
Abstract
Whereas postmortem ischemic damage is common in head injury, antemortem demonstration of ischemia has proven to be elusive. Although 15O positron emission tomography may be useful in this area, the technique has traditionally analyzed data within regions of interest (ROIs) to improve statistical accuracy. In head injury, such techniques are limited because of the lack of a priori knowledge regarding the location of ischemia, coexistence of hyperaemia, and difficulty in defining ischemic cerebral blood flow (CBF) and cerebral oxygen metabolism (CMRO2) levels. We report a novel method for defining disease pathophysiology following head injury. Voxel-based approaches are used to define the distribution of oxygen extraction fraction (OEF) across the entire brain; the standard deviation of this distribution provides a measure of the variability of OEF. These data are also used to integrate voxels above a threshold OEF value to produce an ROI based upon coherent physiology rather than spatial contiguity (the ischemic brain volume; IBV). However, such approaches may suffer from poor statistical accuracy, particularly in regions with low blood flow. The magnitude of these errors has been assessed in modeling experiments using the Hoffman brain phantom and modified control datasets. We conclude that this technique is a valid and useful tool for quantifying ischemic burden after traumatic brain injury.
Commonly quoted CBF and CMRO2 thresholds for neuronal survival based upon oxygen-15 positron emission tomography (15O PET) studies of experimental ischemia and clinical stroke (Heiss et al., 1992; Marchal et al., 1996; Powers et al., 1985) cannot be translated directly to head injury. A depressed level of consciousness, therapeutic sedation, and trauma-induced mitochondrial dysfunction (Verweij et al., 2000) can reduce metabolic rate (and hence coupled perfusion) in the injured brain and reduce critical CBF thresholds for ischemia (Bergsneider et al., 2000). Conversely, epileptiform activity, or hypermetabolism associated with excitotoxicity, may increase CMRO2 and make “normal” CBF levels inadequate. A clear definition of ischemia in situations where CMRO2 is altered depends upon the demonstration of compensatory increases in oxygen extraction fraction (OEF). Such data from patients with head injury in the PET literature are sparse and limited by methodologic difficulties (Diringer et al., 2000, 2002). Furthermore, even if such thresholds can be defined, their application to parametric PET images obtained in head injury may require methodologic adaptation. Ischemia in stroke usually conforms to topographical patterns, with identification of an ischemic core and penumbra (Baron, 1999). Whereas ischemia may be prominent in perilesional areas in head injury (Bouma et al., 1992; McLaughlin and Marion, 1996), significant ischemia may also be observed in structurally normal brain (Coles et al., 2002b). Consequently, a method is needed that can estimate the burden of critical hypoperfusion and ischemia across the entire brain, making no assumptions regarding its location. Such an approach requires definition of tissue with evidence of “misery perfusion” based upon individual voxel measurements and construction of a region of interest (ROI) based upon physiology rather than spatial contiguity. This voxel-based approach has clear methodologic pitfalls. It is highly dependent upon the statistical accuracy of the PET methods used and the underlying signal to noise characteristics of the PET data (Lammertsma et al., 1982). Such concerns are particularly relevant in disease states such as head injury where acute reductions in blood flow are likely. The reduction in emission counts within regions of the brain with low blood flow compromises the statistical accuracy of the technique.
The aim of this report is to quantify some of the methodologic problems of voxel-based summary measures of ischemia using 15O PET. We have used control and phantom data sets to explore the confidence with which differences in voxel-based measurements of ischemic burden can be ascribed to real physiologic changes in the presence of emission data of varying statistical quality.
METHODS
To illustrate the difficulties in the selection and interpretation of ROI based analyses and the benefits of a voxel-based approach in head injury, we present results from two patient data sets and a typical control. To assess the effect of a reduction in emission counts, and by inference statistical accuracy, upon voxel-based measurements of ischemia and critical hypoperfusion, we have used a range of different methods. First, we obtained tracer concentrations from clinical studies and used these figures as a basis for producing realistic phantom data sets. Second, control data sets were manipulated by varying the duration of emission acquisition to model a reduction in statistical accuracy. Third, data were collected from the Hoffman brain phantom (Hoffman et al., 1990) using the tracer concentrations obtained from clinical studies to produce clinically relevant phantom data sets. We varied tracer concentrations (and hence the signal to noise) in these experiments while keeping physiologic parameters (CBF, CMRO2, and OEF) unchanged. Data collected using these methods were used to assess the effect of a reduction in signal-to-noise upon voxel-based measurements of ischemia. Finally, we investigated the effect of changes in the small-to-large vessel hematocrit ratio (R), blood-brain partition coefficient for H2 15O (ρ), and signal-to-noise in C15O emission data using simulations.
Data acquisition
All PET studies were undertaken on a General Electric Advance scanner (GE Medical Systems, Milwaukee, U.S.A.).
Emission data were acquired in 3D mode during a 20-minute steady state infusion of 800 MBq of H2 15O (two 5-minute frames at the end of the administration), following a 60-second inhalation of 300 MBq of C15O (single 5 minute frame), and in 2D mode during a 20-minute steady state inhalation of 7200 MBq of 15O2 (two 5-minute frames at the end of the administration). Just before emission data acquisition, a 10-minute transmission scan was performed using rotating germanium, 68 rods (2 × 300 MBq). This data, in combination with that from a 60-minute blank scan acquired on the same day, was used to correct the emission data for photon attenuation.
Control data with reduced acquisition time
One way to assess the impact of a reduction in image statistics on voxel-based measurements of ischemia is to reduce emission counts in control data to simulate the effect of a reduction in CBF. The 10-minute emission data from H2 15O and 15O2 scans were acquired in at least two 5-minute frames in all subjects and in four 2.5-minute frames in six of the control subjects. We therefore recalculated the control data using 25% and 75% of the emission data (using one or three of the four 2.5-minute frames respectively) in the six control subjects for whom data was available in this format and using 50% of the emission data (using two of four 2.5-minute frames or one of two 5-minute frames) in all 10 controls. These reductions in acquisition time simulate the counts acquired within a 10-minute acquisition but with reduced tracer concentration (Ct). The effective reduction in Ct for 25%, 50%, and 75% of the emission data is related to CBF through the steady state equation (Frackowiak et al., 1980),
where Λ is the decay constant for 15O, and Ca is the arterial tracer concentration.
Consequently, these reductions in acquisition time result in images with statistical quality corresponding to a global CBF of 5.0, 11.7, and 21.5 mL·100g−1·min−1 respectively, compared with a baseline value in controls of 37 mL·100g−1·min−1. These analyses would therefore simulate the effect of a CBF of approximately 5, 10, and 20 mL·100g−1·min−1 without any change in physiology (Lammertsma et al., 1982).
Hoffman 18F phantom studies
Emission data were acquired sequentially in 2D and 3D modes as the radioactivity in the phantom decayed from an initial 150 MBq of 18F-fluoride. A series of 2 × 5-minute emission frames were obtained in each acquisition mode over a range of count rates that encompassed those from patient and control 15O2 and H2 15O scans. Emission data were corrected for photon attenuation using two combinations of transmission and blank scans: 10-minute transmission and 1-hour blank (as used for clinical data); 2-hour transmission and 2-hour blank (to minimize any noise propagation from the attenuation correction).
