
Abstract
Purpose:
This study aimed to elucidate the concordance between human epidermal growth factor receptor 2 (HER2) immunohistochemistry (IHC) and in situ hybridization (ISH) and the diagnostic accuracy of HER2 IHC in non-small cell lung cancer (NSCLC) through a meta-analysis and diagnostic test accuracy review.
Methods:
Seven eligible studies and 1,217 patients with NSCLC were included in the review. The concordance between HER2 IHC and ISH was analyzed. To confirm the diagnostic accuracy of HER2 IHC, the sensitivity and specificity were analyzed and the area under the curve (AUC) in the summary receiver operating characteristic (SROC) curve was calculated.
Results:
The concordance rate between HER2 IHC and ISH was 0.795 (95% confidence interval [CI] 0.534-0.929). In the HER2 IHC-negative (score 0/1+) subgroup, the concordance rate was 0.975 (95% CI 0.854-0.996). The concordance rates of the HER2 IHC score 2+ and 3+ subgroups were 0.091 (95% CI 0.039-0.197) and 0.665 (95% CI 0.446-0.830), respectively. In diagnostic test accuracy review, the pooled sensitivity and specificity were 0.67 (95% CI 0.54-0.78) and 0.89 (95% CI 0.87-0.91), respectively. The AUC in the SROC curve was 0.891 and the diagnostic odds ratio was 16.99 (95% CI 5.08-56.76).
Conclusions:
HER2 IHC was largely in agreement with ISH in cases of HER2 IHC score 0/1+. Because the concordance rates of HER2 IHC score 2/3+ cases were lower than that of HER2 IHC score 0/1+ cases, further studies for detailed analysis criteria for HER2 IHC score 2+ or 3+ are required.
Keywords
Introduction
Non-small cell lung cancer (NSCLC) is one of the actively studied cancers for developing targeted therapies (1, 2). The information available regarding EGFR, KRAS, BRAF, ALK, ROS1 and MET gene mutations in NSCLC is consistently increasing. In addition, human epidermal growth factor receptor 2 (HER2) is expressed in many cancers, including NSCLC (3). HER2 is a transmembrane receptor glycoprotein with tyrosine kinase activity and is involved in adhesion, migration and differentiation of tumor cells (3-5). In NSCLC, the most common HER2 mutations are exon 20 insertions and extracellular domain mutations (1, 6). HER2 amplification has been reported to occur in up to 22.8% of NSCLCs (7-16). The prognostic role of HER2 status in NSCLC is controversial (2, 3, 13) and may differ depending on the detection method used, immunohistochemistry (IHC) or in situ hybridization (ISH) (3). The therapeutic effect of targeted HER2 monoclonal antibodies such as trastuzumab has not been fully elucidated in NSCLC (17). However, accurate evaluation of HER2 status can be very important in the evaluation of this therapeutic effect. HER2 IHC and ISH are currently used as diagnostic tests for HER2 status. In breast and gastric cancers, it is common practice to obtain additional ISH confirmation for cases with a HER2 IHC score of 2+ (4, 18). The concordance between HER2 IHC and ISH results for cases with HER2 IHC scores 0/1+ or 3+ can be even more important, because such cases are confirmed without additional ISH tests. However, no detailed information about the concordance between HER2 IHC and ISH in NSCLC cases is available. Though various factors are known to contribute to the discordance between HER2 IHC and ISH, these factors are not fully understood.
To elucidate the concordance rate between HER2 IHC and ISH, we performed a meta-analysis and subgroup analysis based on detection methods and histological type of NSCLC. In addition, the diagnostic accuracy and usefulness of the HER2 IHC scoring system in NSCLC were evaluated by a diagnostic test accuracy review.
Materials and methods
Search and selection criteria
Relevant articles were obtained by searching the PubMed and MEDLINE databases through December 31, 2016. These databases were searched using the following key words: “lung cancer OR non-small cell lung cancer”, “HER2” OR “HER-2”, and “immunohistochemistry”. The titles and abstracts of all searched articles were screened for exclusion. Review articles were also screened to find additional eligible studies. The search results were then reviewed and included if the study was on human NSCLC and there was information about the correlation between HER2 IHC and ISH, and excluded if the articles were case reports, non-original articles, or publications that were not in English.
