
Abstract
Locally administered tissue plasminogen activator (TPA) accelerates clearance of intraventricular hemorrhage (IVH), but its impact on neurologic outcomes remains unclear and preclinical research suggests it may have pro-inflammatory effects. We randomly allocated patients with ruptured cerebral aneurysms and IVH, treated with endovascular coiling and ventricular drainage, to receive either 2-mg intraventricular TPA or placebo every 12 hours. Cerebrospinal fluid (CSF) and serum cytokine and white blood cell (WBC) concentrations were measured before drug administration and daily for 72 hours. Cerebrospinal fluid D-dimer levels were assessed 6 and 12 hours after administration to quantify fibrinolysis. Six patients were randomized to each group. Patients treated with TPA developed higher CSF cytokine concentrations compared with placebo-treated patients (P < 0.05 for tumor necrosis factor-α, interferon-γ, interleukin (IL)-1α, IL-1β, IL-2, IL-4, and IL-6), as well as higher CSF WBC counts (P = 0.03). Differences were greatest after 24 hours and decreased over 48 to 72 hours. The magnitude of the inflammatory response was significantly associated with peak CSF D-dimer concentration and extent of IVH clearance. We conclude that intraventricular TPA administration produces a transient local inflammatory response, the severity of which is strongly associated with the degree of fibrinolysis, suggesting it may be induced by release of hematoma breakdown products, rather than the drug itself.
Keywords
INTRODUCTION
The volume of subarachnoid hemorrhage (SAH) and intraventricular hemorrhage (IVH) occurring in the setting of a ruptured cerebral aneurysm, as well as the rate of blood clearance, are strongly associated with a greater risk of complications and poor neurologic outcomes.1–3 The accumulation of hemoglobin breakdown derivatives, including iron, bilirubin oxidation products, and oxygen-free radicals, contributes to early brain injury and a higher risk of hydrocephalus and delayed cerebral ischemia.4–6 The presence of blood in the ventricular and subarachnoid spaces induces inflammation, which may be an additional important mechanism contributing to early and delayed brain injury.7–10 These observations provide a rationale for therapeutic measures aimed at accelerating the clearance of blood.
Numerous small clinical trials, with various treatment protocols and methodological limitations, have suggested that administration of fibrinolytic drugs into the basal cisterns of patients with SAH may reduce the risk of complications and improve neurologic recovery. 11 The most convenient method of administering intrathecal fibrinolytics is through an external ventricular drain (EVD), which is commonly inserted in patients with high-grade SAH or clinical evidence of hydrocephalus. Randomized trials involving patients with SAH or spontaneous intracerebral hemorrhage complicated by IVH have shown that low-dose intraventricular tissue plasminogen activator (TPA) hastens clearance of blood, although a meaningful impact on clinical outcomes has yet to be showed.12–16
Preclinical studies have reported that TPA may have neurotoxic effects by inducing inflammation, disrupting the blood–brain barrier, causing neuronal degeneration, and exacerbating cerebral edema.17–21 Observational human studies have reached conflicting conclusions, with some suggesting that intraventricular TPA induces sterile meningitis and increases perihematomal edema, and others reporting that it has no such effect and may, by removing blood, actually reduce inflammation.22–25
If intraventricular TPA does have toxic effects, it could attenuate any therapeutic benefit derived from more rapid clearance of blood. Concentrations of cytokines are known to be elevated in the cerebrospinal fluid (CSF) of patients with SAH, particularly among those with a higher clinical grade, and to be associated with a greater risk of complications and poor neurologic outcomes.26,27 Therefore, as part of a pilot clinical trial, we compared cytokine concentrations and white blood cell (WBC) counts in CSF and peripheral blood among patients randomly allocated to treatment with either intraventricular TPA or placebo.
MATERIALS AND METHODS
Trial Design
This was an ancillary study to a prospective, placebo-controlled, randomized pilot trial assessing the use of intraventricular TPA in the care of patients with aneurysmal SAH and IVH. 12 The study was performed in accordance with the Canadian Tri-Council Policy Statement regarding Ethical Conduct for Research Involving Humans and was approved by the Conjoint Health Research Ethics Board at the University of Calgary. The study was funded by grants from the University of Calgary and Hotchkiss Brain Institute, and was registered at www.clinicaltrials.gov (NCT01098890).
Participants
Patients with SAH were eligible if they had a modified Fisher score of 4 (thick subarachnoid blood with IVH), an aneurysm was identified and successfully treated with endovascular coil embolization, and an EVD was placed as part of routine clinical care. To be enrolled, patients also required a computed tomography (CT) scan performed after coil embolization and EVD insertion showing no increment in the amount of intracranial blood relative to a previous scan. Randomization occurred within 72 hours of aneurysm rupture. Informed consent was provided by the most appropriate surrogate decision maker.
Interventions
Patients were allocated to receive either 2 mg TPA (2 mL Cathflo Activase, Genentech USA Inc, 1 DNA Way, South San Francisco, CA, USA) or 2 mL of 0.9% saline every 12 hours, for a maximum of five doses. The TPA dose was lower than that used in other clinical trials of patients with SAH (3 to 5 mg every 12 hours),13,28 slightly higher than that used in the ongoing multicenter CLEAR-intraventricular hemorrhage trial (1 mg every 8 hours in the setting of intracerebral hemorrhage/IVH), 29 and comparable to that used in previous case series.30,31 The two preparations were visually indistinguishable. External ventricular drain tubing was cleansed with chlorhexidine, and drug administration occurred using maximal barrier precautions. Prior to drug delivery, 5 mL of CSF plus ~ 50% of the average hourly CSF output were slowly aspirated. Drug administration was followed by a 3-mL flush of 0.9% saline, and the drain was clamped for 1 hour. Patients underwent CT scans 12, 48, and 72 hours after the first dose of drug. Treatment was continued for the full five doses unless there was new blood seen on CT; if EVD closure was not tolerated because of high intracranial pressure; or when there was ‘sufficient’ clearance of SAH and IVH (defined a priori as the absence of SAH in the basal cisterns, no blood obstructing the third and fourth ventricles, and more than a 50% reduction in IVH volume).
