
Abstract
Mastoscopic axillary lymph node dissection (MALND) is a currently used and safe surgical treatment option for breast cancer. However, the extensive application of MALND is still debatable because of the use of conventional axillary lymph node dissection (CALND). Therefore, in the current study, we aimed to compare the efficacy and safety of MALND and CALND for obtaining evidence-based conclusions about the short-term and long-term outcomes of MALND for patients with breast cancer. PubMed, Web of Science, Cochrane Library, and CNKI were comprehensively searched for articles published between January 1998 and January 2019. Then Newcastle-Ottawa scale was used for quality assessment. The Review Manager software version 5.0 was utilized for generating forest maps and funnel plots. Twelve studies including 2157 patients were selected for the meta-analysis. There were no significant differences in the number of lymph node dissections, tumor recurrence rate, axillary drainage, postoperative hospitalization time, and tumor size between the MALND and CALND groups (P > .05). In the MALND group, the surgery time was longer, while the incidence of intraoperative bleeding was lesser and the duration of drainage was shorter than those in the CALND group (P < .01). The complications in the MALND group were also fewer than those in the CALND group (P < .05). The results of the current study showed that MALND is reliable and feasible for breast cancer owing to the lesser incidence of intraoperative bleeding, shorter drainage duration, and lower incidence of complications compared to CALND.
Introduction
Breast cancer (BC) is the most frequently diagnosed cancer in women and the major cause of cancer death among women in most countries. 1 When axillary lymph node metastasis occurs, axillary lymph node dissection is an essential procedure during the surgical treatment of BC, as well as a key step for evaluating the clinical stages and prognosis of patients with BC. 2 Conventional axillary lymph node dissection (CALND) results in obvious damage to the body, such as the presence of a large incision scar in the axilla that affects the appearance, and the incidence of complications is quite high. 3 Currently, the treatment for BC has transformed from performing the “maximum tolerable treatment” to performing the “minimal effective treatment” while improving the survival rate; in addition, we emphasize more on enhancing the quality of life (QOL) of patients, 4 -6 but the trauma and complications of CALND seriously affect the QOL of patients. 7,8 The mastoscopic technique was first introduced in the 1990s and it covers almost all aspects of breast surgery, such as breast-conserving surgery, mastectomy, breast reconstruction, and sentinel lymph node and axillary lymph node dissection. Moreover, mastoscopic axillary lymph node dissection (MALND) is among the most widely used breast minimally invasive surgeries. 4,9,10 Although many studies have evaluated the safety and effectiveness of MALND, in the era of evidence medicine, only limited meta-analyses have compared MALND and CALND. 11,12 Therefore, we performed the current meta-analysis of 12 studies including 2157 patients to compare the efficacy and safety of MALND and CALND. The results of the current research would provide evidence-based conclusions regarding the short-term and long-term outcomes of MALND for patients with BC, thus providing useful information to guide clinicians in their decision-making.
Materials and Methods
Search Strategy
PubMed, Web of Science, Cochrane Library, and CNKI were comprehensively searched for articles published between January 1998 and January 2019. We used the following terms: [Breast Neoplasms (MeSH) OR mammary carcinoma] AND [Mastoscopic axillary lymph node dissection OR Endoscopic axillary lymphadenectomy OR minimal invasive surgery] AND [conventional axillary lymph node dissection OR open axillary lymphadenectomy OR open resection]. The language of the published articles was limited to Chinese or English according to the reviewers’ language competence. Chinese terms were utilized when we searched the Chinese database (CNKI).
Study Selection
The articles were selected according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 13 Three authors were responsible for reviewing the titles, abstracts, and full text, and any disagreements about study inclusion were resolved by discussions among all the authors. The inclusion criteria for including meta-analysis in this study were as follows: (1) the study should have compared MALND and CALND for patients with BC; (2) the article must be a full-text article; and (3) the study was observational studies or randomized controlled trials (RCTs). Studies that met the following exclusion criteria were excluded: (1) studies that were abstracts, expert opinions, case reports, reviews, letters, editorials, or technical notes; (2) studies that included other endoscopic auxiliary methods instead of full-cavity mirror technology or other irrelevant types of surgical options; and (3) screened articles from which it was very difficult to extract the complete and appropriate information needed for meta-analysis.
