
Abstract
We present an overview of the wide range of potential applications of optical methods for monitoring traumatic brain injury. The MEDLINE database was electronically searched with the following search terms: “traumatic brain injury,” “head injury,” or “head trauma,” and “optical methods,” “NIRS,” “near-infrared spectroscopy,” “cerebral oxygenation,” or “cerebral oximetry.” Original reports concerning human subjects published from January 1980 to June 2015 in English were analyzed. Fifty-four studies met our inclusion criteria. Optical methods have been tested for detection of intracranial lesions, monitoring brain oxygenation, assessment of brain perfusion, and evaluation of cerebral autoregulation or intracellular metabolic processes in the brain. Some studies have also examined the applicability of optical methods during the recovery phase of traumatic brain injury . The limitations of currently available optical methods and promising directions of future development are described in this review. Considering the outstanding technical challenges, the limited number of patients studied, and the mixed results and opinions gathered from other reviews on this subject, we believe that optical methods must remain primarily research tools for the present. More studies are needed to gain confidence in the use of these techniques for neuromonitoring of traumatic brain injury patients.
Keywords
Introduction
Traumatic brain injury (TBI) is characterized by a diversity of pathophysiological changes occurring simultaneously following trauma. Secondary insult can lead to irreversible changes in the brain that result in permanent disability or death. Processes underlying the second phase of injury include intracranial bleeding, inadequate cerebral oxygenation, changes in cerebral blood flow (CBF) (hypo- and hyperperfusion), impairment of cerebrovascular autoregulation, and cerebral metabolic dysfunction. 1 Considering the complexity and dynamics of these changes, rapid diagnosis and vigilant neuromonitoring are mainstays of TBI management.
At present, only a few techniques are available for continuous bedside monitoring of brain tissue viability during the first hours and days after TBI. They aim at identifying potential episodes of neuronal hypoxia and cerebral ischemia. Intracranial pressure (ICP) is the most fundamental of these. 2 Together with mean arterial pressure (MAP), ICP provides a measurement of cerebral perfusion pressure (CPP) and a rough estimate of CBF. However, estimation of CBF from these variables is much dependent on the status of cerebral autoregulation. Therefore, the latest strategies are recommending the monitoring of cerebral autoregulation as part of neuromonitoring, which can, in turn, contribute to realizing the optimal CPP target for a given patient.3,4 Assessment of cerebral perfusion can be supplemented by invasive, local CBF measurements such as thermal diffusion flowmetry. More commonly, noninvasive transcranial Doppler (TCD) ultrasonography is used, which is able to identify hypo- and hyperperfusion in larger regions of the brain. 5 However, neither these direct perfusion techniques nor the previously mentioned ICP and CPP approaches directly answer questions of oxygen delivery and consumption, or of cerebral metabolic rate. To assess the adequacy of brain tissue oxygenation, two invasive methods are currently available: brain-tissue oxygen tension (PbtO2), and jugular venous-oxygen saturation (SjO2). It has been suggested that both methods can guide TBI therapy and even influence patient outcomes. 6
Cerebral metabolic rate can be assessed using cerebral microdialysis, which measures the concentrations of markers of energy metabolism directly in the brain. Monitoring these biomarkers during the course of treatment can help clinical management. 7
Although all the above-mentioned techniques can provide clear benefits, all carry some disadvantages; most of them are invasive, they are expensive, and they are not universally accessible.
Ideal neuromonitoring would be continuous, affordable, and noninvasive and could be readily applied at the bedside or in the field. Such neuromonitoring should also allow monitoring over multiple regions of interest simultaneously, particularly in conditions like TBI wherein there is substantial regional heterogeneity in pathophysiology. Optical methods that allow detection of intracranial bleeding, assessment of brain tissue oxygenation and cerebral perfusion, and evaluation of cerebral autoregulation or the intracellular metabolic state during this early post-traumatic period could potentially address these requirements and complement or even replace existing modalities. Furthermore, they can be applied not only in the acute phase of TBI, but also during neurorehabilitation.
Clinical data on the usefulness of optical techniques in patients with TBI are still limited with mixed results. We searched the MEDLINE database to review studies relevant to the application of optical methods in TBI patients. The following search terms were used: “traumatic brain injury” or “head injury” or “head trauma” and “optical methods” or “NIRS” or “near-infrared spectroscopy” or “cerebral oxygenation” or “cerebral oximetry.” Original reports published in English and concerning human studies from 1980 to June 2015 were analyzed (last search 30 June 2015). References were also made to the papers in PubMed. The following criteria were necessary for inclusion: (1) diagnosis included TBI and (2) optical method was used for neuromonitoring. We eliminated theoretical articles, animal studies, and conference proceedings. All reviews were analyzed to determine their relevance to our review. Of 195 studies, initial title selection and abstract screening using the above-mentioned inclusion and exclusion criteria yielded a total of 54 relevant studies: 12 on hematoma detection, 21 on brain oxygenation, 5 on cerebral perfusion, 6 on cerebral autoregulation, 3 on cerebral metabolism, and 7 on neurorehabilitation.
Physical and technical background
The optical methods used for neuromonitoring are based on emission of near-infrared light (NIR) at the surface of the head and detection of remitted light at a distance of a several centimeters. The emitted light undergoes two main processes: scattering and absorption. Scattering depends on the cellular structure of the tissue and leads to stochastic movement of photons in the medium, as described by diffusion theory. The strong scattering and good transparency of tissue layers of the head for NIR light result in sufficient reemission of photons back to the surface to allow for detection of photons that penetrated the brain cortex. 8 The absorption is mainly associated with the interaction of photons with chromophores in the tissue, including hemoglobin, water, lipids, and a variety of proteins (such as cytochrome c). 9
The most basic optical method is based on single-wavelength diffuse reflectance. The attenuation of light increases when an absorber (e.g., hematoma) is encountered between the source and detector (see Detection of intracranial hematoma section). The more advanced and frequently used technique is NIRS in which light attenuation is monitored at several (at least two) wavelengths. According to Lambert-Beer's law, changes in the attenuation of light due to absorption are directly proportional to the concentration of chromophores. The spectra of the hemoglobin and the cytochrome c oxidase (CCO) vary depending on their oxygenation and oxidation states, respectively. Thus, it is possible to obtain information about changes in the oxygenation-deoxygenation states of hemoglobin (ΔcHbO2 and ΔcHb) and the oxidation–reduction state of CCO.
