
Abstract
Background
This meta-analysis aimed to elucidate the prognostic role of the Ki-67 labeling index (LI) in gastric cancer (GC).
Methods
The current study included 3,615 GC patients in 20 eligible studies, and evaluated the prognostic role of Ki-67 LI in GC. Subgroup analysis was conducted based on depth of invasion and cutoff value for high Ki-67 LI.
Results
A high Ki-67 LI correlated significantly with worse survival (hazard ratio [HR] = 1.214, 95% confidence interval [CI], 1.004-1.468). However, there was no significant correlation between high Ki-67 LI and worse survival in advanced GC (HR = 1.252, 95% CI, 0.801-1.956). The subgroup with cutoff value ≤25% showed a significant correlation with worse survival, but this was not seen in the subgroup with cutoff >25% (HR = 1.433, 95% CI, 1.094-1.876 vs. HR = 1.005, 95% CI, 0.801-1.262). In addition, in the 10% < Ki-67 LI ≤ 20% range, there was a significant correlation between high Ki-67 LI and worse overall survival (HR = 1.931, 95% CI, 1.013-3.310).
Conclusions
A high Ki-67 LI correlated significantly with a worse prognosis in GC patients. Further cumulative studies for the optimal cutoff value for high Ki-67 LI are needed before application in clinical practice.
Introduction
Gastric carcinoma (GC) is a biologically and genetically heterogeneous tumor and one of the most common malignant tumors worldwide (1). The incidence of GC varies markedly with geography. In Asia, Eastern Europe, Chile and Costa Rica, the incidence is significantly higher than in North America, Northern Europe, Africa and Southeast Asia (1, 2). In regions with successful endoscopic screening programs, the incidence of early GC (EGC) is higher than in other regions.
The American Joint Committee on Cancer tumor-node-metastasis (TNM) classification is an important prognostic factor (3), but GCs of the same TNM stage may show variable prognoses. Many studies have reported several biological and molecular biomarkers, such as HER2 (4), p53 (5), FOXO1A (6), Bcl-2 (7), E-cadherin (8), cyclooxygenase 2 (9, 10) and VEGFR (11) for predicting GC prognosis. However, for the prediction of prognosis in GC, the use of these histopathological and biological markers has not been fully elucidated, and these candidates have not been widely used in daily clinical practice. Therefore, studies of novel prognostic markers or systematic reviews and meta-analyses for previously discovered markers are needed.
The Ki-67 protein, a nuclear nonhistone protein, is differentially expressed according to the cell cycle and could be expressed in the nuclei of cells in the G1, S, G2 and M phases of proliferating cells (12). However, the Ki-67 protein is not expressed in quiescent or resting cells in the G0 phase (13). Therefore, cells expressing the Ki-67 protein are considered to be proliferating cells. Although the Ki-67 labeling index (LI) might be a useful prognostic marker in various malignancies (14), its prognostic role is controversial in GC. In the present meta-analysis, we investigated the correlation between the Ki-67 LI and overall survival in 3,615 patients using data from 20 eligible studies (7, 9, 10, 15-31). Moreover, the correlation between pathological stages and a high Ki-67 LI was elucidated from all available studies.
Materials and methods
Search of published studies and selection criteria
Relevant articles were obtained by searching the PubMed and MEDLINE databases up to January 31, 2017. Searches were performed using the following key words: “gastric carcinoma,” “Ki-67,” “MIB-1” or “survival.” The title and abstract of all searched articles were screened for exclusion. Review articles were also screened to find additional eligible studies. Articles were included if the study was performed in human GC patients and if there was information about the correlation between high Ki-67 LI and survival rate. Articles were excluded if they were case reports or nonoriginal articles, or if the article was not written in English or Korean. Among the eligible studies, Tokuyasu et al (26) demonstrated separate information according to intestinal and diffuse type; therefore, we counted it as 2 studies in the data extraction process (Tab. I) after the study search (Fig. 1).
