
Abstract
Introduction
The aim of this study was to elucidate the clinicopathological significance of HER2 expression and the diagnostic accuracy of HER2 immunohistochemistry (IHC) in colorectal cancer (CRC). A total of 2,573 CRC cases from 13 eligible studies were included.
Methods
We performed a meta-analysis to examine the correlations between HER2 expression and clinicopathological characteristics in CRC. Concordance analysis between HER2 IHC and in situ hybridization (ISH) and diagnostic test accuracy review was conducted.
Results
The estimated rate of HER2 IHC overexpression was 0.162 (95% confidence interval [CI] 0.106-0.240). HER2 IHC overexpression was significantly correlated with lymph node metastasis and distant metastasis but not tumor depth. HER2 IHC overexpression was not correlated with overall survival. The concordance rates between IHC and ISH were 0.968 (95% CI 0.881-0.992), 0.377 (95% CI 0.225-0.557) and 0.780 (95% CI 0.390-0.952) for HER2 IHC scores of 0/1+, 2+ and 3+, respectively. The diagnostic test accuracy review of HER2 IHC revealed that the pooled sensitivity and specificity were 0.71 (95% CI 0.58-0.82) and 0.96 (95% CI 0.94-0.97), respectively. The diagnostic odds ratio and area under the summary receiver operating characteristic curve were 51.34 (95% CI 3.82-690.54) and 0.9704, respectively.
Conclusions
HER2 IHC overexpression was significantly correlated with lymph node metastasis and distant metastasis. CRC cases with HER2 IHC scores of 0/1+ exhibited good agreement with the ISH data. However, additional ISH analysis is needed to confirm HER2 status in cases with IHC scores of 2+ or 3+.
Keywords
Introduction
Colorectal cancer (CRC) is one of the most common malignant tumors worldwide (1). Although cytotoxic agents and surgical techniques have yielded improved survival in CRC, mortality rates vary worldwide according to treatment availability (1). Recently, several biological and molecular markers, such as BRAF and HER2, have been applied to patient treatment. The HER2 oncogene, also known as ERBB2 or neu, encodes a transmembrane receptor glycoprotein with tyrosine kinase activity (2). HER2 overexpression is found in various malignant tumors including breast, gastric and lung cancers (2-3-4). Although HER2 is associated with tumor cell adhesion, migration and differentiation (2), its clinicopathological significance in CRC is not fully understood. Targeted therapy using HER2 monoclonal antibodies has been shown to yield survival benefits; this modality is one of the most important treatment options in advanced gastric cancer (5). Accurate evaluation of HER2 status is important for the success of HER2 monoclonal antibody-based treatments. However, in contrast to gastric and breast cancers, the therapeutic effect of HER2 monoclonal antibodies and the diagnostic accuracy of HER2 immunohistochemistry (IHC) in CRC have not yet been elucidated.
In the present study, we determined the clinicopathological significance of HER2 overexpression in CRC and examined the correlation of HER2 overexpression with survival. With the aim of using HER2 IHC data to classify HER2 status, the diagnostic accuracy of HER2 IHC in CRC was evaluated.
Materials and methods
Published Study Search and Selection Criteria
Relevant articles were obtained by searching the PubMed and MEDLINE databases on November 30, 2015. These databases were searched using the following keywords: “colon”, “rectum”, “colorectum”, and “HER2” or “HER-2”. The titles and abstracts of all identified articles were then screened for exclusion. Review articles were also screened to find additional eligible studies. The following inclusion and exclusion criteria were applied to the search results: 1) HER2 status was investigated in human CRC tissue, 2) correlations between HER2 IHC and clinicopathological parameters or in situ hybridization (ISH) were reported, 3) case reports and non-original articles were excluded, and 4) all publications were in English.
Data Extraction
Two authors independently extracted data from all eligible studies (3, 6-7-8-9-10-11-12-13-14-15-16-17). The following data were extracted from each study: the first author's name, year of publication, study location, antibody clone and manufacturer, number of patients analyzed, and ISH method. For meta-analysis, all data associated with the IHC results (scores 0, 1+, 2+ and 3+) and ISH results (number of amplifications and non-amplifications) were extracted.
