
Abstract
Knowledge on autoregulation of cerebellar blood flow in humans is scarce. This study investigated whether cerebellar autoregulation dynamics and CO2 reactivity differ from those of the supratentorial circulation. In 56 healthy young adults, transcranial Doppler (TCD) monitoring of the posterior inferior cerebellar artery (PICA) and, simultaneously, of the contralateral middle cerebral artery (MCA) was performed. Autoregulation dynamics were assessed by the correlation coefficient method (indices Dx and Mx) from spontaneous blood pressure fluctuations and by transfer function analysis (phase and gain) from respiratory-induced 0.1 Hz blood pressure oscillations. CO2 reactivity was measured via inhalation of air mixed with 7% CO2. The autoregulatory indices Dx and Mx did not differ between the cerebellar (PICA) and cerebral (MCA) vasculature. Phase and gain, which describe faster aspects of autoregulation, showed slightly better values in the PICA compared with the MCA (higher phase,
Introduction
The human cerebellum contains more neurons than the rest of the brain combined (Andersen et al, 1992). It is a phylogenetically old part of the brain involved in basic processing of motor, sensory, and mental skills (Bellebaum and Daum, 2007). Cerebellar blood supply is characterized by a lack of anastomoses between the cortical penetrator branches. Ischemic borderzone lesions in the cerebellum are more frequent than previously assumed (Amarenco et al, 1993). For instance, 7% of persons with migraine with aura show such ischemic cerebellar lesions suggesting a particular vulnerability of the cerebellum to hypoperfusion and a lower capacity of blood flow autoregulation in migraine (Kruit et al, 2005). Also prodromal symptoms of syncope can be partially attributed to cerebellar hypoperfusion (Lempert et al, 1994), suggesting an earlier exhaustion of the cerebellar autoregulatory reserve. Basically, the vertebrobasilar circulation has a lower autonomic innervation (Edvinsson et al, 1976) and this fact has been linked to a lower autoregulatory ability in the posterior cerebral artery (Haubrich et al, 2004).
The knowledge on blood flow autoregulation of the cerebellum, however, is scarce. Animal studies showed conflicting results with a better static autoregulation than in the cerebrum (Sato et al, 1984), whereas others found a poorer cerebellar autoregulation in rats during progressive hypotension (Merzeau et al, 2000). Studies in humans refer to steady-state measurements of autoregulation in patients with Moya-Moya disease not primarily focusing on cerebellar autoregulation (Ogawa et al, 1990).
Transcranial Doppler sonography (TCD) permits noninvasive investigation of cerebral hemodynamics (Aaslid et al, 1982). This technique is widely used to measure the reactivity of cerebral arterioles to vasodilatory stimuli such as CO2 (Ringelstein et al, 1992). Its high temporal resolution also allows measuring of the dynamic properties of the cerebral autoregulatory system during minor, even spontaneously occurring, blood pressure changes (Panerai, 2007; Aaslid et al, 1989; Zhang et al, 1998; Kuo et al, 1998; Czosnyka et al, 1996b). Although the posterior inferior cerebellar artery (PICA) can be insonated via a transnuchal approach, TCD has not been used for continuous monitoring of the PICA and thus the assessment of cerebellar hemodynamics. So far, the superior cerebellar artery has been monitored in the first functional TCD study (Aaslid, 1987).
In this study, we applied simultaneous transtemporal and transnuchal TCD monitoring to investigate whether cerebellar autoregulation dynamics differ from those of the supratentorial circulation in healthy human adults. Secondly, we examined whether Doppler CO2 reactivity varies between the cerebellar and cerebral vasculature.
Subjects and methods
We studied 60 healthy adults with no history of vascular or neurologic disease. All persons were free from any medication apart from contraceptives (
Insonation of the Posterior Inferior Cerebellar Artery
With transnuchal Doppler sonography, the PICA is usually found at a depth of 60 to 75 mm as a strong flow signal heading toward the Doppler probe (von Reutern and von Büdingen, 1993). Such a signal can rarely also be caused by an elongation of the V4 segment of the vertebral artery and, theoretically, by the anterior spinal artery. The anterior spinal arteries are small and descend from the vertebral artery close to the vertebrobasilar junction. To guarantee that the assessed transnuchal TCD signal truly represented the PICA, all persons initially underwent a non-contrast-enhanced transnuchal color-coded duplex sonography examination. Thereby, color flow signals of both V4 segments of the vertebral artery and their continuous confluence to the proximal basilar artery were identified and any loops, coils, and kinks of the vertebral artery were searched for. In anatomic studies, the PICA usually branches off the distal vertebral artery at a mean of 16.9 mm proximal to the vertebrobasilar junction (Lister et al, 1982). Secure identification of the PICA on transnuchal duplex sonography was defined via the following criteria: (1) substantial color flow signal heading toward the ultrasound probe, (2) branching off from the V4 segment of the vertebral artery more than 10 mm away from the vertebrobasilar junction (in contrast to the anterior spinal artery), and (3) heading initially laterally (not medially like the anterior spinal artery). Persons were included in the study only if a complete and continuous depiction of the V4 segments of the vertebral artery without interfering elongations of the respective V4 segment and a clearly identifiable PICA according to the criteria detailed above was present at least on one side.