Image reconstruction and kinetic modeling
Images were reconstructed into 2.34 × 2.34 × 4.25 mm voxels using the PROMIS 3D filtered back projection algorithm (Kinahan and Rogers, 1989), with corrections applied for attenuation, scatter, randoms, and dead time. During reconstruction, a Hanning filter cutoff at the Nyquist frequency was used transaxially, but no apodisation was applied axially. Emission images were then smoothed using an isotropic 4 mm Gaussian filter. Parametric maps of CBF, CBV, CMRO2, and OEF were calculated by inputting PET emission and arterial tracer activity measurements into standard models (Frackowiak et al., 1980; Lammertsma et al., 1987) implemented in custom designed software (PETAN) (Smielewski et al., 2003). We used a blood-brain partition coefficient for H2 15O (ρ) of 0.95 based upon previous in vitro data (Herscovitch and Raichle, 1985) and a small-to-large vessel hematocrit ratio (R) of 0.85 (Phelps et al., 1979). Parametric maps were coregistered to anatomy using magnetic resonance (MR) imaging in phantom and control studies and x-ray computed tomography (CT) in patients.
Generation of parametric maps from Hoffman phantom data.
To generate images that mimicked the heterogeneous pattern of OEF within the injured brain, we constructed an ROI map (Fig 1) consisting of five ROIs with differing physiology. These ROIs were irregular in shape and spatial distribution so as to mimic the spatially heterogeneous pattern of pathophysiology observed in patients (Coles et al., 2002b). We defined the physiology in these ROIs as follows: first, we rearranged Equation 1
to select 3D phantom data (which simulated H2 15O scans) with average Ct values corresponding to a range of clinically relevant CBF values. The CBF values chosen (28, 31, 34, 38, and 43 mL·100g−1·min−1) ranged around the mean CBF obtained in patients (34 mL·100g−1·min−1). Each CBF value was attributed to one of the regions in the ROI map. To vary the image statistics within a clinically relevant range, Ct values in each region were calculated for six different arterial tracer activity inputs (Ca). The Ca values used were those observed in the average patient (AP), worst patient (WP), and best patient (BP), and the average control (AC), worst control (WC), and best control (BC).
Next, for each CBF and Ca value, once the required Ct for the ROI was determined, we calculated the tissue tracer concentration required in the 2D phantom data (which simulated the 15O2 scans) to achieve a range of OEF values using the standard equation for OEF (Frackowiak et al., 1980). The 2D emission frames chosen for each region were selected to maintain unchanged CMRO2 and result in OEF values of 60, 55, 50, 45, and 40% within the respective ROIs (Fig. 1).
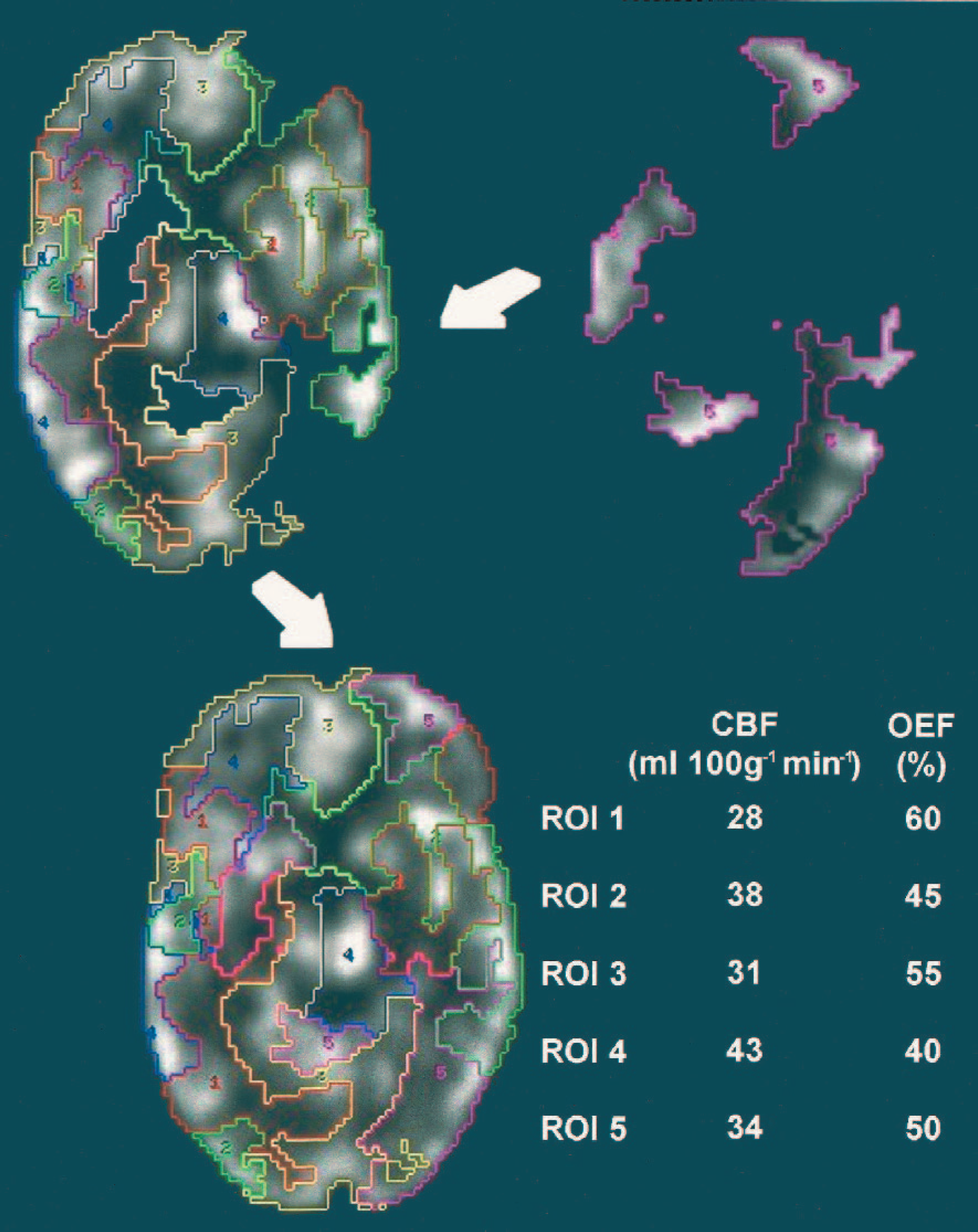
Construction of parametric maps for the phantom data sets. These ROI were designed to cover the whole brain and include mixed regions of grey and white matter and cerebrospinal fluid. For each of the clinical scenarios and reference data sets, the composite emission images for H2 15O and 15O2 were created using regions selected from appropriate 3D and 2D emission frames respectively. Each data set was processed to produce CBF, CMRO2, and OEF maps with identical physiology but varying statistical accuracy. ROI, regions of interest; OEF, oxygen extraction fraction.
As the phantom data did not have tracer concentrations that exactly matched those calculated from the CBF and OEF equations, the 3D and 2D data selected for the regions were scaled (average correction 6 ± 3%). This ensured that the regional and global CBF, CMRO2, and OEF were unchanged, with global values comparable with those obtained in a typical patient (CBF 34 mL·100g−1·min−1, CMRO2 2.4 mL·100g−1·min−1, and OEF 50%). Whereas the regional and global physiology in each of these composite data sets was identical, the varying tissue tracer concentrations resulted in varying image statistics.