Statistical Analysis
For the meta-analysis, the Comprehensive Meta-Analysis software package (Biostat) was used. We investigated the correlations between HER2 IHC overexpression and clinicopathological characteristics using data from all eligible studies. In the present study, HER2 IHC 2+ and 3+ cases were considered to have HER2 protein overexpression, as described previously (9, 16, 18). In addition, the rates of HER2 gene amplification according to HER2 IHC scores were investigated for concordance analysis. The concordance rates between HER2 IHC and ISH were measured by agreement rates. Heterogeneity between the studies was determined by calculating the Q and I2 values and is reported as p values. Sensitivity analysis was conducted to assess the heterogeneity of the eligible studies and the impact of each study on the combined effect. For quantitative aggregation of survival results, the correlation between HER2 IHC overexpression and survival was analyzed according to hazard ratios (HRs) obtained from eligible studies. All graphical representations of survival distributions in eligible studies were used, and survival rates were extracted at specified times to reconstruct the HR estimates and their variances. This method relied on the assumption that patients were censored at a constant rate during the time intervals (19). To reduce interpretation variability, all published survival curves were read independently by 2 authors. The HRs were then combined into an overall HR using Peto's method (20). In the current meta-analysis, a random-effects model was more suitable than a fixed-effects model because the eligible studies used various diagnostic criteria and populations. To assess publication bias, Begg's funnel plot and Egger's test were used. If significant publication bias was found, the fail-safe N and trim-fill tests were additionally conducted to confirm the degree of publication bias. Results were considered statistically significant at p<0.05.
Diagnostic test accuracy review was carried out using the Meta-Disc program (version 1.4) (Unit of Clinical Biostatistics, the Ramón y Cajal Hospital, Madrid, Spain) (21). Forest plots for the sensitivity and specificity of the summary receiver operating characteristic (SROC) curves were obtained. The area under the curve (AUC) and the diagnostic odds ratio (OR) were calculated by the Meta-Disc program.
Results
Selection and Characteristics of the Studies
In this systematic review and meta-analysis, 223 reports were identified in the database search. Of these reports, 118 were excluded because of insufficient or no information regarding correlations between HER2 IHC and clinicopathological parameters. In addition, 78 reports were excluded because they reported the results of non-CRC diseases or used animals or cell lines, whereas 14 were excluded because they were not in English or were not original articles. Finally, 2,573 patients of 13 studies were included in this systematic review and meta-analysis (Fig. 1 and Tab. I). The overall HER2 IHC overexpression rate in CRC was 17.0% (437 of 2,573 patients).
Main characteristics of the eligible studies
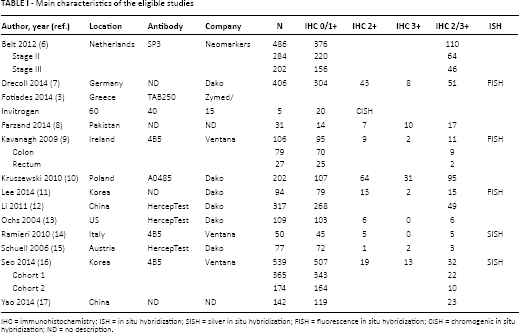
IHC = immunohistochemistry; ISH = in situ hybridization; SISH = silver in situ hybridization; FISH = fluorescence in situ hybridization; CISH = chromogenic in situ hybridization; ND = no description.
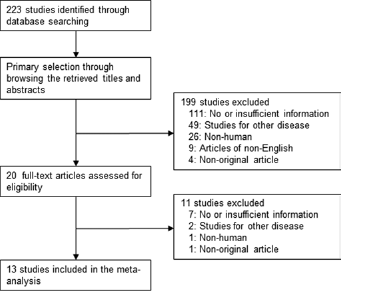
Flowchart for study search and selection methods.
Systematic Review and Meta-Analysis
Correlations between HER2 IHC Overexpression and Clinicopathological Parameters
In CRC, the estimated HER2 IHC overexpression rate was 0.162 (95% CI 0.106-0.240). The HER2 IHC overexpression rates for males and females were 0.177 (95% CI 0.097-0.302) and 0.224 (95% CI 0.086-0.471), respectively. HER2 IHC overexpression rates in the right and left colon were not significantly different (0.099, 95% CI 0.052-0.181 vs. 0.107, 95% CI 0.064-0.174) (Tab. II). T3-4 tumors showed slightly higher rates of HER2 overexpression than T1-2 tumors (0.226, 95% CI 0.115-0.397 vs. 0.189, 95% CI 0.077-0.397). The HER2 IHC overexpression rate in patients with lymph node metastasis was significantly higher than that in patients without lymph node metastasis (0.356, 95% CI 0.199-0.551 vs. 0.255, 95% CI 0.119-0.466). In addition, patients with distant metastasis showed a significantly higher rate of HER2 IHC overexpression than patients without distant metastasis (0.277, 95% CI 0.203-0.367 vs. 0.131, 95% CI 0.108-0.158). No significant publication bias was observed in the primary tests (Begg's funnel plot and Egger's test) or in the secondary tests (fail-safe N and trim-fill tests). The meta-analysis of overall survival did not reveal a significant correlation between HER2 IHC overexpression and overall survival rate (HR 0.960, 95% CI 0.776-1.188) (Fig. 2).