The PICA side, which was better visible on duplex sonography, was chosen to be monitored with the TCD probe from the same site and depth as depicted with the duplex ultrasound probe. Continuous insonation was achieved by fixing the TCD probe to the transnuchal position using a special custom-built headframe (Figure 1). As a second supratentorial vessel, the middle cerebral artery (MCA) contralateral to the insonated PICA was monitored in a standard fashion (Multidop-X, DWL, Sipplingen, Germany). The side of PICA and MCA monitoring did not significantly influence any of the assessed hemodynamic parameters.
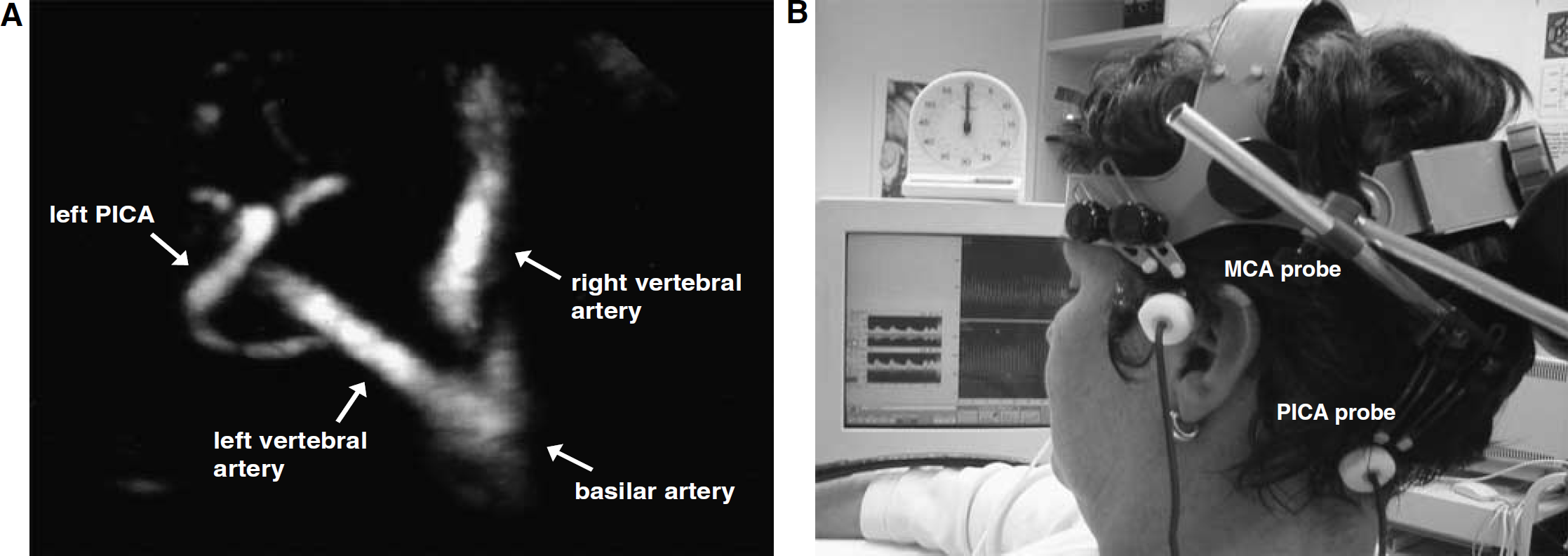
Transcranial Doppler monitoring of the posterior inferior cerebellar artery (PICA). (
Measurement of Standard Hemodynamics
Arterial blood pressure (ABP) at heart level was monitored continuously via fingerplethysmography (Finapres, Ohmeda, Englewood, CO, USA). End-tidal CO2 partial pressure (PetCO2) was measured by a standard capnometer (Datex, Helsinki, Finland). All measurements were performed with subjects in a semireclining position and moderate anteflection of the head. Mean baseline hemodynamic values were calculated from a period of 120 secs at rest. Pulsatility index (PI) of cerebral blood flow velocity (CBFV) was calculated as PI = (CBFVsystole—CBFVdiastole/CBFVmean).