We defined two additional data sets as points of reference at the two ends of the spectrum of statistical accuracy. These were well outside the range of data sets that we obtained in clinical practice. First, the emission frames with the lowest counts were used to represent the worst 15O2 and H2 15O emission frames. Second, for both 2D and 3D acquisitions, a weighted sum was made from all the frames, which was reconstructed using the 2-hour transmission and blank scans to generate emission frames with the optimal signal-to-noise ratio characteristics. These two were labeled the worst reference (WR) and best reference (BR) data sets, respectively. For the worst and best image data sets, arterial tracer activity measurements equivalent to those for the average patient were used, and the five regions were scaled appropriately to maintain CBF, CMRO2, and OEF. Thus all eight data sets represented images of the same virtual physiology (with identical values of CBF, CMRO2, and OEF) but varied in statistical accuracy from extremely poor (WR) to optimal (BR) through the various clinical scenarios modeled (AP, WP, BP, AC, WC, and BC) (Fig. 1).
Image analysis
where CaO2 is arterial oxygen content calculated as (1.34 ϗ Hb ϗ (SaO2/100)) + (0.003 ϗ PaO2), Hb = hemoglobin in g/100 mL, SaO2 = arterial oxygen saturation (%). Application of these thresholds to OEF images allowed us to calculate the volume of voxels with CvO2 values below this threshold and hence allowed estimation of the ischemic brain volume (IBV) (Fig. 2).
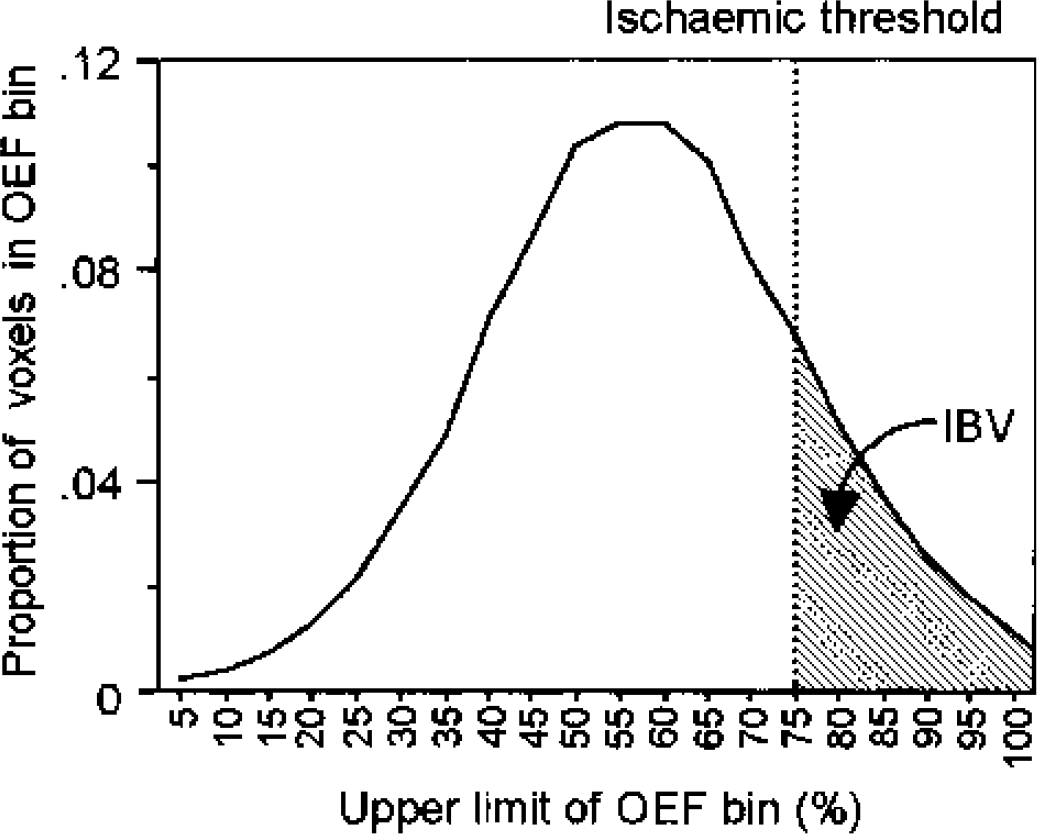
Calculation of the ischemic brain volume. OEF histogram from a single patient, showing the distribution of the number of voxels in each OEF bin. Critical OEF thresholds are derived by calculation of the OEF value above which cerebral venous oxygen content (CvO2) would be less than 3.5 mL/100 mL. The summed volume of voxels with OEF values above this threshold is the IBV. OEF, oxygen extraction fraction; IBV, ischemic brain volume.
Perfusion-utilization matching. OEF values should be closely clustered in normal subjects, suggesting efficient matching of CBF to CMRO2, with a resulting narrow spread of OEF values (Lebrun-Grandie et al., 1983). We assessed the matching of oxygen supply to demand by inspection of the OEF histograms and measurement of the standard deviation of the distribution.
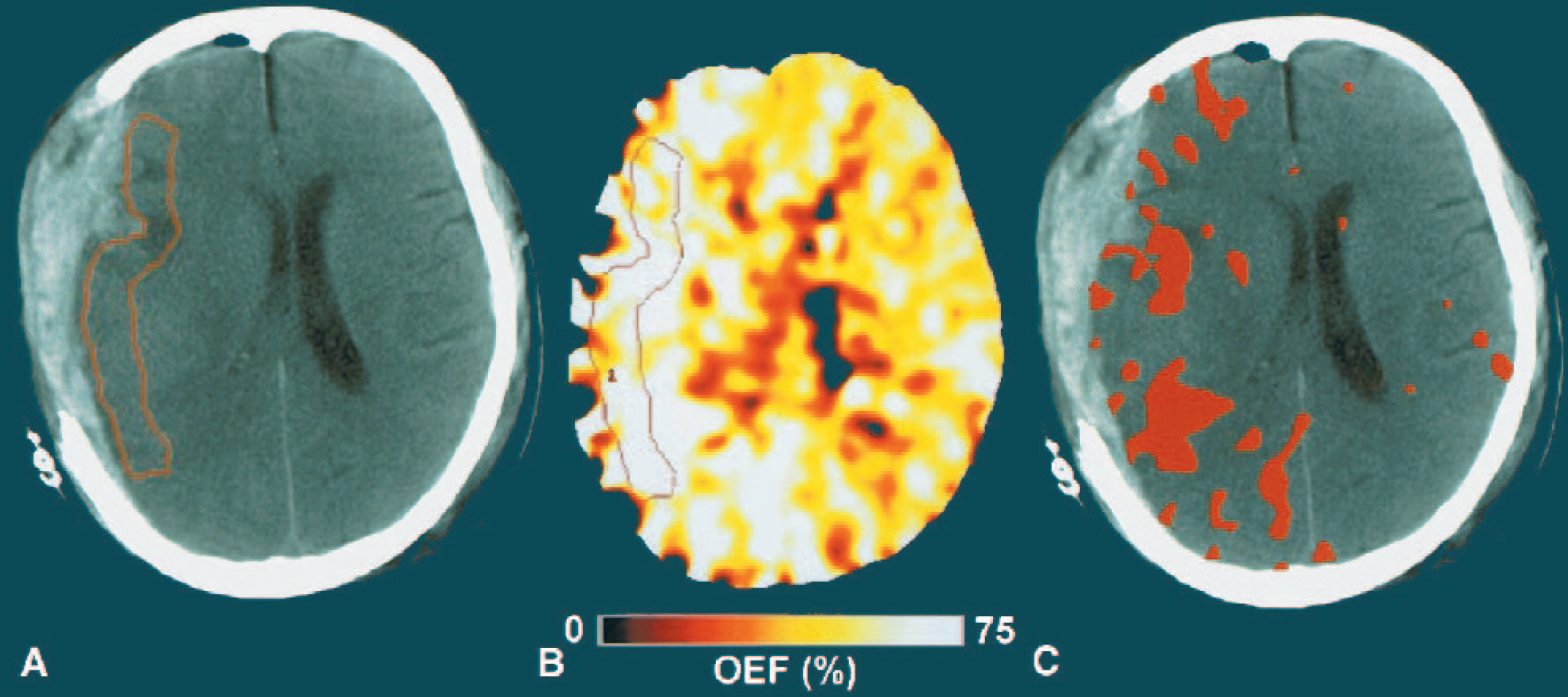
ROI and voxel-based analysis of a patient within 24 hours of head injury. (A) x-ray CT obtained from a 42-year-old woman 16 hours after injury following evacuation of a subdural hematoma. Note the small amount of residual subdural blood with minimal midline shift. A perilesional ROI has been drawn on the entire volume of cerebral tissue within 15 to 20 mm of the subdural hematoma. A single slice is shown here for simplicity. (B) OEF PET image. Note the marked increases in OEF in large portions of the cerebral hemisphere underlying the evacuated subdural hematoma. (C) x-ray CT with those voxels with OEF > 75% (based on a calculated CvO2 < 3.5 mL/100 mL) shown in red. The full extent of the physiologic lesion is greater than can be immediately defined by examination of the structural CT image alone. CT, computed tomography; ROI, regions of interest; OEF, oxygen extraction fraction; PET, positron emission tomography.