Outcomes
Cerebrospinal fluid and blood samples were drawn for analysis immediately before the first dose of study drug and then every 24 hours for three consecutive days. Using the validated Luminex assay (R&D Systems, Minneapolis, MN, USA), we measured concentrations of interleukin (IL)-1α, IL-1β, IL-2, IL-4, IL-6, IL-10, tumor necrosis factor (TNF) α, and interferon (IFN) γ in CSF and serum. Daily serum and CSF WBC, and CSF red blood cell concentrations were also recorded. This was performed in an automated manner, which precluded determination of differential WBC concentrations.
Volume of IVH was estimated on serial CT scans using the IVH score (range 0 to 23; convertible into milliliters). 32 Two investigators, masked to clinical information, independently scored CT scans in a randomly generated order, and the mean of these two values was used for the analysis. Using enzyme-linked immunosorbent assay testing (HYPHEN BioMed, West Chester, OH, USA), D-dimer concentration was assessed in CSF collected into Biopool Stabilyte tubes (Trinity Biotech, Bray, Ireland) at baseline and 1, 6, and 12 hours after the first dose of study drug, to quantify fibrin-derived products released during thrombolysis.
Assessment of the impact of intraventricular TPA on clinical outcomes was not the primary purpose of this study. Nevertheless, neurologic outcomes were assessed at 6-month follow-up, classified using the modified Rankin scale, and dichotomized into categories of ‘favorable’ (score of 0 to 3) and ‘unfavorable’ (score of 4 to 6). Moderate–severe angiographic vasospasm was defined as at least 33% narrowing of any vessel on CT angiography (relative to the baseline CT angiogram used to identify the culprit aneurysm), performed on post-SAH day 8 ± 1. Delayed cerebral ischemia was defined as an otherwise unexplained neurologic deterioration (new focal deficit or sustained decline of ≥ 2 points in the Glasgow Coma Scale score) beginning 3 to 14 days after SAH, regardless of whether angiographic vasospasm was present.
Randomization and Masking
The order of treatment allocation was determined using a random number generator, with the results provided to the institutional research pharmacy. Allocation occurred in variable blocks of four using sealed opaque envelopes. Researchers, clinicians, laboratory personnel, patients, and families remained unaware of group assignment until all outcomes had been adjudicated and finalized.
Statistical Analysis
The rationale for the sample size of this pilot randomized trial was described in a previous publication. 12 Assuming a standard deviation of 5%, we calculated that we would require six patients per group to determine the mean daily percent hematoma clearance from the subarachnoid space with a precision of ± 4%. Categorical variables were summarized as proportions and compared using Fisher's exact tests. Continuous variables were presented as either medians with interquartile ranges or means with standard deviation, and analyzed using Mann–Whitney U-tests. Population-averaged, panel-data models using generalized estimating equations were developed to compare cytokine concentrations over time between the two treatment groups. An exchangeable correlation matrix was used. Model variables included group assignment (TPA versus placebo), time (days) after drug administration and an interaction term between group assignment and time. The analysis was repeated using the number of days after study drug as an ordinal predictive variable, to compare cytokine concentrations on individual days with baseline levels. To assess the relationship between inflammatory markers and the degree of fibrinolysis, linear regression was used to compare the change in CSF cytokine concentration at 24 hours with the peak D-dimer concentration and volume of ventricular blood clearance within the initial 12 hours after the first dose of TPA. P values < 0.05 were considered statistically significant. Analyses were performed using SAS (version 9.3, Cary, NC, USA) and graphs were created using GraphPad Prism (version 6.0, La Jolla, CA, USA).
RESULTS
Patient Characteristics
Recruitment and participant flow in this study has been described previously. 12 Six patients were treated with intraventricular TPA and six with placebo. One patient who was otherwise eligible for the trial received open-label TPA at the request of his attending neurosurgeon because of EVD occlusion and the need for EVD replacement before randomization in the context of massive IVH. Informed consent was obtained to use this patient's data for the translational component of the study, but the data was not included in comparisons between TPA and placebo groups. Baseline characteristics for the 12 randomized patients, as well as previously reported clinical outcomes, 12 are shown in Table 1. Patients were treated with TPA or placebo at a median of 44 hours after aneurysm rupture.
