
Abstract
Recently, two randomized controlled phase II studies showed that acute initiation of statin treatment directly after aneurysmal subarachnoid hemorrhage (SAH) decreases the incidence of radiologic vasospasm and clinical signs of delayed cerebral ischemia (DCI), and even reduces mortality. It was hypothesized that the beneficial effect resulted from pleiotropic effects of statins. The purpose of this study was to investigate the biologic effects of acute statin treatment in patients with SAH. We performed an exploratory single-center, prospective, randomized, double-blind, placebo-controlled trial. Patients were randomized to simvastatin 80 mg or placebo once daily. A total of 32 patients were included. There were no statistically significant differences in clinical baseline characteristics. With regard to primary outcomes, there were significant differences by treatment group for total cholesterol and low-density lipoprotein (LDL) cholesterol (
Introduction
Patients surviving aneurysmal subarachnoid hemorrhage (SAH) are at risk of delayed cerebral ischemia (DCI). Currently, the only drug that decreases the incidence of DCI is the calcium channel blocker nimodipine (Rinkel et al, 2005). As the risk reduction of nimodipine is modest, intense efforts are made worldwide to find new treatments for this complication.
Recently, two randomized controlled phase II studies showed that acute initiation of statin treatment directly after aneurysmal SAH decreases the incidence of radiologic vasospasm and clinical signs of DCI, and even reduces mortality in patients already treated with nimodipine (Lynch et al, 2005; Tseng et al, 2005, 2007a). The results were remarkable, as the trials were not powered to detect differences in clinical outcome. As DCI is associated with increased morbidity and mortality after SAH (Rabinstein et al, 2004) and the observed risk reductions as a result of acute statin treatment were large, many neurocritical care units decided not to await the results from phase III trials and to implement statin treatment in their SAH management protocol (Kramer et al, 2008). However, several other studies found no effect of statin treatment in patients with SAH (Chou et al, 2008; Kramer et al, 2008; Singhal et al, 2005; Kerz et al, 2008). For example, no beneficial effect was observed in a recent double-blind, placebo-controlled pilot study (Chou et al, 2008). Furthermore, a recent retrospective study showed that after implementation of statins in the routine treatment of SAH patients, the rate of radiographic vasospasm, symptomatic vasospasm, delayed cerebral infarction, and outcome did not change compared with patients who were treated before alteration of the treatment protocol (Kramer et al, 2008). Earlier, a case-control study investigating 514 SAH patients of whom 36 used statins at the moment of SAH neither showed an effect of statins (Singhal et al, 2005). Moreover, even an increased incidence of radiologic vasospasm, but not of symptomatic vasospasm, was observed in patients treated with statins. However, as only 17 out of 36 patients continued statin treatment during hospitalization, a rebound effect could not be ruled out. A recent case-control study found an increased incidence of DCI in patients treated with statins (Kerz et al, 2008). Therefore, there is considerable doubt on the effects of statin treatment in this group of patients. Moreover, the mechanism by which statins can decrease DCI in SAH patients also remains to be elucidated. Clearly, additional studies are needed to investigate the effect of acute statin treatment on DCI and outcomes in patients with SAH.
The purpose of this study was to investigate the biologic effects of acute statin treatment in patients with aneurysmal SAH. If biologic effects are found which may explain the earlier observed beneficial effects of treatment with statins, this would support the use of statins in SAH patients. In addition, this would provide more insight into the pathogenesis of DCI.
Materials and methods
We performed a single-center, prospective, randomized, double-blind, placebo-controlled trial. The study protocol was approved by the local Institutional Review Board (IRB 06/33). This trial is registered in the International Standard Randomised Controlled Trial registry (ISRCTN45662651).
Patients
All patients with symptoms and signs of SAH with evidence of an aneurysmal bleeding on the initial computed tomography (CT) scan were eligible for the study. If CT scan was negative but lumbar puncture showed evidence of bleeding in the cerebrospinal fluid, patients were still eligible for inclusion if CT angiography or conventional angiography showed an aneurysm. Patients with a non-aneurysmal pattern of bleeding on the initial CT scan were only eligible for inclusion if (CT) angiography showed an appropriate aneurysm. Exclusion criteria were as follows: (1) under 18 years of age; (2) patients using aspirin, warfarin, and/or statins; (3) contra-indication for simvastatin (active liver disease, liver alanine aminotransferase or aspartate aminotransferase more than three times the normal upper limit, myopathy); (4) kidney insufficiency (defined as serum creatinine more than twice the normal upper limit, or patients requiring dialysis); (5) pregnancy or lactation; and (6) if death appeared imminent. All patients received standard care including treatment with nimodipine 360 mg a day orally (60 mg every 4 h). Initiation of hypertension and hypervolemia therapy was at the discretion of the treating neurosurgeon, according to the Academic Medical Center Subarachnoid Hemorrhage Treatment guidelines to which all neurologists, neurosurgeons, and intensive care physicians adhere.
Clinical Baseline Characteristics
At baseline, several characteristics were recorded, such as age, sex, Glasgow Coma Scale, the presence of focal neurologic deficits, loss of consciousness during ictus, warning leak, blood pressure at admission, smoking, history of hypertension, and location of aneurysm.
Randomization and Drug Administration
The randomization plan was developed by the local Department of Clinical Pharmacy, using permuted-block randomization (random number tables). Study medication was designed according to Good Manufacturing Practice (GMP) guidelines. Simvastatin and placebo were packed in identical capsules. Medication was available in numbered treatment boxes containing capsules for a complete 15-day course of simvastatin or placebo. As soon as the diagnostic inclusion criteria were fulfilled and written informed consent was obtained from the patient or a legally acceptable surrogate, the patients were randomized to receive oral simvastatin 80 mg or placebo once daily. Randomization and subsequent start of study medication had to take place as soon as possible, but never later than 72 h after SAH. Study treatment was continued until day 14 after SAH (the day of the hemorrhage was defined as day 0). In case of good clinical condition and hospital discharge before day 14 after SAH, patients were asked to continue the study medication at home and to return the treatment box by mail. All clinicians, nurses, patients, and investigators were blinded for study treatment. Unblinding of the treatment codes was carried out 6 months after the inclusion of the last study patient. All outcome assessments were carried out before the treatment codes were broken.