Measurement of Dynamic Cerebral Autoregulation
Cerebral autoregulation was calculated by two different methods (Czosnyka et al, 1996b; Diehl et al, 1995). (1) Calculation of the correlation coefficient index from 10 mins of spontaneous fluctuations of ABP and CBFV; briefly, mean and diastolic values of ABP and CBFV were averaged over 3-sec periods and from 20 consecutive 3-sec averages single Pearson's correlation coefficients were calculated (i.e., for every 1-min period). The so collected ten 1-min period correlation coefficients were then averaged to form the autoregulatory indices
Measurement of CO2 Reactivity
CO2 reactivity to hypercapnia was determined via inhalation of air mixed with 7% CO2 for 90 to 120 secs and calculated as the relative increase of CBFV per mm Hg increase of PetCO2 (% per mm Hg). In a
Statistical Analysis
Data were checked for normality of distribution by the Kolmogorov—Smirnov test. Between-group differences were analyzed by the two-tailed Students
Results
Posterior Inferior Cerebellar Artery Monitoring and Results of Standard Hemodynamics
The PICA was identified on transnuchal duplex sonography according to the predefined criteria on at least one side in 57 persons (95%) and on both sides in 34 persons (57%). In two persons, an anatomic variant was suspected with both PICAs originating from the proximal basilar artery and in one person there was no transnuchal insonation window. These 3 persons were excluded from the study along with 1 of the 57 persons with identifiable PICA in whom continuous TCD monitoring was not possible because of overlaying venous signals. An example recording of MCA and PICA is shown in Figure 2. Detailed characteristics of the finally studied 56 persons and baseline hemodynamics are summarized in Table 1. Notably, the PI at rest was significantly lower in the PICA.
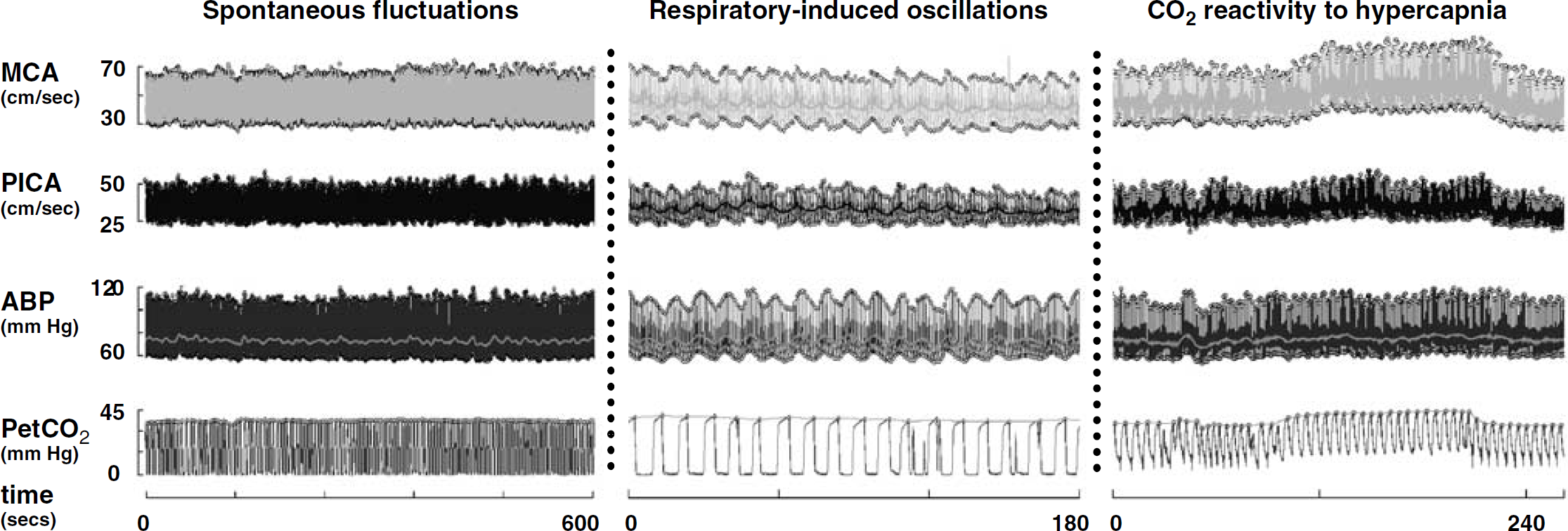
Illustrative recordings. Example of TCD monitoring of the middle cerebral artery (MCA) and posterior inferior cerebellar artery (PICA) in a 51-year-old woman. Arterial blood pressure (ABP) was monitored with fingerplethysmography, nasal end-tidal CO2 partial pressure (PetCO2) with capnometry. The left panel shows spontaneous fluctuations of ABP and their transmission to Doppler signals. The middle panel shows slow oscillations of ABP and Doppler signals induced by regular breathing at 6/min. (0.1 Hz). The right panel illustrates CO2 reactivity to hypercapnia, which was induced by inhaling a mixture of 7% CO2 and air for 120 secs. Note the different time scales on the × axis.
