
Abstract
Although ischemic stroke is a major cause of morbidity and mortality, current therapies benefit only a small proportion of patients. Transplantation of mesenchymal stromal cells (MSC, also known as mesenchymal stem cells or multipotent stromal cells) has attracted attention as a regenerative therapy for numerous diseases, including stroke. Mesenchymal stromal cells may aid in reducing the long-term impact of stroke via multiple mechanisms that include induction of angiogenesis, promotion of neurogenesis, prevention of apoptosis, and immunomodulation. In this review, we discuss the clinical rationale of MSC for stroke therapy in the context of their emerging utility in other diseases, and their recent clinical approval for treatment of graft-versus-host disease. An analysis of preclinical studies examining the effects of MSC therapy after ischemic stroke indicates near-universal agreement that MSC have significant favorable effect on stroke recovery, across a range of doses and treatment time windows. These results are interpreted in the context of completed and ongoing human clinical trials, which provide support for MSC as a safe and potentially efficacious therapy for stroke recovery in humans. Finally, we consider principles of brain repair and manufacturing considerations that will be useful for effective translation of MSC from the bench to the bedside for stroke recovery.
INTRODUCTION
Stroke is the second most common cause of death 1 and a major cause of adult-acquired disability2–4 worldwide. The estimated direct and indirect costs of stroke are over $50 billion a year in the United States alone. 5 Currently, the only drug approved for the treatment of acute ischemic stroke is the thrombolytic drug recombinant tissue plasminogen activator (tPA).6,7 Unfortunately, the time window for therapeutic intervention with tPA is only 4.5 hours, and as a result only 1 in 20 patients with acute ischemic stroke currently receives this therapy in the United States. 8 Moreover, approximately half of the patients who do receive tPA for acute ischemic stroke and survive to day 90 have a significant long-term disability. As a result, there has been considerable interest in developing new treatment modalities to reduce disability from stroke. One area of increased focus has been restorative therapeutics, particularly the use of stem cells.
Mesenchymal stromal cells (MSC; also termed as mesenchymal stem cells or multipotent stromal cells) are adult non-hematopoietic pluripotent cells that have received considerable study as a cellular therapy due to their multiple modes of action that collectively respond to many of the fundamental pathologic events underlying stroke injury in the central nervous system (CNS).
9
The International Society for Cellular Therapy has defined human MSC based on three criteria:
1
adherence to plastic in standard culture conditions;
2
expression of surface antigens that include CD105, CD90, and CD73 (≥95% positive), but not CD34, CD45, HLA-DR, and other hematopoietic markers (≤2% positive); and
3
the ability to differentiate
This review will consider the extensive experience regarding MSC-based therapies, including their excellent safety profile in preclinical and human studies, with the focus being treatment of ischemic stroke, particularly in relation to stroke recovery. A key feature of MSC is that these cells have multiple mechanisms of action. This is somewhat of a paradigm shift in that most therapies are evaluated in relation to a single main mechanism of action. Stem cell therapies have multiple mechanisms of action and have nonetheless been considered to have great potential as stroke therapies.20,22–25 The current review extends previous reviews that examined the use of MSC to treat stroke by performing a systematic evaluation of preclinical MSC studies in stroke for the first time. These preclinical results are considered in relation to emerging human clinical trial results, as well as the underlying basic biology of MSC and ischemic stroke. The evidence that MSC have a favorable effect on functional outcomes in animal models, across a range of doses and therapeutic time windows, is compelling. In addition, topics important to successful translation of MSC from bench to bedside are considered, including points related to MSC manufacturing, patient stratification, and the time window for MSC therapy in human stroke.
THERAPEUTIC APPLICATIONS OF MESENCHYMAL STROMAL CELLS
Transplantations of MSC in human patients began in 1995, with most early trials focusing on potential benefits of autologous MSC in promoting the engraftment of hematopoietic stem cells in the setting of hematological malignancy.26,27 Early trials established a positive role for MSC in promoting hematopoietic stem cells engraftment and survival, which was supported by subsequent larger trials. 28 Bolstered by the lack of side effects in these early investigations, additional clinical trials investigated the utility of MSC in patients with Hurler syndrome, metachromatic leukodystrophy, and osteogenesis imperfecta. 28 These early trials were instrumental in both showing the safety of MSC transplantation in humans and establishing baseline criteria for design of MSC-based trials.
In the subsequent years, MSC have been investigated in the context of numerous diseases and disorders, in trials initiated around the world. Current ongoing trials are examining potential therapeutic roles of MSC in diseases ranging from amyotrophic lateral sclerosis to myocardial infarction to hepatic cirrhosis.
26
Due to the ability of MSC to differentiate into cardiomyocytes
Perhaps, the most encouraging and dramatic clinical application of MSC to date has occurred with graft-versus-host disease (GVHD). In up to 40% of children who receive allogenic bone marrow transplants, immune cells within the transplanted material may attack host’s cells. This leads to often life-threatening complications that are most often treated with immunosuppressive regimens, typically corticosteroids. 29 The immunomodulatory effects of MSC have generated significant interest in their potential to change the graft immune response in patients refractory to steroid-based treatments. In 2012, the MSC-based therapy Prochymal (Osiris Therapeutics) was approved for use in children with GVHD in Canada and New Zealand—the first approved stem cell treatment for systemic disease (outside of bone marrow transplants). In clinical trials, Prochymal showed clinically meaningful responses in 64% of patients. 21 This is particularly remarkable as the mortality rate of steroid-refractory GVHD can be as high as 85%. 29 The approval of MSC for treatment of GVHD emphasizes not only the safety of MSC, but also their potential to treat diseases that are refractory to current therapies. This long-term track record of safety combined with extensive clinical interest suggests that the therapeutic potential of MSC may soon be realized for multiple diseases.
MECHANISMS OF MESENCHYMAL STROMAL CELLS ACTION IN STROKE THERAPY
The experimental rationale for the use of MSC in stroke therapy includes a number of divergent mechanisms of action such as differentiation into cell types relevant to repair, modulation of the immune system, promotion of angiogenesis and neurogenesis, and secretion of neuroprotective and neurotrophic factors (Figure 1). Common to MSC effects in CNS and non-neural tissue is their ability to selectively target regions of injury. Numerous techniques have been used to gain insight into these mechanisms (Table 1). Understanding the relative contribution of each potential mechanism may be useful to optimize future clinical trial design.