Data extraction
Data from all eligible studies (19-25) were extracted by 2 independent authors and included the following: the first author’s name, year of publication, study location, antibody clone and manufacturer, cutoff value, ISH method, number of patients analyzed, and histological type of NSCLC. For the meta-analysis we extracted all data associated with IHC results (scores 0, 1+, 2+ and 3+) and ISH results (numbers of amplification and non-amplification).
Statistical analysis
To perform the meta-analysis, we analyzed all data using the Comprehensive Meta-Analysis software package (Biostat). The concordance rates were measured using agreement rates between HER2 IHC and ISH. Because eligible studies used various antibodies and evaluation criteria, a random-effects model was more suitable than a fixed-effects model. In addition, subgroup analyses based on HER2 scores and ISH methods were performed. Heterogeneity between the studies was checked using the Q and I2 statistics and presented using p values. Sensitivity analysis was performed to evaluate the heterogeneity of eligible studies and the impact of each study on the combined effect size. Publication bias was assessed using Begg’s funnel plot and Egger’s test. If significant publication bias was found, the fail-safe N and trim-and-fill tests were performed to confirm the degree of publication bias. The results were 2-sided and considered statistically significant when p<0.05.
Diagnostic test accuracy review was carried out using the Meta-Disc program (version 1.4) (26). Forest plots for sensitivity and specificity, and the summary receiver operating characteristic (SROC) curve were obtained. The area under the curve (AUC) in the SROC curve and the diagnostic odds ratio (OR) were calculated using the Meta-Disc program.
Results
Selection and characteristics of the studies
A total of 264 reports were identified in the database search. Among them, 112 were excluded because of insufficient information on the correlation between HER2 IHC and ISH. Other studies were excluded because they reported the results of other diseases (n = 103), used animals or cell lines (n = 12), or were non-English (n = 5) or non-original articles (n = 25). Finally, 7 studies were included in this analysis (Fig. 1 and Tab. I), which contained data from 1,217 patients with NSCLC. The included cases were primarily assessed by HER2 IHC and the IHC result was confirmed by HER2 ISH.
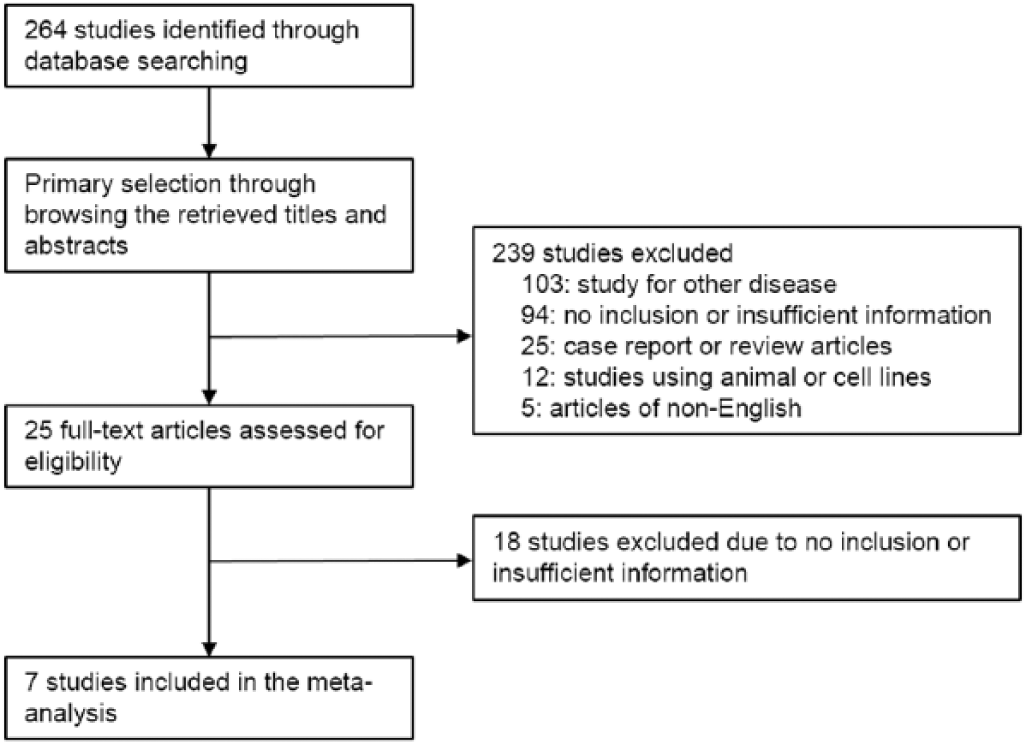
Flowchart for study search and selection methods.