Blood Samples
Study blood samples were taken within 72 h after arrival in the hospital before the initiation of study medication, and at 4 ± 1, 7 ± 1, 10 ± 1, 14 ± 1, and 17 ± 1 days after SAH. All blood withdrawals were carried out by the same investigator (MDIV). In case of hospital discharge before day 17 after SAH, patients did not return to the hospital for the remaining blood withdrawals. All blood withdrawals were taken between 0800 and 0930 hours because of diurnal fluctuations of certain parameters such as plasminogen activator inhibitor (PAI)-1 antigen. After withdrawal, blood was directly processed and stored in a −80°C freezer until laboratory tests were carried out, which occurred after all patients were included in the trial.
To investigate the biologic effects of simvastatin, we studied both cholesterol-dependent (total serum cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides) and cholesterol-independent, so called pleiotropic, effects. With regard to pleiotropic effects, we studied parameters of fibrinolysis (tissue-type plasminogen activator (tPA) antigen, tPA activity, PAI-1 antigen, PAI-1 activity,
Measurements of tPA antigen (Innotest, Hyphen BioMed, Andrésy, France), PAI-1 antigen (Hyphen BioMed), vWF antigen (antibodies from Dako, Glostrup, Denmark), sTM (Asserachrom, Roche, Almere, The Netherlands), and prothrombin fragment F1 + 2 (Dade Behring, Marburg, Germany) were carried out by ELISA. Plasminogen activator inhibitor-1 activity was determined using Berichrom PAI-1 (Dade Behring) on a Behring Coagulation System (Dade Behring). Tissue-type plasminogen activator activity was determined in Stabilyte plasma by an indirect two-stage enzymatic procedure (Biopool, Umea, Sweden).
Transcranial Doppler (TCD) examinations were carried out for both anterior and middle cerebral arteries on the same day of study blood withdrawals. All TCD examinations were carried out by the same investigator (MDIV). Maximum and mean blood flow velocities (
Definition of Events
An event was defined as the occurrence of focal neurologic impairment and/or a decreased level of consciousness of at least 2 points as recorded on the Glasgow Coma Scale. Events were distinguished in rebleeding, DCI, hydrocephalus, and other events as follows: (1) rebleeding events were defined as sudden clinical deterioration with increased hemorrhage on CT scan compared with earlier CT imaging or autopsy finding, or no CT scan or autopsy showing sudden deterioration or death suspect for rebleeding. (2) DCI events were gradual deterioration or death with infarction on CT scan compatible with clinical presentation or proven at autopsy, or no CT scan or autopsy showing gradual deterioration suspect for infarction after exclusion of other causes by appropriate laboratory studies. (3) Hydrocephalus was defined as an event with CT-proven hydrocephalus. Other causes of clinical deterioration, such as pneumonia, coiling related complications, and operative complications (other than ischemia), were also recorded. Events were scored by one investigator (MDIV), and in case of uncertainty discussed with another investigator (YBWEMR).
Outcomes
Primary outcome was the effect of simvastatin on laboratory parameters of endothelial function, fibrinolysis, coagulation, inflammation, and cholesterol after aneurysmal SAH. Secondary outcomes were the occurrence of TCD vasospasm, the occurrence of clinical signs of DCI after SAH, and outcome on the Glasgow Outcome Scale 3 and 6 months after SAH. Poor outcome was predefined as Glasgow Outcome Scores ‘dead,’ ‘persistent vegetative state,’ and ‘severe disability.’ Favorable outcome was predefined as ‘moderate disability’ and ‘good recovery,’ Furthermore, the reason of poor outcome was scored.
Statistical Analysis
As the main purpose of our study was to investigate the biologic effects of statins in patients with aneurysmal SAH, the study had an exploratory design and no sample size calculation was carried out. Clinical baseline characteristics were summarized using descriptive statistics. The analyses involved all randomized patients irrespective of duration of treatment, timing of coiling or operation, etc. (intention-to-treat principle).
For the primary outcome analyses, the difference in development of laboratory markers by treatment group was investigated by random effects models. In these models, the parameters that describe the trend were allowed to differ per individual. The parameters per individual (the intercept, slope, and possibly quadratic term) were assumed to originate from a multivariate normal distribution. The mean of this distribution yielded the average development at the group level. For all ILs, there were many values below the detection limit of 2.5 pg/mL. For these models, a random effects logistic regression was carried out, with a value above or below the detection limit as an outcome variable. For all other markers, a suitable transformation was carried out to make the values more symmetrically distributed, after which a linear random effects model was fitted. The general regression strategy was as follows: For total cholesterol and LDL cholesterol, a polynomial trend over time was assumed, which was allowed to differ by treatment group. For all other markers, an intercept and a slope parameter were included in the model, which was allowed to differ by treatment group. If the trend parameter (slope or polynomial trend) did not differ significantly by treatment group, it was excluded from the model. Analyses were carried out with the nlme and lme4 packages in the R statistical program (R Development Core Team, 2008). For the primary outcome analyses, a
For the secondary outcome analyses, we calculated relative risks and used χ2 and Fisher's exact tests when appropriate to analyze differences in the outcome parameters between the treatment groups. Fisher's exact test was used when an expected cell value was < 5. The Mann-Whitney
Results
During the study period from May 2006 until August 2007, 75 patients with a bleeding pattern suggestive for aneurysmal SAH were screened for study eligibility. Reasons for exclusion are listed in Figure 1. In total, 32 patients were included.
