
Abstract
Purpose
The aim of this study was to investigate the antibacterial surface properties of high-viscosity glass ionomers (Fuji IX GP, Ketac Molar), a resin-modified nano-ionomer (Ketac N100), resin-modified glass ionomers (Fuji II LC, Vitremer), a compomer (Compoglass F) and a resin-based composite (Filtek Z250).
Methods
ISO-standardized specimens 6 mm in diameter were prepared for each restorative material. The antibacterial properties of the materials were tested in an agar diffusion assay using Streptococcus mutans (ATCC 25175) for 24 and 48 hours. An inhibition zone greater than 6 mm was defined as diffuse inhibition, whereas zones ≤6 mm were described as contact inhibition.
Results
All tested materials exhibited a contact antibacterial effect against S. mutans. Vitremer showed the most remarkable antibacterial diffuse inhibition.
Conclusions
These materials might cause antibacterial effects against S. mutans when placed on cavity surfaces in both enamel and dentine, thereby preventing secondary caries formation.
Introduction
Acidogenic bacteria play a major role in the development of dental caries (1, 2). Treatment approaches used to treat caries do not always eliminate all of the microorganisms from dental hard tissue (3-4-5). The presence of cariogenic bacteria in the dental tissue left inadvertently after treatment procedures, as well as bacteria colonization and plaque formation, may result in secondary caries at the restoration margins (6). Moreover, bacterial penetration via microleakage may also lead to secondary caries, which is one of the main reasons for failures in dental restorations (7). Therefore, antibacterial action is a desired effect of dental materials used for restorative treatment. Restorative materials with long-lasting antibacterial surface properties may reduce the formation of biofilm and thus caries recurrence (8). However, most dental materials exhibit microleakage to a degree, which may lead to leakage of oral fluids and a percolation effect, followed by bacterial penetration and growth (8, 9).
Fluoride is considered to be an important factor in the anticariogenic effect of restorative materials (10, 11). Fluoride is capable of incorporating itself into dental hard tissues, thereby making them more resistant to acid degradation, and it also has antibacterial effects against cariogenic oral bacteria (12).
Streptococci play a decisive role in the process of initial bacterial adhesion, which is in turn an essential step in the formation of dental biofilm within the oral cavity (13). Streptococcus mutans has also been found in early plaque (14), although it is not among the predominant species. As S. mutans is the primary factor in the etiology of secondary caries (15), it is crucial to evaluate the interaction of dental restorative materials with these bacteria. The antimicrobial effects of glass ionomers have been reported in many in vitro studies (16, 17), whereas fewer studies evaluating the antimicrobial properties of compomers and composites have been published. These have shown less or no antibacterial effects compared with glass ionomers (18, 19).
Antibacterial properties of restorative materials have been evaluated in vitro using various methods. The agar diffusion test has been used as the standard assay in some of these studies (20, 21). This method is based on measuring water-soluble components released from the bulk of the materials and is often used to evaluate antibiotics (8).
The aim of this study was to investigate the antibacterial surface properties of various fluoride-releasing restorative materials, as well as a resin-based composite, against S. mutans.
Materials and Methods
The dental restorative materials tested in this study were as follows: Fuji IX GP (high-viscosity glass ionomer; GC Corp., Tokyo, Japan), Ketac Molar (high-viscosity glass ionomer; 3M ESPE, Seefeld, Germany), Ketac N100 (resin modified nano-ionomer; 3M ESPE, Seefeld, Germany), Fuji II LC (resin modified glass ionomer, GC Corporation, Tokyo, Japan), Vitremer (resin-modified glass ionomer; 3M ESPE, Seefeld, Germany), Compoglass F (compomer; Ivoclar Vivadent, Liechtenstein) and Filtek Z250 (resin-based composite; 3M ESPE, Seefeld, Germany) (Tab. I).