Main characteristics of the eligible studies
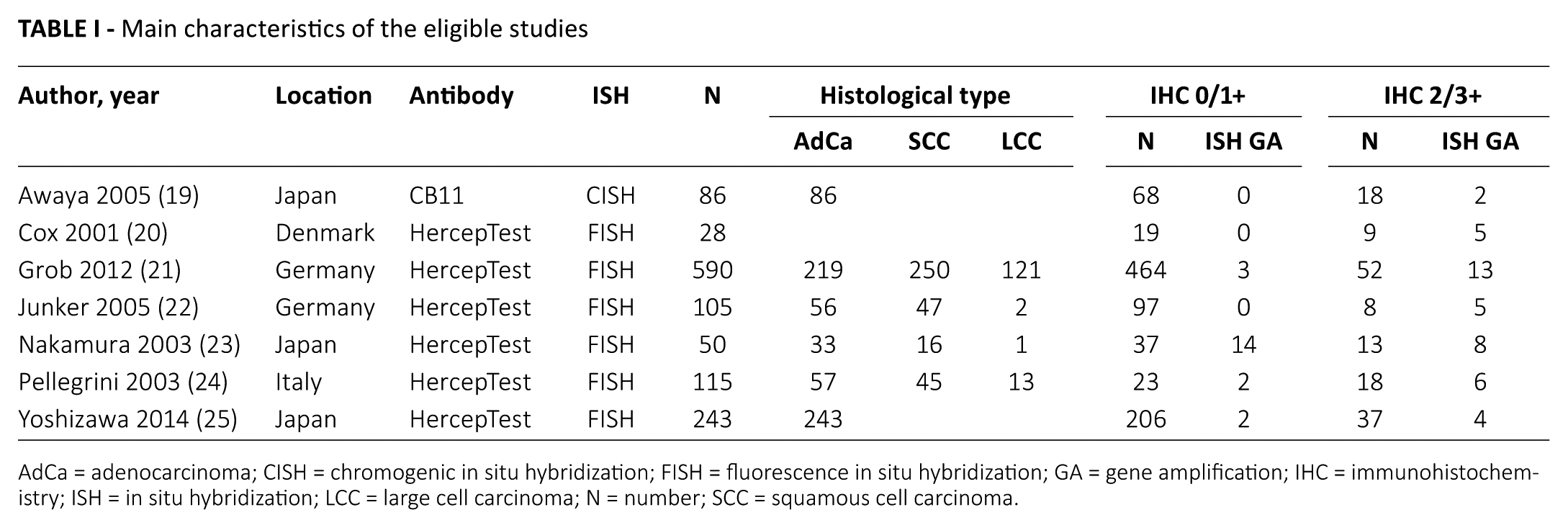
AdCa = adenocarcinoma; CISH = chromogenic in situ hybridization; FISH = fluorescence in situ hybridization; GA = gene amplification; IHC = immunohistochemistry; ISH = in situ hybridization; LCC = large cell carcinoma; N = number; SCC = squamous cell carcinoma.
Concordance analysis between HER2 IHC and ISH
The overall estimated concordance rate was 0.795 (95% confidence interval [CI] 0.534-0.929). In subgroup analysis based on HER2 IHC scores, the concordance rates were 0.975 (95% CI 0.854-0.996) and 0.329 (95% CI 0.188-0.509) in the HER2 IHC score 0/1+ and 2/3+ subgroups, respectively. In addition, the concordance rates of the HER2 IHC score 2+ and 3+ subgroups were 0.091 (95% CI 0.039-0.197) and 0.665 (95% CI 0.446-0.830), respectively. In subgroup analysis based on ISH methods, there was no significant difference in concordance rates between fluorescence ISH (FISH) and chromogenic ISH (CISH) (Tab. II). No significant publication bias was found.
