
Abstract
Background
Metastasis is the primary cause of death in patients with breast cancer. Although VEGF-A, C and D are considered to be prime factors in lymph node metastasis in breast cancer, the published studies have conflicting conclusions.
Methods
To resolve this conflict, we conducted a meta-analysis of 37 studies (n = 5,001 patients) evaluating the correlation between VEGF-A, C and D immunohistochemical expression and lymph node metastasis (LNM). The meta-analysis included 22 studies of VEGF-A, 17 of VEGF-C, and 6 of VEGF-D. The relationships between VEGF-A, C and D and clinicopathological parameters were also examined.
Results
The results showed a significant association between VEGF-A or VEGF-C overexpression and LNM (risk ratio [RR] = 1.28 [95% CI 1.04-1.58], p = 0.02; and RR = 1.36 [95% CI 1.07-1.72], p = 0.01, respectively). Subgroup evaluation showed a significant association between VEGF-A, C and D overexpression and LNM when analyses were limited to Asian patients (RR = 1.78 [95% CI 1.28-2.46], p = 0.0005; RR = 1.38 [95% CI 1.04-1.84], p = 0.03, and RR = 2.62 [95% CI 1.35-5.09], p = 0.004, respectively). VEGF-A overexpression was significantly associated with lymph vessel invasion (RR = 1.86 [95% CI 1.33-2.60], p = 0.0003). Overexpression of VEGF-C or VEGF-D was significantly associated with HER-2 positivity (RR = 1.30 [95% CI 1.06-1.59], p = 0.01; and RR = 1.75 [95% CI 1.01-3.03], p = 0.05, respectively).
Conclusions
With some limitations, our meta-analysis indicated that VEGF-A and C could predict LNM in patients with breast cancer, particularly Asian patients.
Introduction
Breast cancer is the most common malignancy and the second most common cause of cancer-related mortality among women (1). Some 232,340 new breast cancer cases, accounting for 29% of all new cancer cases, have been predicted for women in the United States in 2013 (2). Metastasis is the primary cause of death in patients with breast cancer. The lymph nodes are the first sites of metastasis for most types of cancer including breast cancer; axillary lymph node status is still the strongest prognostic marker in breast cancer patients (3-4-5). Gene expression microarrays and functional studies in vitro and in vivo, together with detailed clinical observations, have identified many factors that affect metastasis to lymph nodes. However, little knowledge of crucial factors is available to predict metastasis of lymph nodes in breast cancer. Previous studies have shown that members of the vascular endothelial growth factor (VEGF) family are leading candidates among cytokines that cause lymph node metastasis (LNM) in tumors. VEGF-C and VEGF-D are well recognized as mediators of LNM, and VEGF-A is associated with angiogenesis in breast cancer (6, 7). Recently, Hong and Björndahl demonstrated that VEGF-A can also promote lymphangiogenesis and lymphatic metastasis (8, 9).
Several studies have evaluated whether VEGF-A, C or D proteins (measured by immunohistochemistry) may be activation factors for LNM in patients with breast cancer. However, the conclusions of these studies were inconsistent. To resolve the controversy, we conducted a meta-analysis to examine if VEGF-A, C or D protein expression can regulate LNM in patients with breast cancer.
Methods
Publication Search
To identify all articles that examined the association between lymph node involvement and immunohistochemical expression of VEGF-A, VEGF-C or VEGF-D protein in patients with breast cancer, we conducted a literature search in the PubMed database in November 2014. The search strategy was based on combinations of “VEGF,” “VEGF-A,” “VEGF-C,” “VEGF-D,” “immunohistochemistry,” “IHC,” “lymph node,” “lymphatic metastasis,” and “breast cancer.” The reference lists of the retrieved articles were also screened to identify additional published studies that were not indexed by PubMed.
The search results were then screened according to the following inclusion criteria: 1) proven diagnosis of breast cancer in human subjects; 2) VEGF-A, C or D measurement using immunohistochemistry; 3) sufficient data to derive numbers of patients with LNM in both groups of high and low VEGF-A, C or D expression; and 4) exclusion of letters, reviews, editorials and articles published in languages other than English.