The continuous wave (CW) NIRS technique is the most basic, inexpensive, and wildly used solution. However, because only the intensity of the remitted light is measured, the two optical properties (absorption and scattering coefficient) cannot be independently determined. CW measurement is very sensitive to changes in oxygenation of the extracerebral tissues. 9 Thus, the technique does not provide depth sensitivity because layers beneath the probe cannot be differentiated. To calculate changes in concentrations of hemoglobin, the pathlength of the photons penetrating through the tissue should be known. 10 Typically, this pathlength is estimated based on the source–detector separation used and so-called differential pathlength factor (DPF), which is obtained using the more sophisticated optical methods described below. However, this estimation is based on the assumption that the tissue under investigation can be modeled by semi-infinite homogeneous medium, which is far from reality. 9 With the latter assumption, it is also possible to estimate the absorption and scattering coefficient of the tissue using multiple source–detector separations (spatially resolved spectroscopy – SRS). Furthermore, this technique allows the derivation of absolute concentrations of Hb and HbO2, total hemoglobin concentration (cHbT = cHb + cHbO2), and regional cerebral tissue oxygen saturation (rSO2 = cHbO2/cHbT). 9 Most of the commonly available NIRS oximeters currently use SRS (technical differences between devices are discussed elsewhere10,11). The absolute values of optical coefficients can be also obtained using more advanced methods: frequency domain (FD) or time domain (TD). In FD technique, the light emitted into the tissue is intensity-modulated and the change in amplitude and change in phase of the waveform as the light propagates through the medium are measured. 12 In the TD technique (sometimes called time-resolved, tr-NIRS), ultrashort light pulses are emitted into the tissue. 13 These pulses are broadened and attenuated as they pass through the tissue and the shape of the distribution of times of flight of photons remitted from the tissue contains information about changes in absorption of the tissue at different depths.
Besides the TD technique, the methods of data acquisition described above were implemented for a variety of the commercially available instruments. The TD requires complex and expensive instrumentation and tends to be confined to optical laboratories; it has been validated only in few clinical studies. However, recent advancements in the development of this technique have led to the commercial availability of two TD instruments (TRS-20, Hamamatsu Ltd, Japan and PicoXea TCSPC Analyzer, Aurea Technologies, France).
Two major limitations of the NIRS measurements should be noted. The first is related to the difficulty in obtaining absolute values of concentrations of chromophores. The second is related to the influence of oxygenation of the extracerebral tissues on measured signals originating from the brain. The advanced data acquisition techniques and signal processing algorithms allow improved tissue oxygenation estimates and, to a certain degree, eliminate the influence of the scalp on the NIRS signal. The available techniques and physiologically useful variables that can be derived are summarized in Figure 1. Additional technical considerations related to specific application of optical methods are presented in the following sections.
NIRS data acquisition modes and obtained physiologically useful parameters.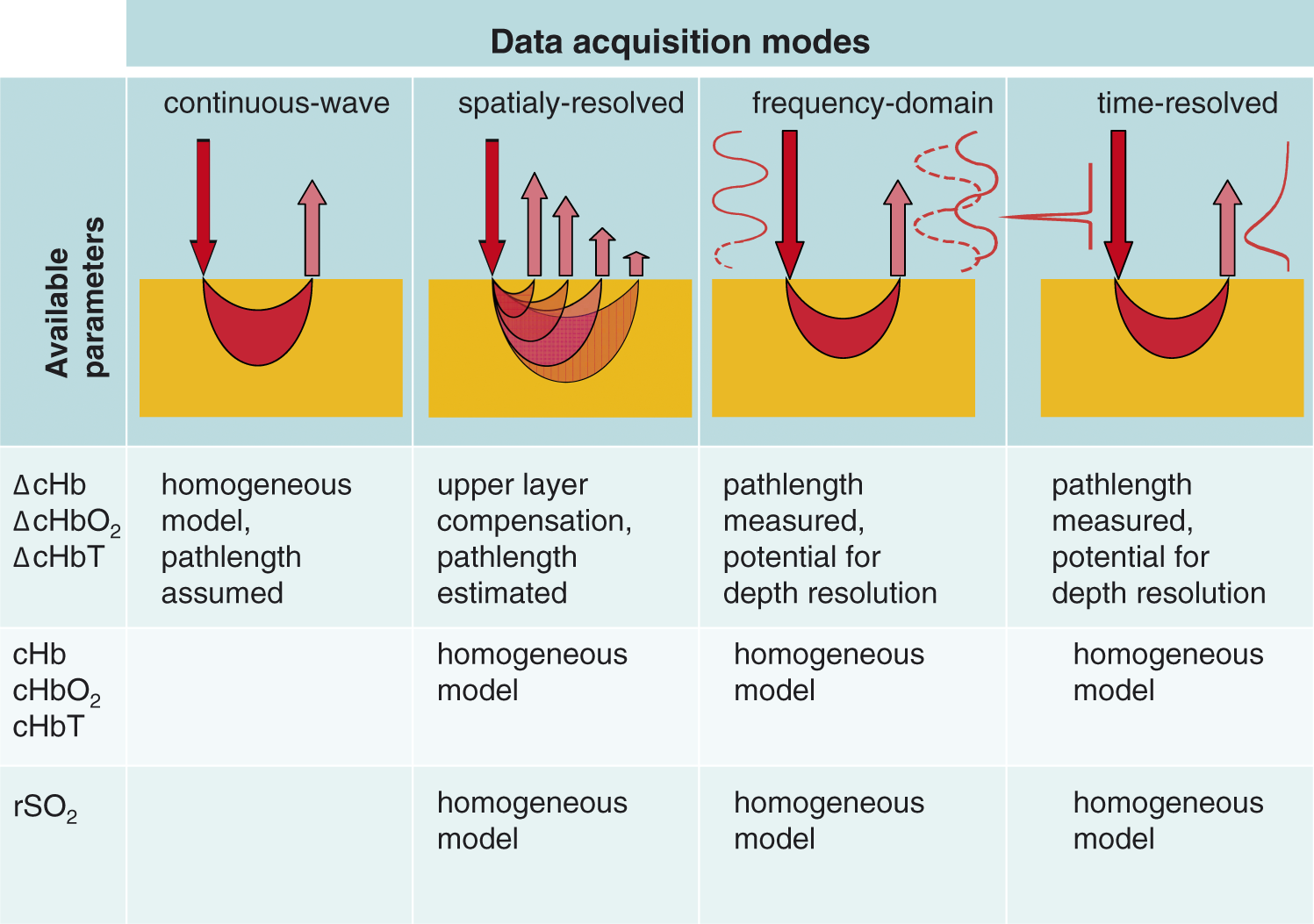
Another optical method being intensively developed for neuromonitoring is diffuse correlation spectroscopy (DCS). This technique offers a possibility of noninvasive assessment of CBF changes that is complementary to information from the NIRS modalities. In DCS, single-wavelength coherent light is introduced into the tissue. After multiple scattering events at the tissue particles, fluctuations in the light are observed by a single-photon detector placed at a distance of several centimeters from the source. In classic DCS, a single-mode optic fiber is mounted in an optode attached to the surface of the head, which delivers light that is diffusely reflected from the tissue to the photodetector. The temporal autocorrelation function of the fluctuations is analyzed in real time by electronic autocorrelators. Fast decays of the autocorrelation function are caused by higher particle velocities inside the medium, which are mainly red blood cells in the case of living tissue. Slow decays indicate low blood flow or absence of blood flow. 14 New generations of single-photon-sensitive semiconductors arranged in large arrays can advantageously be used for the DCS detectors. This enables observation of fluctuations of the optical signal from larger areas of tissue. 