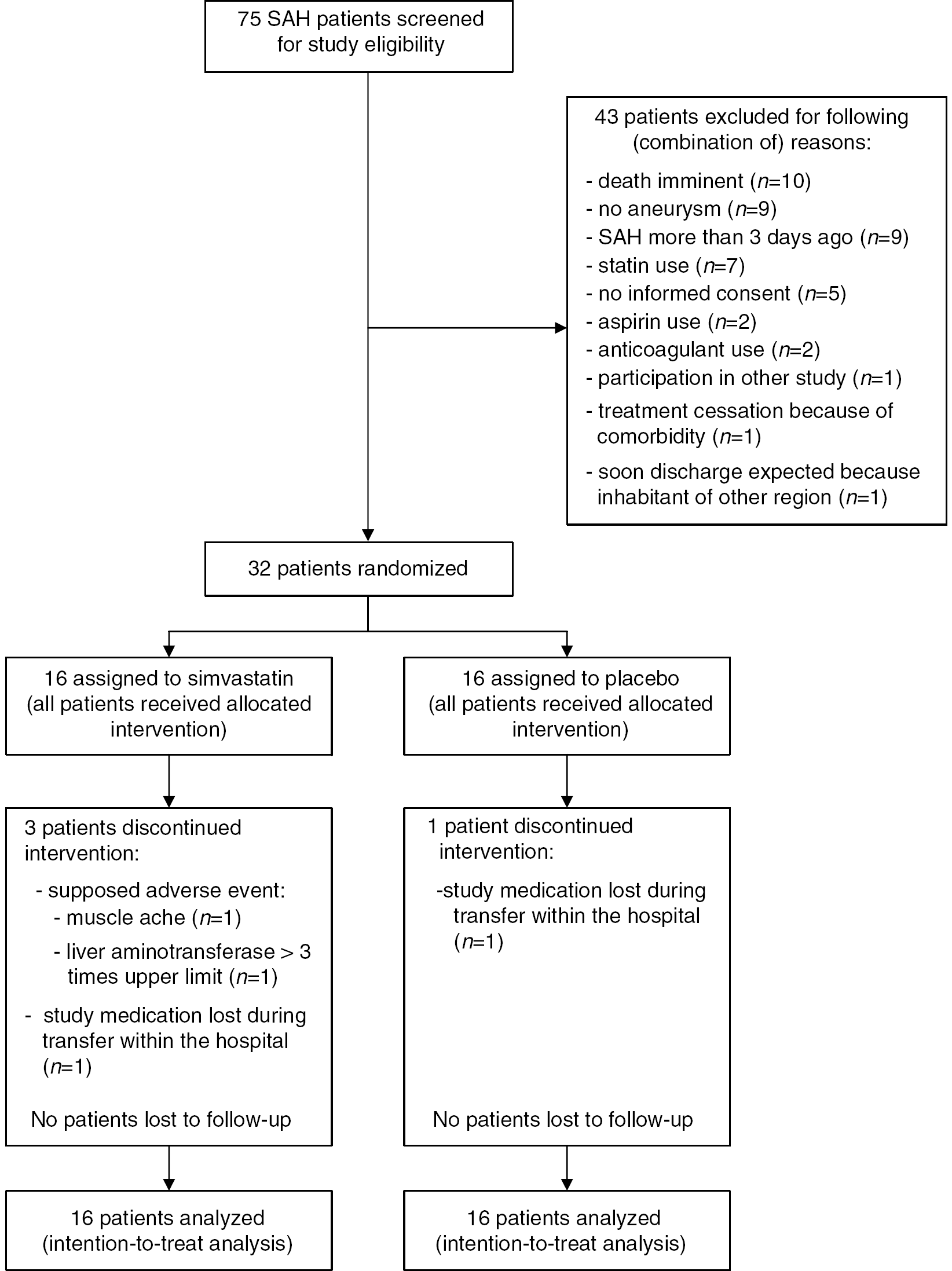
Enrolment and number of patients studied.
Baseline characteristics of the included patients are summarized in Table 1. In the placebo group, there were more women and more patients with focal neurologic impairment on admission, but this difference did not reach statistical significance. One patient in the simvastatin group had an aneurysmal bleeding pattern and was randomized before angiography, which did not show an aneurysm. This patient was included in the intention-to-treat analysis. Furthermore, no substantial baseline differences between the treatment arms were observed.
