
Abstract
To compare the effect of long-term mild hypothermia versus short-term mild hypothermia on the outcome of 215 severe traumatic brain injured patients with cerebral contusion and intracranial hypertension. At three medical centers, 215 patients aged 18 to 45 years old with an admission Glasgow Coma Scale ⩽ 8 within 4 h after injury were randomly divided into two groups: long-term mild hypothermia group (n = 108) for 5 ± 1.3 days mild hypothermia therapy and short-term mild hypothermia group (n = 107) for 2 ± 0.6 days mild hypothermia therapy. All patients had intracranial hypertension and frontotemporoparietal contusion with midline shift > 1 cm confirmed on computed tomographic scan. Glasgow Outcome Scale at 6-month follow-up, 47 cases had favorable outcome (43.5%), and other 61 cases had unfavorable outcome (56.5%) in the long-term mild hypothermia group. However, only 31 cases had favorable outcome (29.0%), and other 76 cases had unfavorable outcome (71.0%) in the short-term mild hypothermia group (P<0.05). The intracranial pressure significantly rebounded after rewarming in the short-term mild hypothermia group, but not in the long-term mild hypothermia (P<0.05). Furthermore, the incidence of stress ulcer, epilepsy, pulmonary infection, intracranial infection did not significantly differ between the two groups (P>0.05). Compared with short-term mild hypothermia, long-term mild hypothermia significantly improves the outcome of severe traumatic brain injured patients with cerebral contusion and intracranial hypertension without significant complications. Our data suggest that 5 days of long-term cooling is more efficacious than 2 days of short-term cooling when mild hypothermia is used to control refractory intracranial hypertension in patients with severe traumatic brain injury.
Introduction
Mild to moderate hypothermia as a treatment of brain injury has been a major area of research during the last decade. Laboratory studies have shown that mild to moderate hypothermia (32°C to 35°C) plays a significant protective effects, diminishes the degree of neural damage, reduces the mortality as well as improves neurologic outcome (Busto et al, 1987; Chopp et al., 1991; Clark et al, 1996; Clifton et al, 1991; Clifton, 1995; Dixon et al, 1998; Green et al, 1992; Jiang et al, 1991; Pomeranz, 1993; Welsh et al, 1990). It is believed that the beneficial effects of mild to moderate hypothermia act via metabolic and biochemical processes. Such mechanisms include temperature-dependent reduction of CMRO2, decrease of free radical production (Hagerdal, 1979; Hayashi et al, 1997; Vink et al, 1987), limitation of BBB disruption (Jiang et al, 1992; Smith and Hall, 1996) and brain edema (Shiozaki et al, 1993) attenuation of ionic disruption (Welsh et al, 1990), and decrease of excitatory amino-acid releases (Busto et al, 1989; Mitani and Kataoka, 1991b), reduction of cerebral lactate accumulation (Jiang et al, 2004), shunt of an increased fraction of glucose metabolism (Kaibara et al, 1999), inhibition of excessive calcium neuronal entry and intracellular calcium overload (Mitani and Kataoka, 1991a).
Since 1990s, more than 25 clinical studies have reported effects of therapeutic hypothermia on outcome of traumatic brain injury (TBI), as well as its secondary injury mechanisms and complications after TBI (Kochanek and Safar, 2003; McIntyre et al, 2003). McIntyre and co-workers report a systemic review of 12 trials of therapeutic hypothermia involving 1069 patients. The results show an overall beneficial effect of mild to moderate hypothermia in severe TBI, with a 19% relative reduction in the risk of death and a 22% relative reduction in the risk of poor neurologic outcome compared with normothermia (McIntyre et al, 2003). Furthermore, the finding of this systemic review also suggest that patients with severe TBI may benefit most from a longer duration of cooling, that is, more than 48 h. In fact, beneficial effects on secondary injury mechanisms may have occurred in patients treated with mild or moderate hypothermia for longer than 48 h, despite the established risks of complications from prolonged moderate hypothermia (Shann, 2003).
Clifton et al (2001) report that treatment with short-term mild hypothermia fails to show the beneficial effects on outcome after severe TBI in adults. However, several important limitations in that trail were later identified (Clifton et al, 2002a; Kochanek and Safar, 2003). For instance, although a cerebral perfusion pressure-targeted therapeutic protocol was used in the study, the means by which that therapeutic goal was achieved varied between centers and may have created an impossible challenge for the therapeutic hypothermia. Furthermore, the duration of mild hypothermia by Clifton et al is only 48 h, which may have been too short to control brain edema and intracranial hypertension, because cerebral swelling and brain edema are often greatest at 48 h after injury (Shann, 2003).