Main characteristics of the eligible studies
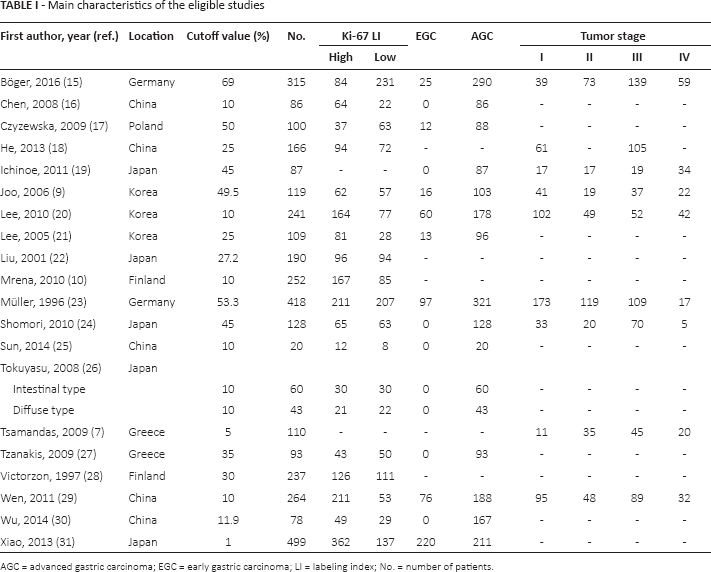
AGC = advanced gastric carcinoma; EGC = early gastric carcinoma; LI = labeling index; No. = number of patients.
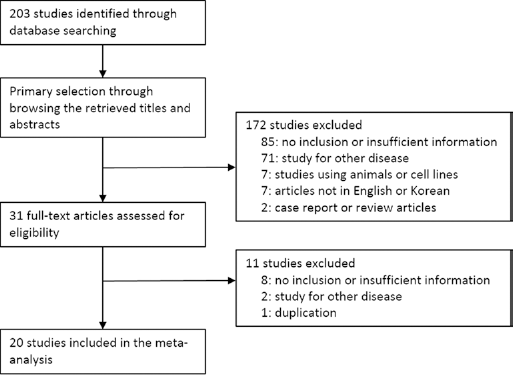
Flow chart for study search and selection.
Data extraction
Data from all eligible studies were extracted by 2 authors. The included data were extracted from each of the eligible studies (7, 9, 10, 15-31): the first author's name, year of publication, study location, antibody manufacturer, dilution ratio of Ki-67 or MIB-1 antibody, cutoff value for high Ki-67 LI, number of patients analyzed, and pathological tumor-node-metastasis (pTNM) stage. For quantitative aggregation of survival results, the correlation between high Ki-67 LI and overall or disease-free survival rate was analyzed according to the hazard ratio (HR) using 1 of 3 methods. In studies not quoting the HR or its confidence interval (CI), these variables were calculated from the presented data using the HR point estimate, log-rank statistic or its p value, and the O-E statistic (difference between the number of observed and expected events) or its variance. If those data were unavailable, HR was estimated using the total number of events, number of patients at risk in each group, and the log-rank statistic or its p value. Finally, if the only useful data were in the form of graphical representations of survival distributions, survival rates were extracted at specified times to reconstruct the HR estimate and its variance under the assumption that patients were censored at a constant rate during the time intervals (32). The published survival curves were read independently by 2 authors to reduce reading variability. Data associated with survival were extracted after a 60-month follow-up period. The HRs were then combined into an overall HR using Peto's method (33).
Statistical analysis
To perform the meta-analysis, all data were analyzed by the Comprehensive Meta-Analysis software package (Biostat, Englewood, NJ, USA). We investigated the correlation between high Ki-67 LI and survival rate in GC. To obtain the optimal cutoff value for high Ki-67 LI, subgroup analysis was conducted. In addition, the rates of high Ki-67 LI according to depth of invasion, lymph node metastasis and TNM stage were investigated. Heterogeneity between studies was checked by the Q and I2 statistics and demonstrated p values. Meta-regression test and sensitivity analysis were conducted to assess the heterogeneity of eligible studies and the impact of each study on the combined effect, respectively. In the current meta-analysis, because eligible studies used various detection methods and populations, the application of a random-effects model rather than a fixed-effects model was more suitable. For assessment of publication bias, Begg's funnel plot and Egger's test were performed. If significant publication bias was found, fail-safe N and trim-fill tests were performed to confirm the degree of publication bias. The results were considered statistically significant when p was <0.05.