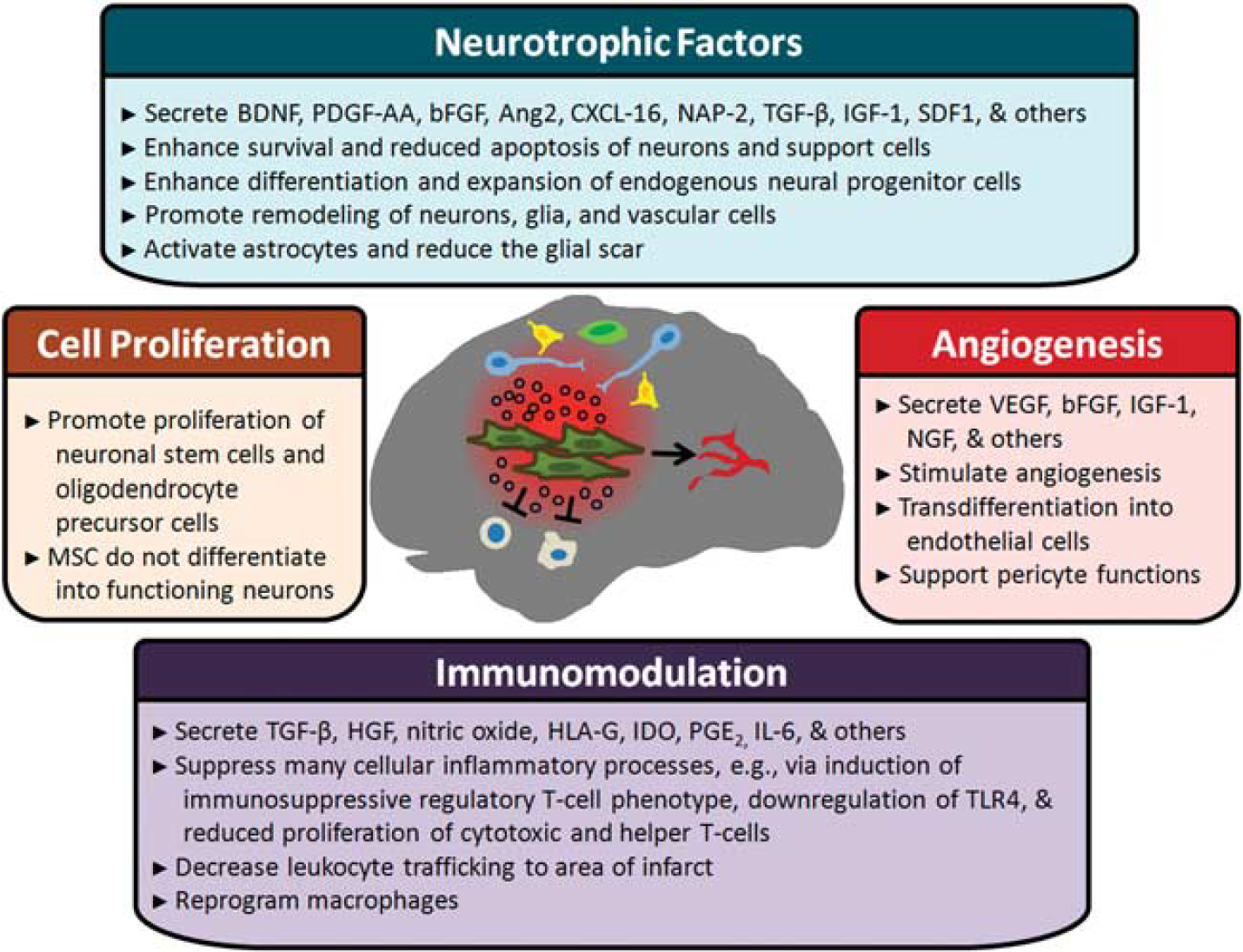
Overview of proposed mechanisms of mesenchymal stromal cells (MSC)-based stroke therapies. Important potential mechanisms mediating MSC action in stroke include secretion of neurotrophic factors,49,103–105,107,181,182 promotion of angiogenesis,114,183,184 and modulation of immune responses.60–63 Note that some of the factors secreted by MSC may have multifactorial roles, i.e., affect multiple pathways. Cell replacement is no longer thought to play a major role in the therapeutic effects of MSC in stroke; although transplanted MSC may express markers of neuronal lineage, there is no evidence that they are functional. In the figure, MSC are olive colored, neurons are blue, glial cells are yellow, neural progenitor cells are green, and immune cells are tan. BDNF, brain-derived neurotrophic factor; PDGF-AA, platelet-derived growth factor AA; bFGF, basic fibroblast growth factor; Ang2, angiopoietin 2; C-X-C motif, chemokine; CXCL-16, ligand 16; NAP-2, neutrophil activating protein 2; TGF-β, transforming growth factor beta; IGF-1, insulin-like growth factor 1; SDF-1, stromal cell-derived factor 1; NGF, nerve growth factor; HGF, hepatocyte growth factor; HLA-G, histocompatibility antigen class I G; IDO, indoleamine 2,3-dioxygenase; PGE2, prostaglandin E2; TLR4, toll-like receptor 4; VEGF, vascular endothelial growth factor; IL-6, interleukin 6.