Baseline characteristics and outcomes of patients treated with TPA or placebo
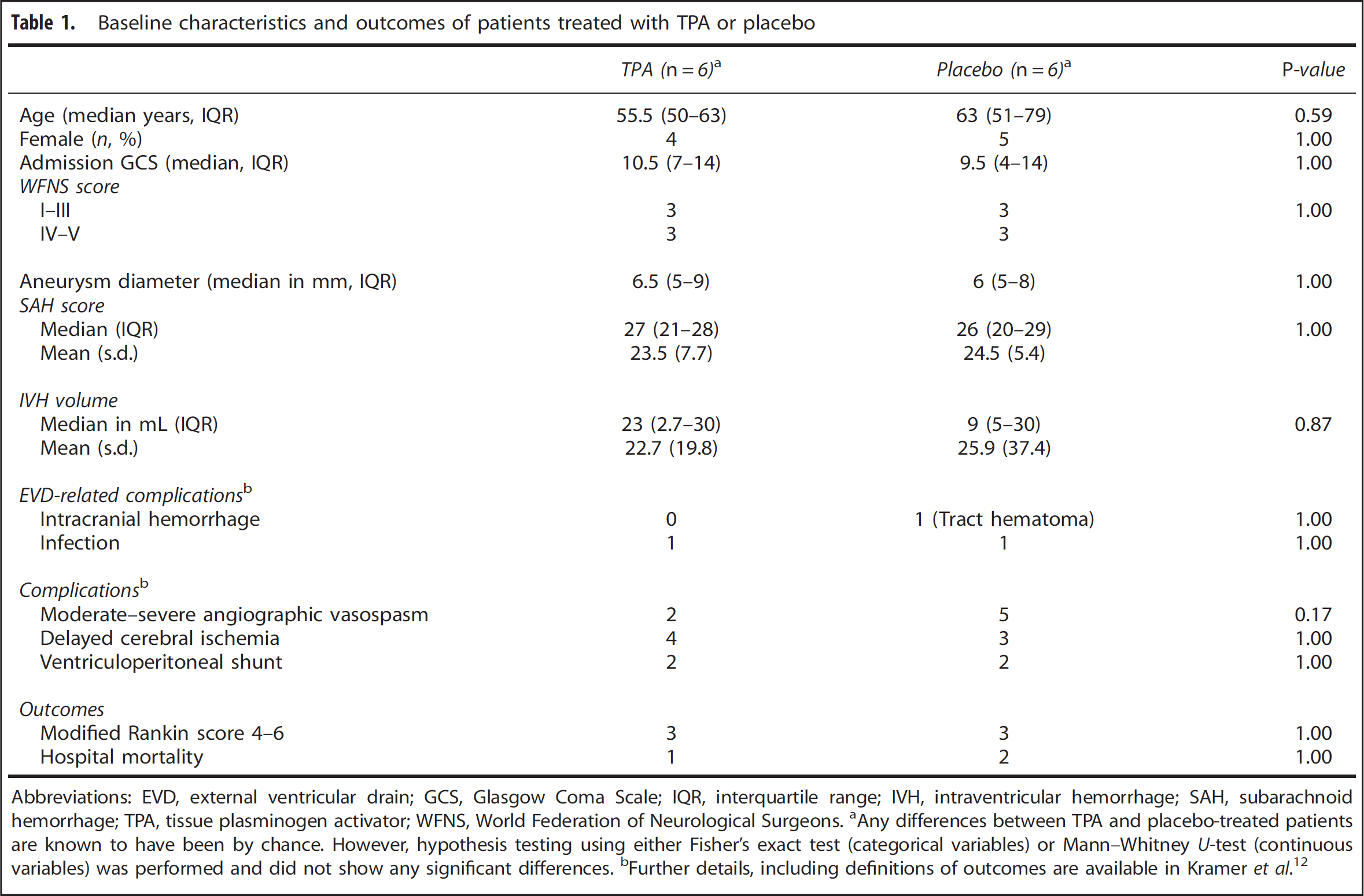
Abbreviations: EVD, external ventricular drain; GCS, Glasgow Coma Scale; IQR, interquartile range; IVH, intraventricular hemorrhage; SAH, subarachnoid hemorrhage; TPA, tissue plasminogen activator; WFNS, World Federation of Neurological Surgeons.
Any differences between TPA and placebo-treated patients are known to have been by chance. However, hypothesis testing using either Fisher's exact test (categorical variables) or Mann–Whitney U-test (continuous variables) was performed and did not show any significant differences.
Further details, including definitions of outcomes are available in Kramer et al. 12
Cerebrospinal Fluid and Blood Inflammatory Markers Cerebrospinal fluid cytokine concentrations did not differ significantly between groups at baseline, but all cytokines increased in concentration after TPA administration (Figure 1). At 24 hours, TPA-treated patients had statistically significantly higher concentrations of IFNγ (P = 0.02), IL-1α (P = 0.01), IL-2 (P = 0.009), IL-4 (P = 0.03), and IL-6 (P = 0.02), but not TNFα (P = 0.06), IL-1β (P = 0.07), and IL-10 (P = 0.24) when compared with patients receiving placebo. When days were regarded as an ordinal variable (using day 0 as the baseline reference), treatment with TPA significantly modified the relative effect of time on the concentration of several cytokines, but only on day 1. This was true for TNFα (P = 0.04), IL-1α (P = 0.04), IL-1β (P < 0.05), and IL-2 (P < 0.05), but not IL-4 (P = 0.06), IL-6 (P = 0.09), IL-10 (P = 0.14), and IFNγ (P = 0.15). In contrast, serum concentrations of all cytokines were consistently similar between patients treated with TPA or placebo (Figure 2).