Meta-analysis for overall HER2 overexpression rate in colorectal cancer
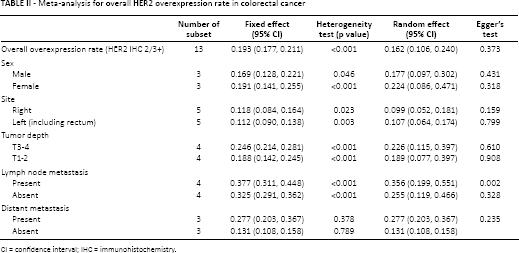
CI = confidence interval; IHC = immunohistochemistry.
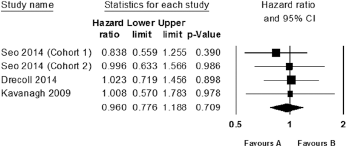
Forest plot diagram for the correlation between HER2 immunohistochemistry results and overall survival rate (cohort 1: 365 consecutive colorectal cancer patients; cohort 2: 174 advanced colorectal cancer patients with synchronous or metachronous distant metastasis who had undergone surgical resection for primary colorectal cancer).
Diagnostic Accuracy of HER2 IHC
We next evaluated the concordance between HER2 IHC and ISH results in CRC. The overall concordance rate between HER2 IHC and ISH was 0.777 (95% CI 0.502-0.924). In subgroup analysis based on HER2 IHC scores, the concordance rates of HER2 IHC scores of 0/1+, 2+ and 3+ were 0.968 (95% CI 0.881-0.992), 0.377 (95% CI 0.225-0.557) and 0.780 (95% CI 0.390-0.952), respectively (Tab. III). Egger's test did not reveal any significant publication bias in the IHC 0/1+, 2+ or 3+ group (p = 0.849, p = 0.777 and p = 0.146, respectively), and no asymmetry was identified in any of the Begg's funnel plots.
Concordance analysis between HER2 immunohistochemistry and in situ hybridization in colorectal cancer
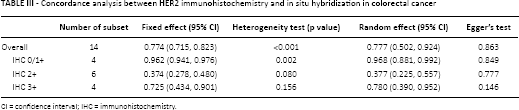
CI = confidence interval; IHC = immunohistochemistry.
Next, we performed diagnostic test accuracy review to elucidate the diagnostic accuracy of HER2 IHC. The sensitivity and specificity of studies with HER2 IHC scores of 2+ and 3+ ranged from 0.14 to 1.00 and 0.77 to 1.00, respectively. The pooled sensitivity and specificity were 0.71 (95% CI 0.58-0.82) and 0.96 (95% CI 0.94-0.97), respectively. The diagnostic OR and AUC on the SROC curve were 51.34 (95% CI 3.82-690.54) and 0.9704, respectively.
Discussion
Targeted therapy using HER2 monoclonal antibodies has recently been applied to patients with CRC. However, unlike gastric and breast cancers, detailed evaluation criteria for HER2 status have not yet been established in CRC. The present study is the first meta-analysis to examine the clinicopathological significance of HER2 IHC overexpression and to investigate the concordance between HER IHC and ISH in CRC. This study had 5 major findings. First, the estimated HER2 IHC overexpression rate in CRC was 16.2%. Second, HER2 IHC overexpression was significantly correlated with lymph node metastasis and distant metastasis, but not tumor depth. Third, HER2 IHC overexpression was not correlated with survival rate in CRC. Fourth, HER2 IHC scores of 0/1+ and ISH exhibited higher concordance rates in CRC. Fifth, HER2 IHC scores of 3+ exhibited a lower concordance rate in CRC compared with gastric and breast cancers.
In the current systematic review, the HER2 IHC overexpression rates ranged from 3.9% to 54.8% in the eligible studies (3, 6-7-8-9-10-11-12-13-14-15-16-17) and the overall rate was 17.0%, similar to that in gastric cancer (2). In the present meta-analysis, the estimated HER2 IHC overexpression rate was 0.162 (95% CI 0.106-0.240). Since not all eligible studies confirmed their rates by ISH, a conclusive rate of HER2 overexpression/gene amplification in CRC could not be obtained. In the eligible studies that did conduct ISH, the HER2 overexpression/gene amplification rates ranged from 2.0% to 18.3%, with an overall rate of 6.5% (3, 11, 14, 16). In the present meta-analysis, HER2 IHC overexpression was not correlated with poor prognosis (HR 0.960, 95% CI 0.776-1.188) as in gastric cancer (22, 23). However, CRC with HER2 IHC overexpression showed higher rates of lymph node and distant metastasis than CRC without HER2 IHC overexpression. Some eligible studies included only stage II and III CRC (6). Thus, selection bias cannot be excluded as a possible cause for this finding. However, potential correlations between HER2 IHC overexpression and tumor stages could not be investigated due to insufficient information.