Until now, the duration of mild to moderate hypothermia, short-term (24 or 48 h) or long-term (5 days), for treatment of severe TBI patients has not been well explored. We have performed a randomized study to compare the effect of long-term mild hypothermia versus short-term mild hypothermia on outcome of 215 severe TBI patients with cerebral contusion and intracranial hypertension (Glasgow Coma Scale (GCS) ⩽ 8).
Materials and methods
Patients
From May 2000 through May 2003, 215 patients aged 18 to 45 years old with an admission GCS score of 8 or less within 4 h after injury were admitted to three hospitals and randomly divided into two groups: long-term (5 ± 1.3 days) mild hypothermia (n = 108) and short-term (2 ± 0.6 days) mild hypothermia (n = 107). The protocol and consent procedures were approved by the expert review board of each participating center.
The criteria for inclusion in the trial were age 18 to 45 years, a nonpenetrating head injury, a GCS score 3 to 8 after resuscitation, frontotemporoparietal contusion with midline shift > 1 cm on computed tomographic scan, and intracranial pressure (ICP) > 20 mm Hg. Patients were excluded if they had a score of 3 with un-reactive pupils and no spontaneous breathing, a life-threatening injury to an organ other than the brain, a systolic blood pressure of less than 90 mm Hg after resuscitation, oxygen saturation of less than 94% after resuscitation, pregnancy, or known preexisting medical conditions (e.g., severe heart disease), or if doctors were not able to initiate cooling within 4 h after injury.
Eligible patients were randomly assigned to long-term hypothermia or short-term hypothermia according to the day of the month, with patients assigned to long-term hypothermia on odd-numbered days.
Treatment Protocol