Cell Replacement
Initial
Techniques and markers that provide insight into MSC mechanisms of action after stroke in animal models
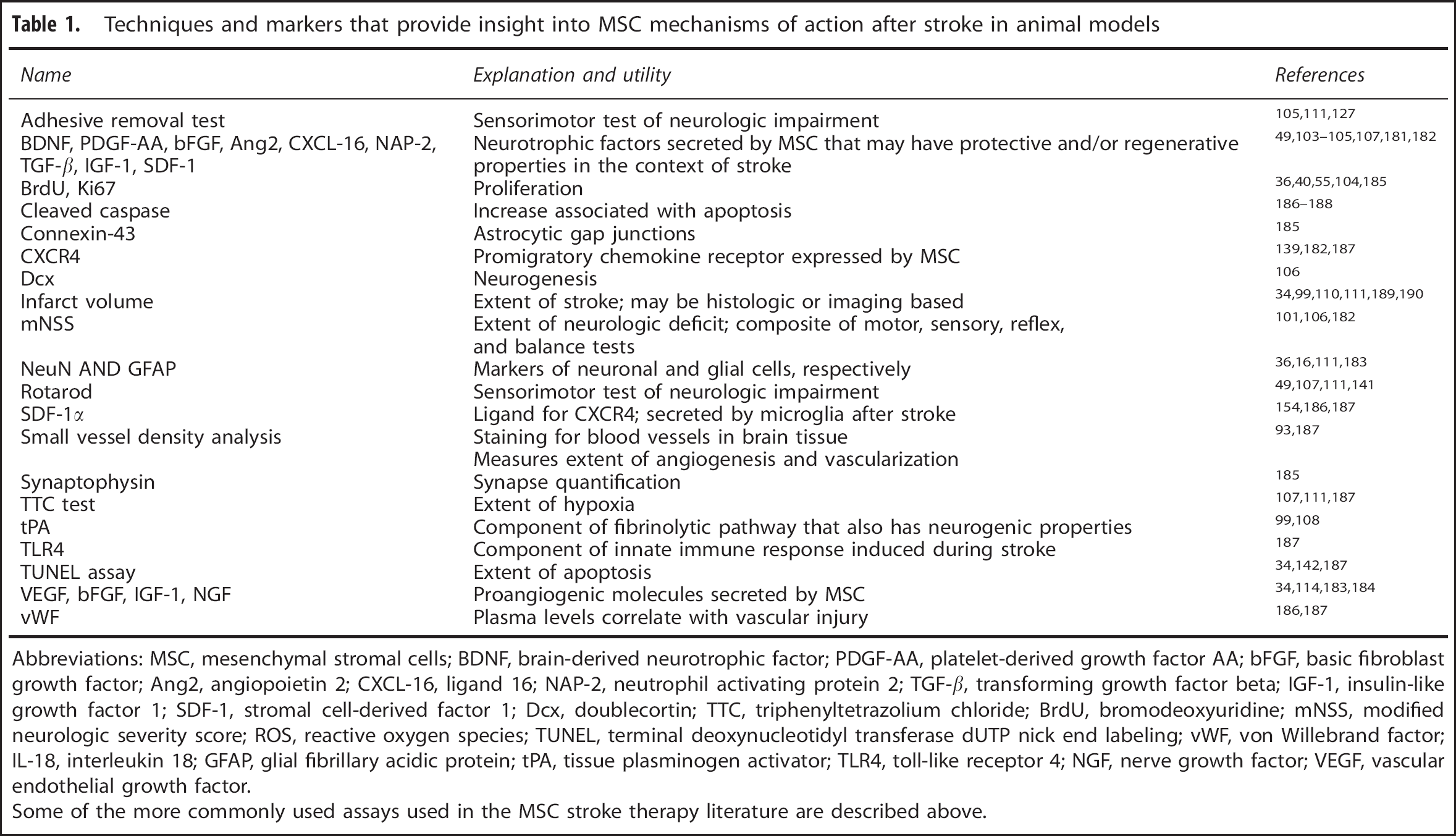
Abbreviations: MSC, mesenchymal stromal cells; BDNF, brain-derived neurotrophic factor; PDGF-AA, platelet-derived growth factor AA; bFGF, basic fibroblast growth factor; Ang2, angiopoietin 2; CXCL-16, ligand 16; NAP-2, neutrophil activating protein 2; TGF-β, transforming growth factor beta; IGF-1, insulin-like growth factor 1; SDF-1, stromal cell-derived factor 1; Dcx, doublecortin; TTC, triphenyltetrazolium chloride; BrdU, bromodeoxyuridine; mNSS, modified neurologic severity score; ROS, reactive oxygen species; TUNEL, terminal deoxynucleotidyl transferase dUTP nick end labeling; vWF, von Willebrand factor; IL-18, interleukin 18; GFAP, glial fibrillary acidic protein; tPA, tissue plasminogen activator; TLR4, toll-like receptor 4; NGF, nerve growth factor; VEGF, vascular endothelial growth factor.
Some of the more commonly used assays used in the MSC stroke therapy literature are described above.
Mesenchymal stromal cells may have a more indirect role in modulating changes in cell numbers after stroke, however, the effect of which is to promote recovery. Introduction of MSC after stroke is associated with increased cell proliferation in the subventricular and subgranular zones, suggesting mobilization of endogenous neuronal precursors.34,49,50 The MSC paracrine secretions (below) promote survival of some cells including neurons, and promote proliferation of other cells such as glia.51,52 The MSC can also limit secondary neurodegeneration after stroke.
53
Interestingly, MSC can both promote plasticity among damaged neurons and activate astroglial cells to induce secretion of neuroprotective molecules such as brain-derived neurotrophic factor and glial cell derived neurotrophic factor.54,55 The MSC robustly and specifically upregulate glial cell derived neurotrophic factor in astrocytes
Immunomodulation
Ischemic stroke induces a strong inflammatory response that leads to subsequent recruitment of leukocytes to the infarct zone.
59
Mesenchymal stromal cells are also immunomodulatory, in particular having been found capable of attenuating both innate and adaptive immune responses. They have well-characterized roles in regulating T cell-mediated processes by inhibiting T-cell proliferation, promoting a T-regulatory cell phenotype, and by exerting a non-specific suppressive effect on CD4 + and CD8 + T cells.60–63 In addition, exposure of MSC to cytokines such as interferon-γ promotes the immunoregulatory phenotype of MSC, leading to further suppression of T cells or natural killer cells.
64
Importantly, many of the effects that MSC have on the immune system are directly linked to the processes underlying neural repair after stroke. For example, MSC promote resolution of the poststroke inflammatory milieu that can impede repair, and can shift macrophage profiles to those that are more conducive to repair.68,71 A key feature of MSC transfusion is the remote effect these cells can have on immunologic function. For example, systemically administered MSC may be entrapped in the lung but have immunomodulatory effects on distant organs including the brain.72–74 Interestingly, the spleen is instrumental in mediating the systemic immune response to ischemic stroke; splenectomy leads to significantly reduced neurodegeneration and reduced immune response after middle cerebral artery occlusion (MCAO) in rats. 75 The dramatic accumulation of MSC in the spleen after intravenous administration hints at possible roles for systemic immunomodulation here,76,77 although this hypothesis has not yet been tested.