Results
Selection and characteristics of studies
The current study discovered 203 reports from the database search. Among these reports, 93 were excluded because of insufficient or no information. In addition, 73 reports were excluded as they focused on other diseases, and 17 because they were studies that used animals or cell lines (n = 7), were non-English or non-Korean (n = 7) or were duplicated (n = 1) or nonoriginal (n = 2) reports. Finally, 20 eligible studies were included in the current meta-analysis (Fig. 1; Tab. I). This study included data about 3,615 GC patients. In addition, the cutoff values for the Ki-67 LI varied between 1% and 69.0% (Tab. I).
Meta-analysis
A high Ki-67 LI was significantly correlated with worse overall survival (HR = 1.214, 95% CI, 1.004-1.468; Fig. 2A). Eligible studies showed significant heterogeneity (I2 = 94.4%, p<0.001). Sensitivity analysis was also performed and included studies which had no effect on the pooled HR. The range of HRs was 1.158-1.274 in the sensitivity analysis. There was no significant publication bias revealed by Egger's test (p = 0.986) or Begg's funnel plot. In the advanced GC (AGC) subgroup, there was no significant correlation between a high Ki-67 LI and worse overall survival (HR = 1.252, 95% CI, 0.801-1.956; Fig. 2B).
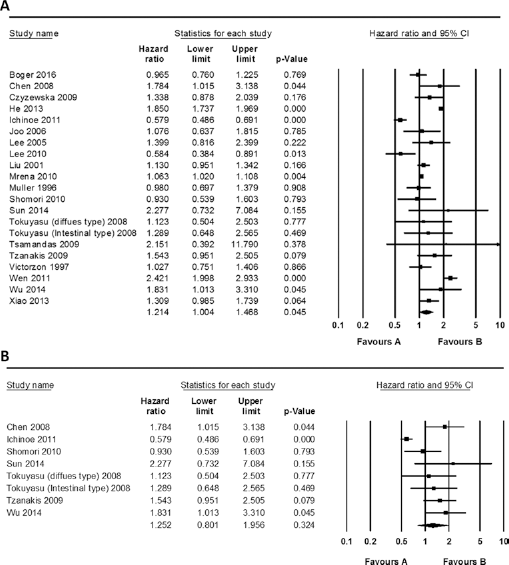
Forest plot diagram for the correlation between high Ki-67 labeling index and overall survival in overall cases (
Next, we performed subgroup analyses to obtain the optimal cutoff value for high Ki-67 LI. Subgroups with cutoff values of 25% and those with lower than 25% showed significantly poorer survival rates (HR = 1.433, 95% CI, 1.094-1.876) than the subgroup with cutoff values of higher than 25%, which showed no significant difference between high and low Ki-67 LI patients (HR = 1.005, 95% CI, 0.801-1.262). In addition, in various cutoff value ranges, the prognostic roles of high Ki-67 were analyzed. In the range 10% < Ki-67 LI ≤ 20%, there was a significant correlation between high Ki-67 LI and worse overall survival (HR = 1.931, 95% CI, 1.013-3.310). However, in other cutoff value ranges, there was no significant correlation (Fig. 3).
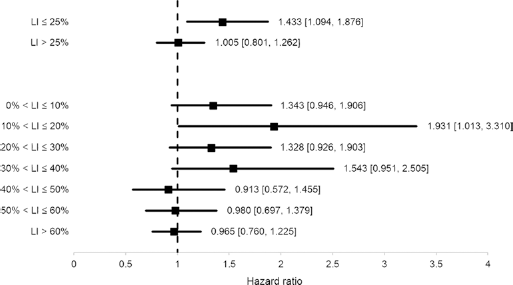
Forest plot diagram for subgroup analysis based on Ki-67 labeling index (LI) cutoff value: hazard ratios with 95% confidence intervals.
