular clear space.
Radiographic parameters.

Data are presented as mean ± standard deviation.
TCA: talocrural angle, MCS: medial clear space, TFCS: tibiofibular clear space.
Following the anatomical reduction and internal fixation of a displaced malleolar fracture, 54 (81.8%) of 66 patients showed syndesmotic instability by the hook test and underwent reduction and fixation of an AITFL avulsion fracture; these patients included 24 (80%) of 30 patients with a modified Wagstaffe type II injury, 24 (85.7%) of 28 patients with a type III injury, and 6 (75.0%) of 8 patients with a type IV injury. The intraoperative findings revealed no case of the intrasubstance rupture of the AITFL. After AITFL avulsion fracture fixation, 45 (83.3%) of 54 patients achieved syndesmotic stability with lateral translation of less than 2 mm by the hook test. Only 9 (16.7%) of 54 patients who showed residual syndesmotic instability even after AITFL avulsion fracture fixation needed additional syndesmotic screw fixation; these patients included 2 (9.1%) of 24 patients with a modified Wagstaffe type II injury, 6 (25.0%) of 24 patients with a type III injury, and 1 (12.5%) of 6 patients with a type IV injury (Table 1).
The intraclass correlation coefficients for the two examiners’ measurements of radiographic parameters ranged from 0.82 to 0.98 among 45 patients who underwent AITFL avulsion fracture fixation without syndesmotic screw fixation, (Table 2). Given the high interobserver reliability, the measurements of only one examiner were used in the analysis. The mean and standard deviation of the measured radiographic parameters were calculated (Table 3). The paired-sample t-tests showed significant differences in the talocrural angle, medial clear space, and tibiofibular clear space between the injured and contralateral uninjured ankles on initial radiographs ( p = 0.001, 0.001, and 0.007, respectively) (Figure 4). However, such differences were not observed on radiographs taken at 6 weeks or 1 year after surgery (Figures 5 and 6). The mean AOFAS score was 94 (range, 80–100) at 1 year after surgery. No patients developed complications, such as delayed union, nonunion, infection, wound problems, or neurovascular injury.

Preoperative radiographic parameters of the injured and contralateral uninjured ankles. Significant differences were found in the talocrural angle, medial clear space, and tibiofibular clear space (p = 0.001, 0.001, and 0.007, respectively).

Radiographic parameters at 6 weeks after surgery. There were no significant differences in any parameters between the injured and contralateral uninjured ankles.