Data Extraction and Quality Assessment
We extracted the baseline information from the articles, including the first author, publication date, study period, geographical region, number and demographic characteristics of patients, and tumor characteristics. Crucial indicators were also extracted, such as the number of lymph node dissections, tumor recurrence rate, axillary drainage, postoperative hospitalization time, tumor size, surgery duration, intraoperative bleeding, complications, and drainage duration. The data were extracted by 3 independent reviewers. Disagreements were resolved by discussions among all the authors. The methodological quality of the cohort studies and case–control studies were assessed using the Newcastle-Ottawa scale (NOS). 14 The NOS scale utilizes a “star” rating system to evaluate the quality by considering the following 3 aspects of the selected study: the selection of the study groups, the comparability of the study groups, and the assessment of the outcomes; the maximum number of stars a research might receive in each aspect is 3, 2, and 3, respectively.
Statistical Analysis
Long-term complications were classified as surgical complications including wound hematoma, lymph node injury, edema, limb movement disturbance on the affected side, paresthesia, and incision infection. This classification system was based on the Memorial Sloan-Kettering Cancer Center system for reporting complications. 15
Statistical differences between the 2 groups were evaluated via the Fisher exact test for categorical data and by using the Student t test for continuous data. For dichotomous outcomes, we expressed results using odds ratios (ORs) with 95% CIs. For continuous outcomes, we expressed findings using the weighted mean differences (MDs) with 95% CIs. We evaluated the statistical heterogeneity using the χ2 test and assessed the extent of inconsistency using the I2 statistic. If heterogeneity was observed, data were finally analyzed using a random effects model; if no heterogeneity was observed, a fixed effects model was used. P values <.05 were considered to indicate statistical significance. The funnel plot method was utilized to evaluate the possible presence of publication bias. 16 Review Manager (RevMan) software version 5.0 (The Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, 2008) was used for data entry, forest plots, and statistical analysis.
Results
Selection of Studies
The initial search included 194 potentially related articles, of which 53 articles were eliminated, as they were duplicates. Among the remaining 141 articles, 85 articles were eliminated after reading the title and abstract. Then, the remaining 56 studies were obtained and reviewed, of which 44 articles were excluded because of major data were not available (n = 36) or because the full English article was not available (n = 8). Finally, 12 observational studies were eventually included, 12,17 -27 and the complete text for all the articles was accessible. Eight articles were published in English and 4 in Chinese. A flow diagram of the search strategies along with the reasons for elimination is shown in Figure 1.

Flowchart showing the search strategy and selection of studies in the meta-analysis.
Characteristics and Quality of the Included Studies
A total of 2157 participants were included in the 12 studies: 1097 (50.9%) in the MALND group and 1060 (49.1%) in the CALND group; the 12 studies were mainly from 6 different countries (5 studies were from China, 3 from Italy, and 1 each from Japan, France, Germany, and Egypt). On using the NOS, 3 of the 12 studies received 6 stars, 8 articles received 7 stars, and 1 article received 8 stars. All the studies included in the current meta-analysis were prospective cohort studies. The characteristics and the quality of studies are summarized in Table 1.
Summary of Studies Included in Meta-Analysis.