Clinical baseline characteristics of included patients
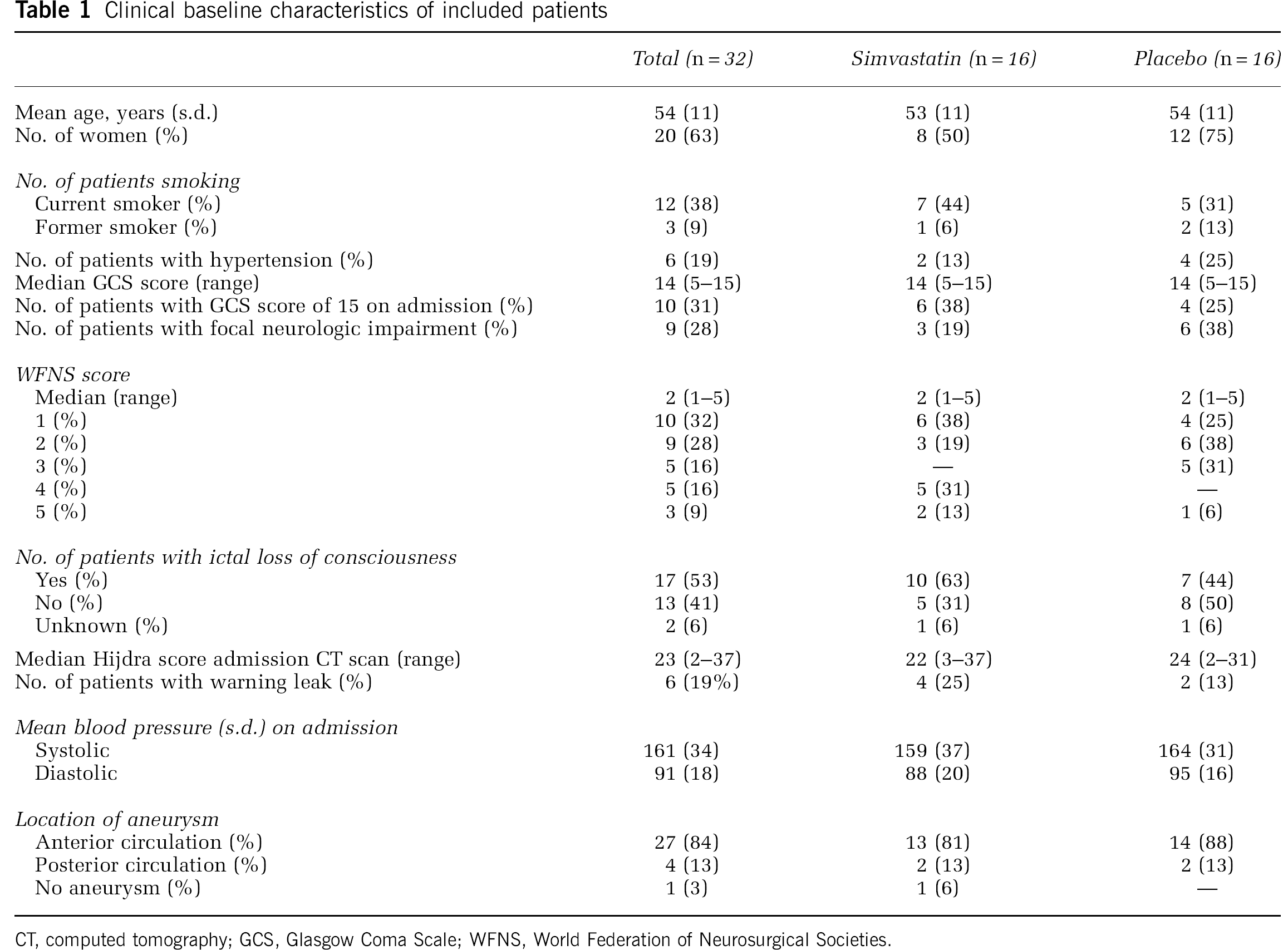
CT, computed tomography; GCS, Glasgow Coma Scale; WFNS, World Federation of Neurosurgical Societies.
Thirty-one patients received treatment of the aneurysm (24 (77%) patients were coiled and 7 (23%) patients were clipped). Median day of aneurysm treatment after SAH was day 1 (range: 0 to 30). Distribution of type and day of treatment was similar in both groups. A larger number of patients in the simvastatin group received hypertension/hypervolemia therapy (9 (56%) patients in the simvastatin group versus 4 (25%) in the placebo group).
In total, 28 (88%) patients completed the study medication treatment period or continued study medication until death. In two patients, study medication was stopped early, because of potential side effects (muscle ache (