Phantom data. To examine the effect of emission data signal-to-noise characteristics on the IBV and SD of the OEF histograms the phantom data modeling the different clinical scenarios and reference phantom data sets were compared.
To model the effect of variation in the value for ρ upon OEF and voxel-based measures of ischemia, we used the arterial tracer concentration of the average patient within 24 hours of head injury and variable tissue tracer concentrations to construct data with a range of OEF values (20%, 40%, 60%, and 80%). In these simulations, the CMRO2 and CBV remained constant and comparable to the typical values obtained in a patient (2.4 and 4.2 mL·100g−1·min−1, respectively), and changes in OEF were achieved by varying CBF from a baseline value of 34 mL·100g−1·min−1. In each case the effect of a change in the value of ρ upon the calculated OEF was assessed.
Statistical analysis
Statistical analysis was undertaken using Statview (Version 5, 1998, SAS Institute Inc., Cary, NC, U.S.A.). All data are expressed and displayed as mean ± SD unless otherwise stated. Voxel-based PET data from the modified control data were compared using two-tailed paired t-tests. P values of < 0.05 were considered significant.
RESULTS
ROI and voxel-based analyses in illustrative clinical data sets
In Fig. 3, the results of a perilesional ROI based upon structural imaging are compared with that of a voxel-based analysis technique. Although the ROI data are suggestive of compromised tissue (CBF 15 mL·100g−1·min−1, CBV 3.3 mL·100g−1, CMRO2 1.6 mL·100g−1·min−1, and OEF 65%), they are not conclusive. In fact, the ROI fails to capture the entire physiologic injury, whereas the voxel-based technique generated from those voxels with a calculated CvO2 of < 3.5 mL/100 mL suggests that large portions of the cortex ipsilateral to the lesion are at risk of ischemic damage and neuronal loss, with a calculated IBV of 92 mL. In comparison with a typical control data set, the OEF histogram from this patient is broader and shifted to the right with a standard deviation of 25.7% versus 9.3% (Fig. 4A). In Fig. 4B, the OEF distribution of a second patient data set shows greater variability with regions of both high OEF suggestive of ischemia and low OEF suggestive of hyperemia or neuronal dysfunction (SD 17.6%). This suggests a more generalized impaired coupling of flow and metabolism, rather than classical regional ischemia.
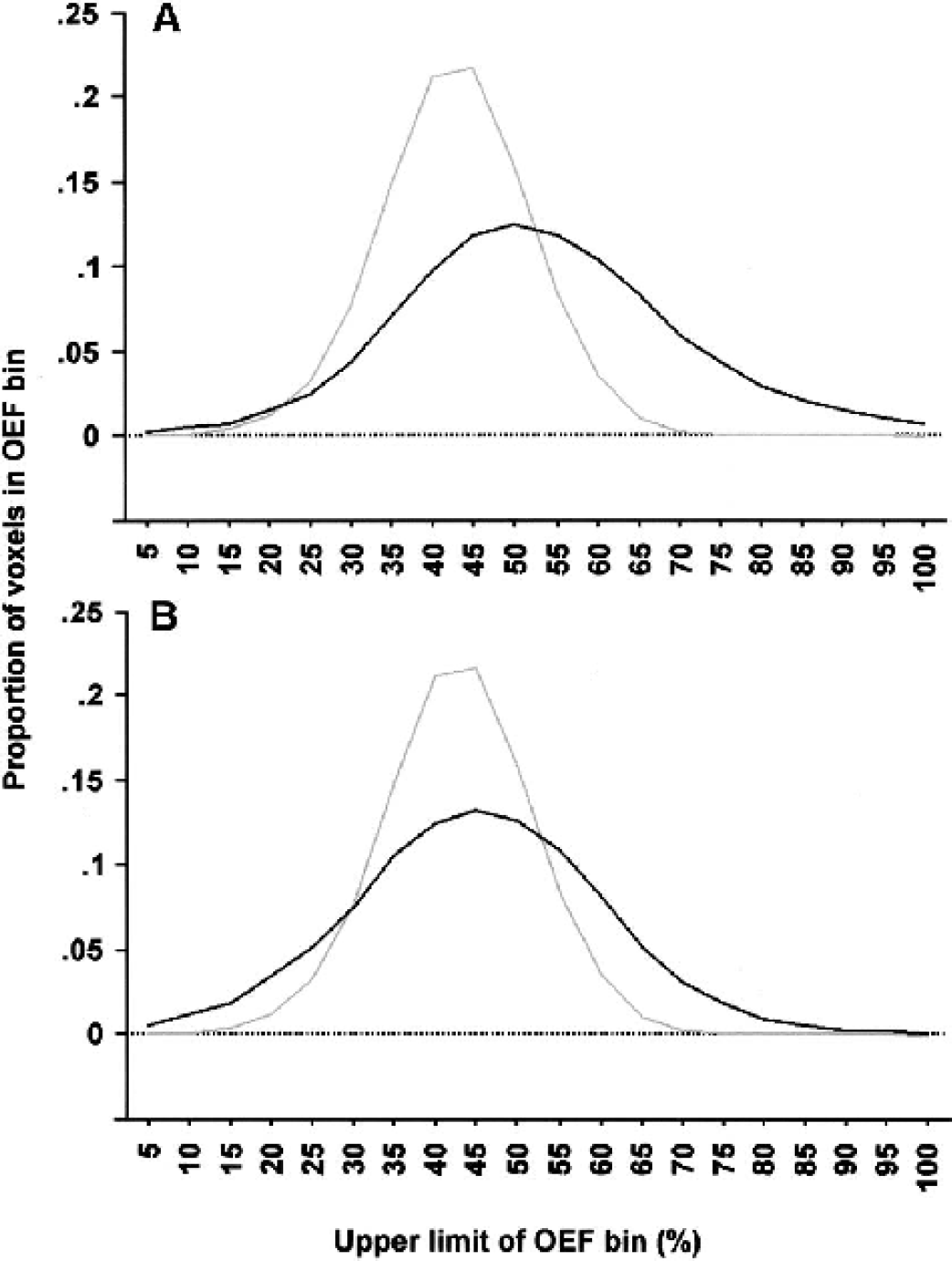
Comparison of patient and control OEF histogram distributions. OEF histograms from a volunteer (grey) and two representative patients within 24 hours of injury (black). (A) The patient histogram is broader and shifted to the right, with a prominent ischemic “tail” composed of voxels with high OEF values. (B) The patient histogram is broader with regions of both high and low OEF suggestive of ischemia and hyperemia respectively. OEF, oxygen extraction fraction.