15 In recent clinical studies, both optical techniques, trNIRS and DCS, have been combined to monitor CBF and oxygenation of brain tissue simultaneously. This multimodal approach allows regional evaluation of the cerebral metabolism ratio of oxygen (CMRO2), which is a physiological parameter useful in the diagnosis of brain disorders. 16
Detection of intracranial hematoma
Detection of intracranial hematoma by NIRS is based on the assessment of optical density (OD), which is a measure of light absorption by the tissues. Extravasated blood exhibits high absorption, and a difference in OD between two symmetrical points on the head measured over hemispheres is highly specific for intracranial hematoma.17–19 OD differences are high in patients with extracerebral hematomas and are related to their size. 20 By contrast, these differences are not significant in cases of deep lesions, small hematomas, or bilateral abnormalities. 21 Unilateral abnormalities other than hematoma, such as contusion or infarction, can also be detected by side-to-side differences in OD, but with less reliability.20,21 These findings reveal one of the major drawbacks of all optical methods, namely a limited depth of intracranial light penetration, no greater than 2.5 cm for a typical interoptode separation of 3–5 cm. The depth of penetration can be increased by increasing the source-to-detector distance, but this requires higher energy light, which can increase the risk of thermal damage to the skin. 22 Attempts to maximize the interoptode distance to 9 cm have only been made in experimental settings. 23
Studies of near-infrared spectroscopy (NIRS) for detection of intracranial hematoma.

ΔOD: difference in optical density between left and right hemispheres.
Assessment of brain oxygenation
Regional cerebral tissue oxygen saturation (rSO2), derived by NIRS, is a complex variable that reflects the balance between the cerebral oxygen delivery and utilization. Not all the oxygen that reaches the brain is consumed; therefore, knowing the arterial and venous saturation of hemoglobin, as well as the blood flow, makes it possible to obtain the cerebral oxygen extraction fraction (OEF). Usually, low rSO2 is indicative of increased OEF due to decreased CBF (hypoperfusion), and high rSO2 is indicative of decreased OEF due to luxury perfusion. Based on this basic physiological information, Gersten et al. made an interesting calculation of what should be the value of cerebral rSO2 derived by NIRS. 31 With several assumptions, i.e., that arterial and venous oxygen saturations are 95% and 56%, respectively, and assuming a ratio of 25% vs. 75% of the arterial to venous contribution to the NIRS measurements (which is a common assumption based on PET studies), rSO2 should be approximately 66%. However, in vivo studies have been unable to determine reference ranges for rSO2 in healthy volunteers or ischemic thresholds in study patients. 32 Moreover, normal brain oxygenation values have been reported in the setting of confirmed cessation of CBF. 33 This could be explained because cerebral oximetry depends on two different processes: CBF and cerebral metabolism. In case of brain death, when there is a cessation of CBF, metabolism will also be decreased to zero. If there is a steal effect of blood from extracerebral tissues to the cortex, the venous compartment will be filled with oxygenated blood. Therefore, the NIRS values could be within normal range.
NIRS and other indices of cerebral oxygenation
Brain oxygenation studies.

CBF: cerebral blood flow; ΔcHb: changes in deoxy-hemoglobin concentration; ΔcHbO2: changes in oxy-hemoglobin concentration; ΔcHbT: changes in total hemoglobin concentration; CPP: cerebral perfusion pressure; CT: computed tomography; DCS: diffuse correlation spectroscopy; GCS: Glasgow coma scale; ICP: intracranial pressure; n.a.: not available; PbtO2: brain tissue oxygen tension; rSO2: regional cerebral tissue oxygen saturation; SjO2: jugular venous oxygen saturation; TCD: transcranial Doppler; XeCT: xenon-enhanced computed tomography.