For all 215 patients with severe TBI, cooling began immediately after randomization and was continued during surgery (if required) using cooling blankets (Gaymar MTA-4702, USA) placed below and above the patients with extensive application of ice packs around the neck and limbs as we described before (Jiang et al, 2000). When patient's rectal temperature reached 33°C to 35°C, this temperature was maintained 5 ± 1.3 days for long-term mild hypothermia group, and 2 ± 0.6 days for short-term mild hypothermia group. Patients were continuously sedated and paralyzed with tracrium (10 mg to 40 mg/h) and chlorpromazine (5 to 10 mg/h) with infusion pump to prevent shivering during cooling and rewarming periods. All patients of both groups were passively rewarmed to 36.8°C ± 0.5°C at a rate no greater than 1°C per hour, by a gradual adjustment of the blanket thermostat (Jiang et al, 2000). All patients received the tracheotomy for ventilation (Aridyne 3600, USA) during treatment.
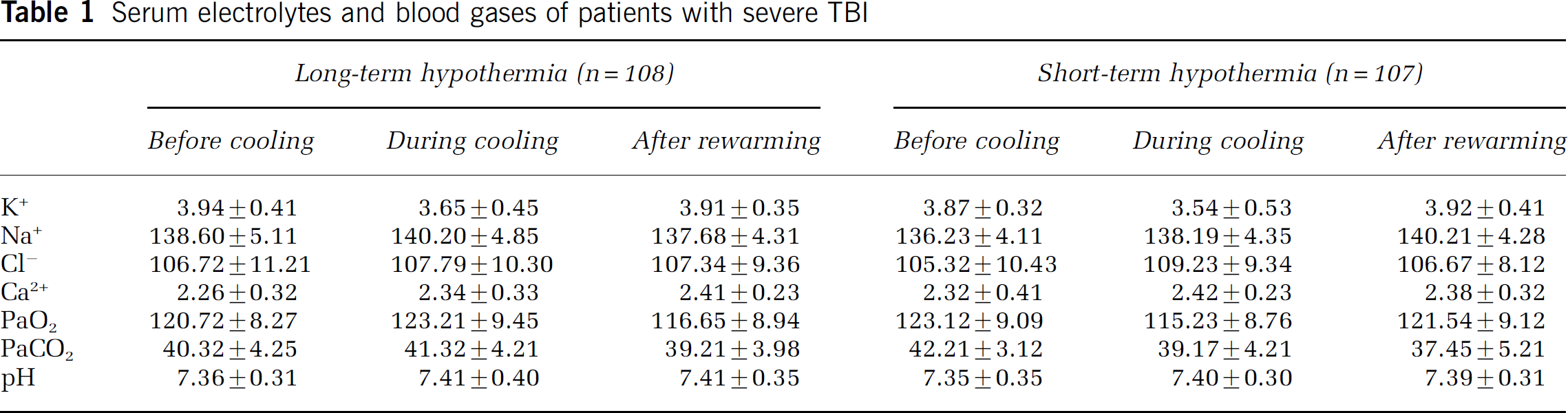
The patients were treated according to the principles described in ‘Guidelines for the management of severe head injury’ (Bullock et al, 2000). We rapidly evacuated large intracranial hematomas and hemorrhagic contusions. Intracranial pressure was monitored with fiberoptic catheter (Camino 3000, USA) in all patients. Increased intracranial pressure (> 20 mm Hg) was treated with bolus intravenous infusion of Mannitol (25 to 50 g every 6 to 8 h), albumin (10 to 20 g every 8 to 12 h) and flurosemide (20 to 40 mg every 6 to 8 h), as well as ventricular drainage. The cerebral perfusion pressure was maintained at a level higher than 70 mm Hg at all time by keeping the mean arterial pressure at a level between 90 and 110 mm Hg. Corticosteroids were