Concordance analysis between HER2 immunohistochemistry and in situ hybridization
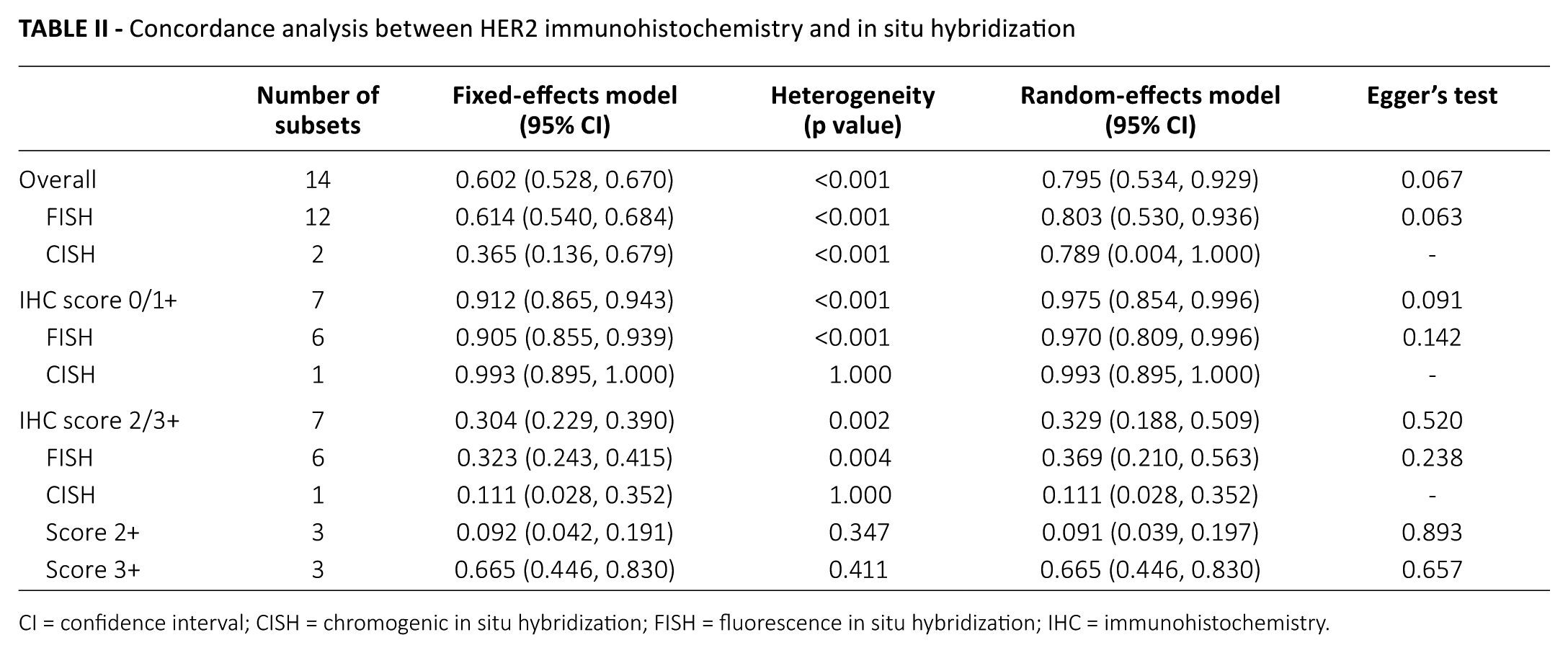
CI = confidence interval; CISH = chromogenic in situ hybridization; FISH = fluorescence in situ hybridization; IHC = immunohistochemistry.