In clinical practice, HER2 ISH data are not available for all patients with CRC. Thus, accurate screening tools such as HER2 IHC assays may be useful for selecting patients who need confirmative ISH, especially patients with gastric or breast cancer. However, the diagnostic accuracy of HER2 IHC for predicting HER2 status must be confirmed before this approach can be used. In our diagnostic test accuracy review, the pooled sensitivity, pooled specificity and diagnostic OR were 0.71 (95% CI 0.58-0.82), 0.96 (95% CI 0.94-0.97) and 51.34 (95% CI 3.82-690.54), respectively. In addition, the AUC on the SROC curve was 0.9704, which is very close to 1. Therefore, HER2 IHC could be a useful screening tool for selecting patients with CRC who should receive certain treatments.
Although several studies have reported the concordance between HER2 IHC and ISH in CRC, conclusive information is not yet available. The HER2 overexpression/gene amplification rate could be lower than that revealed by HER2 IHC because of false positive cases with HER2 IHC scores of 2+ and 3+. More detailed analyses of HER2 IHC scores will be needed to use this metric as a screening tool in CRC. In CRC, the concordance rate of HER2 IHC scores of 2+ between HER2 IHC and ISH was 0.377 (95% CI 0.225-0.557), similar to gastric and breast cancers (2, 24). The HER2 IHC 2+ group of CRC cases was more heterogeneous than the HER2 IHC 0/1+ and 3+ groups. In gastric and breast cancers, cases with HER2 IHC scores of 0/1+ or 3+ are confirmed without additional ISH tests. In the current CRC meta-analysis, the concordance rates of HER2 IHC 0/1+ and 3+ cases were 0.968 (95% CI 0.881-0.992) and 0.780 (95% CI 0.390-0.952), respectively. Since the concordance rate of HER2 IHC 0/1+ cases was relatively high, HER2 IHC 0/1+ cases can be considered HER2-negative without any additional ISH testing. In a previous meta-analysis, the concordance rates between HER2 IHC and ISH in HER2 IHC 3+ cases was 0.915 (95% CI 0.882-0.939) (2). However, in CRC, the discordance rate between HER2 IHC and ISH in HER2 IHC score 3+ cases was higher (0.220) than in gastric cancer (2). In daily practice, precise evaluation of HER2 status in the HER2 IHC 3+ group without additional ISH tests may be more important than in the HER2 IHC 2+ group. Our results indicate that different algorithms will be needed in CRC than in gastric and breast cancers. Moreover, our data suggest that additional ISH testing is required to confirm HER2 status in HER2 IHC score 3+ CRC cases.
There are some limitations to the current study. First, since the evaluation criteria for HER2 IHC in CRC have not yet been fully established, some eligible studies used the criteria of gastric cancer. As mentioned above, the concordance rate of HER2 3+ cases was 0.780 (95% CI 0.390-0.952), meaning that additional tests will be required to eliminate false positive cases. However, our results indicate that HER2 IHC 0/1+ cases can be classified as HER2-negative cases in CRC. Second, we investigated the correlation between HER2 IHC overexpression and survival rate in 4 eligible studies. Thus, this correlation is somewhat limited in that only a small number of studies were included. Third, subgroup analyses based on HER2 antibodies or ISH methods could not be performed due to insufficient information and a lack of eligible studies. In a previous study of gastric cancer, the concordance rates between HER2 IHC and ISH were not significantly different according to many different factors, including HER2 antibodies and ISH (2). In addition, in the present study we were unable to examine whether the specimen type (i.e., biopsied vs. surgically resected) affects concordance. Fourth, Wu et al (25) reported the correlation between HER2 status and clinicopathological parameters through meta-analysis. Their meta-analysis included studies which used HER2 IHC as well as Western blot and fluorescence ISH, limiting the interpretation of the clinicopathological significance of HER2 IHC overexpression (25). The current study on the other hand included eligible studies that used HER2 IHC and carried out meta-analysis and diagnostic test accuracy review of HER2 IHC as well as concordance analysis between HER2 IHC and ISH, unlike the meta-analysis by Wu (25). Therefore, the results obtained with our meta-analysis will be suitable for the interpretation of the clinicopathological significance and the diagnostic role of HER2 IHC.
In conclusion, we showed that HER2 IHC overexpression was present in 16.2% of all patients with CRC and that HER2 IHC overexpression was significantly correlated with lymph node metastasis and distant metastasis. HER2 IHC exhibited good concordance with HER2 ISH in HER2 IHC score 0/1+ cases and showed high diagnostic accuracy. However, HER2 IHC score 2+ and 3+ cases require additional ISH testing to confirm their HER2 status.
Footnotes
Financial support: This work was supported by the 2015 Inje University research grant (R07) for Kyeongmee Park.
Conflict of interest: The authors declare that they have no conflict of interest.