not used in all patients. The patient's temperature, respiratory rate, heart rate, blood pressure, cardiac rhythm, oxygen saturation were continuously monitored (Hewlett-Packard, USA) in neurosurgical intensive care unit. Serum glucose, blood gases and serum electrolytes were regularly determined (Table 1).
Serum electrolytes and blood gases of patients with severe TBI
Vigilance with regard to respiratory care and monitoring for infection was in place related to the use of hypothermia. Nutritional support by either the enteral or the parenteral route was started 48 h after injury.
Assessment of Neurologic Outcome
A specialist in physical medicine and rehabilitation, who was unaware of the patients' treatment assignment, determined the neurologic outcome 6 months after the injury. The neurologic outcome was scored according to the five-category Glasgow Outcome Scale (Teasdale and Jennet, 1974) as follows: 1, death; 2, vegetative state–-unable to interact with the environment; 3, severe disability–-unable to live independently but able to follow commands; 4, moderate disability–-capable of living independently but unable to return to work or school; and 5, good recovery–-able to return to work or school. Good recovery and moderate disability were designated as favorable outcomes; severe disability, a vegetative state, and death were designated as unfavorable outcomes.
Statistical Analysis
The baseline characteristics, complications, blood glucose values, serum electrolytes and outcomes in the two groups were analyzed by two-sided χ2 tests or Fisher's exact tests. Comparisons for some simple continuous variables (e.g., ICP) were performed with two-sided t-tests. All data are expressed as means ± s.d. A P-value of < 0.05 was considered significant.
Results