In the adenocarcinoma subgroup, the concordance rate was 0.776 (95% CI 0.072-0.994) when all cases were considered. However, in adenocarcinomas with a HER2 IHC score 2/3+, the concordance rate was significantly lower than in adenocarcinomas with a HER2 IHC score 0/1+ (0.109, 95% CI 0.050-0.222 vs. 0.991, 95% CI 0.969-0.997; p<0.001). In addition, in adenocarcinomas with a HER2 IHC score of 2/3+, the concordance rate was significantly lower than in the mixed subgroup (0.109, 95% CI 0.050-0.222 vs. 0.437, 95% CI 0.274-0.615; p = 0.006). In HER2 IHC score 2/3+ cases, the mixed subgroup was found to have a publication bias when assessed using Egger’s test (p = 0.024). To define the degree of publication bias, secondary assessments using the fail-safe N and trim-and-fill tests were performed. Publication biases were not significant in the fail-safe N test or the trim-and-fill test.
Diagnostic test accuracy review
In diagnostic test accuracy review, cases with HER2 IHC scores 2+ and 3+ were considered IHC positive. The pooled sensitivity and specificity were 0.67 (95% CI 0.54-0.78) and 0.89 (95% CI 0.87-0.91), respectively. The ranges of sensitivity and specificity of eligible studies were from 0.36 to 1.00 and from 0.64 to 0.97, respectively (Fig. 2). The SROC curve is shown in Figure 3, and the AUC of the SROC curve was 0.891. The diagnostic OR was 16.99 (95% CI 5.08-56.76), and the range of diagnostic ORs in eligible studies was from 2.63 to 306.43.
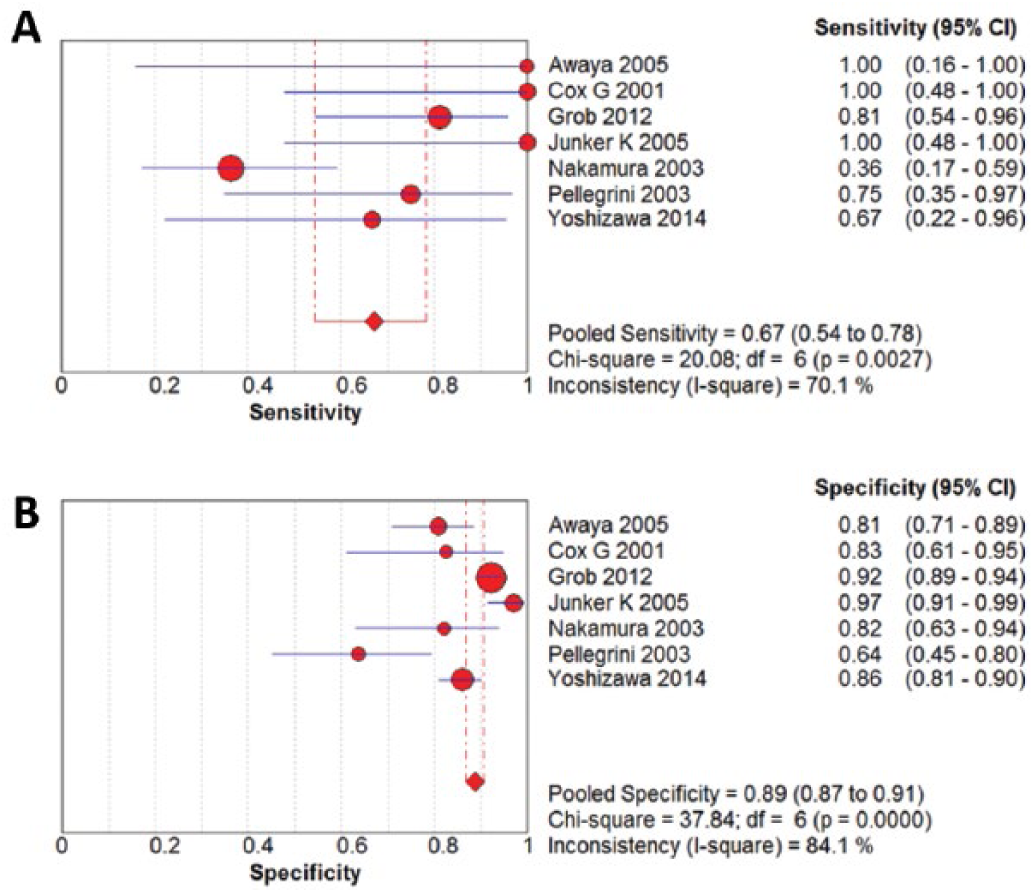
Forest plot diagram of the pooled sensitivity (
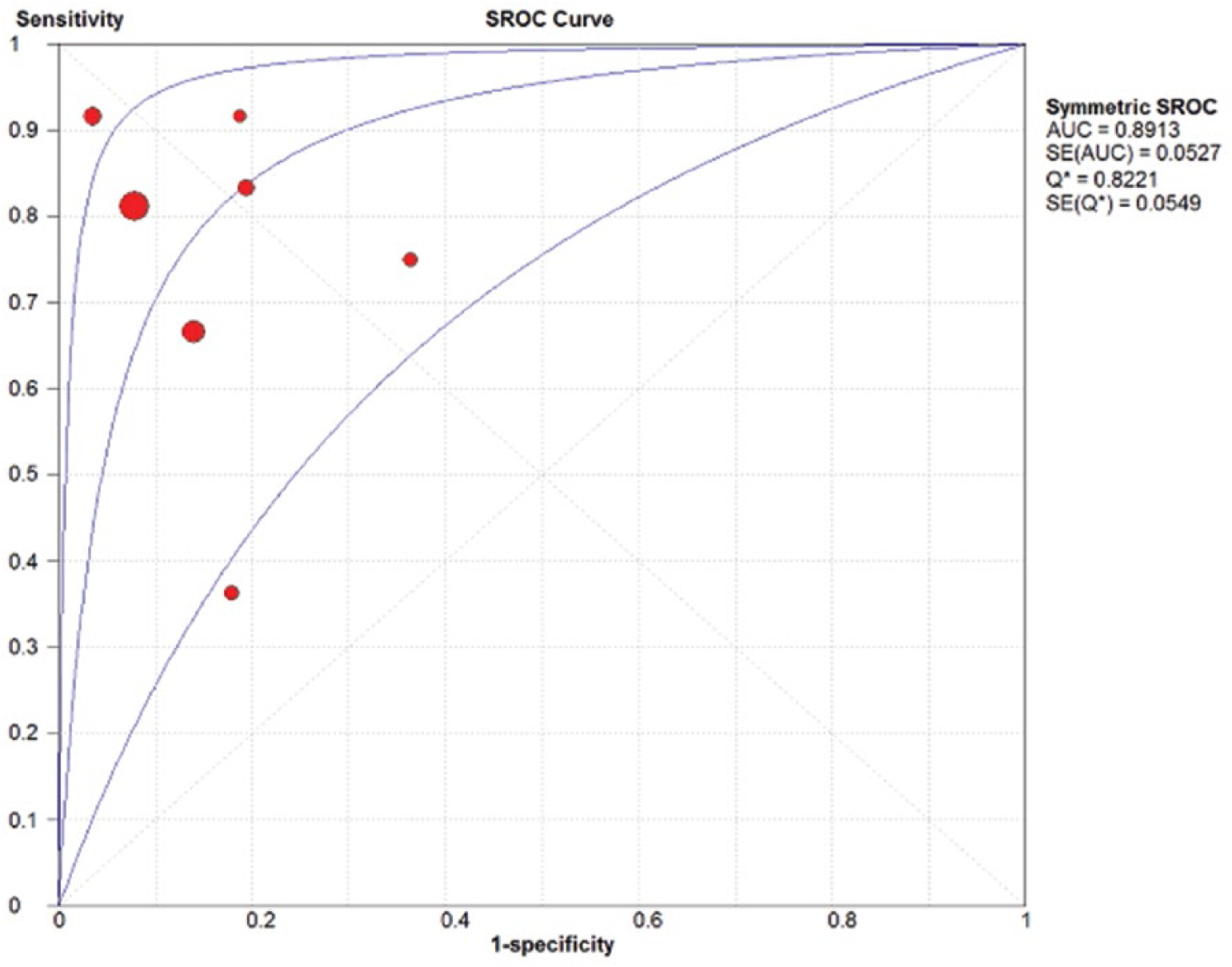
Summary receiver operating characteristic (SROC) curve of HER2 immunohistochemistry.