Primary Outcome
Results of laboratory investigations are listed in Table 2 and Figure 2– Figure 4. For total cholesterol and LDL cholesterol, but not for high-density lipoprotein cholesterol and triglycerides, there were significant differences by treatment group (
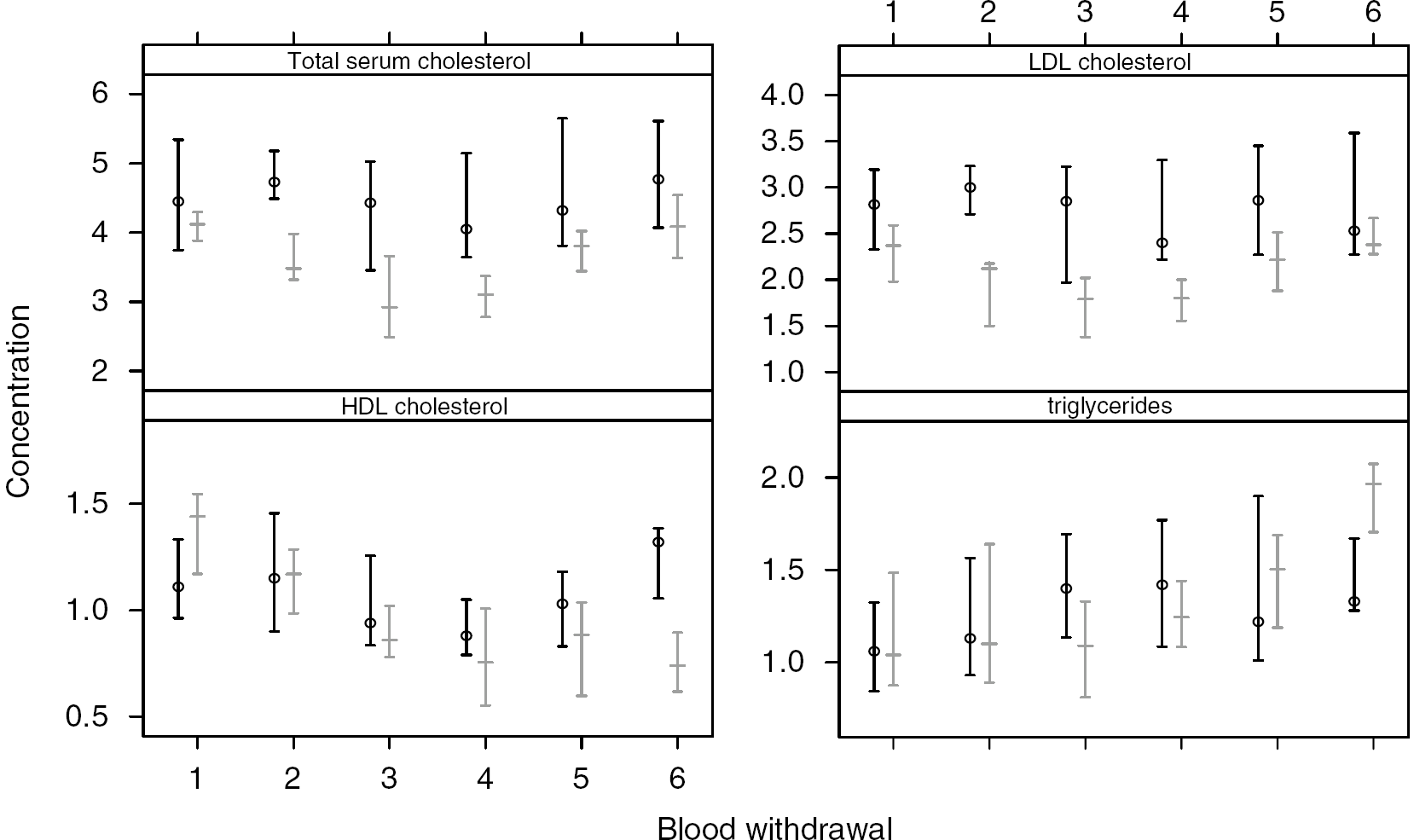
Error bars showing results of total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides. Error bars are medians with interquartile ranges. Black lines indicate patients randomized to placebo; gray lines indicate patients randomized to simvastatin. All values are expressed in mmol/L.
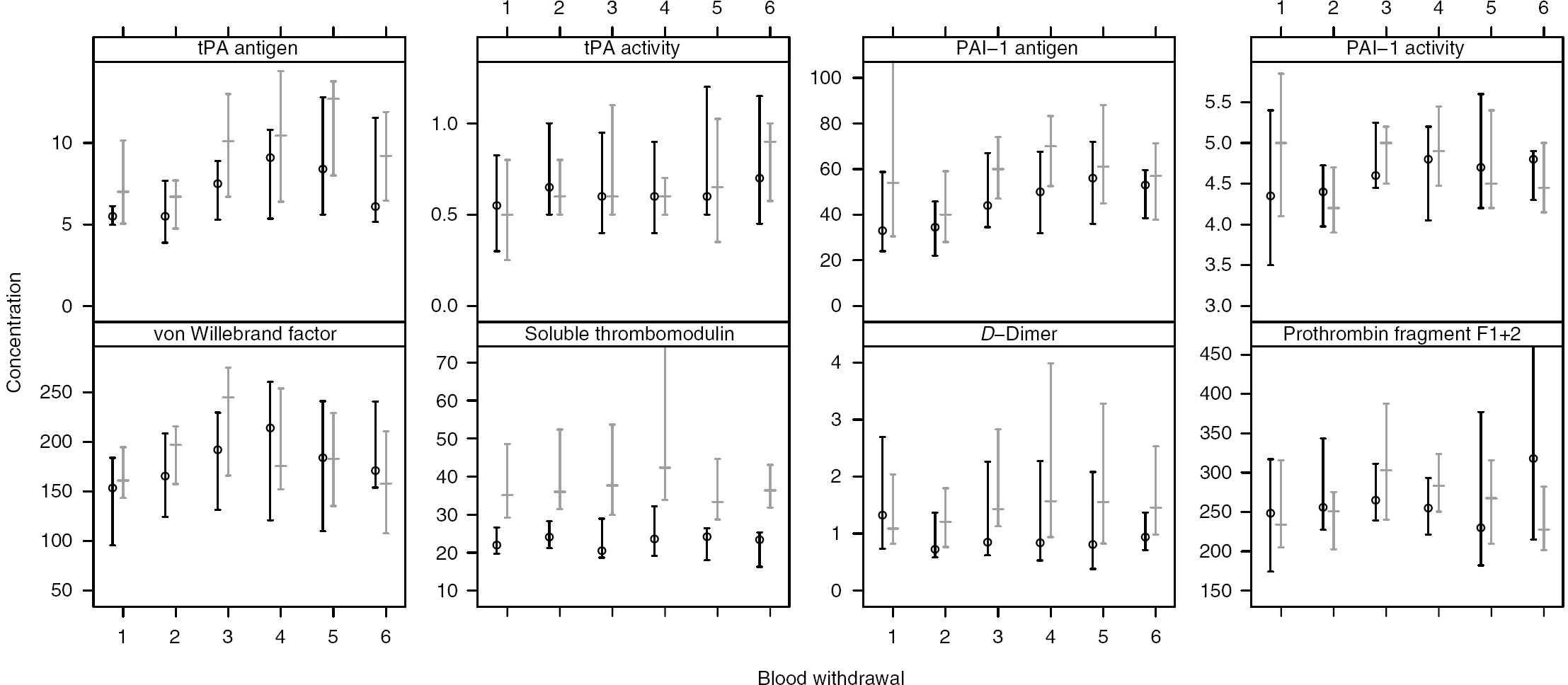
Error bars showing results of parameters of fibrinolysis, coagulation, and endothelium function. Error bars are medians with interquartile ranges. Black lines indicate patients randomized to placebo; gray lines indicate patients