
Abstract
Experimental stroke treatment by mesenchymal stem cell (MSC) populations is an attractive paradigm in stroke research. There are many studies describing improved functional outcomes after MSC delivery in stroke, but the mechanisms through which the transferred cells exert these effects are less well understood. Moreover, commonly applied functional tests may not be suitable for discriminating real functional recovery from compensation, which is a frequently encountered phenomenon in rodents. This commentary highlights some of the potential risks for the translational process associated with these tests and proposes some alternative test arrays which may achieve more specific functional phenotyping.
Keywords
The therapeutic options in stroke are extremely limited and thus, much hope is placed on experimental treatments such as cell therapies. Mesenchymal stem cells (MSCs) represent an attractive option as these cells can be easily and safely derived from multiple sources such as bone marrow, adipose, and placental tissues. In addition, the excellent safety profile and low immunogenicity after allogeneic application may enable their use as an ‘off-the-shelf’ therapeutic product. It is thought that MSCs may improve brain repair through a number of mechanisms ranging from immuno-modulation to increased angio- and neurogenesis. 1 Whether the cells actually gain access to the brain after intravascular delivery remains an open question, 2 but paracrine secretion of neurotrophic factors is commonly believed to contribute to the observed therapeutic benefits. There is emerging evidence to suggest that cell-based therapies might promote functional recovery, but it is not completely understood how the cells exert these effects.
In their recent review article, Eckert et al 3 provided an excellent overview on the use of MSCs as a treatment of experimental stroke highlighting the outstanding translational relevance of the cells. Behavioral outcome was assessed in 39 out of the 46 studies reviewed, with 38 studies reporting significantly better outcomes with MSCs as compared with control treatment. Interestingly, therapeutic efficacy has been detected regardless of the MSC type, delivery route, or time of administration. The modified neurologic score point system (mNSS) was the most frequently applied behavioral test in the reviewed studies, followed by the adhesive tape removal test.
Hicks et al 4 analyzed common neuro-functional assessment strategies in cell-based studies after experimental stroke; their main conclusion was that many of the widely used behavioral tests, including mNSS, adhesive tape removal, and Rotarod, are prone to yield positive treatment effects. In addition, one should note that stroke animals may be suffering from severe loss of body weight or infections, and thus behavioral tests such as mNSS may merely measure the general well-being of animals, particularly during the first days after the surgery involved in experimental stroke induction. Therefore, the apparently improved mNSS scores by restorative therapies may be attributable to recovery from these complications rather than the restoration of sensorimotor functions per se, 5 particularly in studies with incomplete or even without any randomization.
Hicks et al 4 also postulated that the posttreatment behavioral improvement may be because of enhanced compensatory strategies rather than a true motor recovery. In reality, it is not clearly understood whether MSC-based therapies promote primarily functional recovery or behavioral compensation. Although compensation (e.g., by trunk rotation, or use of tail, or adjustment of body weight for balance) is recognized as a relevant con-founder in behavioral testing, it is challenging to eliminate its contribution to the results if one does pay attention to the quality of task performance. Moreover, rats may attempt to hide or overcome a motor impairment, an apparent evolutionary mechanism needed for defense, escape, and survival. To distinguish recovery from compensatory behavior, more demanding behavioral testing or kinematic analyses are required.
The extent to which compensation contributes to behavioral improvement promoted by restorative treatments has not been adequately studied. In their elegant work, Knieling et al 6 conducted a parallel quantitative (reaching success) and qualitative (movement pattern) analysis to evaluate the effect of an enriched environment in stroke-lesioned rats. They demonstrated that enriched environment improved behavioral outcome mainly through compensatory movements. This is similar to the situation in stroke patients, i.e., a recent study revealed that improvement after constraint-induced movement therapy appears to be mediated through compensatory strategies rather than by any decrease in impairment or a restoration of more normal motor control. 7
In general, any motor deficit compensation in human stroke survivors could be considered beneficial should it lead to a recovery of function for daily activities. However, it is far from clear whether compensation induced by experimental therapies in rodents will be observed to the same or even any extent in patients. Moreover, permitting the use of motor compensation can lead to a pattern of learned nonuse, limiting the capacity for subsequent motor function restoration in the paretic limb. Although compensatory movements may help patients to perform tasks in the short term, they can be associated with long-term problems such as reduced range of joint motion and pain. 8
We encourage researchers working with experimental cell or restorative therapies to select the kinds of behavioral tests which are minimally affected by repeated testing or by the appearance of compensatory strategies. This is the only way to prevent false-positive classification of apparently beneficial outcome results being interpreted as functional restoration. These tests include the tapered/ledged beam walking, the cylinder test, and Montoya's staircase which are relatively easy to perform and no more laborious than the standard mNSS or the adhesive removal test (Table 1).