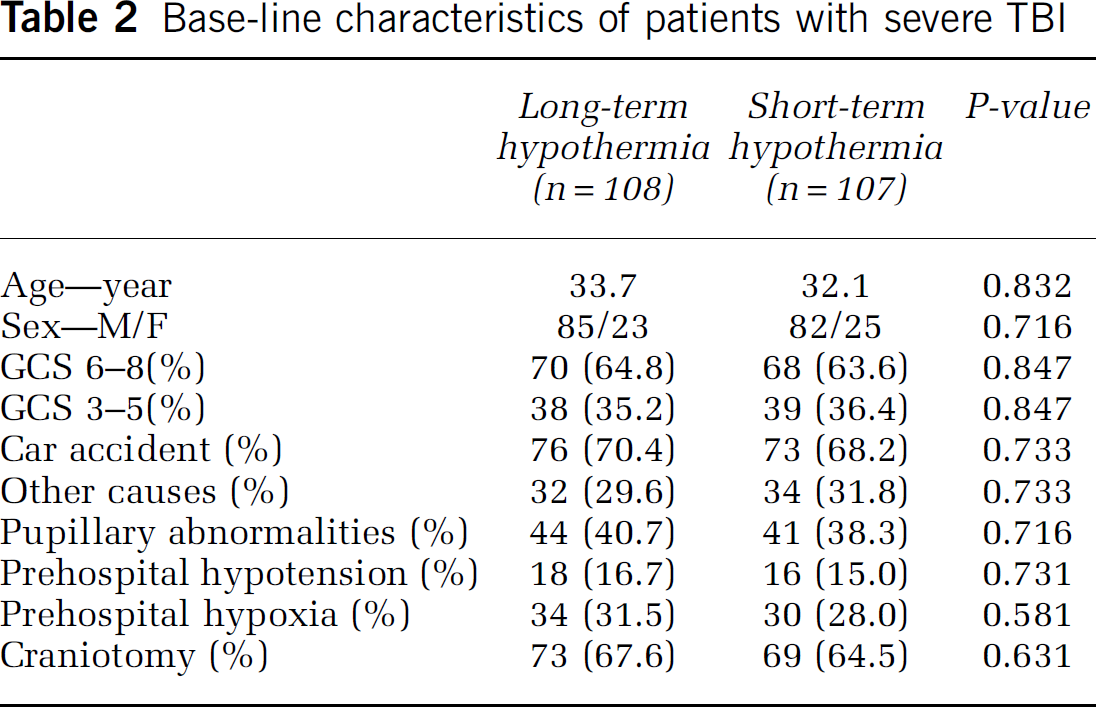
Patients did not significantly differ in terms of age, the initial Glasgow Coma Scale, intracranial hematoma, cerebral contusion, pupil abnormalities or craniotomy between the long- and short-term hypothermia group (P > 0.05) (Table 2).
Base-line characteristics of patients with severe TBI
Cooling began at 3.0 ± 0.2 h after injury for long-term hypothermia group and 3.1 ± 0.3 h after injury for short-term mild hypothermia, respectively (P > 0.05). Once the rectal temperature reached target temperature (33°C to 35°C), this temperature was maintained 5 ± 1.3 days in long-term mild hypothermia group, and 2 + 0.6 days in short-term mild hypothermia group, respectively. The rate of rewarming was not different between the two groups (P>0.05) (Figure 1).
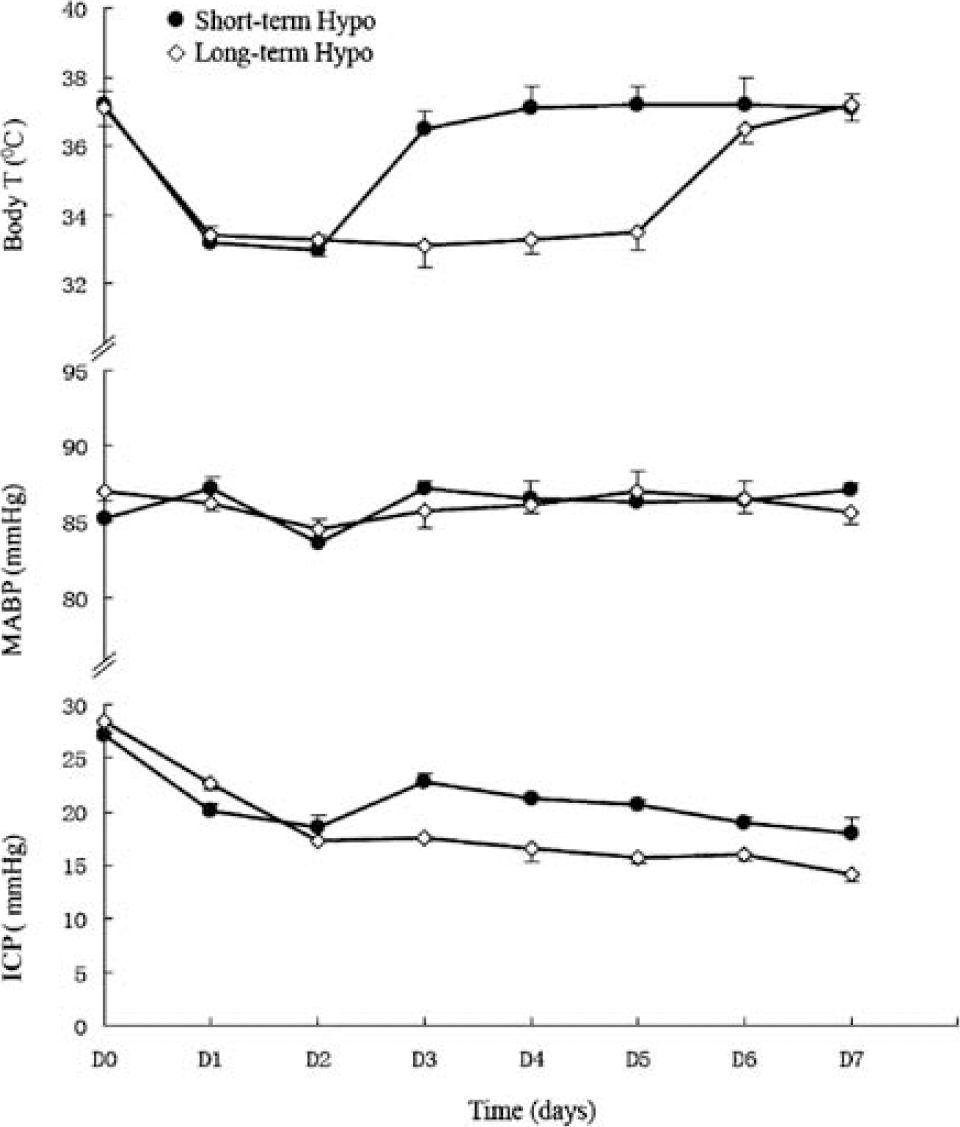
Physiological parameters in patients with severe traumatic brain injury. Mild hypothermia was kept for 5 ± 1.3 days in long-term mild hypothermia group, and only 2 ± 0.6 days in short-term mild hypothermia group. The ICP significantly rebounded after rewarming in short-term mild hypothermia group, which did not show in long-term mild hypothermia group (P < 0.05).
The ICP significantly rebounded after rewarming in short-term mild hypothermia group, and was significantly higher than that of the long-term mild hypothermia (P<0.05) (Figure 1).
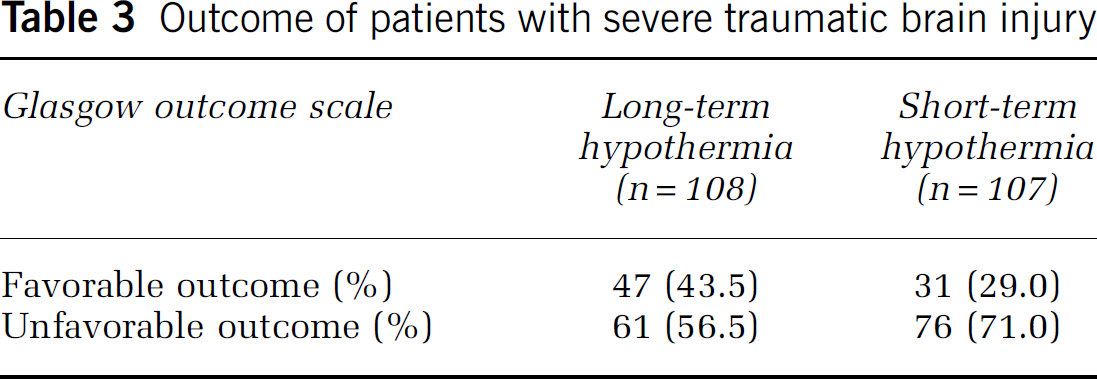
The Glasgow Outcome Scale at 6-month follow-up indicated that 47 cases had a favorable outcome (43.5%), and 61 cases had unfavorable outcome (56.5%) in the long-term mild hypothermia group. In contrast, only 31 cases had a favorable outcome (29.0%), and 76 cases had an unfavorable outcome (71.0%) in the short-term mild hypothermia group (P < 0.05) (Table 3).