randomized to simvastatin. Values of tPA antigen and PAI-1 antigen are expressed in ng/mL; tPA activity and PAI-1 activity are in IU/mL; vWF (von Willebrand factor) antigen is in %; sTM (soluble thrombomodulin) is in ng/mL;
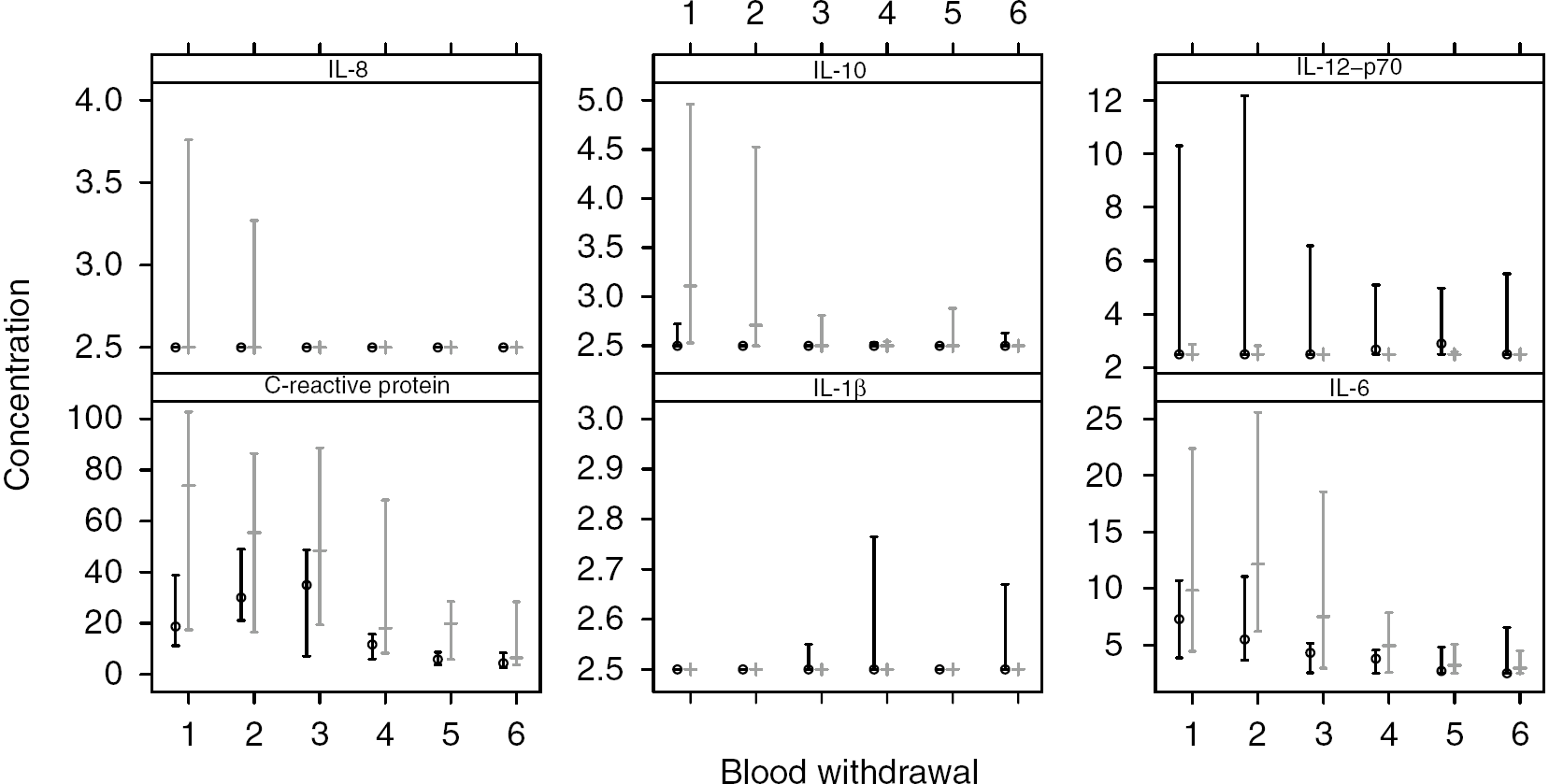
Error bars showing results of parameters of inflammation. Error bars are medians with interquartile ranges. Black lines indicate patients randomized to placebo; gray lines indicate patients randomized to simvastatin. Values of C-reactive protein are expressed in mg/L; all ILs and TNF-α are in pg/mL
Results of laboratory investigations
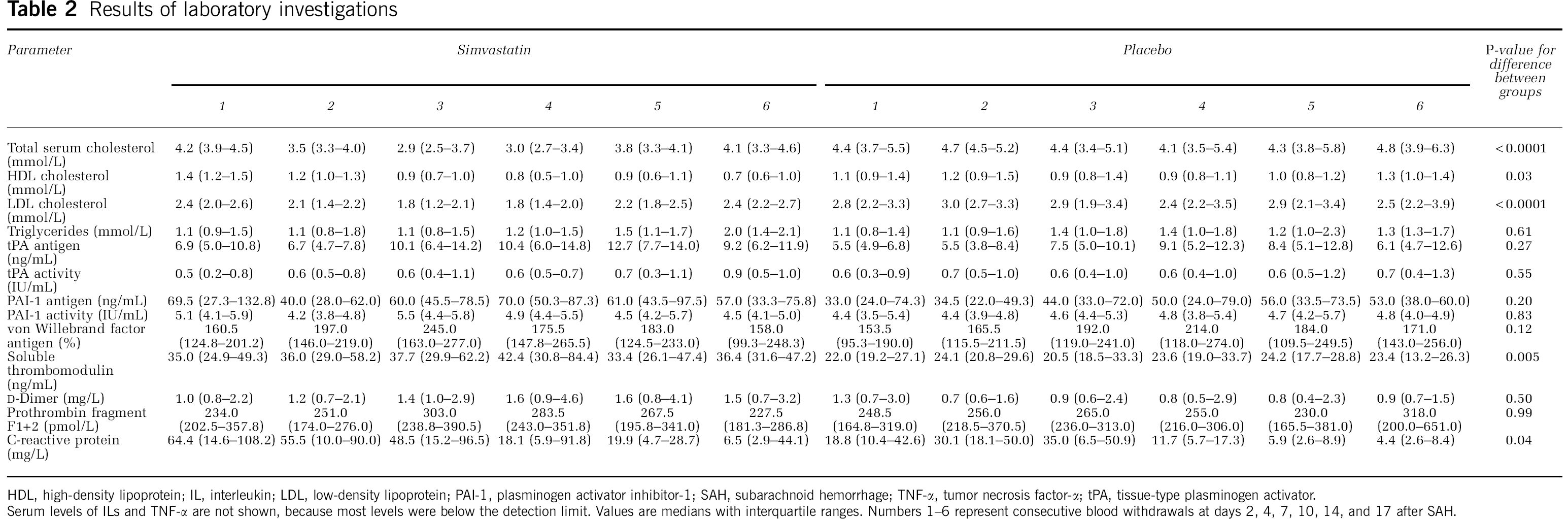
HDL, high-density lipoprotein; IL, interleukin; LDL, low-density lipoprotein; PAI-1, plasminogen activator inhibitor-1; SAH, subarachnoid hemorrhage; TNF-α, tumor necrosis factor-α; tPA, tissue-type plasminogen activator.
