
Abstract
A cross-sectional study in Nigeria was undertaken to determine the epidemiology, seroprevalence, and associated risk factors, of hepatitis E virus (HEV). A total of 462 subjects were used for the study, categorized into four groups: apparently healthy persons, pregnant women, HIV positive subjects, and animal handlers. Information was obtained from subjects using interviewer-administered questionnaire. Blood samples were collected and analyzed for HEV antibodies (IgG and IgM) using enzyme-linked immunosorbent assay (ELISA) technique. Results obtained were analyzed using Statistical Package for Social Sciences (SPSS) version 17.0 statistical software. The overall seroprevalence of IgG and IgM was 42.7 and 0.9%, respectively. Animal handlers had the highest seroprevalence (66.7%). The associated risk factors for IgM seroprevalence were rural dwelling (
Introduction
Hepatitis E virus (HEV) is a causative agent of enterically transmitted acute hepatitis in humans.1,2 It is a major public health issue in developing countries, where it causes large waterborne epidemics. 3
HEV infection is a significant global public health concern and is associated with particularly high mortality rates in pregnant women. 4 HEV is transmitted primarily by the fecal–oral route or through contaminated water. 5 It can also be transmitted across species between humans, pigs, boars, deer, chickens, and rabbits. 6 Evidence has shown that veterinarians working with pigs were at increased risk of acquiring HEV infection. 7 Pigs serve as an important reservoir for HEV, and exposure to pigs may pose a risk of zoonotic infection. Various animal species have serum antibodies to HEV, suggesting hepatitis E is a zoonotic disease. 8 Antibodies to HEV (IgM and IgG) develop at the time symptoms occur, usually before the development of jaundice. IgM anti-HEV precedes the IgG anti-HEV by a few days.
IgM anti-HEV is acute response to recent infection and its titer declines rapidly during early convalescence. IgG anti-HEV is immune response and provides protection against subsequent infections. It has been shown to persist for long periods of time (>14 years).
As cases of hepatitis E are not clinically distinguishable from other types of acute viral hepatitis, diagnosis is made by laboratory evaluation IgM and IgG. Acute hepatitis E is diagnosed when the presence of IgM anti-HEV is detected.
Although initial evidence suggested that HEV was an enterically transmitted virus with transmission mechanisms similar to those of the hepatitis A virus (HAV), the differences in the prevalence of infection of the two viruses and their differential distributions in specific population groups have led to a search for risk factors associated with HEV infection. 9
Waterborne and person-to-person spread has been documented. The potential exists for food-borne transmission, as well as from close interactions with animals and poor sanitary condition of environment and water supplies in Nigeria. It is likely that HEV infection has been thriving unnoticed since epidemiology or epidemic in Nigeria has not been documented, justifying this research. There is therefore an urgent need for a research of this nature to provide necessary information for pro-active strategy formulation especially in the study area.
Materials and Methods
Study Area
The research was carried out in Plateau State with its capital, Jos. The state is located in the North Central region of Nigeria. Jos is situated on latitude 9.5°N and longitude 8.5°E, and is 4000 feet above sea level. Principally, the state experiences two types of seasons (dry and rainy seasons), with modifications resulting from its high altitude.
Plateau State comprises 17 local government areas and 3 geographical zones. The populations are predominantly farmers and public workers. This project was carried out among rural dwellers, students, farmers, public workers, from six local government areas, representing the three geographical zones.
Inclusion Criteria
Adults and children of both sexes and all age groups that are sick or apparently healthy in these areas were chosen as the study population.
Exclusion Criteria
Individuals with drug history of immunosuppressive therapy or critically ill were excluded from the study population.
Ethical Consideration
The study protocol was reviewed and approved by the ethical committee of Plateau State Specialist Hospital Jos. All participants endorsed a written informed consent form.
Data Collection
A well-structured psychosocial questionnaire based on direct and indirect questions to obtain demographic characteristics such as age, sex, marital status, occupation, and education level was used. Behavioral characteristics as well as possible associated risk factors such as previous history of hepatitis, source of drinking water, type of toilet, personal hygiene, waste disposal, and interaction with animals were also recorded. Other factors include smoking, consumption of alcohol, blood transfusion, surgery, etc. The administered questionnaire was filled by consenting the individual before sample collection. Those who could neither read nor write were assisted using the local lingua franca, mainly Hausa and indigenous dialects.
Study Population
The populations for this study were chosen from the representative zones of Plateau State. Participants were chosen according to a stratified, multistage algorithm to produce a representation of the populace. Extensive efforts were made to ensure high participation rates ie through the hospital authorities, village heads, and churches by announcements and encouraging the people to participate. The study population included apparently healthy persons, pregnant women, HIV positive patients, and animal handlers.
Sample Size
The minimum sample size was calculated from the general formula as described by Thrustfield. 10 Sample size greater than the value determined by the formula was used to improve precision estimates of the study.
Sampling Technique
A non-probability sampling technique by purposive selection was used to select the study subjects as described by Thrustfield. 10 Those who did not fit the inclusion criteria were eliminated and the next on the list simply replaced.