Behavioral tests used to assess sensorimotor impairment with the relative amounts of time required to perform the task, time to analyze the task, and the sensitivity of the task for subjective scoring, compensation, or repeated testing
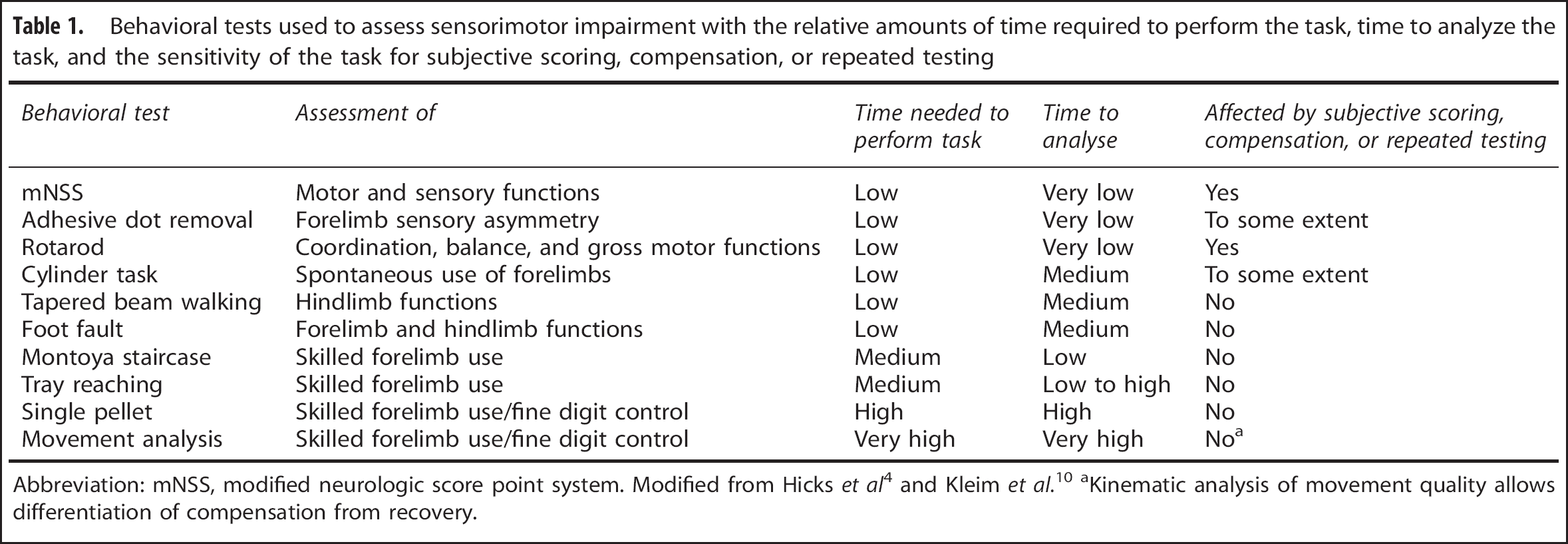
Abbreviation: mNSS, modified neurologic score point system. Modified from Hicks et al 4 and Kleim et al. 10
Kinematic analysis of movement quality allows differentiation of compensation from recovery.
To preserve and assure the translational value of experimental MSC stroke therapies, the treatment paradigm could include additional testing in old and/or comorbid animals. Another possibility would be to create stroke research networks collaborating to mimic clinical trial designs in multicenter preclinical studies. 9 Behavioral hands-on courses could be organized through such networks to train young scientists and to help in selecting test alternatives more appropriate at detecting ‘true’ recovery, so that experimental investigators can obtain reliable test results. Finally, we have to clarify the relevance of compensatory strategies for functional recovery in stroke survivors. Taken together, these measures can be anticipated to contribute to the prevention of future translational failures, i.e., therapies which appear to be promising in experimental stroke models failing to exert any beneficial effects in stroke patients.
Footnotes
The authors declare no conflict of interest.
ACKNOWLEDGMENTS
The authors thank the MEMS-IRBI consortium members and in particular Dr Miroslaw Janowski, for the stimulating scientific discussions and his expert input on this topic.
The MRI navigated Enhancement of Mesenchymal Stem Cell Homing Toward Stroke Lesion-Evaluating an Impact on Animal Recovery with Behavioral Testing and Imaging (MEMS-IRBI) consortium (in alphabetic order): Anna Andrzejewska; Dr Lili Cui; Dr Alexander Deten; Franziska Nitzsche; Dr Adam Nowakowski; Dr Daniel-Christoph Wagner; and Dr Piotr Walczak.