Serum levels of ILs and TNF-α are not shown, because most levels were below the detection limit. Values are medians with interquartile ranges. Numbers 1–6 represent consecutive blood withdrawals at days 2, 4, 7, 10, 14, and 17 after SAH.
Secondary Outcome
Distribution of events in both treatment groups is summarized in Table 3. The occurrence of TCD vasospasm and clinical signs of DCI was similar in both treatment groups. Signs of DCI started at a median of 6 days (range: 4 to 10). Two patients who did not complete study medication had clinical signs of DCI. Both were randomized to the simvastatin group and had clinical signs of DCI before medication was stopped: both patients developed DCI at day 5, whereas the last study medication was given at day 6.
Distribution of events, TCD vasospasm, and outcome after SAH
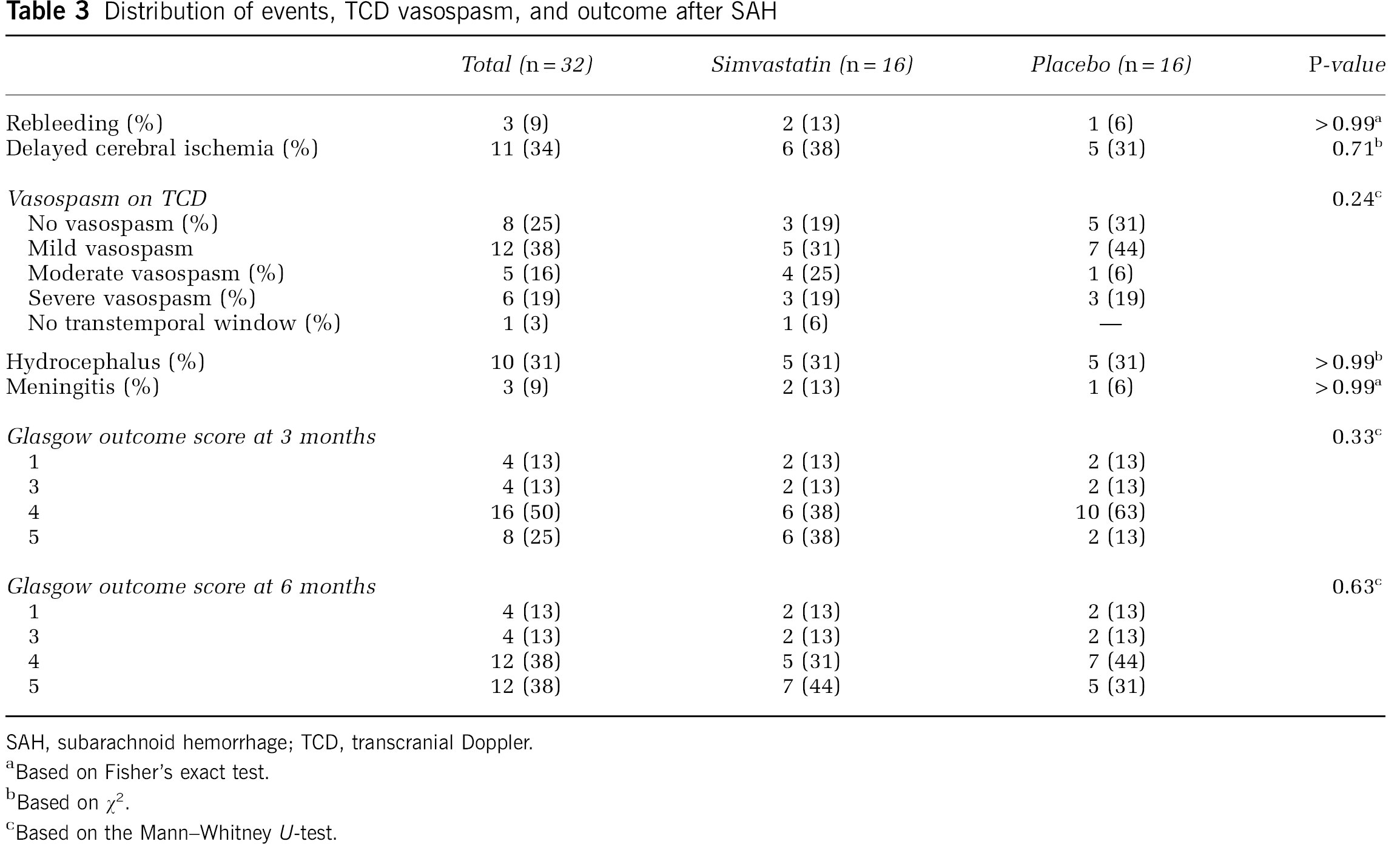
SAH, subarachnoid hemorrhage; TCD, transcranial Doppler.
