
Abstract
Background
The Toll-like receptor plays an essential role in controlling immunity and inflammation. This study was to investigate the relationships of genetic variants in TLR2 and TLR3 with hepatitis B virus (HBV) natural clearance and HBV-related hepatocellular carcinoma (HCC) risk in a Chinese male population.
Methods
We analyzed 5 polymorphisms of TLR2 (rs3804099 and rs3804100) and TLR3 (rs5743305, rs3775296 and rs3775291) in a population consisting of 686 participants with HBV natural clearance, 293 chronic HBV carriers and 395 HBV-positive HCC patients, using the improved multiplex ligase detection reaction method.
Results
After adjustment for age and smoking and drinking status, no associations were observed either between the 5 single-nucleotide polymorphisms (SNPs) and the HBV natural clearance participants, or between the 5 SNPs and HCC patients. Whereas the stratified analysis showed that under the dominant models, nondrinkers with TLR2 rs3804100 and participants younger than 40 years old with TLR3 rs3775291 were significantly associated with HCC risk when compared with persistent HBV carriers (adjusted odd ratio [OR] = 0.49, 95% confidence interval [95% CI], 0.31-0.78, p = 0.003; and adjusted OR = 0.50, 95% CI, 0.29-0.86, p = 0.013, respectively). Furthermore, the TTTCT haplotype was found to promote the progress of HBV clearance and inhibit development of HBV-related HCC (OR = 0.77, 95% CI, 0.61-0.97, p = 0.029; and OR = 0.72, 95% CI, 0.55-0.94, p = 0.016, respectively). And the CCACC and CCTCT haplotypes were observed to decrease susceptibility to HCC (OR = 0.64, 95% CI, 0.40-1.00, p = 0.048; and OR = 0.43, 95% CI, 0.28-0.68, p<0.001, respectively).
Conclusions
This study revealed that TLR2 rs3804100 and TLR3 rs3775291 polymorphisms may be protective factors for HBV-related HCC.
Introduction
Hepatocellular carcinoma (HCC) has long been an important malignancy in the world, and it is the second most common cause of death from cancer (1). China is one of the regions with the highest incidence of HCC, and accounts for about 50% of the total number of cases and death (2). Development of HCC is a multifactorial process. It has been recognized that chronic infections with hepatitis B virus (HBV) and hepatitis C virus (HCV) are important risk factors for HCC (3). In addition, aflatoxin, obesity, type 2 diabetes and cirrhosis related to heavy alcohol consumption have also been demonstrated to be causes of HCC (1, 2, 4). HBV is a leading risk factor for HCC, and at least 50% of HCC cases worldwide can be attributed to it (5). Shi et al reported that risk for HCC is 15-20 times greater among HBsAg-positive individuals, compared with the HBsAg-negative population (6). However, the mechanisms of initiation and progression of HCC have not been elucidated completely.
Toll-like receptors (TLRs) are vital pattern recognition receptors. They play essential roles in controlling immunity and inflammation, including both innate and acquired immune responses, antigen presentation and most important cytokine gene expression (7). In humans, TLR2 is out-membraned and responds mainly to bacterial surface-associated pathogen-associated molecular patterns (PAMPs), whereas TLR3 is found on the surfaces of endosomes and binds mainly to the nuclear acid of PAMPs from viruses and bacteria (7). TLRs are also expressed in cancer cells. Specifically, TLR2 has been actively investigated in inflammation and cancer. TLR2 signaling induced by the interaction between Listeria monocytogenes infection and tumor cells results directly in tumor cell proliferation (8). In contrast, TLR2 activation has also been reported to inhibit tumor growth by activating mast cells in lung cancer and melanoma (9). A previous study reported that TLR3 activation induced cell death in HCC cells that express endogenous TLR3, suggesting that the activation of TLR3 promotes natural killer cell activation, secretion of interferon-γ (IFN-γ) and cytotoxicity against HCC cells (10). Accordingly, the associations of TLR2 and TLR3 gene polymorphisms with variant cancers have been widely discussed (11, 12). It was reported that there was a potential association between TLR2 polymorphism and gastric cancer (13, 14). Recent findings suggested that TLR2-196 to TLR2-174del polymorphism could increase TLR2 mRNA expression and was associated with higher colorectal cancer (CRC) risk, indicating an important role in CRC genetic susceptibility (15). He JF, et al found that genetic polymorphisms of TLR3 were associated with nasopharyngeal carcinoma susceptibility in Cantonese population (16). In addition, TLR3 (c.1377C/T) was observed to be not correlated with prostate cancer risk (17). However, the results for TLR2 and TLR3 polymorphisms in HBV-related liver diseases still remain ambiguous (14, 18). Therefore, the aim of this study was to determine the function of TLR2 and TLR3 gene polymorphisms in the risk of HBV clearance and HBV-positive HCC development.