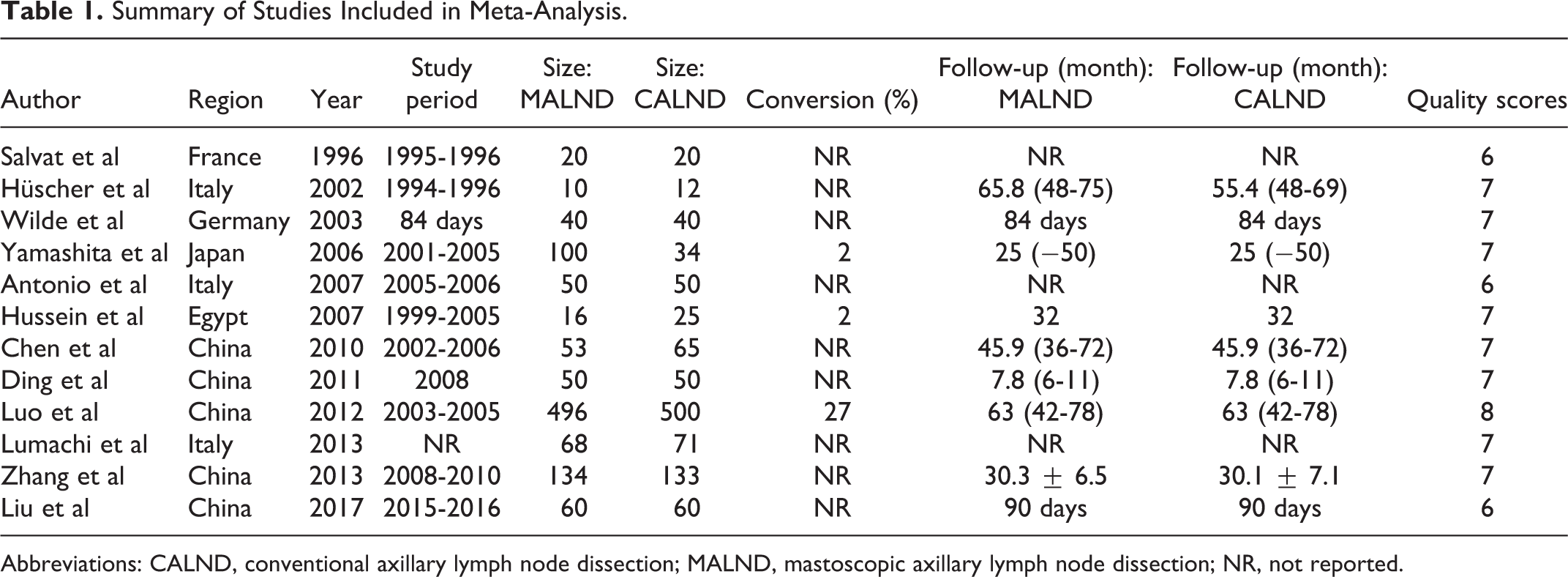
Abbreviations: CALND, conventional axillary lymph node dissection; MALND, mastoscopic axillary lymph node dissection; NR, not reported.
Meta-Analysis of the Surgical Outcomes
In 3 studies, the tumor size was compared between the MALND and CALND groups, and there was no significant heterogeneity between the groups (P = .28, I2 = 21%). 23,25,26 The results showed no significant difference between the 2 groups considering tumor size (MD = −0.15, 95% CI: −0.97 to 0.67, P = .72; Figure 2). Surgery time was significantly different (P < .001, I2 = 99%) among 9 studies 12,17,20 -26 ; the surgery duration was significantly longer in the MALND group than in the CALND group (MD = 18.56, 95% CI: 6.92-30.20, P < .01; Figure 2). Six studies compared the amount of blood loss during the 2 surgical procedures 20,22 -26 ; the results showed that there was significantly less blood loss in the MALND group than in the CALND group (MD = −97.93, 95% CI: −169.71 to −26.14, P < .01; Figure 2). Nine studies provided data about the number of lymph node dissections during MALND and CALND, 12,17,21 -27 with significant heterogeneity among the studies (P < .001, I2 = 80%) using a random effect model. The results showed no significant difference in the number of lymph node dissections between the 2 groups (MD = 0.21, 95% CI: −0.62 to 1.05, P = .62; Figure 2).

Meta-analysis of tumor size and operative outcomes (surgery duration, intraoperative bleeding, and number of lymph nodes harvested). CALND indicates conventional axillary lymph node dissection; MALND, mastoscopic axillary lymph node dissection.
Meta-Analysis of Postoperative Outcomes
Seven studies compared the drainage time between MALND and CALND, 12,20,21,24 -27 with significant heterogeneity among the studies (P < .001, I2 = 95%). The results showed that the axillary drainage time was significantly less in the MALND group than in the CALND group (MD = −1.13, 95% CI: −1.90 to −0.35, P < .01; Figure 3). Six studies compared the armpit drainage flow rate between MALND and CALND, 20,21,24 -27 with significant heterogeneity among the studies (P < .001, I2 = 98%); the armpit drainage flow rate was not significantly different between the groups (MD = −21.50, 95% CI: −53.06 to 10.07, P = .18; Figure 3). Four studies compared the postoperative hospitalization time between MALND and CALND, 17,22,23,26 with significant heterogeneity among the studies (P < .001, I2 = 92%). The results showed no significant difference in the postoperative hospitalization time between MALND and CALND (MD = −1.25, 95% CI: −2.55 to 0.04, P = .06; Figure 3).