Based on Fisher's exact test.
Based on χ2.
Based on the Mann-Whitney
Follow-up data 3 and 6 months after SAH were complete in all randomized patients (Table 3). In each treatment group, 4 (25%) patients had poor outcome 3 and 6 months after SAH. The causes of poor outcome in the simvastatin group were initial hemorrhage (
Discussion
The results of this study show that in patients with SAH, acute simvastatin treatment decreases serum levels of total cholesterol and LDL cholesterol, but has no effect on markers of endothelial function, coagulation, and fibrinolysis. The analysis for IL-10 showed a significant difference in trend for treatment group, but the most plausible explanation for this difference is a return-to-normal phenomenon, as patients who were randomized to simvastatin had a significantly higher probability to have detectable IL-10 levels before the initiation of study medication. After withdrawal of study medication, the levels of IL-10 remained low in both groups, in contrast to total cholesterol and LDL cholesterol levels, which increased in patients randomized to simvastatin. Other serum levels of inflammation also remained unaffected by simvastatin treatment. Finally, simvastatin did not affect TCD vasospasm, clinical signs of DCI, and poor outcome on the Glasgow Outcome Scale 3 and 6 months after SAH.
Statins provide a central basis for cardiovascular prevention in high-risk patients (Scandinavian Simvastatin Survival Study (4S) Group, 1994; Sacks et al, 1996; The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group, 1998; Heart Protection Study Collaborative Group, 2002). However, the impact of pleiotropic effects for clinical benefit is a matter of intense debate. Although data from meta-analyses of lipid-lowering trials suggest that lipid modification alone accounts for the clinical benefits associated with statin therapy, recent studies have implied that statin-induced LDL cholesterol reduction may in fact be more beneficial compared with non-statin-induced LDL cholesterol reduction (Brouilette et al, 2007; Landmesser et al, 2005; Fichtlscherer et al, 2006; Rossebø et al, 2008). These pleiotropic effects have even been suggested to contribute to neuroprotection (Kivipelto et al, 2005).
In this study, we did not find any evidence to support pleiotropic effects in patients with SAH. This is in contrast to two other studies that investigated the effects of statins in this group of patients (Lynch et al, 2005; Tseng et al, 2007b). In one study, lower levels of vWF and of S100β, a marker of astrocyte activation and central nervous system activation, were observed in SAH patients treated with simvastatin (Lynch et al, 2005). However, it is not known whether serum levels of these parameters already differed before the initiation of study medication, and whether these differences disappeared after withdrawal of study medication. Another study reported that SAH patients treated with statins had increased
Although this study was not powered to detect clinical differences, which precludes drawing conelusions, our secondary outcome results are also remarkable. A recent metaanalysis showed that acute statin treatment reduces the incidence of vasospasm, DCI, and mortality in SAH patients (Sillberg et al, 2008). The results of this metaanalysis, which included three phase II studies with 39, 39, and 80 patients, respectively, and therefore had insufficient power to detect clinical differences, were mainly based on two studies (Lynch et al, 2005; Tseng et al, 2005). However, the results of these two studies should be interpreted with caution. For example, in one study, there was an abnormal high rate of DCI in the placebo group (60%) (Lynch et al, 2005). In the group of patients treated with statins, the incidence of clinical signs of DCI was 26%, which is comparable with data from prospective studies that included patients not treated with statins (Roos et al, 2000). Therefore, the placebo group did not have a representative incidence of DCI, which may reflect an imbalance in randomization. In the other study, many patients had DCI more than 14 days after SAH, which is unusual in SAH patients (Tseng et al, 2005). This late occurrence was attributed to cessation of statin treatment after day 14. However, in that study, only 60% of the patients continued study medication until death or until day 14. It is therefore questionable whether this is a valid explanation for this late DCI phenomenon. Furthermore, in the pravastatin study, there was an unusually high sepsis-caused mortality rate in the placebo group compared with the statin group (71 versus 6%, respectively) (Tseng et al, 2007a).
A limitation of this study is that only systemic levels of biomarkers were assessed instead of local levels from the cerebral circulation. This might have resulted in dilution of locally increased levels and an underestimation of a possible effect. Another limitation is that we only studied a number of serological parameters. Therefore, it cannot be ruled out that statins affected other parameters, such as endothelial nitric oxide synthase, oxidases, and dismutases. However, the parameters described in this paper are good representations of various pathways. In addition, blood samples were taken with intervals of 3 to 4 days, which might have resulted in missing important peaks in the levels of various parameters. Furthermore, the sample size of our study was small. Therefore, although our study had a randomized design, it could be that the groups were not well balanced. For example, patients in the simvastatin group had substantially higher baseline levels of C-reactive protein, PAI-1, IL-10, and sTM. Besides, more patients in the simvastatin group had loss of consciousness at the time of ictus, developed moderate TCD vasospasm, and received hypertension/hypervolemia therapy. Therefore, it cannot be excluded that the lack of effect from statins could have, in part, been due to a ‘failure of randomization’ of baseline and patient characteristics. Finally, as our study mainly included good-grade patients, it cannot be ruled out that statins are more beneficial in poor-grade patients.
We conclude that the results of this study do not support a beneficial effect of simvastatin in patients with SAH. The primary end point analysis did not show evidence of acute pleiotropic effects exerted by simvastatin, which were earlier suggested to be the working mechanism in this group of patients. The secondary end points did not show a trend toward lower incidences of vasospasm, DCI, and poor outcome. However, only phase III clinical trials will definitely answer the question whether acute statin treatment is beneficial in patients with SAH.
Footnotes
The authors declare no conflict of interest.