Mesenchymal stromal cells express HLA molecules at very low levels.78,79 As a result, MSC are immunoprivileged—their activity does not vary in relation to extent of MHC match between donor and recipient. Many of their immunomodulatory effects are therefore seen in both the autologous and allogenic setting, a feature that suggests broad therapeutic application. However, reports of immune responses stimulated by MSC suggest that this may be a relative rather than a absolute property,68,80 although MSC show no indication of immunologic sensitization in the brain when given after stroke. 72
Relatively few studies have directly investigated the effects of MSC on the immune response during stroke. Reductions in macrophage recruitment and activation of the innate immune response have been observed after stroke.22,81,82 The need for such studies is highlighted by the fact that MSC effects on the immune system can vary across levels of specific chemokine, disease settings, and species.83–86 This need is further underscored by the fact that, at least for MSC given in the initial days after stroke onset, any effects of MSC on the immune system must be interpreted in the context of the immunosuppressed state that arises after stroke.87,88
Angiogenesis
Angiogenesis within the infarct zone and the surrounding penumbra is thought to play a key role in mediating survival and regeneration of neurons after stroke. Mesenchymal stromal cells secrete a diverse array of cytokines, many of which are proangiogenic.86,89 Although the exact molecules may differ depending on cell source, secretion of vascular endothelial growth factor (VEGF), basic fibroblast growth factor, and placental growth factor have been repeatedly described.89–91 Interestingly, many angiogenic factors have additional neuroprotective roles. For example, VEGF not only induces angiogenesis, but is also anti-inflammatory and promotes the recruitment and differentiation of endogenous neuronal precursors.92–94 The broad effects of angiogenic molecules may therefore help explain the diverse therapeutic benefits of MSC in stroke. In addition, MSC possess many similarities to pericytes that may allow transplanted MSC to have additional roles relevant to neural repair poststroke such as maintenance of the vascular supply 95 and support of normal pericyte interactions with astrocytes and endothelia to maintain blood–brain barrier integrity. 96
Neurotrophic Factors
Mesenchymal stromal cells given after an experimental stroke have been found to secrete a wide number of neuroprotective and neurotrophic factors that promote repair and recovery through numerous pathways. Consistent with this, introduction of MSC-conditioned media reproduces many of the effects of direct MSC transplantation.97,98 The MSC thus serve as a delivery platform for a wide variety of secreted molecules, 97 acting synergistically and in parallel on multiple biologic pathways.
A number of factors secreted by MSC influence cell survival and proliferation after stroke. Stroke leads to necrosis and apoptosis of neurons, endothelial cells, and CNS glia. Studies have consistently found that MSC given after stroke reduce apoptosis and increase proliferation of several cell types including endogenous neural stem cells and glia.49,82,99,100 This likely occurs via both secretion of prosurvival and antiapoptotic factors and via indirect stimulation of CNS parenchymal cells to secrete neurotrophic, neuroprotective, and prooligodendrogenic factors,34,91,101,102 e.g., insulin-like growth factor 1, brain-derived neurotrophic factor, epidermal growth factor, and stem cell factor.49,54,103–107 A particularly important indirect effect of MSC in stroke may be induction of tPA in astrocytes, which both promotes neurite outgrowth and neuroprotection.99,108 MSC secretion of angiogenic factors such as VEGF may have additional roles in support of repair. 92 The result of these MSC activities includes increased neurogenesis, improved white-matter integrity, and synaptogenesis. 20
For other neurotrophic factors secreted by MSC, the main effect on stroke recovery is related to amplification of the molecular and cellular events 25 that underlie spontaneous recovery from stroke. Paracrine secretion of neurotrophic factors by MSC after stroke favorably influences numerous restorative brain events. 109 This was well summarized by Li and Chopp, 72 who described transplanted MSC as working like “small molecular factories’ by secreting neurotrophins, growth factors and other supportive substances after brain attack, which may continually produce therapeutic benefits in the damaged brain. The polypharmacies secreted from MSCs are potentially more important than any single factor to stimulate CNS repair”.
EFFECTS OF MESENCHYMAL STROMAL CELLS SOURCE AND DETAILS OF MANUFACTURE
Source of Mesenchymal Stromal Cells
The majority of animal studies of MSC transplantation in stroke have used bone marrow-derived MSC (BM-MSC), with a smaller proportion studying MSC derived from adipose tissue or the umbilical cord.110,111 Unfortunately, there have been relatively few studies directly comparing the relative efficacy of MSC derived from multiple sources in the setting of stroke. Ikegame
Mesenchymal stromal cells transplantation may be either autologous, in which the cells to be transplanted are derived from the eventual recipient, or allogenic, in which the source of cells is a genetically similar but not identical donor who is of the same species. Autologous transplantation has little risk of immunoreaction, but requires weeks to culture and expand cells for transplant,
113
which severely limits their use in the acute disease setting.
114
Furthermore, MSC derived from patients with chronic disease or advanced age, features common among patients with stroke, consistently exhibit reduced growth rates in culture.115,116 The fact that MSC are immunoprivileged suggests safety for an allogenic approach to MSC administration after stroke.
117
Clinical trials in human subjects with many different disease states have established that transplantation of allogenic MSC is safe.
118
Rodent models provide clear evidence for the functional benefits of allogenic MSC after stroke, with no significant difference in functional recovery between autologous and allogenic MSC in a head-to-head comparison when administered 3 hours after tMCAO.
119
In addition, a study in human subjects with chronic ischemic cardiomyopathy treated via transendocardial injection reported no major differences in safety or regenerative activity between autologous and allogenic MSC.
120
An important caveat is that one study found that MSC derived from rats that had undergone MCAO promoted significantly larger improvements in functional outcome and angiogenesis compared with rats treated with MSC derived from control rats.