NIRS and perfusion measurements
As mentioned above, rSO2 is related to both CBF and metabolism. Considering that metabolism is relatively constant (which is not always true in TBI), it could be assumed that rSO2 is a surrogate of CBF. Therefore, many studies have attempted to compare rSO2 with other perfusion indices (Table 2). One of the most frequently monitored parameters in TBI patients is CPP, which has shown good correlation with rSO2. Specifically, rSO2 values of >75% correlated well with CPP values of >70 mmHg, while rSO2 values of < 55% were associated with CPP values of <70 mmHg and were useful indicators of the need for invasive ICP monitoring. 47
By contrast, other authors noted that cerebral hypoxia was relatively common in cases where CPP was >70 mmHg. These observations suggest that CPP monitoring and cerebral oximetry provide slightly different data and that both can be important. 48 Several other trials explored NIRS data in comparison to CT perfusion measurements. Some found good correlations between these variables, 49 other have not confirmed these results.50,51
NIRS and ICP
As mentioned previously, monitoring of ICP remains the cornerstone of TBI management so far. Realizing the potential to extrapolate from NIRS variables to ICP would provide a valuable neuromonitoring tool for patients with intracranial hypertension. Since elevated ICP compromises CBF and cerebral oxygenation, NIRS variables could theoretically predict intracranial hypertension and thus become a noninvasive ICP monitor. Preliminary experiments carried out on an animal model of hydrocephalus showed that NIRS values were influenced by increased ICP.52,53 Studies on patients with shunted hydrocephalus also demonstrated the ability of NIRS to detect, as variations in the NIRS variables, perturbations such as removal of cerebrospinal fluid and decreasing ICP. 54
However, studies of other kinds of brain injuries have given conflicting results. Some reported no relationship between rSO2 and ICP and discouraged the use of rSO2 to predict ICP.55,56 Others were more promising and described reliable and fast reactions of the NIRS signal to ICP fluctuations. 37 However, no study has reported any plausible threshold of rSO2 that might indicate critically elevated ICP and that would have the potential to improve injury management. One report presented an interesting concept of such a measure based on observations in TBI patients that spontaneous fluctuations of Hb and HbO2 changed their pattern with an increase in ICP. 57
Another optical ICP assessment concept is based on phenomena of light transmission in layers of cerebrospinal fluid in which the layer acts as a waveguide. Changes in the thickness of this layer caused by elevated ICP may induce changes in the intensity of the detected light. 58 Unfortunately, this method has not been validated in systematic studies of TBI patients. Comparison between NIRS-related parameters and ICP in TBI was comprehensively discussed in recently published review of Davies et al. 59
These studies are promising, but the conclusions are sometimes contradictory. Furthermore, the validity of the monitoring values is unclear. A lack of standardizations among devices and not just different marketing names for the same variable makes comparisons difficult. Thus, the current recommendation is that trends over time, rather than absolute values, should be monitored. This adds certain clinical value, but it remains difficult to interpret, and the technology is still far from allowing direct cerebral oximetry-guided therapy. 6
Assessment of cerebral perfusion
Studies on brain perfusion in traumatic brain injury using exogenous contrast tracking or diffuse correlation spectroscopy (DCS).
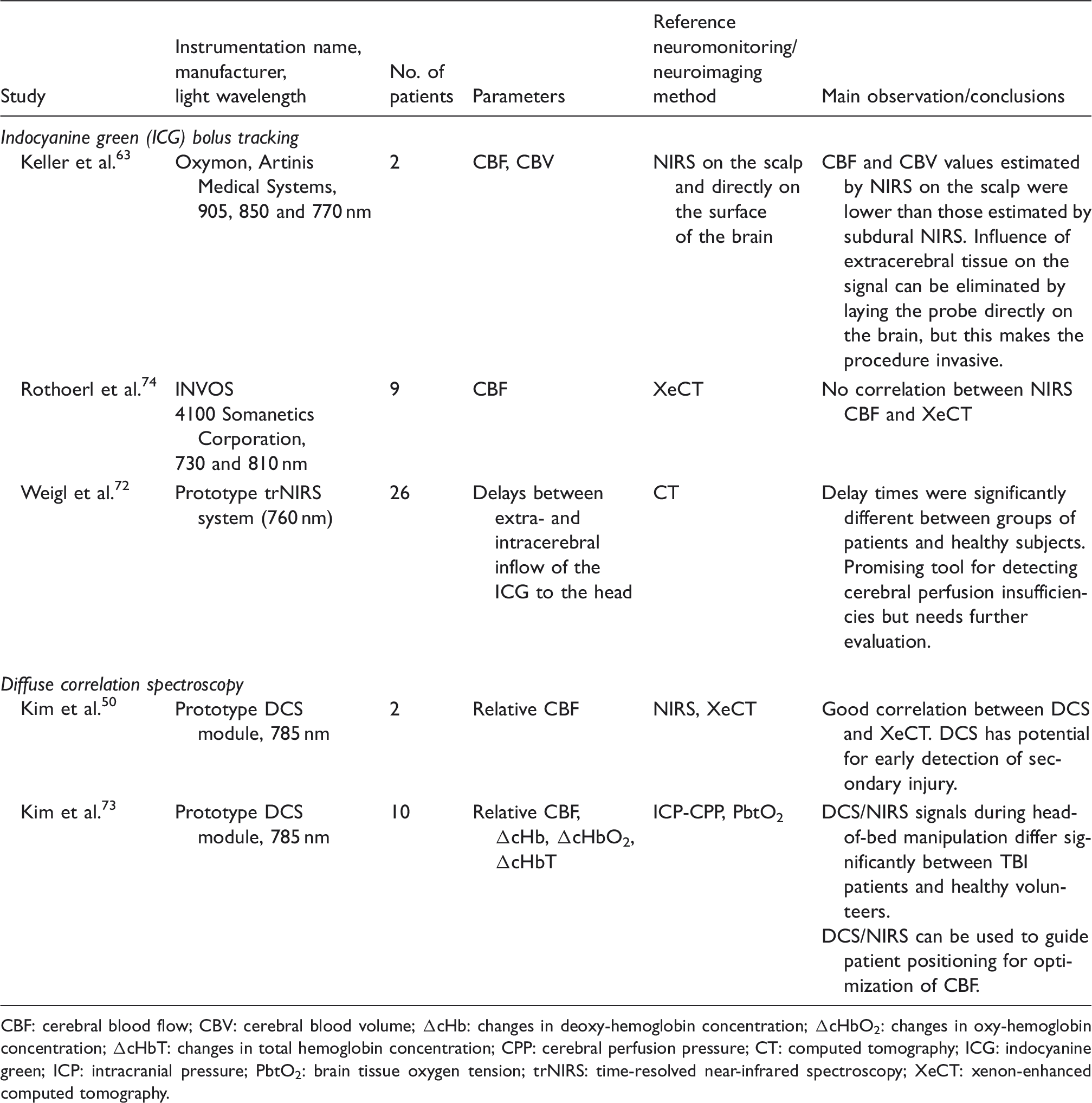
CBF: cerebral blood flow; CBV: cerebral blood volume; ΔcHb: changes in deoxy-hemoglobin concentration; ΔcHbO2: changes in oxy-hemoglobin concentration; ΔcHbT: changes in total hemoglobin concentration; CPP: cerebral perfusion pressure; CT: computed tomography; ICG: indocyanine green; ICP: intracranial pressure; PbtO2: brain tissue oxygen tension; trNIRS: time-resolved near-infrared spectroscopy; XeCT: xenon-enhanced computed tomography.