The rates of high Ki-67 LI were investigated according to depth of invasion, lymph node metastasis and pTNM stage (Tab. II). The rates of high Ki-67 LI were 0.509 (95% CI, 0.304-0.711) and 0.518 (95% CI, 0.260-0.767) in T1 and T2-4 subgroups, respectively. There was no significant difference of the rate of high Ki-67 LI between GC patients with or without nodal disease (0.586, 95% CI, 0.430-0.726 vs. 0.541, 95% CI, 0.364-0.709) or between those with higher and lower TNM stages (0.602, 95% CI, 0.454-0.733 vs. 0.601, 95% CI, 0.423-0.755).
Meta-analysis of higher Ki-67 labeling index and clinicopathological stages of gastric carcinoma
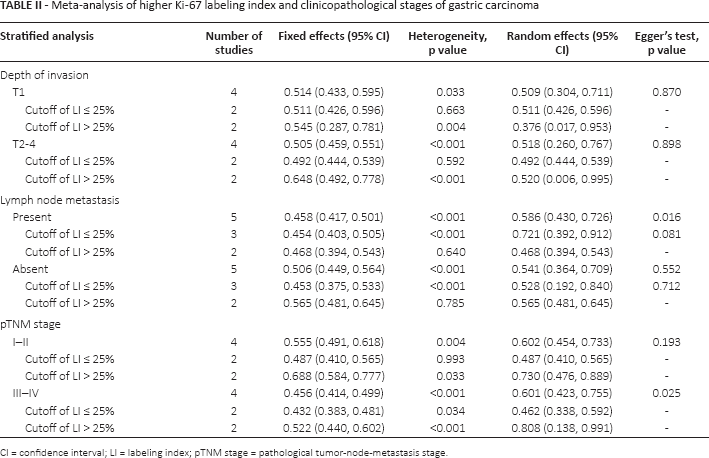
CI = confidence interval; LI = labeling index; pTNM stage = pathological tumor-node-metastasis stage.
Discussion
The Ki-67 LI is a useful prognostic factor in various malignancies, such as neuroendocrine tumors and breast carcinomas (1, 14). In gastrointestinal stromal tumors, the Ki-67 LI has been reported to be an important prognostic factor (34). However, the prognostic role of the Ki-67 LI remains controversial in GC, despite an increase in the number of published reports. To the best of our knowledge, the present study is the first meta-analysis of published studies evaluating the prognostic role of the Ki-67 LI in GC.
The current meta-analysis showed a significant correlation between a high Ki-67 LI and worse overall survival. Eligible studies used mean, median, optimal cutoff value or arbitrary values for the Ki-67 LI. We performed subgroup analysis to determine the optimal Ki-67 LI cutoff value for the prediction of prognosis. A high Ki-67 LI was significantly correlated with a worse prognosis in studies with a cutoff value of 25% and lower (HR = 1.433, 95% CI, 1.094-1.876), but not in studies with a cutoff value higher than 25% (HR = 1.005, 95% CI, 0.801-1.262). A high Ki-67 LI was significantly associated with a poor prognosis in studies with a cutoff value of 10% and lower than 10% (HR = 1.343, 95% CI, 0.946-1.906). In addition, in the range of 10% < Ki-67 LI ≤ 20%, there was a significant correlation between a high Ki-67 LI and worse overall survival (HR = 1.931, 95% CI, 1.013-3.310). These results suggest that the optimal predictive cutoff value may be a certain value within a range for Ki-67 LI > 10% and ≤ 25%. Further cumulative studies for validation of optimal cutoff value and method standardization for evaluating the Ki-67 LI are needed for application in daily clinical practice.
In the current meta-analysis, the pooled HR of overall survival was 1.214, and this was lower than for other malignant tumors (34, 35). In addition, in gastrointestinal stromal tumors, the pooled HR of overall survival was 3.730 (95% CI, 2.819-4.936) (36). As described in the “Results” section, a significant heterogeneity was identified between eligible studies (I2 = 94.4%, p<0.001). In addition, eligible studies have reported varying results for the correlation between a high Ki-67 LI and prognosis. These varying results could be caused by several factors, such as dilution ratios, antibody manufacturers, immunohistochemical staining methods and evaluation protocols for Ki-67 LI. Among the 20 eligible studies, 1 study, by Lee et al, showed that a high Ki-67 LI was negatively correlated with a lower survival rate (20). It posited that early carcinomas with higher proliferative ability may show a high Ki-67 LI, and may be correlated with a better prognosis. However, in the sensitivity analysis, this single report had no noteworthy influence on the pooled HR (from HR = 1.232 to HR = 1.285). In addition, we failed to find a significant difference in method, evaluation system or composition of patients between the report by Lee et al (20) and other eligible reports. Therefore, a detailed analysis is required to obtain the information for the prognostic role of high Ki-67 LI, and meta-analysis could be a suitable method.