Materials and Methods
Study population
The study population consisted of 686 participants with HBV natural clearance, 293 chronic HBV carriers and 395 HBV-positive HCC patients. Participants with HBV natural clearance and HBV persistent carriers were from the Fangchenggang Area Male Health and Examination Survey (FAMHES) in Guangxi (19) and were screened for the HBV markers in 2009. All participants self-reported they were of southern Chinese Han ethnicity. Participants with HBV natural clearances were those who were negative for hepatitis B surface antigen (HBsAg) and hepatitis C antibody (anti-HCV) but positive for both antibodies against hepatitis B surface antigen (anti-HBsAg) and hepatitis B core antigen (anti-HBcAg); HBV persistent carriers were those positive for both HBsAg and anti-HBcAg but negative for anti-HCV. These selected controls were absent of evidence of any kind of cancer. HBV-positive HCC patients were consecutively recruited from the Affiliated Tumor Hospital of Guangxi Medical University between January 2012 and December 2014. HBV-positive HCC patients were diagnosed based on either pathological examinations or α-fetoprotein elevation (>400 ng/mL) combined with imaging examination (i.e., magnetic resonance imaging [MRI] and/or computed tomography [CT]). HCC patients with HCV infection were excluded because HCV infection is rare in Chinese populations. All participants had no history of hepatitis B vaccination. Individuals who had smoked 1 or more cigarettes per day for over 6 months were defined as smokers, and those that consumed 1 or more alcohol drinks a week for over 6 months were considered alcohol drinkers. None of the participants included in the current study were blood relatives, written informed consent was obtained and the study was performed with the approval of the ethics committee of the Affiliated Tumor Hospital of Guangxi Medical University.
Serological testing
The blood samples of HCC came from the specimen bank of the Affiliated Tumor Hospital of Guangxi Medical University. HBV surface antigen (HBsAg), anti-HBs, anti-HBc and HCV antibody (anti-HCV) were measured by enzyme-linked immunosorbent assay. There were 2 negative controls, 3 positive controls and 1 blank control in each reaction plate. One hundred and thirty-eight samples (about 10%) were randomly selected for repeated assay. A 100% concordance rate was achieved.
Genotyping
In this study, single-nucleotide polymorphisms (SNPs) of TLR2 and TLR3 were determined by using publicly available genotype data from the HapMap Project (http://hapmap.ncbi.nlm.nih.gov/index.html.zh). SNP eligibility was based on their location, first selecting every missense variation and then others located in the promoter, 3′UTR and 5′UTR regions with a minor allele frequency (MAF) higher than 0.05 in the Chinese population. In addition, SNPs described to be associated with cancer in relevant publications were also included. Eventually, 2 SNPs (rs3804099 and rs3804100) in TLR2 and 3 SNPs (rs5743305, rs3775296 and rs3775291) in TLR3 were included. Rs3804099, rs3804100 and rs3775291 are located in the exon, rs5743305 in the 5′-UTR and rs3775296 in the 3′-UTR. Genomic DNA was extracted from peripheral blood using a BloodGen Mini Kit (CoWin Biotech). DNA samples were stored at −20°C before genotyping. The genotyping of SNPs were carried out by Shanghai Genesky Bio-Tech Co. Ltd (http://biotech.geneskies.com/index.html) using the improved multiplex ligase detection reaction method (20). The primer sequences are shown in Supplementary Table I (available online at www.biological-markers.com – Single-nucleotide polymorphisms [SNPs] and PCR primer for TLR2 and TLR3 allele genotyping).