Concerns about neurotoxicity of the dye have been addressed in two studies. Both proved that the risk of neurotoxicity was minimal.63,64 An initial study of ICG-based cerebral perfusion analysis in a TBI patient tested an intracranial NIRS probe placed directly over the brain. 65 Although still invasive, the procedure introduced a new concept while excluding extracerebral contamination of the optical signal. The method was further developed into the use of combination intraparenchymal probes for simultaneous measurement of ICP, CBF, and oxygenation. 66
Another noninvasive approach that avoids signal contamination by extracerebral tissues is trNIRS (described in Physical and technical background section). This technique has been validated in a series of methodological experiments in diffuse reflectance geometry that have shown that the late photons have a higher probability of penetrating the cerebral cortex because their pathlength is known and longer then the pathlength of photons penetrating superficial tissues.67–69 A combination of trNIRS with ICG has recently been proposed 70 71 and was validated in a group of TBI patients who had localized cerebral hematoma and cerebral edema. 72 The concept of trNIRS/ICG is applied only in this TBI study, after assuming that temporal differences in inflow to the extracerebral tissues, serving as the arterial input function, and intracerebral tissues can reveal perfusion insufficiencies. Injured patients were statistically distinguished from healthy subjects, but no plausible thresholds were established.
The second method of assessment of cerebral perfusion is based on DCS, which is a technique for analyzing temporal fluctuations in the intensity of re-emitted NIR light depending on the intravascular movement of red blood cells. DCS measures relative CBF, i.e., variations in CBF with respect to a baseline. The method has been tested in neonates and in adult humans as well as in animal models, and it has been applied in