Baseline characteristics
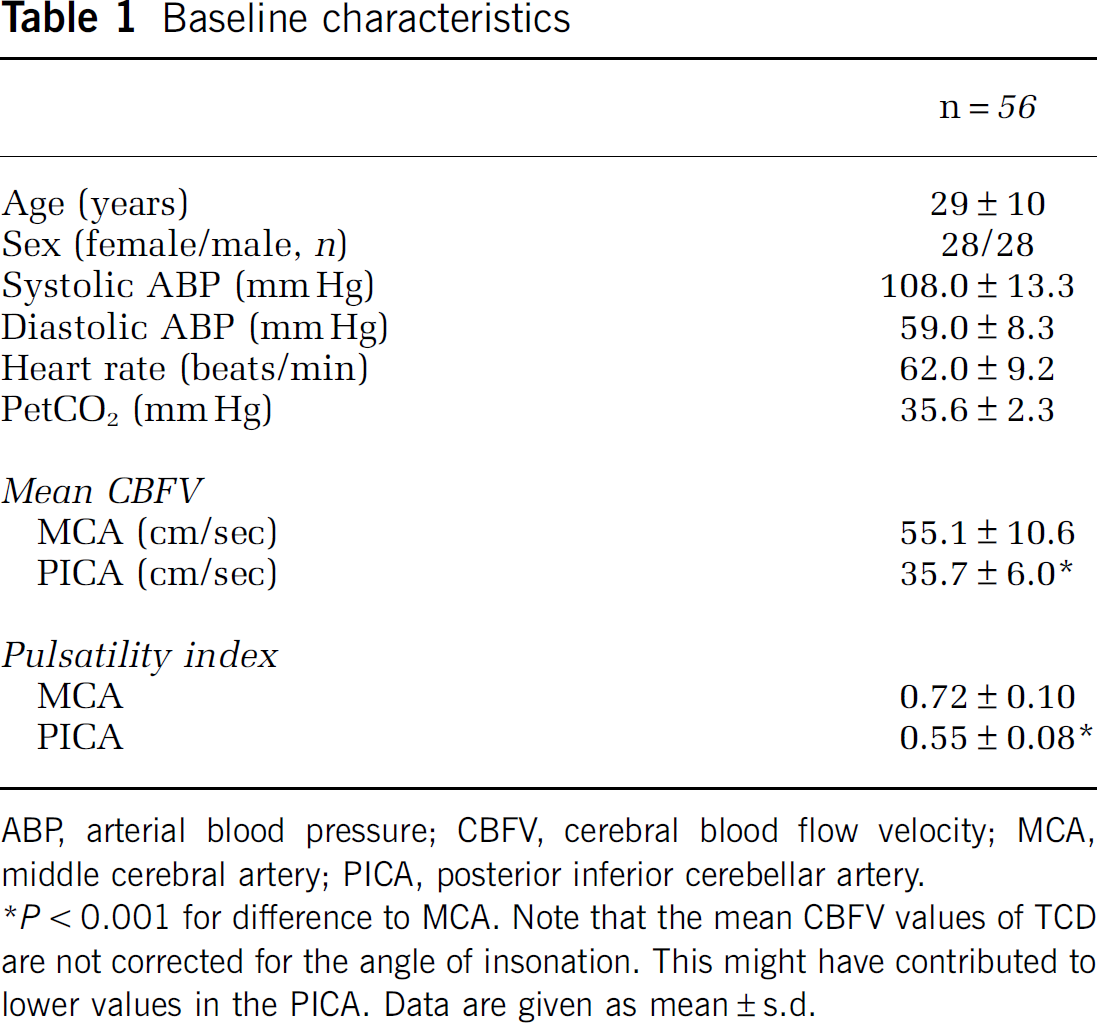
ABP, arterial blood pressure; CBFV, cerebral blood flow velocity; MCA, middle cerebral artery; PICA, posterior inferior cerebellar artery.