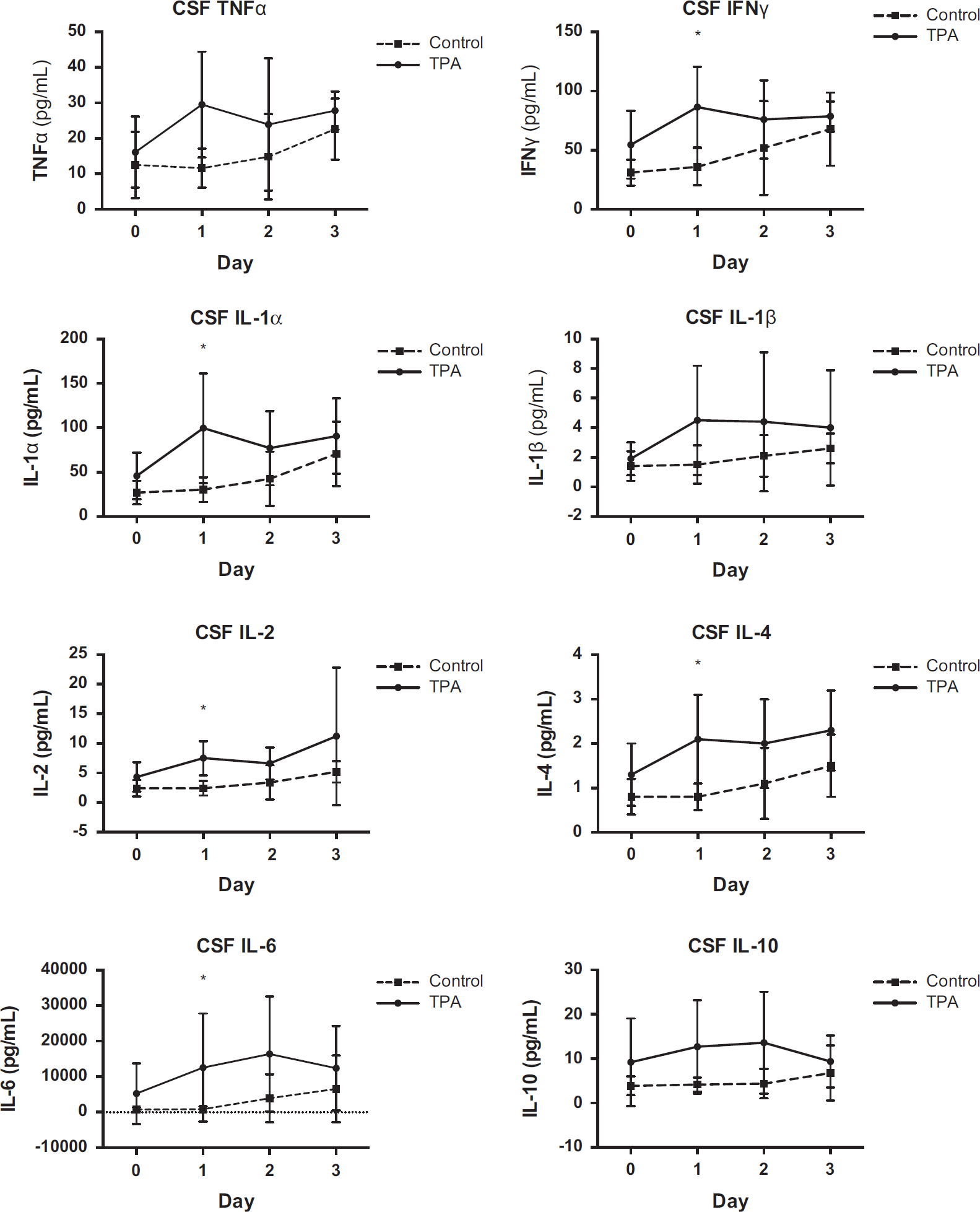
Cerebrospinal fluid cytokine concentrations. IFN, interferon; IL, interleukin; TNF, tumor necrosis factor; TPA, tissue plasminogen activator. The presence of an asterisk indicates P < 0.05 for comparison between TPA versus placebo on an individual day.
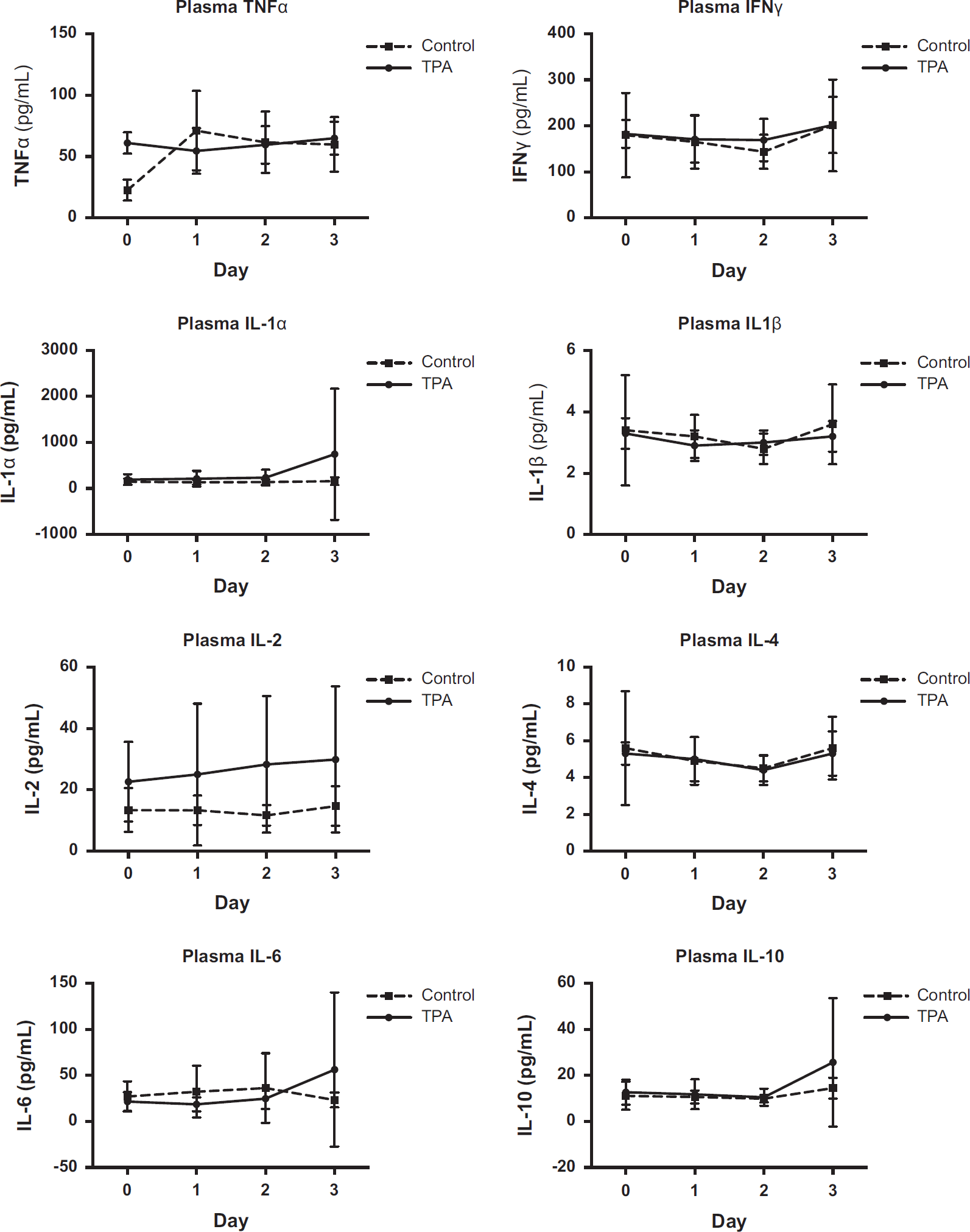
Plasma cytokine concentrations. IFN, interferon; IL, interleukin; TNF, tumor necrosis factor; TPA, tissue plasminogen activator.
Cerebrospinal fluid WBC concentration also increased in patients treated with TPA in the first 24 to 48 hours, before decreasing again at 72 