Emission tracer concentrations in patient and control acquisitions
Mean tracer concentrations in control and patient data sets were similar. Control subjects showed mean (range) tracer concentrations of 6.1(3.4 to 8.1 kBq/mL) for 15O2 and 3.8 (2.5 to 5.4 kBq/mL) for H2 15O. Mean (range) tracer concentrations in patients were 8.6 (5.1 to 13) for 15O2 and 4.4 (3.1 to 7 kBq/mL) for H2 15O. In addition to inter-subject variability, there were clearly significant variations in tracer concentrations across the brain within subjects, and particularly within patients. However, voxels with extremely low emission counts represented a very small fraction of the brain volume. The highest volume of brain tissue in any patient with emission counts consistent with a CBF < 10 mL·100g−1·min−1 was 72 mL (6.5% of the brain volume) and less than one third of these voxels showed high OEF (based upon a calculated CvO2 of < 3.5 mL/100 mL) (22 mL or approximately 2% of the brain volume). Similarly, the highest volume of brain tissue with emission counts consistent with a CBF less than 5 mL·100g−1·min−1 was 32 mL (3% of the brain volume), but voxels with a CBF < 5 mL·100g−1·min−1 coupled with high OEF comprised, at most, 11 mL (representing approximately 1% of the brain volume).
Assessment of signal-to-noise characteristics as a confounder in voxel-based analyses
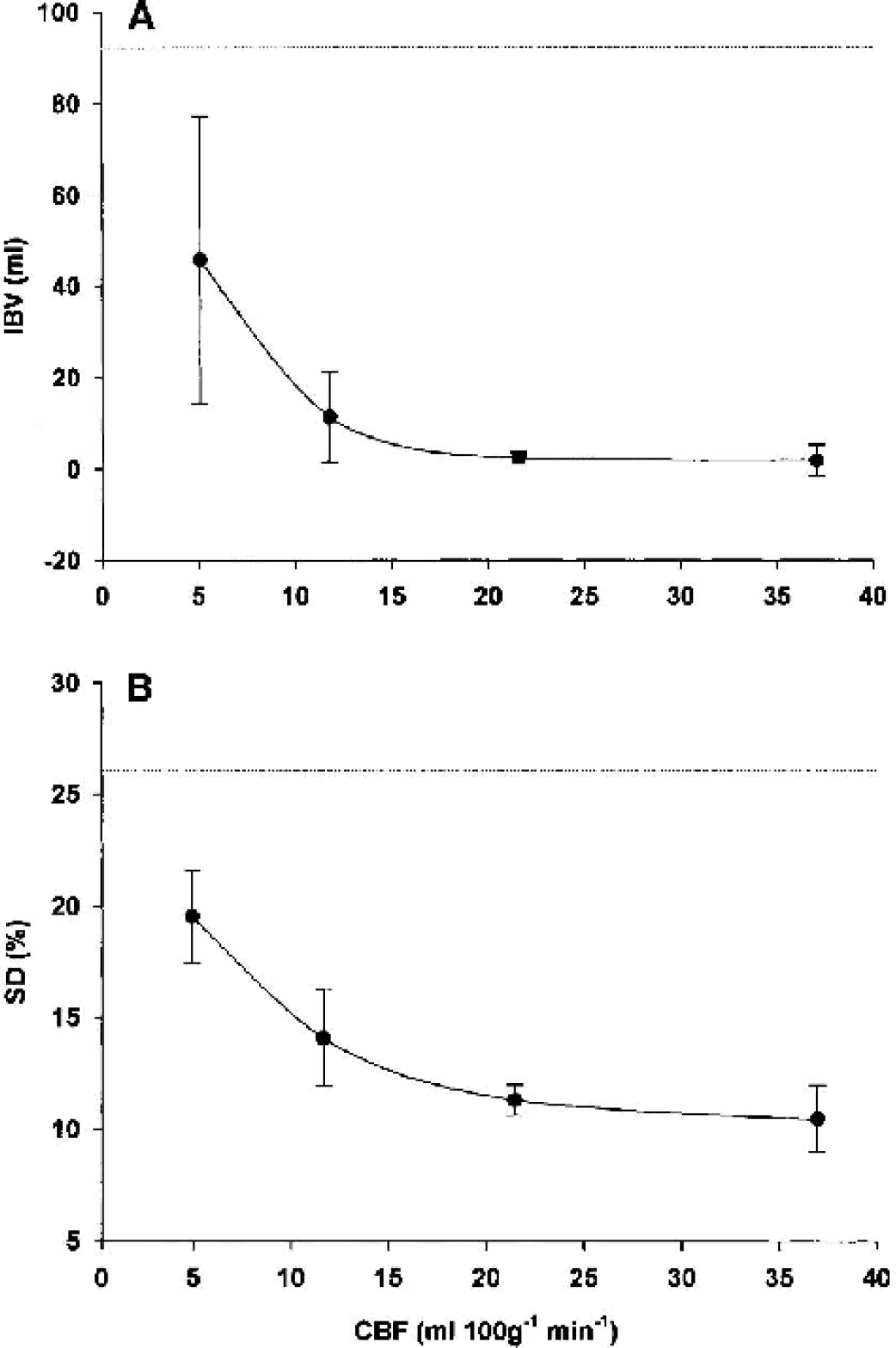
Simulated effects of a reduction in blood flow on control data. Control data reconstructed with 75%, 50%, and 25% of the total emission frame duration to simulate images with a blood flow of approximately 20, 10, and 5 mL·100g−1·min−1, respectively. Baseline data had a CBF of 37 mL·100g−1·min−1. (A) Mean ± SD curve to demonstrate the simulated effect of a reduction in global blood flow on the IBV. The IBV of the first reference patient data set is shown by the dotted line (92 mL). (B) Mean ± SD curve to demonstrate the simulated effect of a reduction in global blood flow on the SD of the OEF histogram. The SD of the OEF histogram of the first reference patient dataset is shown by the dotted line (26%). IBV, ischemic brain volume; SD, standard deviation; OEF, oxygen extraction fraction.
The degradation in image statistics also produced significant increases in the SD of OEF histograms at all stages (P < 0.001; paired t-tests). However, as with the IBV measurements, the absolute increases were relatively modest, except with the most severe degradation in image statistics (Fig. 5B).