121
This suggests that stroke may influence the expression of neurotrophic or angiogenic molecules in endogenous MSC
Details of Mesenchymal Stromal Cells Manufacture
From a broad perspective, issues related to MSC manufacturing could be of critical importance to successful translation of MSC to human trials. Studies in which MSC are given to human subjects must produce these MSC in accordance with Good Manufacturing Practice (GMP), 122 a standard that makes specific and rigorous demands on the materials, processing, documentation, quality assurance testing, release specification, process control, specimen storage, specimen transport, and other features of providing a therapeutic product appropriate for introduction into a human patient. The MSC produced outside of GMP conditions in a preclinical study might not have the same biologic activity, biologic purity, or biologic stability as compared with MSC produced in a GMP-compliant manner for a clinical trial. Differences in the details of manufacture could contribute to differences between preclinical and clinical studies in safety or in behavioral end points. To maximize the success of successful translation, it is critical for preclinical studies not only to report the tissue source and culture conditions, but also to provide detailed information regarding points of compliance with, and points of deviation from, GMP production.
A number of specific issues of MSC manufacture may also be important. Examples include the source of the tissue used to grow the MSC, the expansion rate, choice of culture media, culture conditions, storage conditions, and any transport conditions.123,124 The number of cell divisions and the number of times cells are replated (passage number) dramatically impact MSC potency and viability.125,126 For example, MSC that have undergone two passages improve stroke outcome more than MSC that have undergone six passages do, 127 and MSC that have undergone three passages have superior cardioprotective activity compared with MSC that have undergone five passages. 128 Mesenchymal stromal cells are most commonly grown in basal media supplemented with fetal bovine or calf serum. The precise makeup of these supplements can vary, and use of animal products introduces risk, e.g., of infection or allergic reaction, that while small has nevertheless prompted some investigators to develop xeno-free MSC culture methods. Some authors have studied human-derived sera, as well as media defined in relation to specific bioactive molecules such as transforming growth factor beta, platelet-derived growth factor, and basic fibroblast growth factor 2. 129 The utility of these alternative approaches is a topic of current study.130,131 A number of preclinical studies have modified MSC, e.g., by gene insertion, use of bioscaffolding, or addition of growth factors to culture medium, additional manipulations that could potentially improve MSC restorative effects as well as their safety profile.
PRECLINICAL STUDIES
Fate of Transfused Mesenchymal Stromal Cells
After stroke, MSC can be introduced locally, i.e., by direct injection into an affected brain region (intracerebral), or MSC can be transfused systemically, through the venous (IV) or arterial (IA) routes. The exact pattern of MSC distribution, however, varies with route of delivery.
Mesenchymal stromal cells are selectively attracted to sites of injury and inflammation.132,133 Tissues release numerous inflammatory cytokines after injury,134,135 and MSC express a variety of chemokine receptors.
136
Indeed, simply exposing MSC to hypoxia
Mesenchymal stromal cells are relatively large cells, with diameter 10 to 30 μm. 143 Not surprising, therefore, most MSC are passively entrapped in the lung vasculature after intravenous transfusion. 77 Histologic studies in healthy rodents given intravenous MSC found the MSC to be mainly distributed in lungs and liver at 3 hours; in lungs, liver, and spleen at 24 hours, in bone marrow, spleen, and lung over the next several days; and in bone marrow, spleen, lung, bone, cardiac and skeletal muscle, ear cartilage, and liver several months thereafter.144,145 After stroke, MSC also home to regions of brain injury; 72 in the brain, the majority are found in the ischemic core and its peri-infarct boundary zone. Mesenchymal stromal cells are predominantly eliminated by the kidneys. 77 One year after stroke, i.e., as far out poststroke as has been examined preclinically, most surviving MSC are found within the ischemic brain, with very few present in other organs. 146
These findings have been confirmed by whole body imaging of radiolabeled MSC given intravenously to rats with and without stroke due to MCAO. During the first 2 hours after stroke, MSC are transiently trapped in the lungs, and can be seen to increase within the region of brain ischemia. 77 Interestingly, the clearance and biodistribution of intravenous MSC resembles that of inert microparticles: an initial accumulation in the lungs followed by gradual clearance over a period of days to a week. 147
The exact distribution of MSC differs according to route of administration.76,148 Introduction of MSC via the intraarterial or the intracerebral route reduces avoids first-pass pulmonary effects and so results in fewer MSC in the lung, but these approaches are more invasive and so introduce specific risks.149,150 It remains to be determined whether differences in MSC distribution in relation to route of administration are associated with significant differences in safety or in efficacy of treating stroke recovery.
PRECLINICAL STUDIES OF MESENCHYMAL STROMAL CELLS SAFETY AND EFFICACY FOR PROMOTING STROKE RECOVERY
A systematic search of PubMed and Web of Science identified preclinical studies of MSC in the setting of experimental ischemic stroke. Studies of MSC that have been modified, e.g., genetically or via a bioscaffold were excluded. A total of 46 studies reporting 61 different MSC treatment arms were identified. In 39 of these, behavioral functional outcomes were reported; all but 1 of these 39 found significantly better functional outcomes with MSC as compared with control (see Supplementary Table and References). There has been a dramatic increase in the number of preclinical MSC studies in recent years. The use of MSC to promote stroke recovery has been found safe.
These favorable effects of MSC on functional recovery were robust across rodent and primate species, route of delivery (intravenous, intraarterial, and intracerebral), type of MSC (allogenic versus autologous), time of administration in relation to stroke (from 5 weeks before to 1 month after stroke), and MSC dosage (from 1 × 10 4 to 3.25 × 10 7 cells, i.e., 36.3 cells/g to 1.3 × 10 5 cells/g). Effects were also consistent across species of MSC origin, with studies showing favorable behavioral effects with MSC derived from rat in 24 studies, human in 16, and mouse in 6 studies.
These findings indicate that in animal models of stroke, MSC exert therapeutic effects over a wide dose range, may be administered as late as 1 month after cerebral ischemia, and may be beneficial regardless of cell source or route of delivery. Importantly, the retained efficacy of MSC when given to animals 30 days after stroke 146 mitigates concerns that the time needed to expand MSC in culture for autologous MSC therapy (e.g., 2 to 3 weeks) could be an impediment to this approach after stroke, should this issue be of interest.