hours (Figure 3). The difference in WBC concentration approached, but did not reach, statistical significance on any individual day. However, for the entire 72-hour time period, treatment with TPA did significantly increase CSF WBC concentration (P = 0.03). Cerebrospinal fluid red blood cell concentration was also consistently higher in patients treated with TPA, but the difference was not statistically significant. There was no difference in serum WBC count between groups.
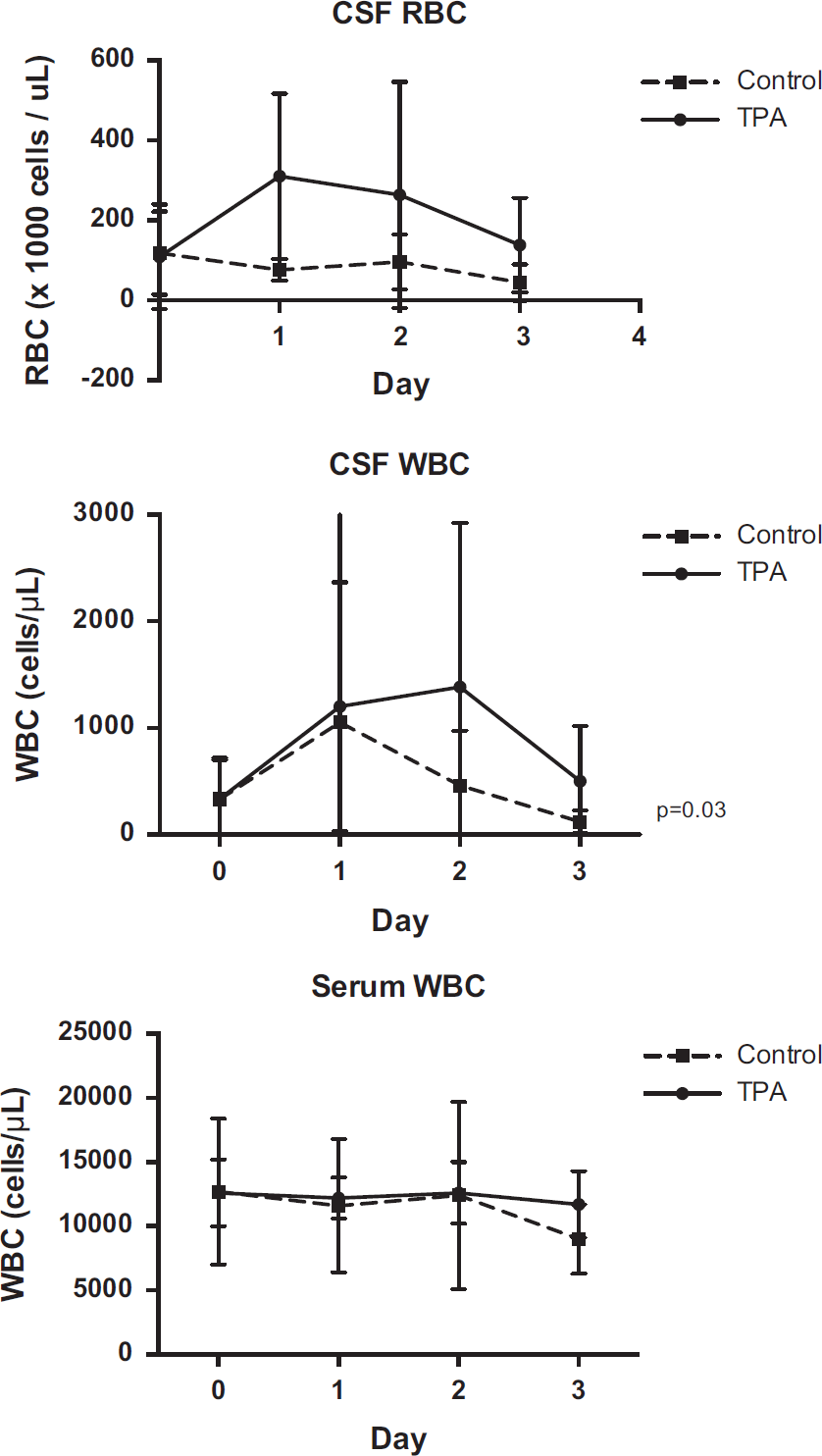
White blood cell and red blood cell concentrations in cerebrospinal fluid and blood.