Outcome of patients with severe traumatic brain injury
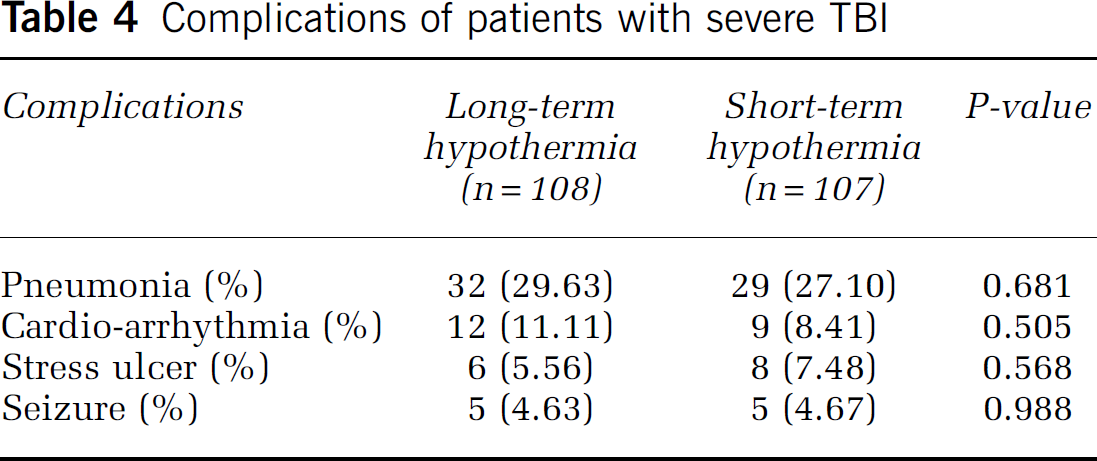
The incidence of stress ulcer, epilepsy, pulmonary infection, and cardio-arrhythmia was not significantly different between the two groups (P > 0.05) (Table 4).
Complications of patients with severe TBI
Discussion
We have found that long-term mild hypothermia significantly improves the outcome of severe TBI patients with cerebral contusion and intracranial hypertension without significant complications compared with short-term mild hypothermia. Our clinical data strongly suggest that 5 days of cooling is more efficacious than 2 days of cooling when mild hypothermia is used to control refractory intracranial hypertension in patients with severe TBI. Furthermore, early rewarming may not be optimal and can lead to both rebound intracranial hypertension and poor long-term outcome, when mild-to moderate hypothermia is used to control refractory intracranial hypertension in patients with severe TBI.
Mild to moderate hypothermia may be beneficial after cardiac arrest in human beings (Bernard et al, 2002; The Hypothermia after cardiac arrest group, 2002) and after TBI in laboratory animals (Safar and Kochanek, 2002). It is still controversial whether mild to moderate hypothermia improves the outcome of patients with severe TBI. Cochrane review of 12 trials with 812 participants found no evidence that hypothermia is beneficial after TBI in humans (Gadkary et al, 2003). However, in another recent systemic review of 12 trials with 1069 participants, McIntyre et al (2003) report that the relative risk of death with hypothermia was only 0.81 (95% CI 0.69 to 0.96), and that hypothermia for longer than 48 h the risk of death was only 0.7 (95% CI 0.56 to 0.87). These researchers add that many of the trials are likely to have underestimated the benefits of hypothermia because the participants were not cooled to low enough temperature or for long enough. Hypoxic-ischemic damage occurs in 90% patients who die from TBI, which suggests that such patients need to be cooled soon enough, cold enough, and long enough to minimize hypoxic-ischemic damage (Shann, 2003).
How soon is soon enough to be beneficial for brain injury? The previous studies have showed that hypothermia must be achieved within 2 to 6 h of severe hypoxic-ischemic injury in sheep, gerbils and rats to afford protection. For example, cooling sheep to 34°C for 72 h gave good protection if started 90 min after the injury, was partly effective if started at 5.5 h, and ineffective if started at 8.5 h (Gunn, 2000). Most clinical trails have suggested that the earlier that mild hypothermia is initiated, the more likely beneficial effects may be obtained. Clinical data further show that mild hypothermia within 6 h after injury may be effective (Shann, 2003). Hypothermia is currently being induced by surface cooling with use of cooling blankets, which usually requires 4 to 8 h to get the target hypothermia temperature (33°C to 35°C) (Clifton et al, 2001; Jiang et al, 2000; Schwab et al, 1998). Bernard et al (2003) recently reported that cooling can be achieved more rapidly (2°C over 30 mins) by intravenous administration of iced (4°C) crystalloid solution. This use of cold intravenous fluids may represent a logical strategy for future clinical trails for hypothermia in severe TBI.