Cerebellar Autoregulation Dynamics
The time domain indices of cerebral autoregulation (Dx, Mx) did not differ between the PICA and the MCA (Table 2). The phase shift between 0.1 Hz oscillations of blood pressure and CBFV was significantly higher in the PICA than in the MCA (mean relative intraindividual difference: + 15% ± 37%). The gain of the transfer function was slightly but significantly lower in the PICA (mean relative difference versus MCA: —5% ± 16%). There was a significant intraindividual correlation between absolute autoregulation values in the PICA and the MCA. No influence of age or sex on any autoregulatory parameter in the MCA or PICA was observed.
Autoregulation dynamics in PICA versus MCA
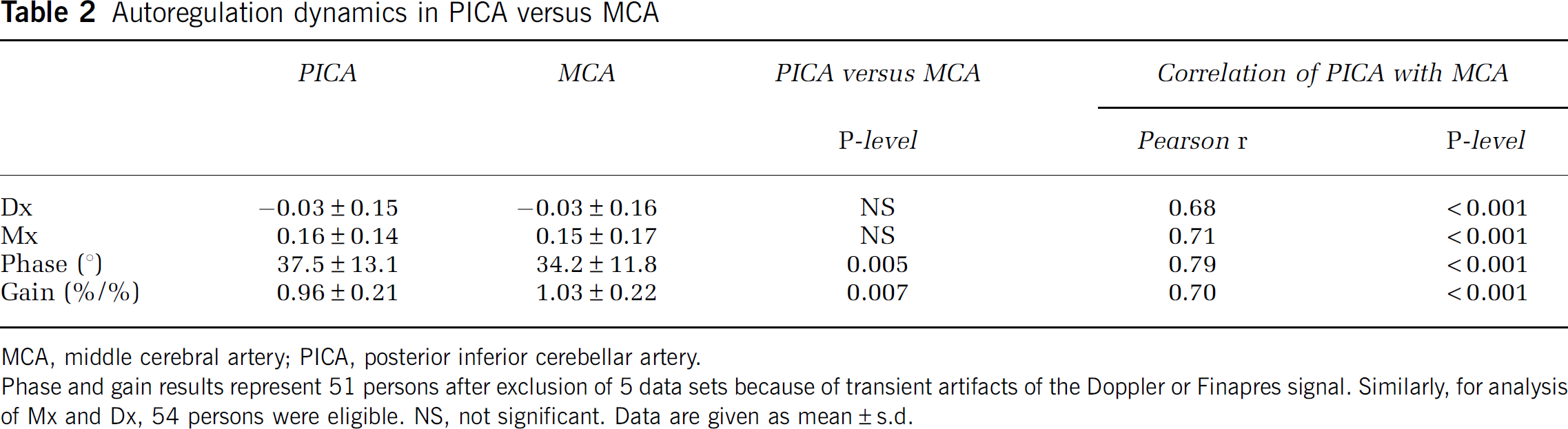
MCA, middle cerebral artery; PICA, posterior inferior cerebellar artery.
Phase and gain results represent 51 persons after exclusion of 5 data sets because of transient artifacts of the Doppler or Finapres signal. Similarly, for analysis of Mx and Dx, 54 persons were eligible. NS, not significant. Data are given as mean ± s.d.
Cerebral and Cerebellar Doppler CO2 Reactivity
Values of CO2 reactivity (response to hypercapnia) were significantly lower in the PICA than in the MCA with a mean relative difference of −27% ± 29% (Table 3; Figure 3). Correspondingly, the PI decreased to significantly lesser extent in the PICA during hypercapnia.