In a post hoc analysis, we identified an additional five patients with aneurysmal SAH who were treated in our ICU with intraventricular TPA since completion of the randomized trial. The median baseline CSF WBC concentration was 500 (interquartile range 200 to 700) cells per μL, and this increased to 1,200 (interquartile range 800 to 1,900), 750 (650 to 800), and 400 (300 to 600) cells per μL, respectively, at 24, 48, and 72 hours after the first dose of TPA. Combining these five nonrandomized with the previously randomized patients, there was a marked increment between the baseline and 24-hour posttreatment CSF WBC concentration (P = 0.001 using Wilcoxon matched-pairs signed-rank test).
Relationship Between Degree of Fibrinolysis and Cytokine Concentrations
Among TPA-treated patients, D-dimer concentration in CSF was 19,834 ng/mL at baseline and increased to 38,937, 279,552, and 194,935 ng/mL at 1, 6, and 12 hours after the first dose, respectively. There was a direct linear relationship between the peak CSF D-dimer concentration and the corresponding 24-hour increment in the concentration of six out of eight cytokines assessed (Figure 4; P < 0.05 for TNFα, IFNγ, IL-1α, IL-2, IL-4, and IL-10). Similarly, the reduction in IVH volume between the baseline and 12-hour CT scan was predictive of the 24-hour increment in the concentration of several cytokines (Figure 5; P < 0.05 for TNFα, IFNγ, IL-2, and IL-4).
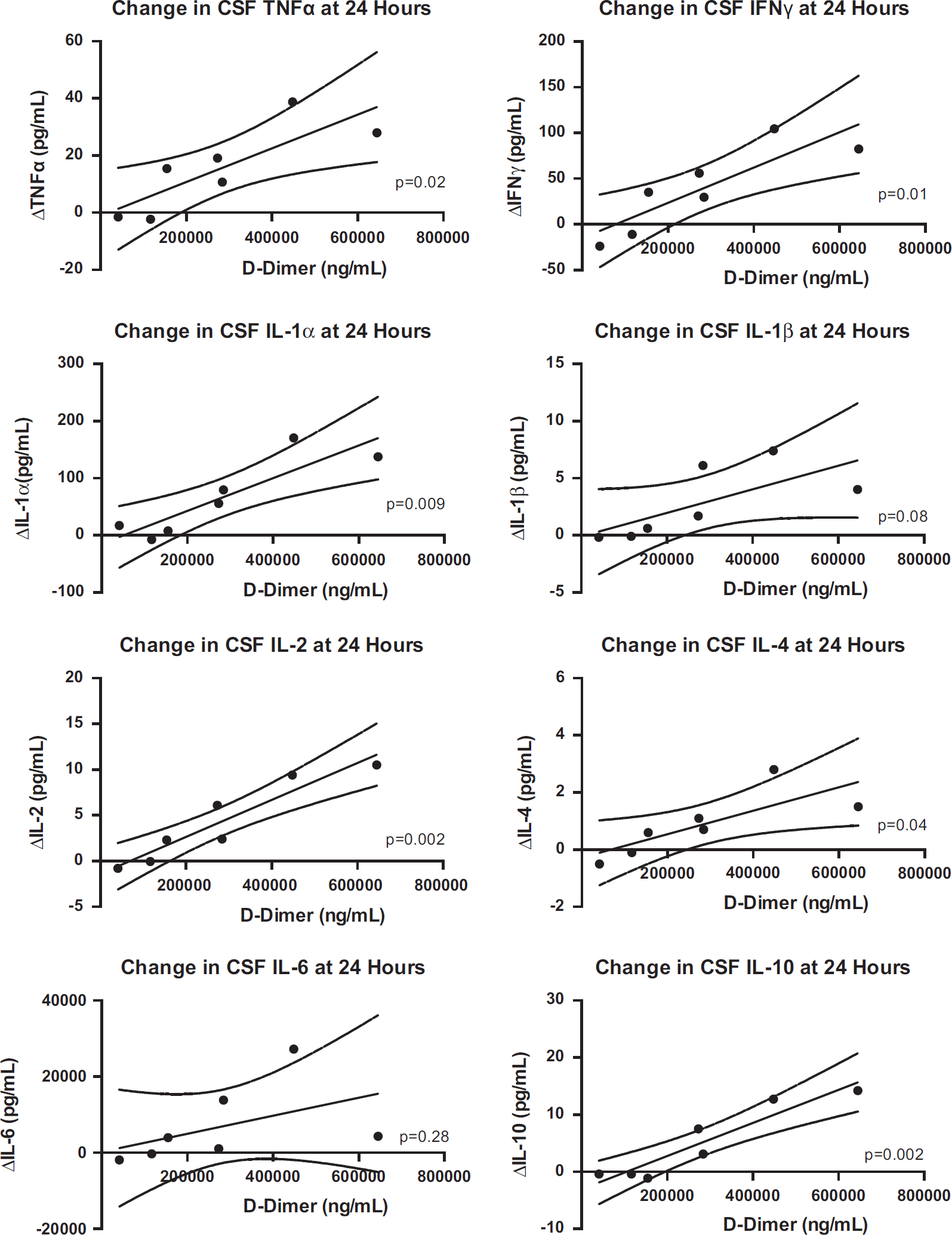
Relationship between increment in cerebrospinal fluid cytokines over 24 hours and efficacy of fibrinolysis, assessed by measurement of fibrin-derived product. IFN, interferon; IL, interleukin; TNF, tumor necrosis factor; TPA, tissue plasminogen activator. The presence of an asterisk indicates P < 0.05 for comparison between TPA versus placebo on an individual day.