What depth of cooling is necessary to be beneficial for brain injury? In severe hypoxic-ischemic injury, animal models suggest that the optimum temperature is between 32°C and 34°C. Clinical trial also shows that 33°C to 35°C, but not higher than 35°C, significantly improves the outcome of severe TBI patients (Clifton et al, 2002b). As body temperature decreases below 32°C, there is an increased risk of infection (Clifton et al, 2002b). Most clinical trials have suggested that 32°C to 35°C may be effective and not cause major complications (Clifton et al, 2002b; Shann, 2003).
How long of duration of hypothermia to be beneficial for brain injury? The optimum duration of hypothermia for hypoxic-ischemic injury depends on the severity of the injury and the delay before hypothermia is achieved. Within limits, a more severe injury or a longer delay can be compensated for by cooling longer. For example, when gerbils or rats are cooled to 32°C, 24 h of cooling is effective when started 1 h after injury, but not when started after 4 h; and cooling for 48 h or more has an effect when it begun 6 h after injury. Cooling for 72 h after a delay of 5.5 h partly protects sheep (Gunn, 2000). Because of the importance of raised ICP in patients with severe TBI, its use in TBI may importantly differ from hypothermic treatment for patients with cardiac arrest. European and Australia randomized prospective clinical trials have found that relatively brief period (24 to 48 h) of mild hypothermia significantly improve outcome (Bernard et al, 2002; Hypothermia after cardiac arrest group, 2002), yet short-term cooling was not effective in the randomized prospective clinical trial of hypothermia in adults with TBI by Clifton et al (2001), and was not as efficacious as more prolonged cooling in our current study in TBI. Why might prolonged cooling be needed in TBI to optimize outcome? Prior studies (Adelson et al, 2005) and our current work suggest that rebound intracranial hypertension often occurs with early but not late rewarming. This is unlikely to occur in cardiac arrest where intracranial hypertension is not thought to be an important factor in salvageable patients. Patients with severe TBI may benefit from being cooled for longer than patients with pure hypoxic-ischemic injury. Intracranial pressure often increases progressively and then remains high for several days following TBI. Mild to moderate hypothermia reliably reduces intracranial pressures, which suggests that it may be sensible to cool patients with severe TBI to 32°C to 35°C within 6 h of the injury for more than 48 h, and continue hypothermia at 32°C to 35°C if the ICP is higher than 20 mm Hg, of if it rises with gradual rewarming. Iida et al (2003) recently monitored the velocity of blood flow in the internal carotid arteries in 11 patients with severe head injury who were cooled within 6 h of injury to 32°C to 35°C for 48 to 72 h. Three of them had evidence of cerebral hyperemia followed by an increase in ICP during rewarming. The hyperemia resolved and ICP decreased when the patients were cooled again with mannitol, and barbiturates. More recently, Adelson et al (2005) have also found that rebound ICP elevations in hypothermia group compared with those in normothermia are noted for up to 10 to 12 h after rewarming if mild hypothermia only kept 24 or 48 h in 48 pediatric TBI patients . This clinical data have further showed that ICP markedly increased again during rewarming period in short-term hypothermia group, but not happened in long-term hypothermia group. This suggests that mild hypothermia should not be discontinued within 48 h after injury because cerebral swelling and brain edema is often greatest (Shann, 2003). In a summary of 12 clinical trials of hypothermia for treatment of severe TBI, McIntyre et al (2003) report that in nine of the studies when body temperature was allowed to rise after either 24 or 48 h (a time when cerebral swelling is often greatest) outcome of hypothermia is ineffective compared with normothermia group. However, in three of the studies when hypothermia was continued until ICP stabilized (3 to 14 days), it significantly reduces mortality and morbidity. Our present clinical study further supports the finding that long-term mild to moderate hypothermia is more efficacious than short-term mild to moderate hypothermia for severe TBI patients with intracranial hypertension. This indicates that early rewarming may not be optimal and can lead to both rebound intracranial hypertension and poor long-term outcome, when mild-to moderate hypothermia is used to control refractory intracranial hypertension in patients with severe TBI.
Finally, systemic long-term mild hypothermia with neuromuscular blockade and sedatives may predispose patients to an increased risk of pneumonia or other infections complications (Tateishi et al, 1998). Enhanced vigilance in respiratory care and monitoring for infection, along with appropriate antimicrobial and nutritional support are likely to represent essential adjuncts to the prolong use of mild hypothermia.
Footnotes
Acknowledgements
The authors thank Professor Bruce Lyeth at Department of Neurosurgery, University of California at Davis for his assistance of English.