Several clinical aspects of stroke could have an important influence on efficacy of MSC in stroke recovery in humans. Few preclinical studies have examined these issues. Several studies have examined the functional effects of MSC in aged rodents (retired Wistar breeder rats) and found evidence of significant improvement in behavioral outcomes as well as in increased proliferation and neurogenesis.105,106 Similarly, a study found that in spontaneously hypertensive rats, MSC effectively homed to the ischemic lesion, although behavioral outcomes were not examined. 33 Conversely, intravenous administration of MSC 24 hours after MCAO in streptozotocin-induced diabetic rats led to significantly worse functional outcome, including mortality, compared with non-diabetic rats. 151 The authors observed elevated levels of angiogenin and increased blood–brain barrier leakage in the brain of diabetic mice that received MSC, which they speculate led to the adverse effects of MSC. Future preclinical studies can expand on this experience, for example, by examining how MSC effects interact with various forms of rehabilitation or commonly used pharmacological therapies after stroke, or by comparing MSC effects across different forms of stroke as captured by divergent stroke models. The observation of adverse effects of MSC in streptozotocin-induced diabetic rats emphasizes that, as with any new potential therapy, the impact of comorbidities must always be considered, although it must be appreciated that 2 weeks of poststreptozotocin hyperglycemia 151 only models a small fraction of the components of years of diabetes mellitus. 152 Understanding the influence that these and other variables can have on the therapeutic effects of MSC after stroke will be important to identify characteristics of those patients most likely to benefit from MSC, and to understand the fundamental limitations of MSC in the treatment of stroke therapy.
CLINICAL TRIALS IN ISCHEMIC STROKE
Based on the encouraging results of preclinical studies of MSC after stroke, the excellent safety profile of MSC in non-stroke human studies, and the potential advantages of MSC in relation to other cellular therapies (e.g., can be derived from multiple sources, immunoprivileged), significant interest in the application of MSC to stroke treatment is emerging. An overview of completed and ongoing clinical trials of MSC in stroke appears in Tables 2 and 3. Importantly, all completed trials have investigated the utility of MSC at relatively late time points, i.e., at least 23 days after stroke. This underscores the fact that trials enrolling patients >23 days after stroke are focusing on restorative targets, an important distinction as compared with stroke trials that enroll patients in the early hours after stroke and use interventions that focus on reducing acute injury via reperfusion or neuroprotective targets. This issue is considered in greater detail in the following section.
The first report of MSC transplantation in stroke patients was performed by Bang
Honmou
Taken together, these data provide preliminary support for the idea that intravenous transfusion of MSC in patients with chronic stroke is safe and might improve quality of life. It is also important to note that the paucity of preclinical data examining the effects of MSC introduced >30 days after stroke onset. A major disparity thus exists in MSC study design between the body of published preclinical studies and completed human trials, in relation to the number of days poststroke when MSC were introduced; this may be reasonable for initial safety studies but will become increasingly important in later phase studies.
A number of guidelines have been published that could maximize the effectiveness with which MSC are translated to human clinical trials. The Stem Cell Therapy as an Emerging Paradigm for Stroke (STEPS) committee158,159 provided a series of recommendations regarding both preclinical and clinical research into stem cell-based therapies for ischemic stroke, including the necessity of validated animal experiments, robust safety studies in humans, and the importance of selecting appropriate time points and patient populations for clinical trials. In particular, they suggested three areas of research that would advance the field: (1) development of cell labeling techniques that are safe and reliable for clinical testing, (2) identification and validation of surrogate markers of stroke recovery, and (3) formation of a stroke recovery imaging consortium to develop imaging end points for stroke clinical trials. Research into all of these areas would clearly also have enormous benefits for understanding the role of MSC in ischemic stroke therapy. Other guidance comes from the Stroke Treatment Academic Industry Roundtable (STAIR) publications, which in addition to providing recommendations regarding the design of preclinical and clinical restorative stroke studies, recommended a focus on treatments with multiple mechanisms of action as well as treatments that targeted systems outside the brain, such as the immune system.160,161 The diverse mechanisms of action of MSC coupled with their potent immunomodulatory functions suggest that they will be promising candidates for future ischemic stroke therapies.
Other clinical trials investigating the safety and efficacy of both allogenic and autologous MSC transplant are ongoing, at multiple study sites (Table 2), some introducing MSC at earlier time points poststroke than currently published studies. Importantly, most of the trials are using stroke-specific measurements of neurologic recovery and are also investigating the role of dosage in therapeutic efficacy. In addition, one of the trials is investigating the safety and efficacy of MSC grown under hypoxic conditions in ameliorating stroke symptoms, with the rationale being that hypoxia better preconditions these MSC to the microenvironment of the infarcted brain. Several of the trials are using proprietary stem cell formulations, including Athersys’ Multistem® product and SanBio’s MSC modified to express Notch. Celgene is also examining the safety and efficacy of PDA001, a placenta-derived stem cell product that may be similar to MSC, for safety and efficacy in a wide variety of stroke settings. These trials in particular will be instrumental in understanding the safety and utility of modifying MSC for stroke therapy. Results from these initial trials will provide needed data on the potential role of MSC-based therapy for cerebrovascular disease in humans.