Data Extraction
Two researchers (F. Su and B. Liu) independently extracted the following information for each eligible study: first author, year of publication, country of the study population, number of patients analyzed, number of patients with LNM, several clinicopathological parameters, definitions of VEGF-A, C and D positivity, and blinding of VEGF-A, C and D measurements to the study outcomes.
Statistical Analysis
The risk ratio (RR) with the corresponding 95% confidence interval (CI) was used to estimate the association between VEGF-A, C or D overexpression and LNM in human breast cancer for each study. A chi-square-based Q-statistics test and I2 test were performed to assess the heterogeneity between studies. p>0.10 for the Q-test indicates a lack of heterogeneity among studies. I2<25% suggests a lack of heterogeneity; I2 = 25-50% suggests moderate heterogeneity; I2>50% suggests large or extreme heterogeneity. If I2 was ≤50%, the fixed-effects model was used; otherwise, the random-effects model was used. Publication bias was diagnosed by inverted funnel plots. An asymmetric plot suggested possible publication bias, which was further examined by Egger's test and Begg's test. In the same way, we estimated the correlation between VEGF-A, C or D overexpression and expression of estrogen receptor (ER), progesterone receptor (PR), HER-2, and other clinicopathological parameters. Meta-analysis was carried out using the Review Manager 5.0 software. p<0.05 was considered statistically significant.
Results
Description of Studies
The systematic literature search yielded a total of 37 studies, which comprised 5,001 patients for a final analysis, including 22 studies involving VEGF-A expression (10-11-12-13-14-15-16-17-18-19-20-21-22-23-24-25-26-27-28-29-30-31), 17 involving VEGF-C expression (20, 32-33-34-35-36-37-38-39-40-41-42-43-44-45-46-47), and 6 involving VEGF-D expression (20, 33, 40, 42, 48, 49). Two studies were excluded because identical patient cohorts were used in other selected studies (50, 51).
The characteristics of the 37 eligible studies are listed in Tables I-II-III. These studies were conducted in different populations of various ethnicities: for VEGF-A expression, 10 studies were from Europe, 11 from Asia, 1 from South America; for VEGF-C expression, 5 were of Europeans, 10 of Asians, 2 of Americans; for VEGF-D expression, 4 were of Europeans and 2 were of Asians.
Baseline characteristics of included studies evaluating correlation between VEGF-A expression and lymph node involvement
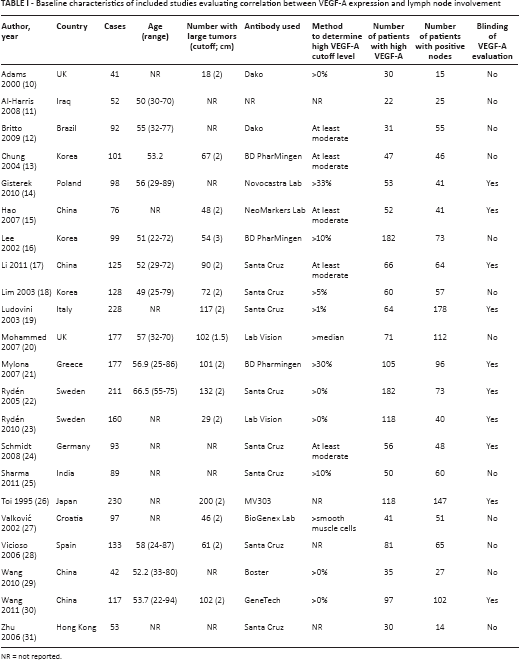
NR = not reported.
Baseline characteristics of included studies evaluating correlation between VEGF-C expression and lymph node involvement
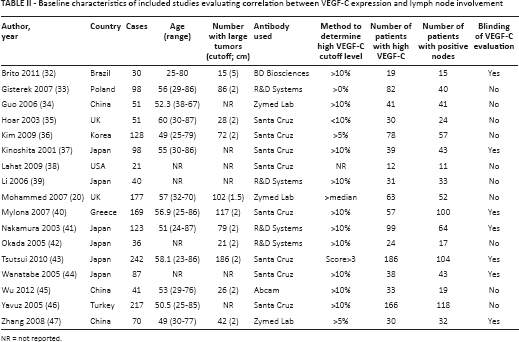
NR = not reported.