RESTORATIVE MATERIALS USED IN PRESENT STUDY
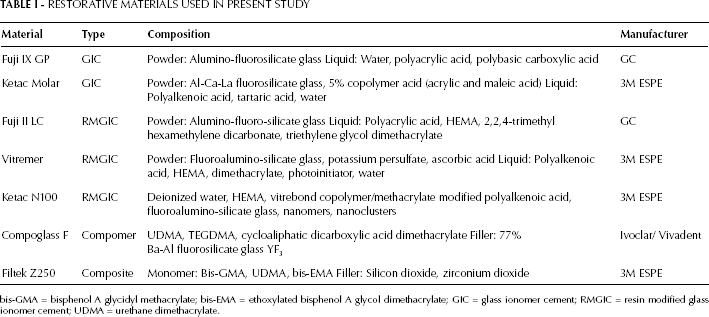
bis-GMA = bisphenol A glycidyl methacrylate; bis-EMA = ethoxylated bisphenol A glycol dimethacrylate; GIC = glass ionomer cement; RMGIC = resin modified glass ionomer cement; UDMA = urethane dimethacrylate.
Specimen preparation
All materials were handled according to the manufacturer's instructions. ISO standardized specimens 6 mm in diameter and 2 mm thick were prepared for each restorative material. The material was placed into a stainless steel mold, slightly filled, covered by Mylar strips and tightly pressed between 2 glass slides to remove the excess material. The conventional glass ionomers were allowed to set at room temperature for 15 minutes, and the resin-modified glass ionomers, resin-modified nano-ionomer, compomer and the resin-based composite were photopolymerized using visible light (Curing light XL 3000™; 3M Dental Products) for 2 times 40 seconds alternately on the top and bottom of the sample. Then, the specimens were removed from the mold and polished with 600 and 1,200 grit sandpaper on both sides under continuous water-cooling. All procedures were performed under aseptic conditions.
Agar diffusion assay
The antibacterial properties of the materials were tested in an agar diffusion assay using S. mutans strain ATCC 25175 for 48 hours. The same operator applied the materials throughout the experiment. The strain was grown on brain-heart infusion (BHI) medium for 18-24 hours at 37ºC in 5% CO2. Bacterial suspensions were prepared to 0.5 MacFarland standard and diluted 100-fold in 0.9% NaCl. Test specimens were immediately placed on the freshly inoculated Mueller Hinton agar plates with 5% sheep blood. Two hundred microliters of 100-fold dilution was then inoculated to agar plates using a Dragalsky glass stick. Test specimens were immediately placed on freshly inoculated agar plates (10 cm in diameter) and were incubated for 48 hours at 37ºC. Each plate contained 4 disks: 1 disk from each experimental group, as well as an additional blank disk which served as negative control. This experiment was repeated 4 times. The diameter of the bacterial inhibition zone around the disks was measured using a caliper. If an inhibition zone was not detected, the disk was removed to determine whether there was growth under it. If an inhibition zone was evident under the disk, this outcome was assumed as a qualitative observation indicating the antibacterial activity on the contact surface (nondiffusible contact inhibition zone). Diffuse inhibition was defined as a zone of inhibition greater than the 6-mm diameter of the disk. The SPSS 13.0 program (SPSS, Chicago, IL, USA) was used for all analyses. Kruskal-Wallis and Mann-Whitney tests were utilized to make comparisons between the inhibition zones of each tested material against S. mutans. The level of significance was set at a p value <0.05.
Results
The mean values and standard deviations of the inhibition zones for each tested material are shown in Table II. All tested materials exhibited a contact antibacterial effect, with the exception of the control group. Regarding diffuse inhibition, only Vitremer showed antibacterial activity against S. mutans, which was statistically significant (p<0.05). No inhibition zone was detected around the blank disks of the control group. The tested bacteria strain yielded consistent growth under the blank disks.
ZONES OF SURFACE GROWTH INHIBITION (DIAMETER IN MILLIMETERS) OF TESTED MATERIALS AGAINST S. MUTANS

Values are means ± SD; n=10, after 48 hours.
Inhibition zones = 6 mm should be interpreted as nondiffusible contact inhibition of the bacterial lawn under the disk.
p<0.05.