Active clinical trials of MSC in human subjects with ischemic stroke
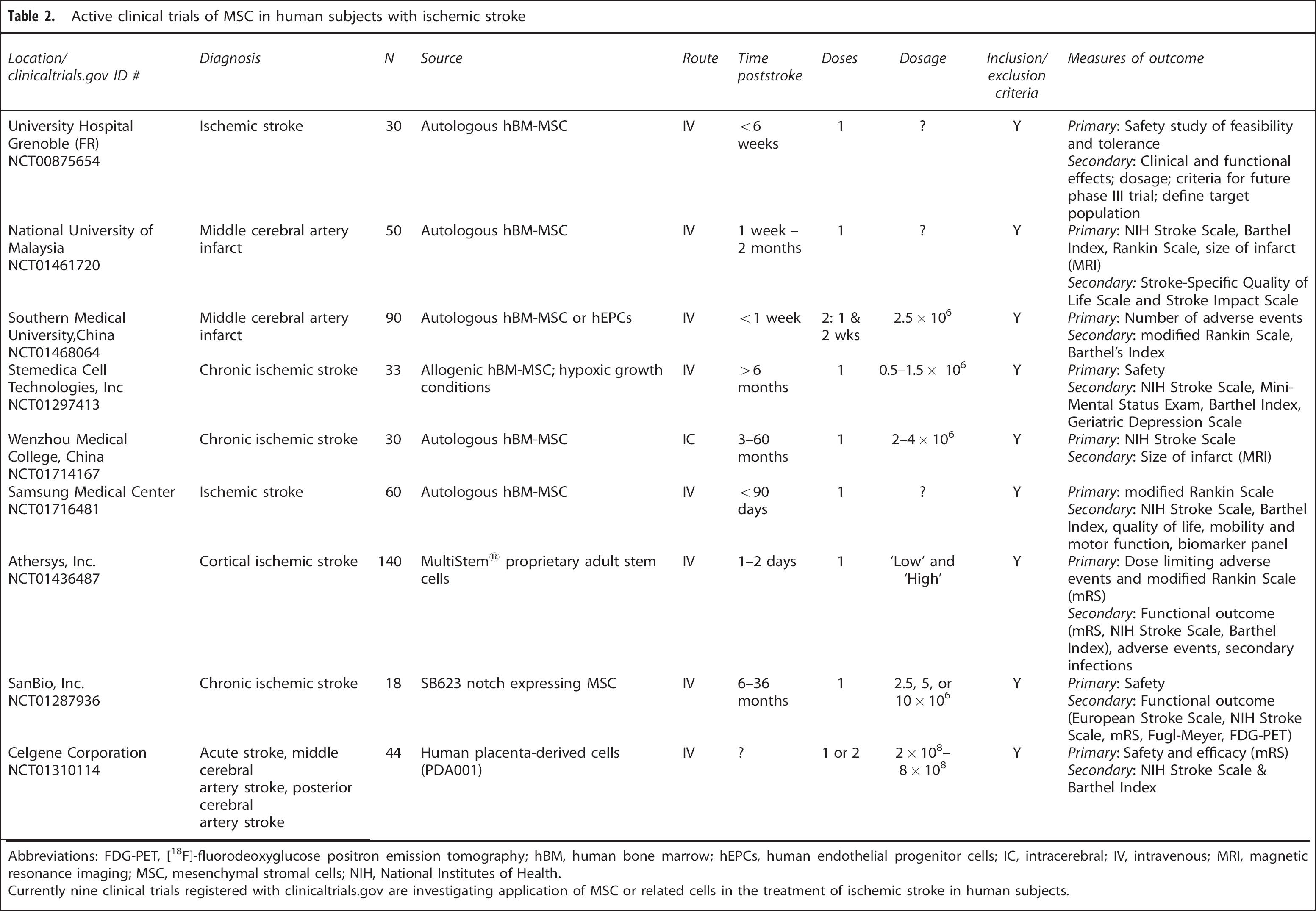
Abbreviations: FDG-PET, [ 18 F]-fluorodeoxyglucose positron emission tomography; hBM, human bone marrow; hEPCs, human endothelial progenitor cells; IC, intracerebral; IV, intravenous; MRI, magnetic resonance imaging; MSC, mesenchymal stromal cells; NIH, National Institutes of Health.
Currently nine clinical trials registered with clinicaltrials.gov are investigating application of MSC or related cells in the treatment of ischemic stroke in human subjects.
Completed clinical trials of MSC therapy in human subjects with ischemic stroke
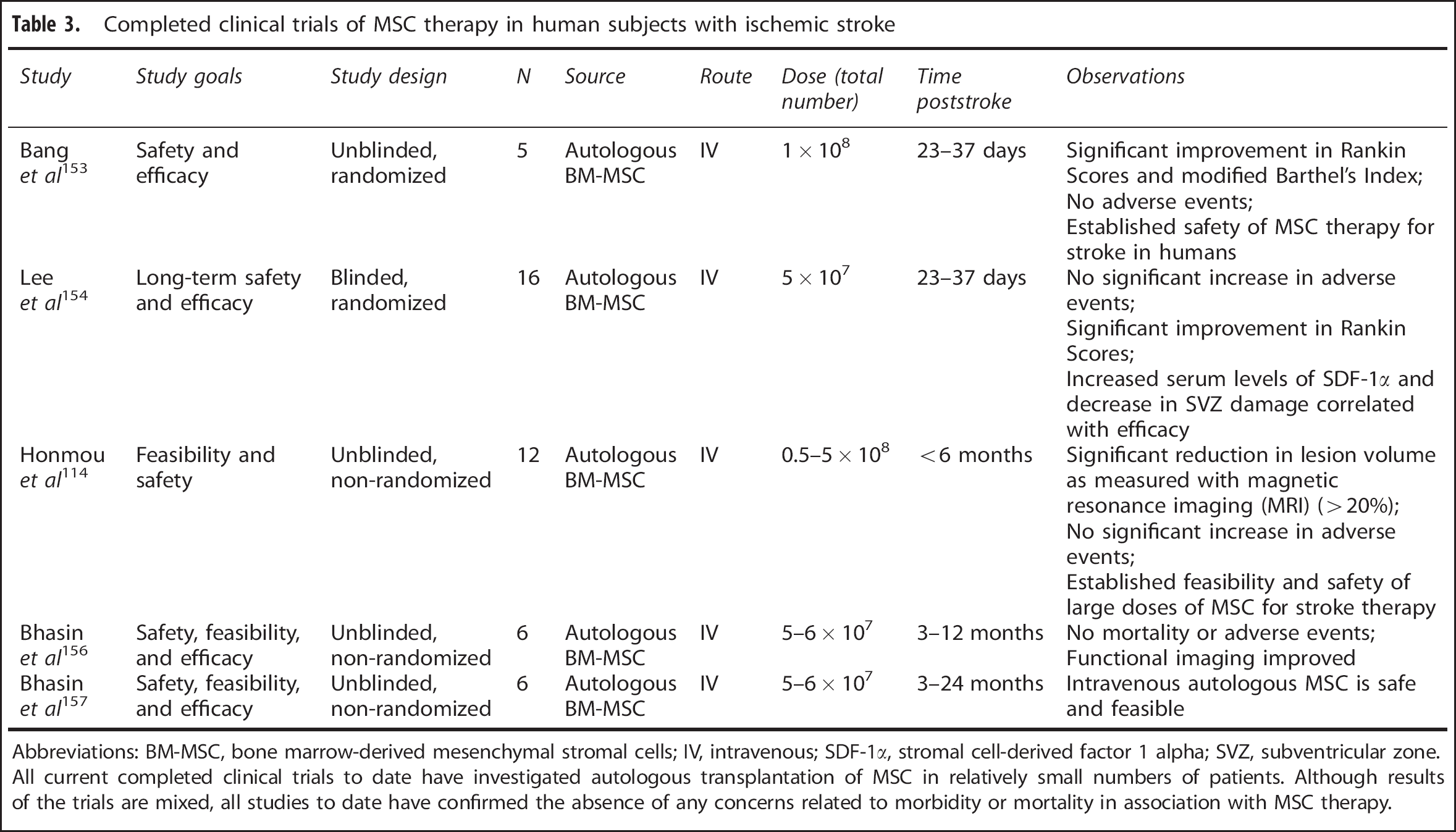
Abbreviations: BM-MSC, bone marrow-derived mesenchymal stromal cells; IV, intravenous; SDF-1α, stromal cell-derived factor 1 alpha; SVZ, subventricular zone. All current completed clinical trials to date have investigated autologous transplantation of MSC in relatively small numbers of patients. Although results of the trials are mixed, all studies to date have confirmed the absence of any concerns related to morbidity or mortality in association with MSC therapy.