Demographic and selected variables in HBV natural clearance study participants, HBV persistent carriers and HCC patients
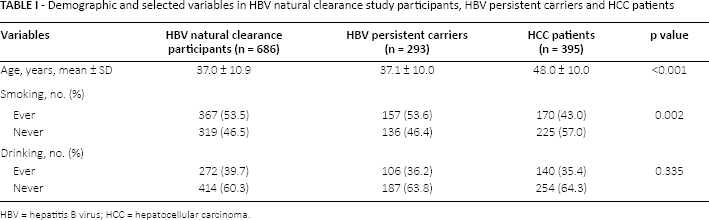
HBV = hepatitis B virus; HCC = hepatocellular carcinoma.
Statistical analysis
Demographic and clinical data for the groups were compared by chi-square test and 1-way ANOVA where appropriate. Hardy-Weinberg equilibrium was tested with the chi-square test with 1 degree of freedom, to compare the observed genotype frequencies with the expected genotype frequencies among the noncancer participants. Binary logistic regression analysis was used to calculate odds ratio (OR) and its 95% confidence intervals (CIs) as a measure of the association between variant allele carriers and the risk for the HBV clearance and HBV-related HCC after adjustments for age and smoking and alcohol consumption status. SHEsis software was employed to analyze the linkage disequilibrium (LD) and haplotype analyses (21). All of the statistical analyses were performed with SPSS 13.0 software, and a p value <0.05 in a 2-sided test was considered statistically significant.
Results
Clinical characteristics of study participants
The demographic and clinical characteristics of the 686 participants with HBV natural clearance, 293 persistent HBV carriers and 395 HBV-related HCC patients are described in Table I. The mean ages (± standard deviation) in the 3 groups were 37.0 ± 10.9, 37.1 ± 10.0 and 48.0 ± 10.0, respectively (p<0.001). In addition, there were more smokers among HCC patients than among HBV carriers and the natural clearance group (p = 0.002 for both comparisons). However, there was no significant difference between the 3 groups with respect to drinking status (p = 0.335).
Genotypes of TLR2 and TLR3
The genotype distributions of TLR2 rs3804099, TLR2 rs3804100, TLR3 rs5743305, TLR3 rs3775296 and TLR3 rs3775291 in participants with HBV natural clearance, HBV persistent carriers and HBV-positive HCC patients are presented in Table II. The observed genotype frequencies for these 5 SNPs in noncancer participants were all in Hardy-Weinberg equilibrium (all p>0.05, results not shown). The genotype distributions of rs3804099, rs5743305 and rs3775296 between HBV persistent carriers and HBV natural clearance, HCC patients and HBV persistent carriers were similar, demonstrating no association for the risk of HBV natural clearance and HCC, respectively (all p>0.05).
Genotypes of TLR2 and TLR3, for HBV natural clearance, HBV persistent carriers and HCC susceptibility (adjusted)
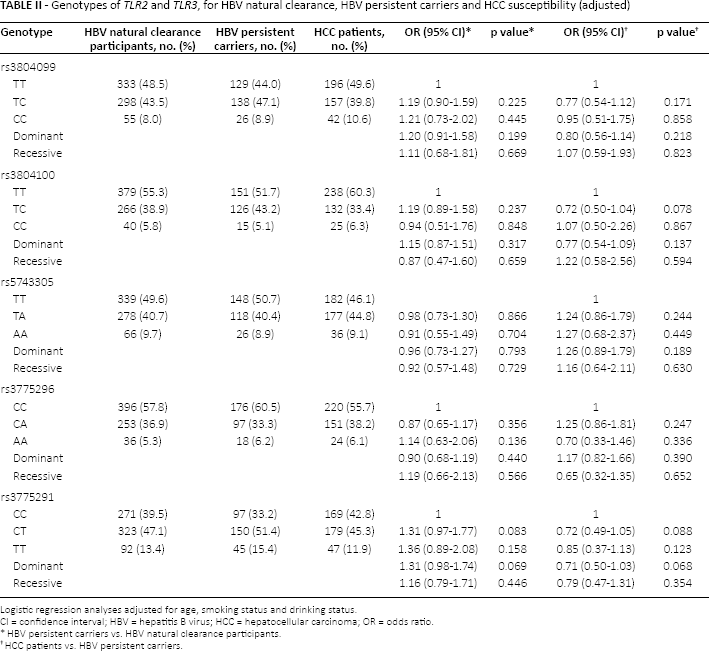
Logistic regression analyses adjusted for age, smoking status and drinking status.
CI = confidence interval; HBV = hepatitis B virus; HCC = hepatocellular carcinoma; OR = odds ratio.