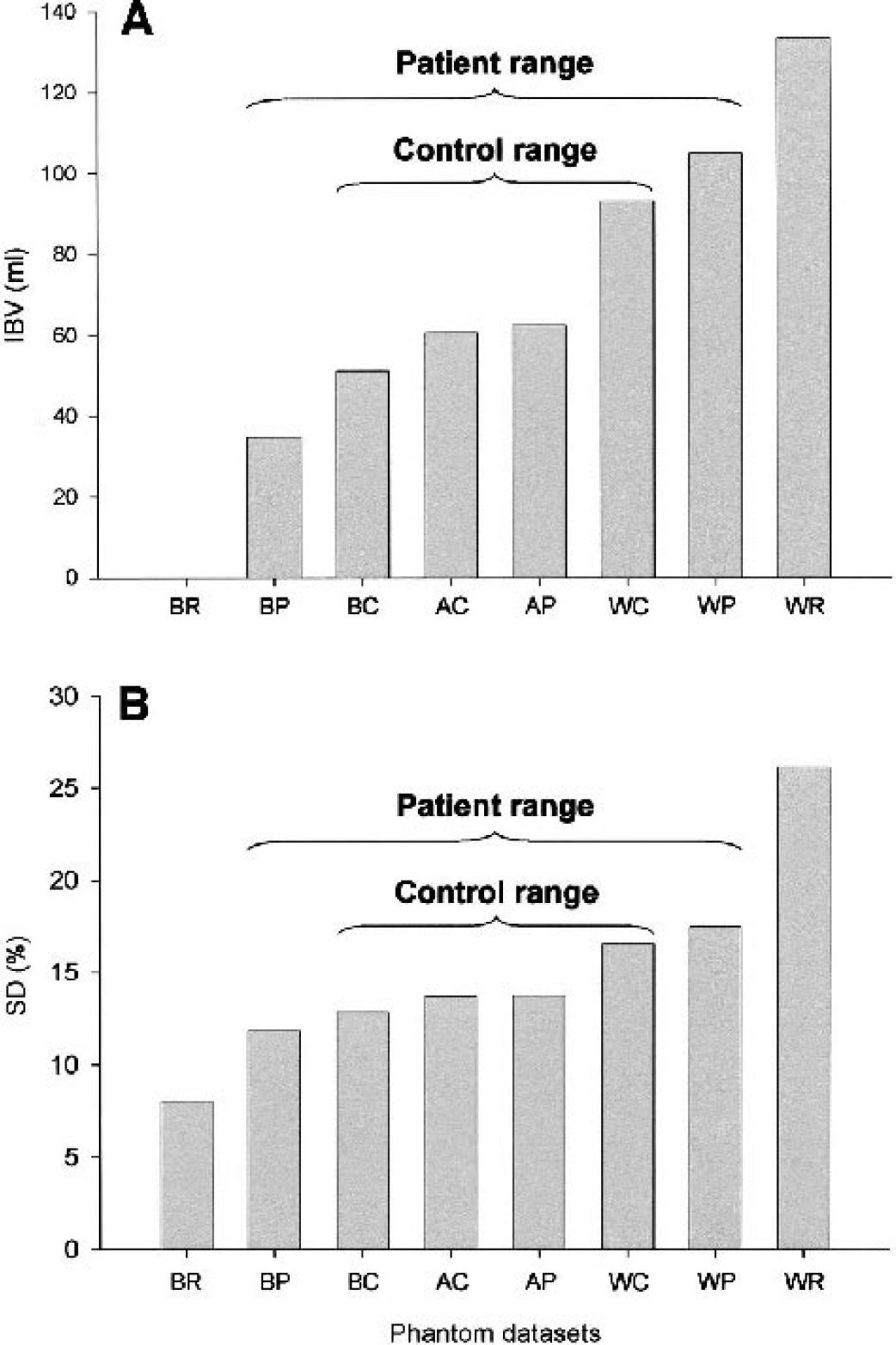
The effect of varying tracer concentrations in phantom data sets. (A) Histogram to demonstrate the calculated IBV of the worst and best reference data sets (WR and BR, respectively), and the best, worst, and average control and patient-simulated data sets (BC, WC, AC, BP, WP, and AP, respectively). (B) Histogram to demonstrate the measured SD of the OEF distribution for the worst and best reference data sets (WR and BR respectively), and the best, worst, and average control and patient-simulated data sets (BC, WC, AC, BP, WP, and AP, respectively). IBV, ischemic brain volume; SD< standard deviation; OEF, oxygen extraction fraction.
Assessment of the effect of the blood-brain partition coefficient (ρ) for H2 15O and C15O signal-to-noise characteristics upon OEF measurement
In Fig. 7, the effect of a change in the value for ρ on the measured OEF is displayed for a range of OEF values. As the value of ρ decreases, there is an increase in the calculated OEF value, particularly for regions with low OEF. Regions of the brain with high OEF appear least sensitive to such errors, with clinically significant increases in OEF only occurring with values for ρ of < 0.4.
In Fig. 8A, the effect of CBV on the calculated OEF is displayed for a range of OEF values. As the CBV value decreases below the baseline value of 4.2 mL·100g−1, there is an increase in the calculated OEF value, particularly for CBV values below zero and within brain regions with low OEF. In Fig. 8B, the CBV histograms of the 12 patients following head injury are shown. The mean (range) volume of brain with CBV values less than zero was 4.7 (0.5 to 19.8) mL. These data show that, within the range of CBV values seen in our patient data sets, the impact of CBV on OEF calculation is small, particularly for high OEF values.
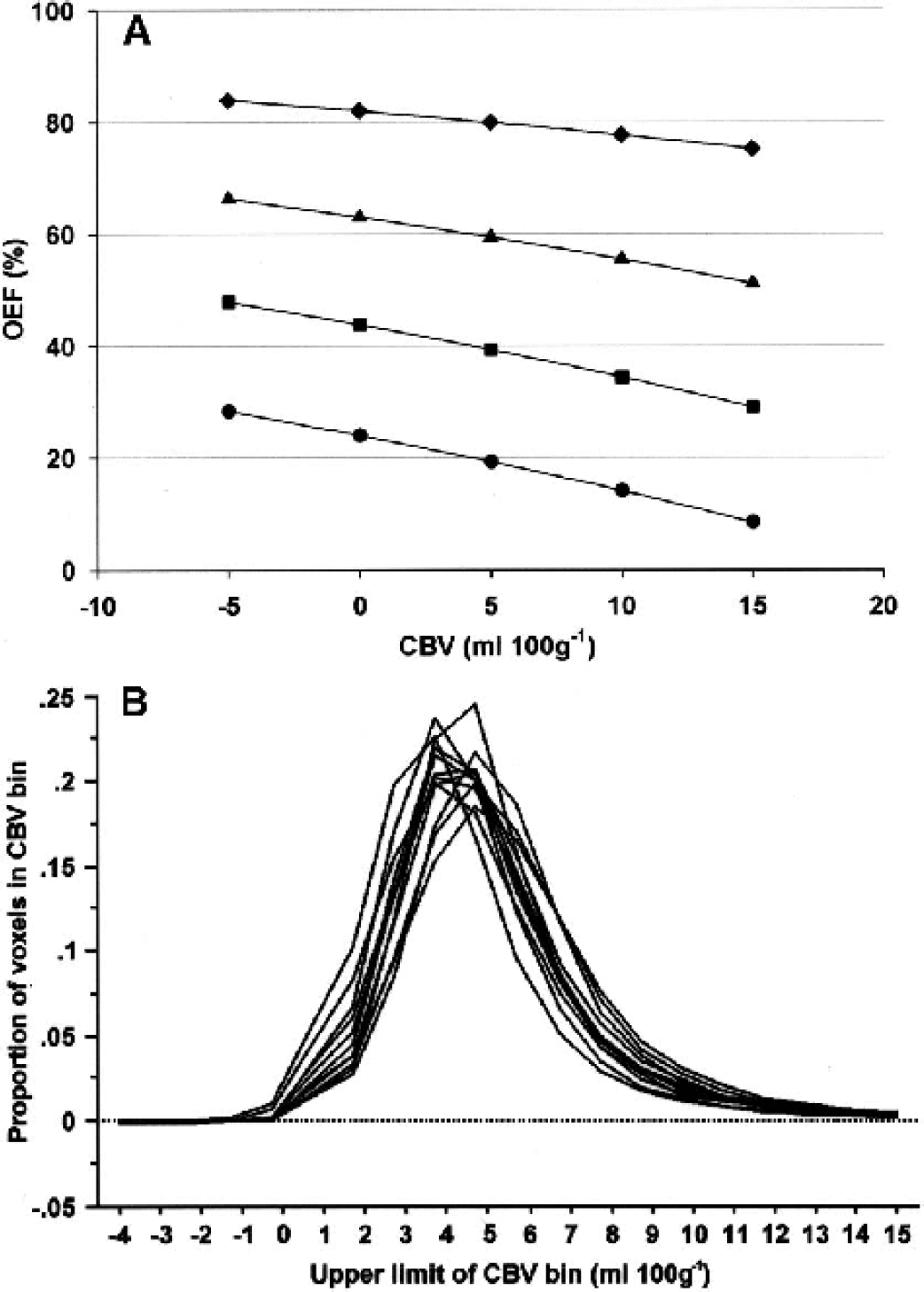
Assessment of the effect of CBV upon OEF measurement within the range of values seen in clinical data sets. (A) Curve to demonstrate the effect of CBV upon simulated patient data with OEF values of 20% (•), 40% (□), 60% (▲), and 80% (♦). In these simulations, the CMRO2 remained constant (2.4 mL·100g−1·min−1), and changes in OEF were achieved by varying CBF from a baseline value of 34 mL·100g−1·min−1. In each case, the effect of CBV upon the calculated OEF was assessed using the baseline CBV of 4.2 mL·100g−1 and the range of voxel values obtained from 12 patients within 24 hours of head injury. (B) CBV histograms from 12 patients within 24 hours of injury, showing the distribution of voxels in each CBV bin. OEF, oxygen extraction fraction.