neurocritical care patients after TBI.50,73 Relative changes in CBF were estimated by DCS during induced blood pressure changes and head-of-bed manipulation. The results were well correlated with XeCT and moderately correlated with CPP, but not with ICP. DCS seems to have great potential for implementation, as it combines information about CBF and rSO2 at the same time. New CBF-measuring approaches are also being introduced; one fuses light and ultrasound technologies. In this technique, one of the emitters sends ultrasound pulses into the tissue, changing locally optical properties and modulating (‘tagging’) the laser light traveling through the tissue at a certain depths. The first commercial device using this technique is now available (c-FLOW™, Ornim Medical, MA).
In conclusion, neither of the above-mentioned methods has yet been well validated against other reference methods in patients with TBI (with one exception of work of Rothoerl et al., 74 which showed poor correlation between NIRS and XeCT), and these studies remain purely experimental (Table 3).
Other applications of optical methods in TBI
Studies on cerebral autoregulation and cerebral metabolism.
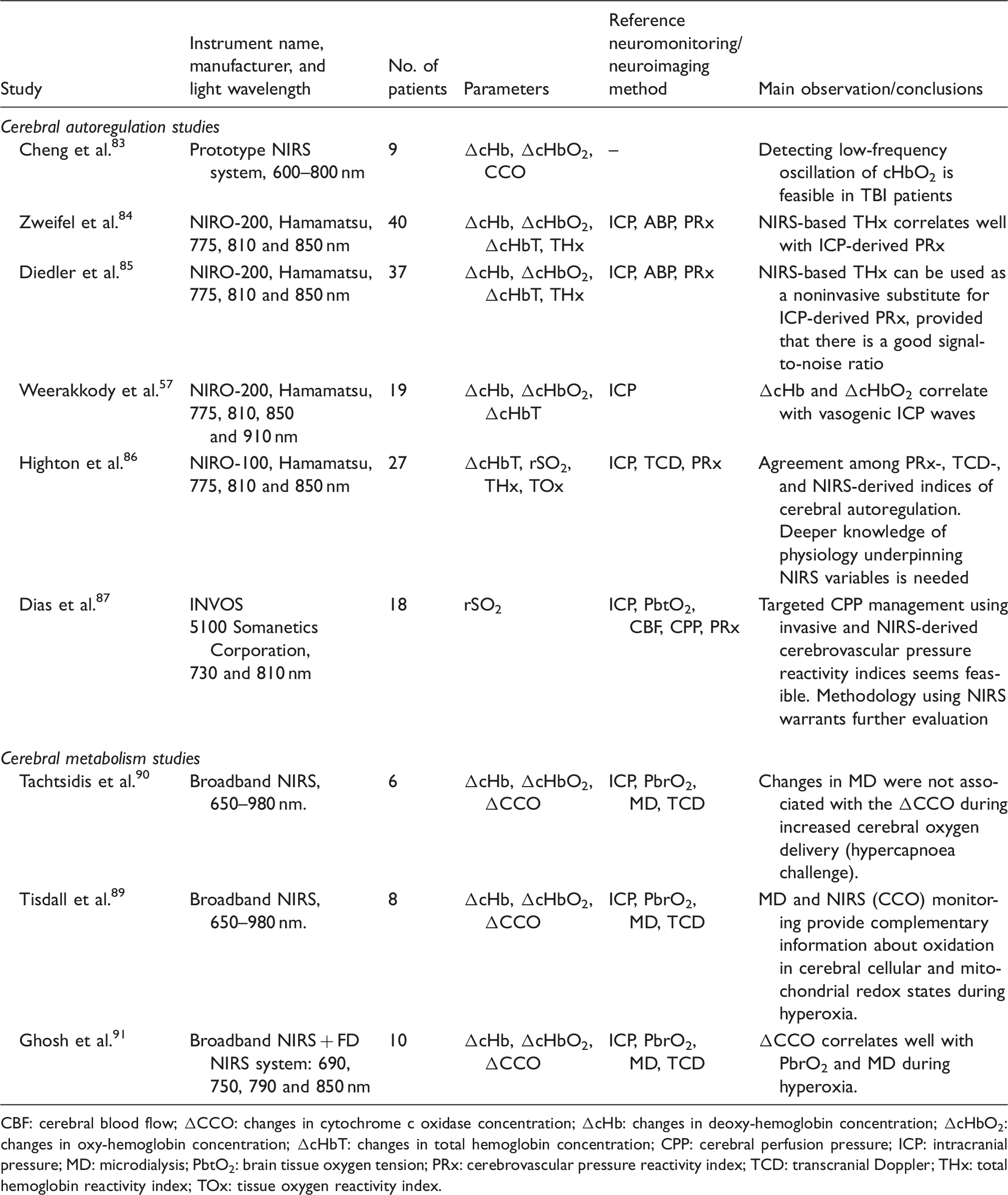
CBF: cerebral blood flow; ΔCCO: changes in cytochrome c oxidase concentration; ΔcHb: changes in deoxy-hemoglobin concentration; ΔcHbO2: changes in oxy-hemoglobin concentration; ΔcHbT: changes in total hemoglobin concentration; CPP: cerebral perfusion pressure; ICP: intracranial pressure; MD: microdialysis; PbtO2: brain tissue oxygen tension; PRx: cerebrovascular pressure reactivity index; TCD: transcranial Doppler; THx: total hemoglobin reactivity index; TOx: tissue oxygen reactivity index.
Studies on fNIRS in neurorehabilitation.
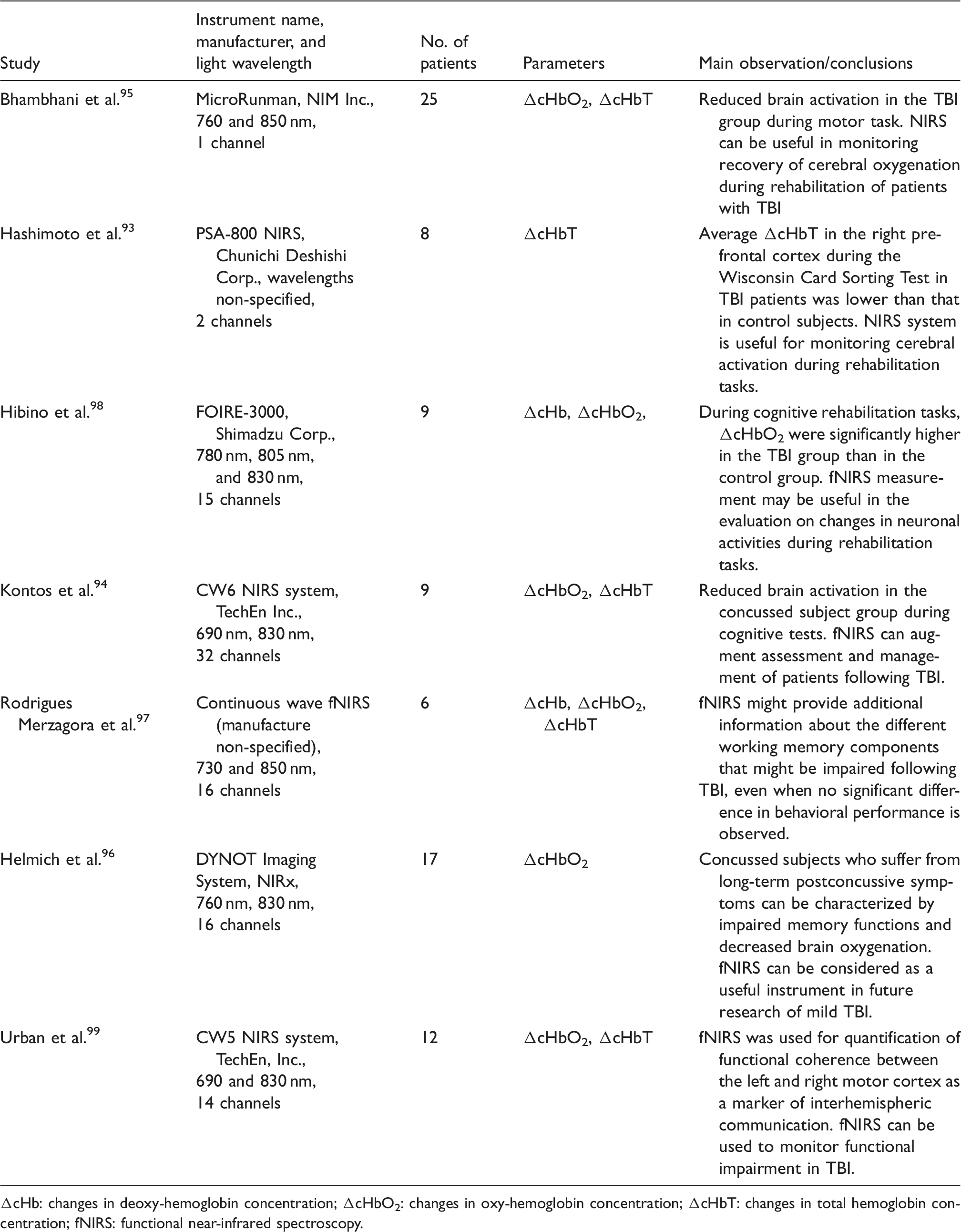
ΔcHb: changes in deoxy-hemoglobin concentration; ΔcHbO2: changes in oxy-hemoglobin concentration; ΔcHbT: changes in total hemoglobin concentration; fNIRS: functional near-infrared spectroscopy.