Radiographic parameters at 1 year after surgery. There were no significant differences in any parameters between the injured and contralateral uninjured ankles.
The injuries were accompanied by medial malleolar fracture in 38 (57.6%) of 66 patients, while deltoid ligament injury without medial malleolar fracture was suspected in 10 patients (15.2%) with increased medial clear space on initial simple radiographs. Because all 10 patients showed recovery of the medial clear space under intraoperative fluoroscopy after malleolar fracture fixation and/or syndesmosis stabilization, none of them underwent deltoid ligament repair.
Discussion
This study was performed to analyze the radiographic and functional outcomes of anatomical reduction and fixation of AITFL avulsion fracture without syndesmotic screw fixation in rotational ankle fracture. The results of this study show that intraoperative syndesmotic instability could be improved after AITFL fracture reduction and fixation in more than 80% of patients with syndesmotic instability following ORIF for a malleolar fracture. Furthermore, those who had undergone ORIF for an AITFL avulsion fracture without syndesmotic screw fixation showed satisfactory postoperative radiographic and clinical outcomes.
Syndesmotic screw fixation is the most popular treatment option for ankle fracture combined with syndesmosis injury. However, there is still much debate regarding the number, diameter, position and cortical purchase of syndesmotic screws.10–18 Furthermore, several authors have described adverse effects of syndesmotic screw fixation such as iatrogenic malreduction of the syndesmosis.20,22,26,27 Gardner et al. 20 reported that more than half of patients who had undergone syndesmotic screw fixation showed incongruity on postoperative CT scans. Song et al. 27 recently reported that 36% of patients with syndesmotic screw fixation showed malreduction on postoperative CT scans. In addition, syndesmotic screw fixation can reportedly limit the normal biomechanics of the ankle joint, suggesting the necessity for screw removal.21,43,44 Manjoo et al. 21 compared the functional outcomes between patients with intact syndesmotic screws and those with broken, loose, or removed screws. They found that patients with intact syndesmotic screws had poorer functional outcomes, suggesting the necessity for the removal of intact syndesmotic screws. Kaftandziev et al. 45 also recently reported that patients with broken screws showed better clinical outcomes than those with intact screws. Moreover, one study showed that complications related to syndesmotic screw removal occurred in approximately 20% of patients who had undergone removal. 25 Alternative treatment methods have been attempted to avoid such complications of syndesmotic fixation. Peter et al. 30 reported that two oblique Kirchner wire fixation methods showed stabilization comparable to that of a single screw fixation method. Several authors have reported that bioabsorbable screw fixation is comparably effective for stabilizing syndesmosis.29,31,32 Suture button fixation has also been introduced with the theoretical advantage of allowing some degree of normal movement of the distal tibiofibular joint.33,34,46 Naqvi et al. 46 found no differences in the clinical outcomes of suture button fixation and syndesmotic screw fixation. Thornes et al. 33 reported that patients who underwent suture button fixation showed better clinical outcomes and earlier return to activity than those who underwent syndesmotic screw fixation. A recent randomized controlled trial revealed that patients with suture button fixation showed better clinical and radiographic outcomes at the 12-month follow-up. 35 Among patients with rotational ankle fracture accompanied by AITFL avulsion fracture and syndesmotic instability, as in our study, only a few studies have revealed good clinical outcomes after AITFL avulsion fracture reduction and fixation.38,39 Park et al. 39 presented 13 cases of AITFL avulsion fracture and reported the achievement of 9 excellent, 2 good, and 2 fair clinical results following AITFL avulsion fracture reduction and fixation. They indicated that anatomical reduction and rigid fixation of an AITFL avulsion fracture was advantageous in that direct bone-to-bone union can lead to improved physiological healing of the syndesmosis compared with other treatment strategies that aim to achieve indirect healing. Chung et al. 38 described 30 patients with AITFL avulsion fracture who achieved good clinical outcomes postoperatively. They reported that only 3 (10%) of 30 patients needed additional syndesmotic screw fixation after ORIF for the AITFL avulsion fracture. In the present study, syndesmotic stability was achieved following anatomical reduction and fixation of the avulsed fragments without syndesmotic screw fixation in more than 80% of patients with AITFL avulsion fracture and syndesmotic instability. Although further studies with a prospective design, control group, and large sample size are warranted, we speculate that reduction and fixation of AITFL avulsion fracture could be an alternative option for stabilizing the syndesmosis.
Regarding the diagnosis of syndesmotic instability in malleolar fractures, several authors have reported that standard radiographs were inadequate and therefore recommended a diagnostic intraoperative stress test following malleolar fracture fixation.40,47 Van Heest and Lafferty 40 emphasized that all operatively treated ankle fractures should be assessed by an intraoperative stress tests to detect any syndesmotic instability. Two intraoperative stress tests are commonly used: the hook test and the external rotation test. Lateral translational force is applied directly to the distal fibula in the hook test, whereas an external rotational force is applied to the distal fibula indirectly through the talus in the external rotation test. 40 Pakarinen et al. 42 reported high interobserver reliability and specificity for both tests. Stoffel et al. 4 found that application of lateral translational force in the hook test produced significantly greater diastasis than external rotational force in cadaveric models. In the present study, we assessed syndesmotic stability using the hook test and measured the translation under direct vision to detect any subtle syndesmotic instability; we diagnosed syndesmotic instability following ORIF for a malleolar fracture in 54 (81.8%) of 66 patients with AITFL avulsion fracture. Nelson 48 emphasized the advantage of intraoperative direct visualization for detecting syndesmotic instability.
Interestingly, in 20 (30.3%) of 66 patients with an AITFL avulsion fracture, the avulsion fracture was not detected by the initial simple radiographs but was only visualized by 3 D-CT (Figure 2). In a study by Pankovich, 49 AITFL avulsion fractures were only evident in four of eight patients with a Wagstaffe type II fracture by simple radiographs. Park et al. 39 suggested using the oblique view of 45-degree internal rotation to detect AITFL avulsion fractures. Haapamaki et al. 50 showed that the sensitivity of radiographs was only moderate to poor in patients with complex foot and ankle fractures and recommended multidetector CT as the primary imaging technique in such patients. We agree that 3 D-CT can be useful for detecting avulsion fractures and planning surgical treatments in patients with displaced ankle fractures.
Several limitations of this study should be noted. First and most importantly, there was no control group because of the retrospective study design. Although intraoperative recovery of syndesmotic stability was observed after anatomical reduction and fixation of the avulsed fracture in more than 80% of patients, we cannot be sure whether this treatment made a significant difference in the natural healing process of a syndesmotic injury without results for comparison. One previous study showed no differences in the functional and radiologic outcomes of accurately reduced and rigidly fixed supination-external rotation stage 4 ankle fractures with or without syndesmotic stabilization. 51 Moreover, we cannot conclude that AITFL avulsion fracture reduction and fixation is superior to syndesmotic screw fixation without a direct comparison of the two methods. Second, although the hook test showed high interobserver reliability and specificity in previous studies, we did not evaluate intraobserver and interobserver reliability in the intraoperative hook test in the present study. Therefore, intraoperative syndesmotic instability might have been defined rather subjectively. Moreover, the hook test alone has limitations in detecting syndesmotic instability. 42 Combining the hook test with stress examination under fluoroscopic control, which was not performed in this study, might reveal syndesmotic instability more accurately. Third, no data with which to directly assess syndesmotic stability during the postoperative follow-up period were available. Although we evaluated patients using static radiographic parameters and functional scores, more direct assessment through provocative physical examination or symptom surveillance might reveal the patients with residual syndesmotic instability. Fourth, deltoid ligament injury was indirectly suspected upon examination of simple radiographs only because no preoperative assessment of the deltoid ligament had been performed by ultrasound or magnetic resonance imaging, which is also crucial for ankle stability. Therefore, deltoid ligament injury might have been underestimated in this study. Furthermore, although 10 patients suspected to have deltoid ligament injury were treated without deltoid ligament repair in this study, we should not conclude that syndesmosis stabilization can obviate the need for deltoid ligament repair. Recent studies have suggested that detecting and repairing deltoid ligament injury produces better results in ankle fractures with syndesmotic instability.52,53 Finally, the number of patients included in this study was small, limiting the generalizability of the results. The small sample size also increases the difficulty of comparing the radiographic and clinical results according to the specific fracture type. Further studies with a prospective design, control group, and large sample are warranted to elucidate the optimal treatment of syndesmotic injury.
Conclusion
We stabilized the distal tibiofibular joint through anatomical reduction and fixation of AITFL avulsion fracture in more than 80% of patients with an AITFL avulsion fracture who showed syndesmotic instability following ORIF of malleolar fracture. If the stability of the distal tibiofibular joint can be improved by fixation of the avulsed fragments, the need for syndesmotic screw fixation might be obviated, thus preventing associated complications.