Meta-analysis of postoperative outcomes (drainage duration, drainage flow, and length of hospital stay). CALND indicates conventional axillary lymph node dissection; MALND, mastoscopic axillary lymph node dissection.
Meta-Analysis of Overall Complications
The incidence of postoperative complications was reported in 12 studies, 12,17 -27 with significant heterogeneity among the studies (P < .001, I2 = 82%) using a random effect model. The incidence of postoperative complications was significantly less in the MALND group than in the CALND group (OR = 0.41, 95% CI: 0.19-0.85, P < .05; Figure 4).

Meta-analysis of overall complications and recurrence. CALND indicates conventional axillary lymph node dissection; MALND, mastoscopic axillary lymph node dissection.
Meta-Analysis of Recurrence
Eight studies reported tumor recurrence rates, 12,17,18,20,22 -25 with no significant heterogeneity between the 2 groups (P = .74, I2 = 0%). The postoperative tumor recurrence rate was not significantly different between the 2 groups (OR = 1.10, 95% CI: 0.68-1.78, P = .70; Figure 4).
Publication Bias
To evaluate the publication bias, we utilized a funnel plot analysis to compare the overall complications between MALND and CALND (Figure 5). We obtained a scatter plot of the treatment effects that were estimated from individual studies; we plotted the OR against the standard error of the estimate [SE (logOR)]. The graphical funnel plot showed that none of the studies were outside the 95% CI boundaries, indicating no evidence of publication bias (P = .862).

Funnel diagram showing the overall complications. CALND indicates conventional axillary lymph node dissection; MALND, mastoscopic axillary lymph node dissection.
Discussion
The results of the current study showed that the surgery duration was longer in the MALND group than in the CALND group. This was probably because during MALND, the additional process of liposuction is required to dissolve fat; moreover, MALND was prolonged owing to the limitations of cavity mirror surgery as well as considering the proficiency of the performer.
The results of the current study showed that there was less amount of blood loss and a lower incidence of postoperative complications in the MALND group than in the CALND group. Moreover, the axillary drainage time was shorter than that required during CALND. These indicate that MALND results in less trauma, faster postoperative recovery, and fewer complications, 28 probably owing to the following reasons: (1) with the help of endoscopic techniques, MALND can better expose the complex anatomy of the axilla and reduce the damage to the blood vessels, lymphatic vessels, and nerves. (2) Lipid agents are injected before MALND, and the epinephrine in the lipid agents has the effect of constricting blood vessels, thus enhancing physical function and immunity. (3) MALND will not result in changes in the pathological characteristics of lymph nodes if the surgery is performed correctly and if the suction pressure is not too high. (4) Laparoscopic surgery using an ultrasonic knife cutting is time saving and can reduce intraoperative trauma.
Considering the number of lymph nodes dissected, the current meta-analysis showed no significant differences between the MALND and CALND groups. This result might indicate that the clearance of lymph nodes is similar between the groups. After liposuction, the visual field of the cavity is artificially established, and the anatomical structure and lymph nodes of the axilla can be clearly observed from different angles, so that the axillary lymph nodes can be removed more accurately.
Oncological outcomes, such as tumor recurrence, are associated with the skill of surgeons; MALND involves the use of liposuction to remove the fat to form the axillary space. Therefore, if the negative pressure device is overpressured, the integrity of the lymph nodes can be destroyed and tumor metastasis may occur. 9 The results of the current study demonstrated no significant difference between the 2 groups considering the postoperative tumor recurrence rate, but the findings need be interpreted carefully. The surgical technique is demanding, and the number of recurrences was not reported in one-third of the included studies. In addition, data on postoperative follow-up were relatively few. Moreover, the tumor size and molecular subtype of BC were not well comparable among the different studies. Accordingly, unlike surgery-related outcomes, oncological outcomes are hard to evaluate. Therefore, RCTs with longer follow-up are urgently needed for further evaluation of the oncological outcomes.