HBV persistent carriers vs. HBV natural clearance participants.
HCC patients vs. HBV persistent carriers.
The frequencies of the TT, TC and CC genotypes of rs3804100 were 51.7%, 43.2% and 5.1% in HBV persistent carriers, and 60.3%, 33.4% and 6.3% in HCC patients, respectively. In logistic regression analyses, rs3804100 genotype TC and TC + CC significant decreased host HCC risk when compared with chronic HBV carriers (OR = 0.67, 95% CI, 0.49-0.91, p = 0.012; and OR = 0.71, 95% CI, 0.52-0.97, p = 0.029, respectively). Analogously, the frequencies of the CC, CT and TT genotypes of rs3775291 were 33.2%, 51.4% and 15.4% in chronic HBV carriers, and 42.8%, 45.3% and 11.9% in HCC patients, respectively. The rs3775291 CT and TT genotypes were associated with a significant decreased risk of HBV-related HCC compared with the CC genotype (OR = 0.96, 95% CI, 0.49-0.95, p = 0.025 and OR = 0.60, 95% CI, 0.37-0.91, p = 0.036, respectively). Moreover, rs3775291 significantly decreased the risk for the development of HCC when compared with persistent HBV carriers in the dominant model (OR = 0.67, 95% CI, 0.49-0.92, p = 0.013) (see Supplementary Table II, available online at www.biological-markers.com – Genotypes of TLR2 and TLR3, HBV natural clearance, HBV persistent carriers and HCC susceptibility). Nevertheless, after adjustment for age, smoking and alcohol consumption status, no significant differences were observed in the genotype distribution of 5 SNPs among 3 groups (all p>0.05) (Tab. II).
Accordingly, to observe whether the relationship between rs3804100 and rs3775291 genotypes and the risk of HCC was modified by epidemiological factors, HBV persistent carriers and HCC patients were stratified on the basis of participants' characteristics including age and smoking and drinking status. As the results showed, smokers or nondrinkers with rs3804100 under the dominant model (TC + CC genotype) were at lower risk of HCC (OR = 0.63, 95% CI, 0.41-0.98, p = 0.038; OR = 0.51, 95% CI, 0.35-0.75, p = 0.001, respectively). After adjustment for age and smoking, a statistically significant difference still existed in nondrinkers (adjusted OR = 0.49, 95% CI, 0.31-0.78, p = 0.003).
Similarly, HBV carriers of rs3775291 CT + TT genotype younger than 40 years may suffer lower risk of HCC (OR = 0.51, 95% CI, 0.30-0.88, p = 0.014). And nonsmokers or nondrinkers under the dominant model (CT + TT genotype) also showed protective effects (OR = 0.50, 95% CI, 0.32-0.78, p = 0.002, OR = 0.65, 95% CI, 0.44-0.96, p = 0.030, respectively). With further adjustment for smoking and drinking, a significant difference was sustained in carriers younger than 40 years (adjusted OR = 0.50, 95% CI, 0.29-0.86, p = 0.013) (Tab. III).
Stratified analysis of rs3804100 and rs3775291 genotype between HCC patients and HBV persistent carriers
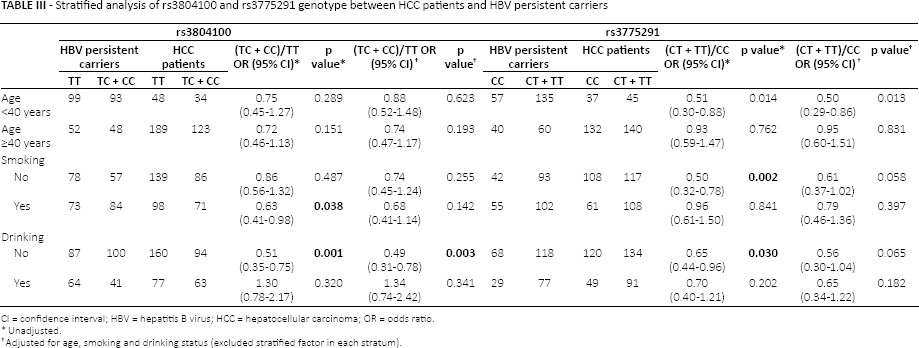
CI = confidence interval; HBV = hepatitis B virus; HCC = hepatocellular carcinoma; OR = odds ratio.