High-incidence regions of GC include Eastern Asia (Republic of Korea and Japan), Eastern Europe and Central and Latin America (1). The current meta-analysis included 13 reported from Asia and 7 reports from Europe. However, a worse prognosis with a high Ki-67 LI was observed in both Asia and Europe (HR = 1.260, 95% CI, 0.941-1.687 and HR = 1.064, 95% CI, 1.022-1.107, respectively). Statistical significance was only identified in the European reports, but the pooled HR in the European reports was lower than that in the Asian reports. In addition, study location had no effect on heterogeneity in the meta-regression test.
Although the Ki-67 LI is associated with tumor proliferation, the correlation with tumor progression in GC is unknown. Our meta-analysis is also the first one showing the correlations between a Ki-67 LI and clinicopathological characteristics, including depth of invasion, lymph node metastasis and pTNM stages. We showed the rates of high Ki-67 LI according to clinicopathological characteristics (Tab. II). However, there were no correlations between high Ki-67 LI and pT, pN or pTNM stages. We performed subgroup analysis for studies involving only AGC. There was no correlation between a high Ki-67 LI and poor prognosis in studies that included only AGC patients. Therefore, further studies are needed to verify the correlation between high Ki-67 LI and pTNM stages.
The current meta-analysis had several limitations, in common with other meta-analyses. Publication bias is a possible bias in all meta-analyses. Although our meta-analysis included positive results as well as negative or noncorrelated results, this common bias cannot be discounted. However, Egger's and Begg's tests were performed for confirming publication bias, and no significant bias was found. A second limitation was that the studies included were performed in regions with a high incidence of GC. Therefore, it was difficult to determine the significance of study location in the current study. A lower incidence of GC might result in a lower publication rate due to less attention to GC. However, study location had no significant influence on heterogeneity in the meta-regression analysis. Thirdly, bias could also be caused by different evaluation methods in eligible studies in the current meta-analysis. The rate of high Ki-67 LI was wide, ranging from 37.0% to 79.9%. We confirmed that dilution ratios, antibody manufacturers, immunohistochemical stain methods, cutoff values and evaluation protocols for Ki-67 LI were highly variable. These discrepancies might be responsible for the difficulty in determining a standard cutoff value in daily clinical practice. Furthermore, it makes it difficult to determine the prognostic role of Ki-67 LI. However, whether the variable results of eligible studies were caused by these discrepancies could not be determined in the current meta-analysis. Fourth, in AGC patients, a high Ki-67 LI did not predict the prognosis. However, an analysis for EGC patients could not be performed owing to insufficient information. Lastly, the comparison of the Ki-67 labeling index, according to Lauren's classification, could be important in understanding the distinct molecular and biological features. Tokuyasu et al reported that the Ki-67 LI of the intestinal type was significantly higher than that of the diffuse type (48.2 ± 14.6 vs. 24.9 ± 11.0, p<0.001) (26). However, the comparison between the intestinal and the diffuse types could not be performed in this meta-analysis owing to insufficient information within eligible studies.
In conclusion, the present meta-analysis showed that a high Ki-67 LI correlated with a poor prognosis in GC and might be an important prognostic factor in GC. Further prospective studies for standardization of methods and for the Ki-67 LI evaluation system are needed to make them eligible for application in daily clinical practice.
Footnotes
Acknowledgements
The authors would like to thank Prof. Jin Hee Sohn of Kangbuk Samsung Hospital for her considered comments.
Financial support: This study is supported by Eulji Medi-Bio Research Institute (EMBRI) grants 2011.
Conflict of interest: The authors declare that they have no conflict of interest.