Discussion
The prognostic role of HER2 overexpression/gene amplification in NSCLC is controversial (3, 27, 28). Recently, several anti-HER2 agents, such as neratinib, dacomitinib, lapatinib and afatinib, have been developed for use in NSCLC (29). Accurate evaluation tests and well-defined detailed criteria are needed for the appropriate selection of patients who can benefit from targeted therapies. The correlation between HER2 IHC and ISH has not been fully elucidated for NSCLC cases. Previous studies have used the diagnostic flow of breast and gastric cancers (19-25). To the best of our knowledge, the present study is the first to show the concordance between HER2 IHC and ISH and the first to assess the diagnostic accuracy of HER2 IHC in NSCLC.
HER2 overexpression and amplification have been reported in 13%-20% and 2%-22.8% of NSCLCs, respectively (9-12, 14, 16, 25), and HER2 IHC score 3+ cases comprise only 2%-6% of NSCLC cases (10-12, 16). Unlike in breast and gastric cancers, the therapeutic effect of trastuzumab has not been fully elucidated in NSCLC with HER2 overexpression (17, 30-33). However, among several kinase inhibitors, neratinib and dacomitinib were shown to have an effect on the inhibition of proliferation of HER2-mutant lung cancer cells (34-36). HER2 status must be taken into account when considering treatment options in NSCLC. In a previous meta-analysis, HER2 IHC overexpression, but not HER2 amplification in ISH, was significantly correlated with worse prognosis (3). In another study, although there was no association between HER2 amplification and tumor stage or metastasis, HER2 amplification was significantly correlated with worse prognosis (21). The reason for these contradictory results may be the use of different detection methods in various populations and histological tumor types. Therefore, the diagnostic flow for HER2 status must be confirmed before evaluation of the correlation between HER2 overexpression/amplification and prognosis and the therapeutic effect of HER2-targeted agents.
Proper evaluation of HER2 status and selection of patients is important in determining the therapeutic effect of HER2-targeted agents in NSCLC. In breast and gastric cancers, the initial test is IHC and the results are confirmed with ISH for HER2 status. When the HER2 IHC score is 2+, an additional ISH test is performed to confirm HER2 gene amplification. Therefore, the concordance between HER2 IHC and ISH in cases with HER2 IHC scores 0/1+ or 3+ could be important, because these cases are confirmed without additional ISH tests. However, in NSCLC, the diagnostic flow for HER2 status has not been fully elucidated. Rather, the diagnostic flow of HER2 status of breast and gastric cancers has been applied to NSCLC in previous studies (19-25). In subgroup analysis based on HER2 IHC scores, the concordance rates were 0.975, 0.091 and 0.665 in HER2 IHC scores 0/1+, 2+ and 3+, respectively. Compared with breast, gastric and colorectal cancers, the concordance rate of HER2 IHC score 0/1+ was not different for NSCLC (4, 5, 18). However, the concordance rate of HER2 IHC score 2+ for NSCLC was lower than those for other cancers (4, 5, 18). The discordance of HER2 IHC score 2+ cases could be caused by several factors, including ISH methods, IHC antibodies/methods, specimen types, and molecular tests. Although the HER2 IHC score 2+ group is heterogeneous, the discordance rate of HER2 IHC score 2+ in NSCLC was 90.9%. In addition, as described above, the discordance rate of HER2 IHC 3+ cases between IHC and ISH was 33.5% in NSCLC, which was higher than that of breast, gastric and colorectal cancers (4, 5, 18). Therefore, evaluation algorithms that differ from gastric and breast cancers will be needed for NSCLC.