Baseline characteristics of included studies evaluating correlation between VEGF-D expression and lymph node involvement
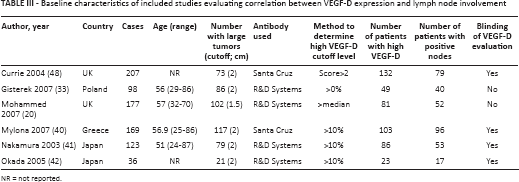
NR = not reported.
For all patients, measurements were taken of the primary tumors and all samples were excised before chemotherapy or radiotherapy. This meta-analysis included 8 male patients enrolled in the study of Yavuz et al (46), which reported the correlation between VEGF-C expression and lymph node involvement.
Impact of VEGF-A, C and D Expression on lymph node Involvement in Patients with Breast Cancer
The effect of VEGF-A on lymph node involvement was evaluated in 22 studies. VEGF-A overexpression was significantly associated with the presence of LNM (RR = 1.28 [95% CI 1.04-1.58], n = 22, p = 0.02, Fig. 1). In studies conducted on Asian patients, the effect was clearer (RR = 1.78 [95% CI 1.28-2.46], n = 11, p = 0.0005). There was no difference in the summary effect for studies of European patients (RR = 0.98 [95% CI 0.75-1.29], n = 10, p = 0.89). In studies clearly declaring that the evaluation of immunohistochemical results was blinded to patient outcomes, the effect was not significant (RR = 0.99 [95% CI 0.79-1.24], n = 10, p = 0.94), whereas larger studies tended to show more conservative and nonsignificant effects (RR = 1.24 [95% CI 0.91-1.69], n = 10, p = 0.16, Tab. IV).
Summary of RR of association between VEGF-A, C and D expression and lymph node involvement
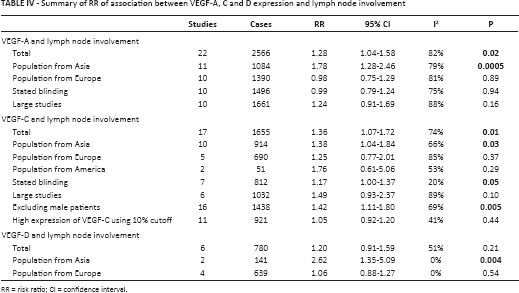
RR = risk ratio; CI = confidence interval.
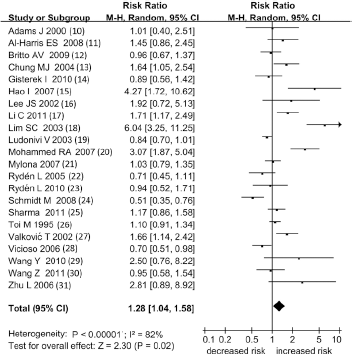
Meta-analysis of the association between VEGF-A overexpression and LNM. Each study is indicated by the name of the lead author, the year of publication and the RR with 95% CI. The summary RR was calculated by the random-effects model.
The effect of VEGF-C on lymph node involvement was evaluated in 17 studies. VEGF-C overexpression was significantly associated with LNM (RR = 1.36 [95% CI 1.07-1.72], n = 17, p = 0.01, Fig. 2). In studies of Asian patients, the effect was similar (RR = 1.38 [95% CI 1.04-1.84], n = 10, p = 0.03), but in European patients the effect was not statistically significant (RR = 1.25 [95% CI 0.77-2.01], n = 5, p = 0.37). In studies clearly stating that the evaluation of immunohistochemical results was blinded to patient outcomes, the effect showed a trend towards statistical significance (RR = 1.17 [95% CI 1.00-1.37], n = 7, p = 0.05). The effect from larger studies was not significant (RR = 1.49 [95% CI 0.93-2.37], n = 6, p = 0.10, Tab. IV).
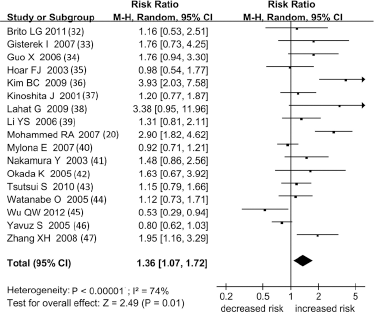
Meta-analysis of the association between VEGF-C overexpression and LNM. Each study is indicated by the name of the lead author, the year of publication and the RR with 95% CI. The summary RR was calculated by the random-effects model.