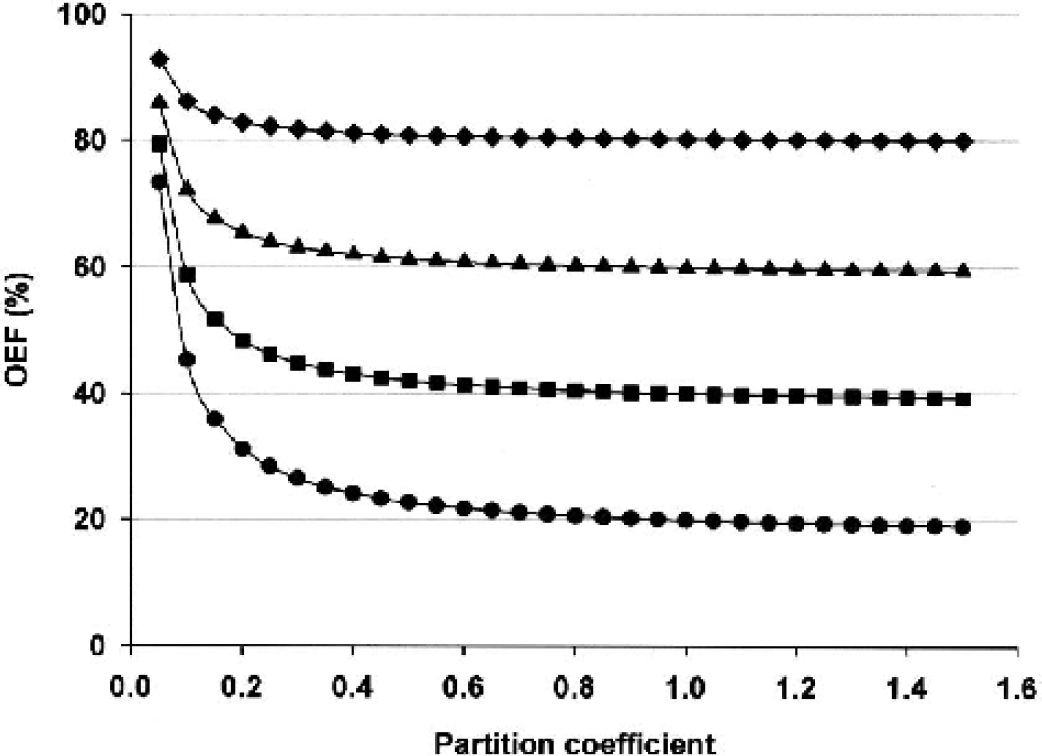
Assessment of the effect of the blood-brain partition coefficient for H2 15O upon OEF measurement. Curve to demonstrate the effect of a change in the value for the partition coefficient for H2 15O upon simulated patient data with OEF values of 20% (•), 40% (□), 60% (Δ), and 80% (♦). In these simulations, the CMRO2 and CBV remained constant (2.4 mL·100g−1·min−1 and 4.2 mL·100g−1, respectively), and changes in OEF were achieved by varying CBF from a baseline value of 34 mL·100g−1·min−1. OEF, oxygen extraction fraction.
DISCUSSION
The purpose of this report was to explore the confidence with which differences in ischemic burden can be ascribed to physiologic changes for PET data of variable statistical quality. We found that the deterioration in image statistics from a simulated reduction in CBF resulted in statistically significant increases in the calculated IBV and SD of OEF histograms. However, the absolute changes in IBV and SD of OEF attributable to this methodologic manipulation were small and clinically insignificant in the context of actual IBV values that we have obtained in patients with severe head injury (Coles et al., 2002a).
It is important to define valid voxel-based methods for assessment of ischemic burden in this patient group. Conventional functional imaging approaches in clinical and experimental stroke have traditionally used CBF thresholds for ischemia and have succeeded in identifying useful predictive values for tissue survival or death (Heiss et al., 1992; Marchal et al., 1996; Powers et al., 1985). However, the situation in head injury is confounded by the use of sedative agents and by the metabolic effects of trauma (Bergsneider et al., 2000; Verweij et al., 2000), which may cause primary reductions in cerebral metabolism; coupled CBF decreases in this context would not represent ischemia. Under these circumstances, the only true measure of the adequacy of CBF is a measurement of the OEF. In addition, pathophysiology in head injury is complex. Although the primary injury is important in terms of eventual outcome, secondary ischemic insults are responsible for worsening of outcome in many patients (Jones et al., 1994). In this case, it is difficult to predict thresholds for tissue viability based on early measurements of CBF and CMRO2 and late structural imaging with any certainty.