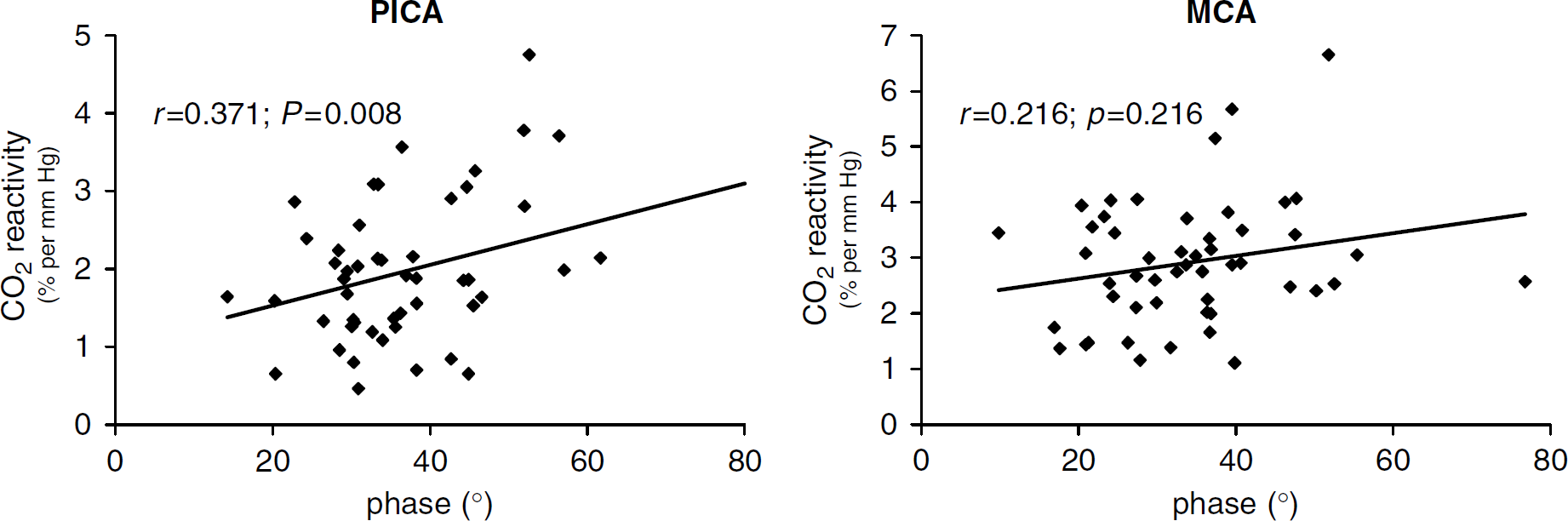
Scatter plots of autoregulation versus CO2 reactivity. Autoregulation phase versus CO2 reactivity to hypercapnia in the posterior inferior cerebellar artery (PICA) and middle cerebral artery (MCA). Pearson's correlation coefficients are given. Comparisons refer to 50 persons because of exclusion of 6 persons (see Tables 2 and 3).
CO2 reactivity in PICA versus MCA
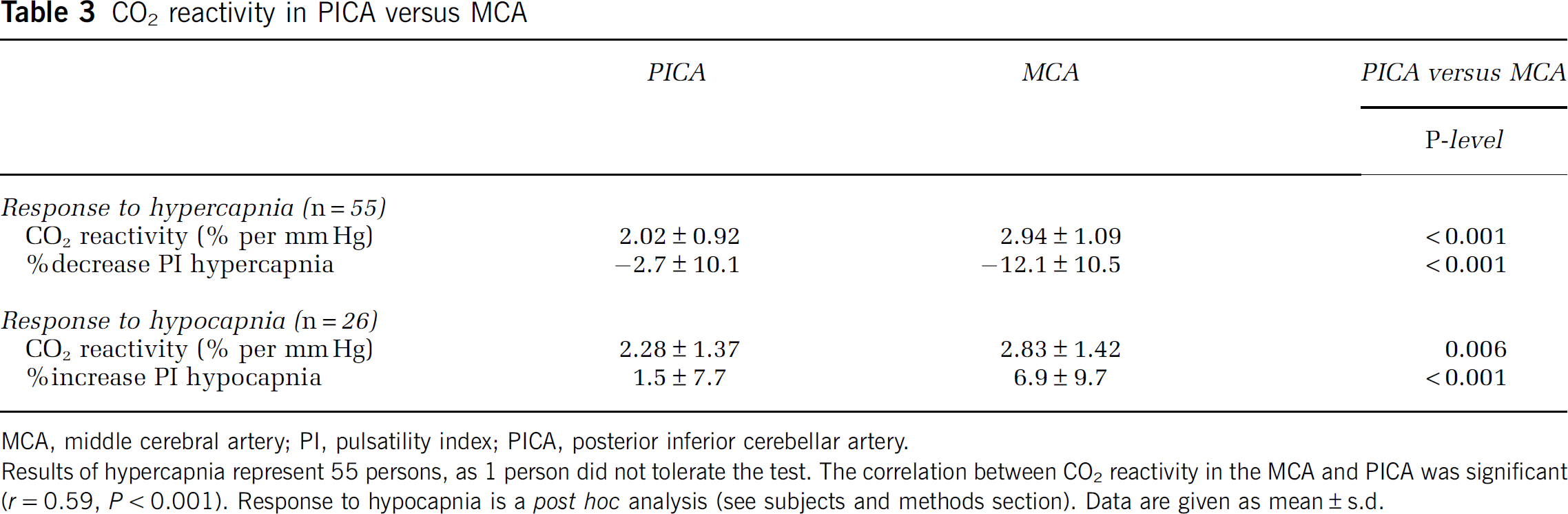
MCA, middle cerebral artery; PI, pulsatility index; PICA, posterior inferior cerebellar artery.