Discussion
As secondary caries is primarily a mutans streptococci (MS)-associated disease, it is important to evaluate the interaction of various fluoride-releasing restorative materials with these bacteria, including the effect on adhesion, bacterial viability and biofilm formation (22). In line with this, bacterial viability as a result of interaction with some fluoride-releasing restorative materials was evaluated in the present in vitro study. The agar diffusion test has been widely used as a standard assay in most studies. Limitations associated with the agar diffusion test include its qualitative nature, ability to measure only soluble components, inability to distinguish between bacteriostatic and bacteriocidal effects and difficulty in comparing large groups of samples and in controlling a large number of variables (23). Nevertheless, recent studies have concluded that this approach has some advantages, such as its being a realistic and rapid characterization for determining the antibacterial effects of restorative materials (24, 25). In the present study, the agar diffusion method was preferred, similar to many in vitro studies (20, 22, 26-27-28-29).
Fluoride-releasing restorative materials have been shown to have antibacterial properties to some extent (19, 30), although conflicting results have been reported (31, 32). The results of the present study demonstrated that only Vitremer inhibited the growth of S. mutans for 48 hours after mixing, whereas none of the tested high-viscosity glass ionomers, resin-modified glass ionomers, compomer or the composite showed such an effect. In a recent study, the antibacterial effect of a Fuji II LC and giomer was compared, and it was concluded that giomer had a superior antibacterial effect against S. mutans (33). Due to their limited indications for usage for restorative procedures in a clinical setting, there are fewer studies regarding the antibacterial effects of resin-modified glass ionomers than regarding glass ionomers (7, 15, 17). The Vitremer group showed the strongest antibacterial effect. This result corresponds to the result of Shirani et al (7), demonstrating considerable antibacterial effects of Vitremer compared with compomer and composites. The relationship between the antibacterial effect of Vitremer and its fluoride release has been mentioned in a large number of studies (15, 18, 19, 34). The authors of some studies have studied the effects of the lower pH of this material (17, 35), and other studies have shown that HEMA (hydrophilic monomer), which exists in resin-modified glass ionomers, has an inhibitory effect on bacterial growth (16, 19).
Marczuk-Kolada et al (27) evaluated the antibacterial effects of Fuji IX and Dyract AP and concluded that only Fuji IX inhibited the growth of S. mutans. Conversely, Botelho (26) did not show any antibacterial effect of Fuji IX against the tested bacteria. Similarly, comparing the surface antibacterial properties of compomers, Matalon et al (22) concluded that none of the compomers tested provided significant long-term antibacterial activity against S. mutans. In the previous studies, slight or no antibacterial effect has been found for compomers, similar to the results of the present study (18, 19).
The antibacterial activity of restorative materials depends on chemical composition, initial setting low pH and the release of fluoride and other metallic ions. The amount of fluoride release has been associated with the composition and cure reaction of the restorative material (15, 36). Fuji IX and Ketac Molar utilize a high powder-to-liquid ratio to improve their mechanical properties. This might cause decreased solubility and fluoride release (11). The exact mechanism of fluoride release from both glass ionomer cement and compomer has not yet been completely explained. Nevertheless, many authors explain the differences in fluoride release among these materials by the mechanism of water sorption (37-38-39). Some authors have suggested that release of metallic ions and low initial setting pH are more significant than fluoride release for any antibacterial properties that may be present (40). This might possibly explain the statistically significant antibacterial effect of Vitremer, which has a low pH during the setting reaction. However, further studies are needed to determine the effects of short- and long-term release of other elements such as aluminum, strontium, calcium, silicon and phosphorus on the viability of cariogenic bacteria (28, 39). Lack of bacterial-growth inhibition by fluoride-releasing materials has also been suggested by some studies (18, 41). This result was attributed to the susceptibility of the tested bacteria species to fluoride ions. DeSchepper et al (42) and Herrera et al (18) suggest that the effects of fluoride activity on bacterial cells not only depends on the amount of ions but also on the material's pH during binding, which might explain the differences in the results with the tested materials.
Further studies are needed to clarify the mechanisms of the antibacterial effects of fluoride-releasing restorative materials and to evaluate the effects of the other released ions on cariogenic microorganisms.
Conclusions
All materials tested in this in vitro study caused contact inhibition of S. mutans growth.
Vitremer showed the most remarkable antibacterial diffuse inhibition.
These materials might cause antibacterials effect against S. mutans when placed on cavity surfaces in both enamel and dentine.