Cerebrovascular autoregulation
Cerebral autoregulation is the ability of the brain to maintain stable CBF while mean arterial blood pressure (MAP) or, more precisely, CPP, changes. A constant CBF during fluctuations in systemic blood pressure indicates that cerebral vasoreactivity is intact. MAP (or CPP) and CBF measurements must be available to assess cerebral autoregulation.
Initial methods included a hemodynamic stimulus, e.g., pharmacologic stimulation, to change MAP (testing methods). Although having excellent signal-to-noise ratio, they were limited to infrequent measurements and developed into continuous monitoring methods that can track rhythmic oscillations in arterial pressure. 75 A variety of algorithms has been applied to assessing the relationship between these spontaneous oscillations in the brain and MAP. They can be divided into analyses in the TD (using correlation methods) and in the FD (using transfer function analysis). 76 Time-domain methods estimate cerebral autoregulation by correlating slow MAP changes with changes in CBF, which are time-averaged to eliminate the influences of pulse and respiration. A positive correlation between MAP and CBF indicates impaired autoregulation, and no correlation indicates preserved autoregulation. Frequency-domain methods assume that cerebral circulation acts as a “high-pass filter,” freely passing high-frequency changes in MAP to CBF but attenuating low-frequency perturbations. 4 These spontaneous oscillations in the low-frequency spectrum (approximate frequency range 0.5 to 2/min, also called B-waves) are monitored by transfer function analysis to determine their relationships to oscillations in CBF, and low signal-to-noise ratio is compensated by averaging the signal over time. The properties of such acquired signals can be expressed by three frequency-dependent parameters of the transfer function, namely phase, gain, and coherence.
As can be seen from this short description, a multitude of cerebral autoregulation indices can be derived dependent on which algorithm (TD or FD) and which monitoring method (choice of input and output signals) is used for assessment of CBF. 77 An example of time-domain measurement of autoregulation based on TCD flow velocity is mean flow index (Mx). 78 Another measure, which takes advantage of ICP waveform as a surrogate for cerebral blood volume, is pressure reactivity index (PRx). For a detailed description of existing algorithms and of cerebral autoregulation indices derived from them, please see the review by Donnelly et al. 4 Some of these indices, such as Mx, are reported to be significantly related to patient outcomes following TBI. 79
Classically, ICP fluctuations, which serve as a surrogate for CBF fluctuations, have been used in assessment of cerebral autoregulation. 80 TCD ultrasound 81 and, more recently, NIRS, 82 have later supplemented invasive methods of assessing CBF. NIRS can be used for assessment of cerebral autoregulation in both the TD and FD and its advantages over TCD include fewer problems with probe fixation, lower risk of probe displacement due to patient movement, and the greater practicality of long-term monitoring. 78 Early trials in TBI patients have identified low frequency oscillations in the NIRS signal that are compatible with B-waves.57,83 This discovery has been applied to the assessment of cerebral autoregulation and new noninvasive indices: total hemoglobin reactivity (THx)84,85 and tissue oxygen reactivity (TOx) 86 have been added to existing indices. Recent studies confirm that these new noninvasive indices correlate well with PRx and Mx. 86
Moreover, initial verification of the feasibility of these methods in targeted individual autoregulation-guided treatment of TBI patients at the bedside has been reported and is based on the concept that optimal CPP should follow the best cerebrovascular pressure reactivity indices. 87
Cerebral metabolism
CCO is the terminal electron acceptor in the electron transport chain in mitochondria and is essential for the efficient generation of ATP. Redox state-dependent changes in this enzyme reflect oxygen utilization in the tissues and can be used as a marker of cellular oxygen metabolism. Cytochrome c has a broad spectral signature, and its concentration is 10 times lower than the concentration of hemoglobin. Thus, the detection of CCO by NIRS is an ambitious goal that requires a system capable of measurements at least at three wavelengths (to measure light attenuation for Hb, HbO2 and CCO). However, new advancements, used by UCL research groups for example, use a combination of SRS, FD method, and multiple wavelengths to improve CCO discrimination. 88 Physiologic changes in CCO after TBI have shown that an increase in cerebral oxygen delivery induced by hypercapnea or hyperoxia results in an increase in aerobic metabolism, leading to an increase in oxidized CCO.89–91 The interpretation of CCO-based parameters is difficult because of the complexity of the correlations between physiological changes and mitochondrial redox states. These issues remain poorly understood and have been described as “challenging aspects” in the application of CCO redox signals to patient monitoring. 92 To date, there are only a limited number of studies concerning this topic, and it is yet to be determined how this cellular metabolism parameter can contribute to the optimal management of TBI.