With the advent of sentinel lymph node biopsy (SNB), patients with BC without sentinel lymph node metastasis, ALND has been replaced by SNB as the standard treatment. Besides, ALND following a positive SN biopsy is being progressively abandoned while patients meet the criteria of AMAROS trial. 29 -32 The results of the ACOSOG Z0011 phase 3 randomized clinical trial were then reported in 2017 with a median follow-up of 10 years. 33 Researchers found that 10-year overall survival (OS) for patients with T1 or T2 invasive primary BC treated with SNB alone was significantly noninferior to OS for those treated with ALND. Meanwhile, SNB without ALND offers excellent regional control for patients with T1 or T2 invasive primary BC treated with breast-conserving therapy and adjuvant systemic therapy. 34 These findings do not support routine use of ALND in abovementioned patient population.
The comparative analysis of MALND and CALND showed that MALND was effective and had wide application prospects for the treatment of BC owing to its unique technical advantages and therapeutic effect. As a minimally invasive surgery technique, it might be feasible to replace CALND with MALND for most cases. However, the overall low quality of the 12 studies included in the current meta-analysis influenced the strength of the evidence in this study. Because most of the studies included did not use the double-blind method, the expression methods for each observation index were different, and some of the indicators of individual studies were transformed, thereby affecting the stability of the results to a certain extent. Therefore, although the findings of this study are relevant, the results should be interpreted with caution.
Conclusions
The current evidence-based analysis revealed that MALND was safer and more feasible than CALND for patients with BC, owing to the lower incidence of intraoperative bleeding, shorter drainage duration, and lower incidence of complications. Nevertheless, well-designed RCTs are needed in future to verify the use of MALND for BC.
Supplemental Material
Supplemental Material, CCX-19-0313.R2_-_prisma_2009_checklist - Contrast of Mastoscopic and Conventional Axillary Lymph Node Dissection of Patients With Breast Cancer: Meta-Analysis
Supplemental Material, CCX-19-0313.R2_-_prisma_2009_checklist for Contrast of Mastoscopic and Conventional Axillary Lymph Node Dissection of Patients With Breast Cancer: Meta-Analysis by Hanchu Xiong, Zihan Chen, Ling Xu, Cong Chen, Qingshuang Fu, Rongyue Teng, Jida Chen, Shuduo Xie, Linbo Wang, Xiao-Fang Yu and Jichun Zhou in Cancer Control
Supplemental Material
Supplemental Material, CCX-19-0313_prisma_2009_checklist - Contrast of Mastoscopic and Conventional Axillary Lymph Node Dissection of Patients With Breast Cancer: Meta-Analysis
Supplemental Material, CCX-19-0313_prisma_2009_checklist for Contrast of Mastoscopic and Conventional Axillary Lymph Node Dissection of Patients With Breast Cancer: Meta-Analysis by Hanchu Xiong, Zihan Chen, Ling Xu, Cong Chen, Qingshuang Fu, Rongyue Teng, Jida Chen, Shuduo Xie, Linbo Wang, Xiao-Fang Yu and Jichun Zhou in Cancer Control
Supplemental Material
Supplemental Material, Ethical_Statement - Contrast of Mastoscopic and Conventional Axillary Lymph Node Dissection of Patients With Breast Cancer: Meta-Analysis
Supplemental Material, Ethical_Statement for Contrast of Mastoscopic and Conventional Axillary Lymph Node Dissection of Patients With Breast Cancer: Meta-Analysis by Hanchu Xiong, Zihan Chen, Ling Xu, Cong Chen, Qingshuang Fu, Rongyue Teng, Jida Chen, Shuduo Xie, Linbo Wang, Xiao-Fang Yu and Jichun Zhou in Cancer Control
Footnotes
Authors’ Note
H.X., Z.C., and L.X. contributed equally to this work.
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the National Natural Science Foundation of China (No. 81972453, No. 81972597, No. 81602471 and No. 81672729), Zhejiang Provincial Natural Science Foundation of China under Grants (No. LY19H160055, LY19H160059, LY18H160005, LY18H160030, and LY20H160026). The work was sponsored by Zheng Shu Medical Elite Scholarship Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.