Unadjusted.
Adjusted for age, smoking and drinking status (excluded stratified factor in each stratum).
Haplotype analyses of TLR2 and TLR3 gene polymorphisms and HBV natural clearance and HCC risk
Haplotype analyses were further performed in participants with HBV natural clearance, HBV persistent carriers and HBV-related HCC patients, to evaluate the haplotype frequencies of polymorphisms located in the same chromosome regions and to assess the effect of haplotypes containing TLR2 and TLR3 variant alleles. LD information for these 5 SNPs is presented in Supplementary Table III (available online at www.biological-markers.com – Linkage disequilibrium (LD) information for TLR2 and TLR3 variations). The haplotype distributions in the 3 groups are shown in Table IV. A total of 9 haplotypes were derived from the observed genotypes. The most frequent haplotype among the 3 groups was TTTCT (0.193, 0.238 and 0.183, respectively), and TTTCT was observed to promote the progress of HBV clearance and inhibit the development of HBV-related HCC (OR = 0.77, 95% CI, 0.61-0.97, p = 0.029; and OR = 0.72, 95% CI, 0.55-0.94, p = 0.016, respectively). In addition, we found that CCACC and CCTCT haplotypes may contribute to reducing the risk of HCC (OR = 0.64, 95% CI, 0.40-1.00, p = 0.048; and OR = 0.43, 95% CI, 0.28-0.68, p<0.001, respectively). In contrast, CCTCC and TTACC haplotypes were positively associated with HCC (OR = 1.79, 95% CI, 1.00-3.20, p = 0.047 and OR = 1.45, 95% CI, 1.07-1.96, p = 0.017, respectively).
Results of association analysis for TLR2 and TLR3 haplotypes
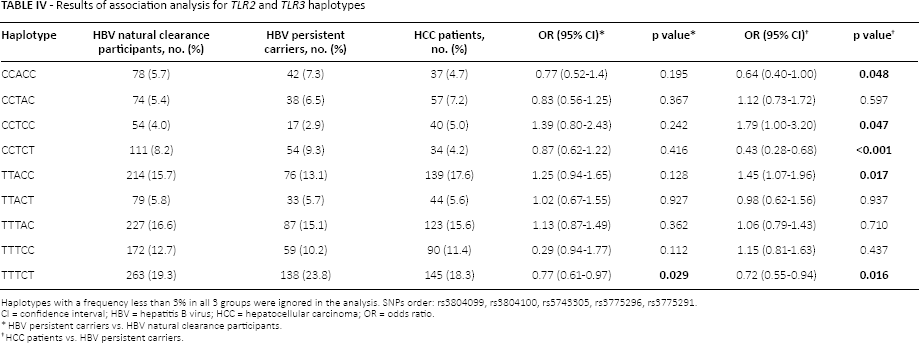
Haplotypes with a frequency less than 3% in all 3 groups were ignored in the analysis. SNPs order: rs3804099, rs3804100, rs5743305, rs3775296, rs3775291.
CI = confidence interval; HBV = hepatitis B virus; HCC = hepatocellular carcinoma; OR = odds ratio.
HBV persistent carriers vs. HBV natural clearance participants.
HCC patients vs. HBV persistent carriers.
Discussion
It is well established that multiple risk factors contribute to hepatocarcinogenesis. Nevertheless, despite the fact that chronic hepatitis B infection is a major cause of HCC, only a fraction of infected patients develop HCC during their lifetime. Therefore, it is essential to clarify other potential protective or risk factors that are connected to HCC susceptibility. As the effects of TLRs gene variants in HBV-related liver disease are not well understood, we conducted the current study to elucidate the association between TLR2 and TLR3 polymorphisms and the risk of HBV clearance and HBV-related HCC incidence in a southern Chinese population.