Neurorehabilitation
Local cerebral hemodynamic and oxygenation changes (assessed by changes in HbT and HbO2 respectively) following focal neuronal activation in the cerebral cortex can be reliably monitored with the use of functional NIRS (fNIRS). fNIRS has been tested as a tool for neuromonitoring of rehabilitation in patients with mild TBI.93–96 Frontal lobe function was monitored by fNIRS during cognitive tests or during motor stimulation. In both protocols, the stimuli were associated with significantly lower rates of change in cerebral oxygenation and blood volume in TBI patients compared to that in nondisabled subjects. By contrast, other studies have reported increased brain activity in concussed patients compared to that in controls during cognitive tests.97,98 These studies also indicated that different regions of the brain were activated in each group. Assuming that brain activation is an effective component of rehabilitation, the authors concluded that training tasks that increased regional cerebral oxygenation might be more beneficial for TBI patients. 98 Another potential application of fNIRS is in the diagnosis of impaired interhemispheric communication, which could be an objective biomarker of concussion injury. 99
NIRS and TBI in children
One of the most commonly raised concerns with optical methods is the potential for contamination of the signal by extracerebral tissues. This technical limitation seems to be less relevant to neonates and children, because they have thinner extracerebral layers. Such thin layers allow increased NIR light transmittance and decreased signal contamination. Thus, NIRS has been used for the detection of intracranial hematoma, motor stimulation, cerebral oximetry, and changes in ICP in children with TBI.19,30,95,100,101
Furthermore, a component of TBI can be found in premature and low-birth-weight infants that are at significant risk for intracerebral hemorrhage, as well as for cerebral ischemia and hypoxia due to a different pathophysiological pathway related to brain immaturity and birth trauma. Therefore, both NIRS-derived cerebral perfusion variables and NIRS-derived cerebral oxygenation variables have found application in neonates. Several studies have demonstrated that monitoring of optical CBF measures combined with monitoring of blood pressure can successfully identify neonates with impaired cerebral autoregulation and perfusion, which are known risk factors for the development of intracranial hemorrhage and poor outcomes.102,103 NIRS signals were also reported to reflect alterations in cerebral hemodynamics caused by removal of cerebrospinal fluid in former premature infants with post hemorrhagic hydrocephalus. 54 Some studies have shown that following birth asphyxia, changes in rSO2 in the first day of life associate with adverse neurologic outcomes. 104 Concerns raised by authors performing measurements in neonates include the wide range of initial “normal” values of rSO2, which leads to the recommendation of monitoring relative changes over time rather than absolute values.105,106 This recommendation, however, has been challenged based on the difficulty of ensuring fixation of the probes during long-term monitoring. 106
Discussion
Currently, there is increasing interest in the use of a variety of optical techniques in different medical fields. 107 These methods, including microscopic, endoscopic, and diffuse reflectance imaging, are capable of structural and functional imaging at tissue, cellular, and even molecular levels. However, those techniques based on visible wavelengths suffer from limited tissue penetration and in practice are often limited to easily accessible regions of the body or to surgically exposed tissues. In the neuroimaging and neuromonitoring field, workers have attempted to overcome these shortcomings by, for example, application of needle-like gradient index lenses to probe deep brain areas (microscopy methods) 108 or by application of neuroendoscopic techniques, which allow physicians to perform endoscope-assisted microsurgery. 109 Another promising direction for future research would be photoacoustic imaging. Preliminary animal experiments have shown that assessment of changes in CBF is possible by this technique. 110 However, at present, it is difficult to say how these techniques will contribute to the neuromonitoring of TBI patients. Practically, only those optical techniques based on monitoring diffusely reflected light and utilizing light at near-infrared wavelengths enable probing of deeper tissues and assessment of physiologically related variables in the human brain. Thus, these techniques become very attractive as research tools in neuroscience. 111 However, as can be seen from the present review, clinical application of optical techniques to TBI is rather infrequent due to the pathophysiologic complexity of clinical scenarios and the heavy demands for precision made on neuromonitoring techniques.112–114
The main strength of presented in this review optical techniques for evaluation of TBI is their noninvasiveness. Certain unsolved problems and well-known limitations of optical methods remain, and most of them are addressed in Physical and technical background section. Furthermore, there are additional challenges that are exclusive to TBI. The assumption of “normal” tissue optical properties under the probe in NIRS algorithms might not be valid for altered post-traumatic tissue composition, which is seen in a variety of clinical scenarios in TBI and includes intracranial pooling of extravascular blood, subdural air after craniotomy, and extracranial contusion. 43 In addition, cerebral edema decreases the thickness of the cerebrospinal fluid layer, and the effects of this process on the pathlength between the light source and the detector remain a topic of debate. 58
One reason for the inability to assess properly described methods in TBI is a limited number of studies that have predominantly observational design with a small number of patients and different instrumentation. The limitation of this review is the lack of comparison between studies using “old” versus “new” instrumentation. The methods are continuously evolving. New approaches (like SRS, additional wavelengths) have been introduced and become standard, as described in Physical and technical background section. These technologies provide more quantitative assessment of brain oxygenation and hemodynamics. However, the clinical significance of this new information in the context of TBI still needs to be determined. There is ongoing improvement in the modeling of propagation of light in tissue. Such model-based analysis could be advantageous in deciding which commercially available device is most fitting certain application. 59 However, these algorithms are not easily accessible or even unknown, and more studies comparing variables derived from them against other physiological parameters are needed.
Considering the technical challenges, the limited number of patients studied, and the mixed results and opinions gathered from other reviews on this subject, we believe that optical methods must remain primarily research tools for the moment. Further studies are needed before these techniques can be used with confidence in clinical settings. However, following dynamic development of these methods in the past and intensive ongoing research activity, we can hope that titles of the studies like “a mix of doubts and hope,” 114 or “a work in progress” 11 will slowly disappear, and optical neuromonitoring methods based on light will await their “brighter” future.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by the EC Seventh Framework Program under grant agreement no. 201076 – Project nEUROPt, “Non-invasive imaging of brain function and disease by pulsed near infrared light,” and by The National Science Centre in the frame of project 2011/03/D/ST7/02522.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors' contributions
WW conceived and designed the study as well as wrote the first draft and revised the final version. DM, DJ, SW, PS, MK, AG, RM, AL contributed to writing parts of the paper and to acquisition, analysis and interpretation of data for preparing tables. DJ performed the search for articles and drafted “Other applications of optical methods in TBI” section. AL revised “Physical and technical background” section and prepared ![]() . All authors revised and approved the final submission.
. All authors revised and approved the final submission.