Results of hypercapnia represent 55 persons, as 1 person did not tolerate the test. The correlation between CO2 reactivity in the MCA and PICA was significant (
Discussion
A rapid autoregulatory response is pivotal for cerebellar circulation because of the urgent need of cerebellar function immediately after achieving upright position, when blood pressure drops temporarily even in healthy adults. This study found a rapid autoregulatory action in the cerebellum, whereas CO2 reactivity was lower than in the cerebrum.
Ultrasound of Cerebellar Vessels
The main limitation of the applied TCD technique is that cerebral blood flow itself is not directly measured. It is, however, valid for detection of relative changes in cerebral blood flow during rapid changes in blood pressure (Newell et al, 1994). Moreover, TCD enables detection of local cerebral hemodynamics in a noninvasive manner. Neither TCD nor invasive CBF techniques with high temporal resolution have been used for monitoring cerebellar autoregulation in humans so far. In the present study, identification of the PICA via transcranial duplex sonography and subsequent TCD monitoring was possible in most of the subjects. The rates of identification of the PICA with transcranial duplex sonography were higher than in the only earlier systematic investigation (Kaps et al, 1992). This is explained by interim advances in the duplex ultrasound technology.
Autoregulation Response
Autoregulation indices in the cerebrum and cerebellum correlate significantly. This suggests that intraindividual autoregulatory ability affects both cerebrum and cerebellum. The indices based on the correlation coefficient method, which reflects both dynamic and static autoregulation properties, show no major difference between cerebellar and cerebral circulation. The more dynamic approach of cross-spectral analysis of 0.1 Hz oscillations, however, indicates a slightly faster reaction of cerebellar circulation toward alternating ups and downs in blood pressure (higher phase shift). Furthermore, the lower dynamic gain suggests slightly better dampening of blood pressure oscillations in the PICA. Such better dampening characteristics are likely to indicate better dynamic autoregulation (Zhang et al, 2007). Interestingly, dynamic gain in the posterior cerebral artery was higher than in the anterior circulation (Haubrich et al, 2004), suggesting lower dampening of blood pressure oscillations. This fact has been associated with lower autonomic (sympathetic) innervation in the posterior vascular territory (Haubrich et al, 2004; Edvinsson et al, 1976). Although low autonomic innervation was also found in the cerebellum (Edvinsson et al, 1976), the present results show that effective dampening of blood pressure oscillations is still possible in this situation and that neurogenic modulation may not critically account for this mechanism. In general, myogenic mechanisms like stretch-activated ion channels sensitive to intramural pressure changes might play a greater role in the autoregulatory mechanism (Earley et al, 2004). Specific differences in the expression of such effectors between the cerebral and cerebellar arteries have not been reported so far.
The only previous study on cerebellar autoregulation in humans analyzed static autoregulatory properties in the cerebrum and cerebellum in patients with variable degrees of Moya-Moya disease (Ogawa et al, 1990). There was active cerebellar autoregulation, but basic physiologic comparisons between the cerebellum and cerebrum were not meaningful in these patients because of the heterogeneous degree of hemodynamic compromise in the anterior circulation.