Based on the result of our diagnostic test accuracy review, HER2 IHC was relatively well concordant with HER2 ISH. However, the AUC of the SROC curve in NSCLC was lower than those for gastric and colorectal cancers (4, 5). The lower concordance rate of HER2 IHC score 2+ may influence the low AUC value in NSCLC. This result was obtained by consideration of HER2 IHC score 2/3+ as IHC positivity. In the current study, to confirm the impact of HER2 IHC score 2+ cases, the diagnostic test accuracy review was additionally performed in a situation where HER2 IHC score 2+ cases were considered as IHC-negative. The pooled sensitivity and specificity were 0.59 (95% CI 0.39-0.78) and 0.99 (95% CI 0.97-0.99), respectively. The AUC of the SROC curve was 0.9869, very close to 1. When HER2 IHC score 0-2+ cases were considered as IHC negative, the concordance rate was 0.985 (95% CI 0.973-0.992) and slightly higher than that of HER2 IHC score 0/1+ cases. According to our results, the classification of equivocal cases (IHC score 2+) may be well matched with IHC negativity in NSCLC. However, further studies will be required to determine whether additional molecular tests for these equivocal cases are needed in NSCLC.
NSCLCs are classified into various histological types including adenocarcinoma, squamous cell carcinoma and large cell carcinoma. HER2 overexpression/amplification was more frequent in lung adenocarcinoma than in other histological types (1). In the present study, we attempted to elucidate the impact of histological type on the concordance between HER2 IHC and ISH. However, the eligible studies did not contain detailed information regarding histological type. Because 2 of the eligible studies included only patients with adenocarcinomas, concordance could only be indirectly compared between histological types (19, 25). In all cases and HER2 IHC score 0/1+ cases, there was no significant difference in concordance rates between the adenocarcinoma and mixed subgroups. However, in HER2 IHC score 2/3+ cases, the concordance rate of the adenocarcinoma subgroup was significantly lower than that of the mixed subgroup (0.109, 95% CI 0.050-0.222 vs. 0.437, 95% CI 0.274-0.615; p = 0.006). We were unable to differentiate between HER2 IHC 2+ and 3+ adenocarcinoma cases owing to insufficient information. Further studies will be needed to determine the discordance between HER2 IHC and ISH in lung adenocarcinomas.
There are some limitations to our study. First, there was no significant difference in concordance rates between FISH and CISH. Silver ISH (SISH) as well as FISH are widely used in pathology laboratories. However, comparison between SISH and other ISH methods could not be performed owing to insufficient information. Second, various HER2 antibody clones, including HercepTest, A0485, 4B5, CB11 and SP3, were used for the evaluation of HER2 IHC status. However, among the 7 eligible studies, 6 used HercepTest and 1 used CB11 (19-25). However, the eligible study using CB11 evaluated concordance using CISH (19). Therefore, direct comparison between antibody clones could not be performed due to different ISH methods. According to our previous study (4), the sensitivity and specificity for the detection of HER2 IHC expression can be altered by antibody clones. Further studies will be needed to obtain this information for antibody clones in NSCLC. Third, as described above, direct comparison between histological types of NSCLC could not be performed due to insufficient information. In addition, we were unable to find the cause of the lower concordance rate of adenocarcinoma. Fourth, if intratumoral heterogeneity is present in NSCLC, the possible difference between biopsied and surgical specimens should be considered. However, our study could not perform this subgroup analysis based on specimen types. Fifth, in this meta-analysis, concordance assessment between HER2 IHC and polymerase chain reaction (PCR) was not performed. However, in previous studies, there was a discordance between HER2 IHC expression and mRNA level in NSCLC (24, 25). Because the gold standard for evaluation of HER2 status has not been established in NSCLC, further evaluation for the correlation between HER2 IHC, ISH and PCR will be required.
In conclusion, our data suggested that HER2 IHC was well concordant with ISH in the HER2 IHC score 0/1+ subgroup. However, unlike breast and gastric cancers, NSCLCs with a HER2 IHC score 2+ show significantly lower concordance with HER2 ISH. Further studies including detailed evaluation criteria and diagnostic flow in NSCLC will be required before application in daily practice can be considered.
Footnotes
Disclosures
Financial support: None.
Conflict of interest: The authors declare that they have no conflict of interest.