Additional problems arise with quantifying ischemic burden in the injured brain because of the lack of a priori knowledge regarding the location of ischemia. Ischemia in stroke usually conforms to topographical patterns, with identification of an ischemic core and penumbra (Baron, 1999). Whereas ischemia may be prominent in perilesional areas in head injury (Bouma et al., 1992; McLaughlin and Marion, 1996), significant ischemia may also be observed in structurally normal brain, and this may be significantly modulated by systemic physiology owing to impaired pressure autoregulation (Czosnyka et al., 1996) and the effect of PaCO2 on the cerebral circulation (McLaughlin and Marion, 1996). Consequently, we needed to identify methods to estimate ischemic burden across the entire brain, making no assumptions regarding the location of such ischemia. The integration of voxels with critically high OEF values provides a novel way of making such estimates in practice, but the identification of ischemic thresholds needs to be based upon sound physiologic premises. Both experimental (Sutton et al., 1990) and clinical (Powers et al., 1985; Yundt and Diringer, 1997) literature suggest that the CvO2 may provide the best variable to predict the risk of ischemic injury because it uses oxygen transport data (derived from hemoglobin and arterial oxygen saturation) to individualize the information provided by OEF values. We provide data on ischemic brain volumes with a CvO2 cutoff of 3.5 mL/100 mL based upon the best available estimates of critical CvO2 (Powers et al., 1985; Sutton et al., 1990; Yundt and Diringer, 1997). Moving this threshold up or down results in small changes in the measured ischemic brain volume but does not materially affect the statistical or clinical significance of the result. It is important to realize that there are no clear data on what constitutes a value of OEF that, if sustained for a period of time, will lead to neuronal damage. We do not claim that our chosen threshold is predictive of such neuronal injury but that it is indicative of an imbalance in normal flow metabolism coupling that suggests tissue is at high risk. The threshold is based upon the best available data and is clinically useful in terms of the management of head injury, where we wish to prevent the occurrence of further neuronal injury. In addition, comparison of the OEF distribution allows further interpretation of the balance between blood flow and metabolism in head injury. Close matching of flow to metabolism normally results in remarkably little variation in OEF across the brain despite wide regional variations in CBF and CMRO2 (Lebrun-Grandie et al., 1983). The wide based OEF histograms after head injury suggest that whereas high OEF values may represent ischemia, the pathophysiology may be more complex than that seen with ischemic stroke. The coexistence of relative ischemia and hyperemia in some patients (Fig. 4) may represent a more fundamental problem with matching of perfusion to oxygen use after head injury.
The use of voxel-based analysis to define tissue at risk is new in this context but has been used in other settings such as stroke (Marchal et al., 1999). However, statistics in such voxel-based measurements are less robust than those from larger ROIs, and the calculated spread of values in metabolic maps may increase when emission counts are reduced, as with low CBF values in patients. The concern is that this would result in more extreme values, which might translate into more voxels with high OEF values and higher ischemic brain volumes. We have confirmed in experiments using the Hoffmann brain phantom that a reduction in emission counts leads to a significant error in the absolute value of individual voxel OEF values. However, the global signal-to-noise characteristics of the patients within 24 hours of severe head injury and our data from healthy volunteers are very similar. This is shown by the fact that the calculated IBV and measured SD of the OEF histograms from phantom data are nearly the same when data with equivalent emission counts to the best, worst, and average control, and patient data sets are compared. This is an important finding as studies to date have suggested that it is during this period after head injury that blood flow is lowest (Martin et al., 1997). The relatively small changes produced by manipulation of the statistical quality of the data suggest that larger differences in the value of IBV or SD of OEF (as observed in representative patient data sets) are likely to be a true reflection of abnormal physiology.
To address the clinical reality of head injury, we took advantage of the fact that we acquired the H2 15O and 15O2 emission frames in 2.5- or 5-minute frames. This allowed us to examine the effect of a reduction in signal-to-noise equivalent to that expected from a reduction in global blood flow in controls from approximately 40 to 20, 10, and 5 mL·100g−1·min−1 without a change in physiology. As expected, the calculated value of IBV and the measured SD of the OEF histograms increased as the emission statistics were reduced. In both cases, the increases were small until the noise was equivalent to a global blood flow below 10 mL·100g−1·min−1. Although the phantom and control data we assessed were based upon the global characteristics of the emission data, it is obvious that there are clear regional differences in patients with head injury. Using the emission data of the patients, we measured the volume of brain with counts predictive of a blood flow below 10 and 5 mL·100g−1·min−1. It is important to realize that during patient image processing we attempt to exclude any extra axial hematomas, cerebrospinal fluid, and extra cranial tissue to reduce error in voxel-based analyses. This is reflected in the mean volume of tissue with a CBF of less than 10 and less than 5 mL·100g−1·min−1 of 32 and 10 mL, respectively. A major part of this volume of tissue was either severely damaged brain with low CMRO2 and OEF or was a result of partial volume effects. This is corroborated, in part, from previous experimental (Astrup et al., 1981) and clinical (Marchal et al., 1999) studies of stroke where a blood flow below approximately 10 mL·100g−1·min−1 leads to a failure of energy metabolism and ion homeostasis and is predictive of neuronal death. In fact, in the 12 patients with head injury, the highest volume of tissue with such low blood flow and high OEF (based upon a calculated CvO2 of < 3.5 mL/100mL) in any patient was only 22 and 11 mL, respectively. It is important to recognize that even this volume of tissue does not exclusively represent noise and may still be clinically relevant.
Two further potential sources of error concern the choice of value for the partition coefficient for H2 15O and the signal-to-noise characteristics of the C15O emission data. Despite publications that have suggested a value for ρ of 0.86 (Lammertsma et al., 1992), the true value remains unknown (Herscovitch and Raichle, 1985; Lammertsma et al., 1981), particularly within pathologic disease states. We chose to use a ρ of 0.95 in both patients and volunteers based upon the in vitro data (Herscovitch and Raichle, 1985). To assess the potential effect of different values of ρ on OEF measures of ischemia, we used patient tracer concentrations to simulate a range of OEF values. Although we found clinically significant increases in OEF, such increases did not occur until ρ was markedly reduced, and regions of high OEF appeared the least sensitive. Another potential source of error concerns the signal-to-noise characteristics of the C15O emission data and the resulting CBV images. To quantify the significance of such effects, the simulated OEF values were recalculated using the range of CBV values obtained from the 12 patients with head injuries. We found that regions with abnormally low or negative CBV resulted in an overestimation of OEF but that the effect was limited to a small volume of the brain and was least prominent in brain regions with high OEF. Because the range of CBV under consideration includes any errors attributable to noise, the implication of these results is that IBV measurement is unlikely to be significantly affected by noise within the C15O emission data. In conclusion, although the true value for ρ and the statistical quality of the CBV images will affect the calculated OEF, we believe that such effects will have limited impact upon the measures of ischemic burden used in these studies.
These data allow us to interpret the results with some certainty. Although an absolute increase in IBV and SD of the OEF distribution will be related, in some part, to a reduction in emission statistics as a consequence of reduced blood flow, a significant increase in comparison with control values provides a robust measure of abnormal physiology. In particular, the degree of error does not become significant until blood flow is reduced below 10 mL·100g−1·min−1. Finally, the location of voxels with such high OEF should be related to the structural injury and their significance interpreted in the light of the clinical condition of the patient.
CONCLUSIONS
This study shows that voxel-based analysis of PET OEF maps is sensitive at defining tissue at risk of ischemic injury after early head injury. Such methodology is dependent upon the underlying signal-to-noise characteristics of PET emission data, but the extent of such effects can be calculated and are unlikely to represent a limiting confound. IBV estimates are independent of the small-to-large vessel hematocrit ratio and are relatively unaffected by changes in the blood-brain partition coefficient for H2 15O within clinically relevant ranges. This is important because these variables may change unpredictably in disease. We conclude that this technique is a valid and useful tool for quantifying ischemic burden after traumatic brain injury.
Footnotes
Acknowledgements
The authors thank Dr JC Matthews and the members of the Wolfson Brain Imaging Center for their help in conducting these studies.