The effect of VEGF-D on lymph node involvement was evaluated in 6 studies. Increased VEGF-D expression was not correlated with LNM overall (RR = 1.20 [95% CI 0.91-1.59], n = 6, p = 0.21, Fig. 3), but a statistically significant correlation was found when the analysis was limited to Asian patients (RR = 2.62 [95% CI 1.35-5.09], n = 2, p = 0.004, Tab. IV).
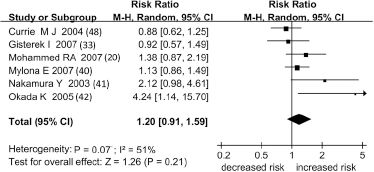
Meta-analysis of the association between VEGF-D overexpression and LNM. Each study is indicated by the name of the lead author, the year of publication and the RR with 95% CI. The summary RR was calculated by the random-effects model.
Correlation of VEGF-A, C and D Expression with Clinicopathological Parameters
VEGF-A overexpression was only significantly associated with the presence of lymphatic vessel invasion (RR = 1.86 [95% CI 1.33-2.60], n = 3, p = 0.0003). VEGF-A overexpression was not associated with other clinicopathological parameters, including high histological grade (RR = 1.25 [95% CI 0.93-1.68], n = 15, p = 0.14), age (>50 years) (RR = 0.97 [95% CI 0.82-1.15], n = 7, p = 0.72), tumor size (>2 cm) (RR = 1.03 [95% CI 0.92-1.15], n = 14, p = 0.61), ER negativity (RR = 1.16 [95% CI 0.84-1.59], n = 12, p = 0.38), PR negativity (RR = 1.08 [95% CI 0.87-1.33], n = 11, p = 0.48), and HER-2 positivity (RR = 1.08 [95% CI 0.94-1.24], n = 8, p = 0.27).
We observed a statistical correlation between VEGF-C overexpression and HER-2 positivity (RR = 1.30 [95% CI 1.06-1.59], n = 8, p = 0.01). However, we observed no correlation between VEGF-C overexpression and other clinicopathological parameters such as age (>50 years) (RR = 1.06 [95% CI 0.96-1.23], n = 6, p = 0.43), high histological grade (RR = 1.34 [95% CI 0.93-1.94], n = 12, p = 0.11), tumor size (>2 cm) (RR = 1.00 [95% CI 0.91-1.10], n = 8, p = 0.98), ER negativity (RR = 0.95 [95% CI 0.83-1.09], n = 12, p = 0.47), PR negativity (RR = 1.00 [95% CI 0.84-1.18], n = 9, p = 0.96) and lymphatic vessel invasion (RR = 1.26 [95% CI 0.83-1.91], n = 7, p = 0.28).
We observed a trend towards a correlation of VEGF-D overexpression with HER-2 positivity (RR = 1.75 [95% CI 1.01-3.03], n = 3, p = 0.05). However, VEGF-D overexpression showed no association with other clinicopathological parameters such as age (>50 years) (RR = 0.99 [95% CI 0.88-1.12], n = 4, p = 0.90), high histological grade (RR = 1.04 [95% CI 0.82-1.33], n = 6, p = 0.73), tumor size (>2 cm) (RR = 1.14 [95% CI 0.77-1.71], n = 5, p = 0.51), ER negativity (RR = 1.13 [95% CI 0.83-1.55], n = 6, p = 0.44), PR negativity (RR = 1.02 [95% CI 0.69-1.50], n = 4, p = 0.92) and lymphatic vessel invasion (RR = 1.26 [95% CI 0.72-2.20], n = 2, p = 0.42).
Publication Bias
Funnel plots and Egger's test were performed to assess publication bias. There was no evidence of publication bias in this meta-analysis.