Rs3804099 and rs3804100 of TLR2 are synonymous SNPs. In the present study, LD analysis showed that these 2 TLR2 synonymous SNPs had high LD (D′ = 0.996; R 2 = 0.795). Xie JJ, et al (22) reported that close associations were observed between rs3804099 and rs3804100 polymorphisms and the risk of HCC, results suggesting that individuals carrying the heterozygous genotypes of these 2 SNPs were at lower risk of HCC than those carrying wild-type homozygous genotypes (22), which was partially in conformity with our findings. In the stratified analysis, we found that carriers of the TC + CC genotype decreased their HBV-positive HCC risk in comparison with TT carriers of TLR2 rs3804100 who were nondrinkers. The biological plausibility of interaction between TLR2 and alcohol is supported by an alcohol-induced inflammatory response together with the mediator roles that TLRs play in live inflammation. Cherfils-Vicini J, et al reported that TLR up-regulated signaling can directly favor tumor development (23). It can up-regulate the nuclear factor kappa-B (NF-κB) cascade and produce antiapoptotic proteins that contribute to carcinogenesis and cancer cell proliferation (24). We reason that polymorphisms could affect the TLR2 signaling to hepatocytes, especially regarding inflammation status, and regulate tumor development via different immune mechanisms which prevent protumor inflammatory skewing, thereby inhibiting the progression of HCC. Moreover, even synonymous SNPs may function differently in regulating immune response and cell proliferation.
The -976T/A SNP (rs5743305) is located in the promoter region within 1 kb upstream of exon 1 in the TLR3 gene and might influence transcriptional activity of TLR3 (17). However, our study did not observe a relationship between rs5743305 polymorphism and HBV-positive HCC, which was in line with what was reported by Li et al (25). TLR3 gene rs3775291 (C1234T in mRNA) is a missense mutation that leads to the replacement of a leucine by a phenylalanine at amino acid position 412 (26). Previous studies have reported the relationship between rs3775291 gene variant and various types of cancer. Chen et al demonstrated that rs3775291 was associated with an increased risk of relapse in breast cancer (27). Other studies reported that rs3775291 polymorphism may be a potential prognostic biomarker of oral carcinoma and lung cancer (28, 29). However, the association between rs3775291 SNP and HCC has scarcely been discussed.
Our study suggested that carriers younger than 40 years with TLR3 rs3775291 could have reduced susceptibility to HCC when they have the CT + TT genotype compared with the CC, showing that rs3755291 polymorphism may be a protective factor for HBV-positive HCC. As previously reported, the expression of TLR3 in HCC tissues may exert a synergistic effect on apoptosis and inhibit the proliferation of HCC cells and angiogenesis (30). We speculated that a missense polymorphism (rs3775291) in the TLR3 gene could enhance its role in anticancer immune stimulator and the apoptotic process. Meanwhile, it may inhibit the activation of NF-κB (31). However, these results are in contrast to those reported by Li et al, who found that the prevalences of CT genotype and TT genotype were significantly increased in the HCC cases compared with controls (OR = 1.51, 95% CI, 1.22-1.93; OR = 3.19, 95% CI, 1.82-5.39) (25). The study by Li et al included participants without malignancies as controls irrespective of their HBV exposure. Thus the discrepancy might be due to the difference in control populations. Further, the orientation of the TLR3 protein may also account for its diverse function in tumor cells (30, 31). Yoneda et al found that functional TLR3 was expressed in both the cell surface and in the cytoplasm of HCC cells. Intracellular TLR3 signaling is involved in cell death, while cell surface TLR3 signaling is responsible for activation of NF-κB (31).
There were several limitations to our study. First, the number of participants in our study was moderate, and the statistical power was limited. Large population-based prospective studies are warranted to further elucidate the impact of TLR2/TLR3 SNPs on HBV clearance and HBV-related HCC susceptibility. Second, the participants were only selected from the Guangxi male population. In consequence, prudence is needed when extrapolating our results to females. Third, our cases were chosen from a hospital, and the controls were from communities, which may not be representative of the general population.
Conclusions
In a Chinese male population, there were no associations between TLR2 and TLR3 polymorphisms and HBV natural clearance. However, our study revealed that TLR2 rs3804100 and TLR3 rs3775291 gene polymorphisms may be protective factors in HBV-positive HCC. Further research with large sample sizes may be required to warrant the genetic effects of TLR2 and TLR3 polymorphisms on HBV-positive HCC.
Footnotes
Financial support: This study was supported by the Guangxi Natural Science Foundation (grant no. 2012GXNSFBA053117), Guangxi Natural Science Fund for Innovation Research Team (2013GXNSFFA019002), National Natural Science Foundation of China(grant no. 81060169), and Science Research Foundation of Guangxi (GUIKEQING 0542064, GUIKEGONG 10124001A-31, ZHONG 200610).
Conflict of interest: There was no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.