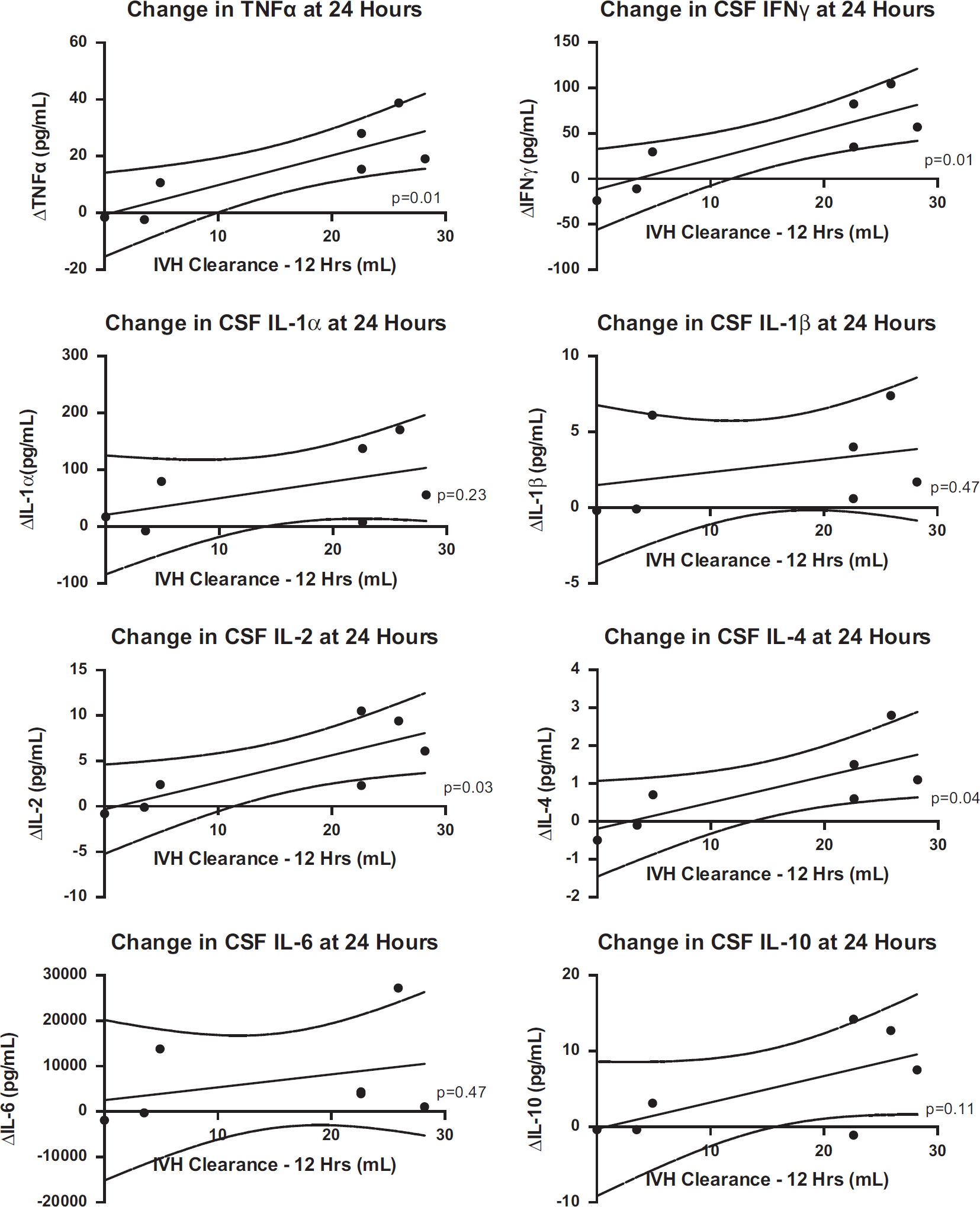
Relationship between increment in cerebrospinal fluid cytokines over 24 hours and degree of ventricular blood clearance. IFN, interferon; IL, interleukin; TNF, tumor necrosis factor; TPA, tissue plasminogen activator. The presence of an asterisk indicates P < 0.05 for comparison between TPA versus placebo on an individual day.