MESENCHYMAL STROMAL CELLS FOR STROKE RECOVERY AND PRINCIPLES OF BRAIN REPAIR
Treatment of cerebrovascular disease encompasses a number of different arenas, each with its own strategies. These include stroke prevention, acute reperfusion, and the focus of the current review, restorative therapy. A number of guiding principles for designing poststroke restorative therapeutics have emerged from preclinical research and human studies.46,162 Consideration of these principles stands to strengthen emerging trials examining MSC as a restorative stroke therapy.
One key principle to consider is the time sensitivity of stroke therapeutic windows. This is a topic common to acute and restorative stroke therapies: in the setting of acute stroke, neuroprotective drugs and reperfusion therapies are known to have specific therapeutic time windows. The same is true in the setting of brain repair after stroke, where biologic targets and so response to therapy change with time.163,164 Preclinical data for MSC suggest that efficacy may change in relation to the time of treatment after stroke. 72 There are limited preclinical data for MSC initiated > 30 days after stroke onset, and it cannot be assumed that the biologic targets present in the first week poststroke remain months or years later. Other lessons from the experience of translating acute stroke therapies165–167 inform the design of MSC clinical trials; for example, having human trials match preclinical data as closely as possible, such as for treatment time window and route of administration. Maximum communication and iterative interactions between preclinical scientists and persons designing translational trials are important.45,168
A second principle is the need to stratify patients with stroke to maximize study power and the likelihood of detecting a treatment effect in a clinical trial.
169
This is also a topic that is relevant to both acute and restorative stroke therapies. Stroke is an extremely heterogeneous clinical diagnosis, patients differ in numerous important ways, and these differences can influence the likelihood that treatment will improve outcome. In the acute stroke setting, much focus has been on identifying ischemic penumbra with methods such as diffusion-perfusion magnetic resonance imaging mismatch. Clinical trials of MSC as a restorative therapy after stroke will have maximum likelihood of identifying treatment effects if patients are selected, or stratified, such that enrollees have sufficient biologic target to derive a benefit. This is an area of active research, and the optimal choices such as entry criteria will likely vary according to particulars of each trial, but two general guiding principles can be considered. First, enrolling patients whose clinical features are aligned with those reported in the positive preclinical studies increases the likelihood that the trial will identify a treatment effect. This point was illustrated in the analysis of a recent restorative stroke trial of cortical stimulation, where preclinical studies found that stimulation improved motor deficits after stroke but a phase III randomized controlled clinical trial in humans failed to detect a difference in motor outcome between study groups. Each of the preclinical studies in rodents and primates required preserved physiologic integrity of the motor system, but the clinical trial did not. A
A third principle is that brain repair is experience dependent. This is a point where acute stroke and restorative stroke therapies differ sharply. Therapy given in the setting of acute stroke, such as intravenous tPA, does not require any specific behavioral experience to achieve efficacy. In the restorative stroke setting, however, evidence suggests that treatment efficacy varies with behavioral reinforcement. An early demonstration of this point was by Feeney
A fourth principle is the potential value of using modality-specific measures. 180 This point is likely of greater importance to restorative stroke trials than acute trials. Of course, achieving gains in global measures of clinical status is important to both acute and restorative stroke therapies. However, restorative therapies such as MSC achieve their effect by promoting plasticity, and trials are more likely to show treatment effects in those brain networks that have sustained subtotal injury—a behavior whose underlying brain networks are destroyed by stroke is less likely to show treatment-related gains than a behavior for which the underlying networks are accessible to treatment. A neurologic modality for which the neural underpinnings are partially spared, such as gait or arm motor function or language, might show significant gains from treatment while global outcome measures, which reflect treatment effects across many brain networks, might show only modest effects.
CONCLUSIONS AND PERSPECTIVES
Mesenchymal stromal cells are remarkable cells with high potential for treating a wide variety of human disease targets, including stroke recovery. Several features make MSC particularly attractive as a therapeutic candidate, including inherent multipotency; ability to promote repair through multiple avenues in parallel such as immunoregulation, angiogenesis, and neurogenesis; their availability from multiple potential sources; and their immunoprivileged status. A large number of diverse preclinical studies have consistently showed that MSC safely improve behavioral outcome after stroke, and initial human trials are encouraging. Additional basic and preclinical research, including efforts to understand the mechanisms of action most important to MSC effects, will provide a fuller understanding as to how to best apply MSC to improve outcome after stroke. Studies in human subjects are needed, as well, for example, because the human experience of stroke is influenced by factors not easily examined in animals, such as psychosocial factors, and human neuroanatomy and vascular anatomy differ from animal models in ways important to MSC biology. Such studies will greatly inform key issues such as selecting the patient population most likely to derive benefit, or defining the optimal time, dose, and route for introducing MSC after stroke. The current preclinical and clinical experience supports the value of continued translation of MSC as a restorative therapy for stroke.
DISCLOSURE/CONFLICT OF INTEREST
Steven Cramer has served as a consultant to GlaxoSmithKline, Pfizer/Cogstate, and Microtransponder.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.