Discussion
Identifying factors that modulate LNM in patients with breast cancer can provide beneficial guidance for clinical therapy and outcome prediction. Although animal tumor models indicate that VEGF-A, C and D promote tumor lymphangiogenesis and metastasis to regional lymph nodes 52-53-54-55-56-57-58-59), and correlations between overexpression of these factors and LNM have been observed in some human cancers including colorectal cancer (60), esophageal cancer (61), lung carcinomas (62) and endometrial cancer (63), their effects in human breast cancer have not been fully elucidated. Our present meta-analysis showed that overexpression of VEGF-A and VEGF-C was significantly associated with LNM in patients with breast cancer, whereas overexpression of VEGF-D was not. Although most subgroup assessments were not quite significant, interestingly, studies conducted on Asian patients but not European patients indicated significant correlations in all 3 VEGF-A, C and D groups. Although no publications reported racial differences in the associations between VEGF-A, C and D expression and lymph node involvement between Asian and European patients, several studies have indicated differences in the characteristics and subtypes of breast cancer among the different ethnicities. Preat et al (64) found more luminal B subtype and fewer luminal A subtype tumors in Arab patients compared to European patients with breast cancer. Horne et al (65) demonstrated that breast cancer morbidity was 5-fold greater in non-Hispanic American women than in Malaysian women. Most breast cancers were ER and PR positive in non-Hispanic American women and ER and PR negative in Malaysian women. A recent study examined the expression of VEGF-C and VEGFR-3 in breast cancer and indicated that the level of these 2 factors was variable in different subtypes (66). Thus, it is proposed that racial differences in the relationship between VEGF-A, C and D expression and lymph node involvement are probably attributable to varying molecular types between Asian and European women with breast cancer. There was no data on molecular types in the studies included in the present meta-analysis. It is necessary to evaluate the expression of lymphangiogenesis factors in breast cancer according to molecular types. Many cytokines including angiopoietins, fibroblast growth factor-2, platelet-derived growth factor, insulin growth factor-1 and -2, and hepatocyte growth factor have been shown to induce lymphangiogenesis and LNM (67-68-69-70-71). It is unclear whether these factors contribute more strongly to induction of LNM in European women with breast cancer.
Reports of correlations between hormone receptor status and VEGF-A, C and D proteins in breast cancer and other cancers have yielded conflicting results (72-73-74). Our present meta-analysis showed no association between VEGF-A, C or D expression and ER/PR status, but this observation requires further confirmation. Our meta-analysis showed an association between VEGF-C and VEGF-D overexpression and HER-2 positivity. This association has been reported not only in human breast cancer (75) but in non-small-cell lung cancer (76), epithelial ovarian carcinoma (77) and head and neck squamous cell carcinomas (78) as well. These studies imply that HER-2 induced lymphangiogenesis and lymphatic metastasis in tumors via increased synthesis of hypoxia-inducible factor-1 (HIF-1), and then upregulated VEGF-C, which suggests a direction in uncovering the lymphatic metastasis mechanism in cancer.
Our meta-analysis had some limitations. Although we tried to collect all relevant data from the included studies, some data could be missing. Many studies that had negative results but lacked detailed data were excluded from the meta-analysis, and in some studies many patients were excluded due to insufficient clinical data; this missing information may reflect “negative” or more conservative associations. The results have shown that increased VEGF-D expression was not correlated with LNM, but they should be interpreted cautiously. Only 6 studies that involved VEGF-D expression and comprised 810 patients were included in the meta-analysis. The insufficient number of examined cases could be an important reason why no significant correlation was obtained. The between-study heterogeneity was significant (Tab. IV). The included studies had several potential sources of heterogeneity. Patients included in the present meta-analysis may have had different baseline characteristics such as age, histological type, clinical stage, and tumor size. In addition, the use of different immunohistochemical markers to assess the expression of VEGF-A, C or D or ER/PR/HER-2 and variability in definitions of immunohistochemical positivity and experimental procedures may have contributed to the between-study heterogeneity.
In summary, even with the mentioned limitations, the present meta-analysis indicated that VEGF-A and VEGF-C could be clinical markers for lymph node metastasis in patients with breast cancer, particularly Asian patients. However, standardized definitions of immunohistochemical positivity would improve their applicability. Moreover, VEGF-A, C and D are not the only lymphangiogenesis factors (71), and they should be assessed in the context of other potential lymphangiogenesis factors. In addition, the present results must be verified by prospective studies.
Footnotes
Financial support: This study was supported by the National Natural Science Foundation, grant number 81372838.
Conflict of interest: The authors have declared that no conflict of interest exists.