Relationship Between Cytokine Concentrations and Outcomes
Patients with poor 6-month outcomes had significantly higher baseline concentrations of CSF TNFα (P = 0.008), IFNγ (P = 0.03), IL-1α (P = 0.008), IL-1β (P = 0.02), IL-2 (P = 0.01), and IL-4 (P = 0.02), but not IL-6 (P = 0.08) and IL-10 (P = 0.10; Supplementary Table). However, CSF concentrations did not differ between patients with poor or favorable outcomes on any of the ensuing 3 days for any of the cytokines measured. Although CSF cytokine concentrations were generally higher in patients who developed delayed cerebral ischemia, none of the differences were statistically significant.
DISCUSSION
This analysis of a placebo-controlled randomized trial shows that administration of intraventricular TPA induces an increment in inflammatory cytokines in CSF. For essentially all measured cytokines, the difference in CSF concentrations between TPA- and placebo-treated patients was maximal in the first 24 hours, immediately after the time period with the greatest degree of ventricular and subarachnoid hematoma clearance.
The difference in CSF cytokine levels between groups decreased beyond 24 hours, even though patients in the experimental arm of the study continued to receive TPA, suggesting that the observed inflammatory response was primarily attributable to the effects of fibrinolysis rather than direct toxicity from the drug. This conclusion was further supported by the observation that there was a direct linear relationship between the rise in CSF cytokine concentrations in the first 24 hours and peak CSF levels of fibrin-derived product (D-dimer), as well as the radiographic quantity of blood cleared over the initial 12 hours. Patients in whom there was a greater degree of fibrinolysis and a larger volume of ventricular blood clearance had a more pronounced CSF inflammatory response.
The release of hemoglobin and its breakdown metabolites, such as iron and bilirubin oxidation products, into the brain and subarachnoid space, has been implicated in the pathophysiology of brain injury in intracerebral hemorrhage, SAH, and IVH.4–8,33–36 When an aneurysm ruptures, erythrocytes rapidly circulate in CSF and cover the surface of the brain. It is likely that heme and its breakdown products gain access not only to the subarachnoid space, but also to brain tissue via the Virchow-Robin space. 37 Heme itself may be neurotoxic and may induce inflammation, before being degraded into carbon monoxide, biliverdin, and iron by the enzyme heme oxygenase, which becomes markedly upregulated in glial cells in the context of SAH.4,6,9,38 Iron subsequently accumulates in glial cells and astrocytes, and also reacts with hydrogen peroxide to form reactive oxygen species, which in turn induces oxidative injury and exacerbates inflammation.4,8,38
It is now well established by randomized trials that pharmacological use of intraventricular TPA accelerates hematoma clearance, both from the ventricles and basal cisterns.12,13,38 Although the removal of blood is thought to be potentially beneficial in reducing the risk of complications, such as hydrocephalus and delayed cerebral ischemia, our findings suggest that the sudden, rapid release of hematoma breakdown products may transiently perpetuate injury and induce inflammation.
Despite these observations, our findings do not entirely rule out the possibility that some of the increment in CSF cytokines was directly attributable to toxic effects of TPA. A recent animal study suggested that intraventricular TPA exacerbates periventricular inflammation to a greater degree than urokinase. 39 However, it is unclear whether this effect was because of toxicity from TPA or a greater degree of fibrinolysis and, in turn, more exposure to toxic blood breakdown products. There have been no human studies directly comparing different intraventricular thrombolytic drugs. Our study assessed the burden of inflammation only in CSF and not in brain parenchyma. Even if TPA is directly neurotoxic, it is unclear to what degree TPA reaches brain tissue when administered into the ventricles.
The clinical implications of our findings require further study. It is conceivable that inflammation induced by fibrinolysis could attenuate any benefit derived from more rapid clearance of intracranial blood. Inflammation has been implicated as contributing to early and delayed brain injury in patients with aneurysmal SAH, and in contributing to hydrocephalus in patients with IVH.8–10,40 Accordingly, we found significantly higher baseline CSF cytokine concentrations among patients who had poor neurologic outcomes at 6 months. Still, it remains possible that more rapid clearance of blood could have a net benefit, since the ongoing presence of blood in the ventricles and subarachnoid space (probably with more gradual release of hemoglobin breakdown products) also induces inflammation that persists for several days.25,41 Future research should further assess whether the magnitude of the inflammatory response induced by fibrinolysis is associated with any subsequent complications (we did not observe such an effect, but our study is likely to have been underpowered). If so, then pharmacological strategies aimed at attenuating inflammation could perhaps be combined with fibrinolysis. For example, administration of the iron chelator deferoxamine has shown promise in preclinical models of both intracerebral hemorrhage and SAH.4,38 A recent animal study showed that injection of deferoxamine into the ventricles reduced hydrocephalus induced by iron. 42
The major strength of this study is the prospective, randomized, masked design, which minimizes the chance of bias. The main limitation is the relatively small sample size. However, despite limited statistical power, we were still able to show a clear increment in CSF cytokines and WBC counts after administration of TPA.
In summary, our results show that intraventricular TPA administration induces a transient rise in inflammatory cytokines in CSF, which appears to be related largely to the extent of fibrinolysis. If this inflammatory response is shown to be harmful, pharmacological strategies aimed at attenuating inflammation induced by liberation of blood breakdown products could conceivably have a therapeutic benefit if combined with intraventricular fibrinolysis.
DISCLOSURE/CONFLICT OF INTEREST
The authors declare no conflict of interest.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.