CO2 Reactivity in the Cerebellum Versus Cerebrum
In a previous study measuring cerebral blood flow by PET (positron emission tomography), the response to hypercapnia (but not to hypocapnia) was larger in the cerebellum than in most of the supratentorial regions supplied by the MCA (Ito et al, 2000). A higher vasodilatory reserve of cerebellar arterioles to hypercapnia has thus been presumed (Ito et al, 2000). Conversely, a single positron emission computed tomography study using acetazolamide as a vasodilator showed a lower dilatory reactivity in the cerebellum than in the cerebrum (Suzuki et al, 2002).
CO2 reactivity measured by TCD seems to be similar in the middle, posterior, and basilar artery in healthy adults but has not been examined in the cerebellum so far (Kastrup et al, 1998; Park et al, 2003). The present results of lower CO2 reactivity to hypercapnia in the PICA are in contrast to the previous PET study using CO2 as a vasodilator (Ito et al, 2000). One reason might be the different methodology used: TCD can only measure velocities and not the absolute flow. Relative increases during hypercapnia should, however, not be influenced by this limitation in case of stable diameters of the insonated vessel. The TCD response to hypercapnia may be influenced by a 10% vasodilation of the MCAs during hypercapnia (Valdueza et al, 1999), leading to a flow velocity increase lower than the true increase in flow. Yet, high correlations between MCA TCD flow velocities and PET results have been found with varying PETCO2 (Poeppel et al, 2007). Corresponding data on dilation of the PICA are not available. Angiographic studies showed a larger dilation of smaller basal cerebral arteries with a diameter of less than 2 mm (Huber and Handa, 1967). Although not specifically shown, this might also apply for the PICA with mean diameters reported between 1.2 and 2.0 mm (Pai et al, 2007, Lister et al, 1982). A larger dilation in the PICA might thus lead to a lower increase of CBFV during hypercapnia and to lower CO2 reactivity.
Unlike the previously applied PET, the TCD technique applied here allows valid estimation of the current vascular resistance under hypercapnic challenges by the PI (Czosnyka et al, 1996a). The present findings point toward a lower vasodilatory reaction of the cerebellar arterioles to hypercapnia. Notably, the PI was lower in the PICA than in the MCA already at rest, indicating a different working point of vascular tone. This might be explained by the different autonomic innervation but also regional heterogeneity in ion channels and production of nitric oxide or reactive oxygen species (Andresen et al, 2006; Faraci, 2006). In this situation of higher baseline vasodilation, one would expect a preserved vasoconstrictory reaction to hypocapnia. We thus analyzed this response
Overall, the present TCD findings on CO2 reactivity in the PICA could be partly attributed to methodological factors regarding the different vessel size of the MCA and PICA. However, there might also be a genuine lower sensitivity of cerebellar arterioles to changes in CO2 or a lower dilatory capacity. To clarify this issue, future studies comparing vessels of comparable diameters in the cerebral (M2 segment of MCA) and cerebellar circulation should be performed.
Autoregulation Versus CO2 Reactivity in the Cerebellum Versus Cerebrum
The lower cerebellar CO2 reactivity with preserved dynamic autoregulation may also suggest dissociation between dynamic autoregulation and CO2 reactivity in the cerebellum. There are, however, two refutations to be considered. First, the fully preserved dynamic autoregulatory function of cerebellar arterioles does not preclude a possible lower capacity of diameter changes of cerebellar arterioles in the PICA because the dynamic approach does not challenge the full range of dilation but rather its promptness. Second, there was a significant correlation between absolute CO2 reactivity and the quality of dynamic autoregulation in the cerebellum, and this was not observed for the MCA. Previous studies on the correlation between CO2 reactivity and dynamic autoregulation are only available for the MCA. They yielded at best moderate correlations brought forward by pooling pathologic and normal values into one analysis (White and Markus, 1997; Reinhard et al, 2001). The positive correlation observed here between CO2 reactivity and the autoregulatory parameters in the cerebellum rather points to an intraindividual association between cerebellar autoregulation and CO2 reactivity. The dissociation refers to the fact that within this association the CO2 reactivity is systematically lower in the PICA than in the MCA.
Conclusions
Dynamic autoregulation in the human cerebellum is well operating and has slightly faster regulatory properties than the anterior cerebral circulation. The vasoreactivity to CO2 as assessed by TCD is significantly lower in the cerebellum than in the anterior cerebral circulation, which could be partly caused by assumed greater diameter changes of the insonated PICA under hyper/hypocapnia. The introduced methodology of cerebellar TCD monitoring will enhance the understanding of cerebellar hemodynamics under various pathophysiological conditions like orthostatic intolerance, migraine, and cerebellar stroke.