Sample Collection
Altogether, 462 blood samples were collected from apparently healthy persons, pregnant women, and HIV positive subjects. A total of 5 mL of blood was collected from each subject into sterile tubes. Each blood sample was allowed to clot, and the serum was subsequently harvested into a sterile plain container, and allowed to clot and retract. The serum was separated from the clot as early as possible by centrifugation at 3500 rpm for five minutes to avoid hemolysis of the red blood cells. The serum samples were transferred safely into 2 mL cryovial and stored at −80°C until tested.
Detection of HEV Antibodies
The serum samples were screened for the presence of HEV IgM and IgG antibodies. The test was carried out using enzyme-linked immunosorbent assay (ELISA) kits for the qualitative detection of IgG- and IgM-class antibodies to HEV in human serum. The ELISA kits were manufactured by Diagnostic Automation, Inc, Calabasas, USA. Testing was carried out according to manufacturer's instructions.
Data Management and Analysis
Data recorded during sampling and laboratory findings were entered and stored in MS-Excel. The data were thoroughly screened for errors and properly coded before being subjected to statistical analysis using the Statistical Package for Social Sciences (SPSS) version 17.0 statistical software (SPSS, Inc., Chicago, IL, USA). Pearson Chi-square test was used to establish association between serological results and different risk factors considered in the study. Descriptive statistics were prepared from the study samples, and results were presented as means ± SD or percentage. To determine the correlation between the data obtained from the questionnaire and the laboratory results, odds ratios (ORs) and their corresponding 95% confidence intervals (CIs) were calculated using binary logistic regression analysis. This was to determine whether a variable was associated with HEV infection. The Pearson chi-square (χ
2
) test was used to compare categorical data, and to evaluate the difference in prevalence between groups in the univariate analysis as well as the statistical significance between relevant variables. All
Results
Seroprevalence of HEV
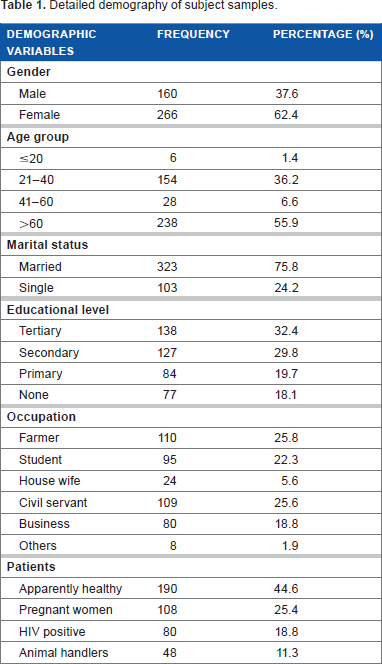
Seroprevalence of HEV in human subjects studied is presented in Table 1, indicating that an overall prevalence of 45.5% was recorded. HEV IgG recorded a significant prevalence of 42.7% (
Detailed demography of subject samples.
Analysis of Associated Risk Factors
Demographic Characteristics
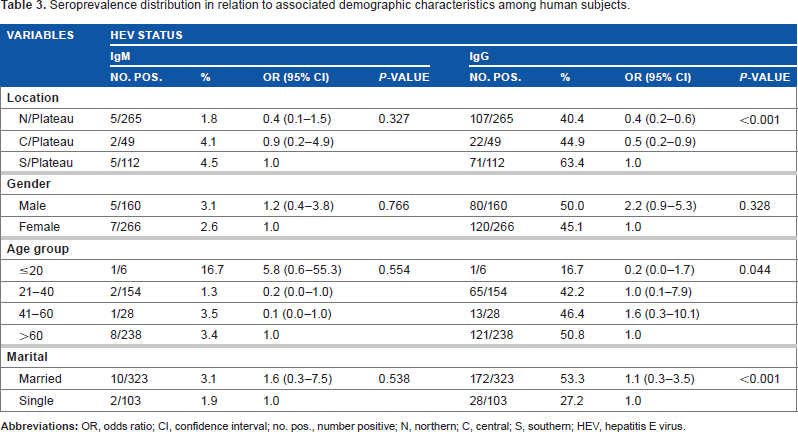
Table 2 shows the seroprevalence distribution in relation to associated demographic characteristics. Location was significantly associated with IgG seropositivity (
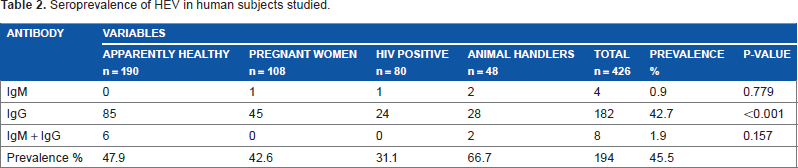
Seroprevalence of HEV in human subjects studied.
The highest prevalence was observed among older subjects in age group >60 and the lowest in subjects ≤20. A significant difference was observed with regard to IgG (
In relation to marital status, the result revealed that married people accounted for the highest prevalence with IgG 53.3% (OR 1.1; 95% CI 0.3–3.5), as against singles with 27.2% (
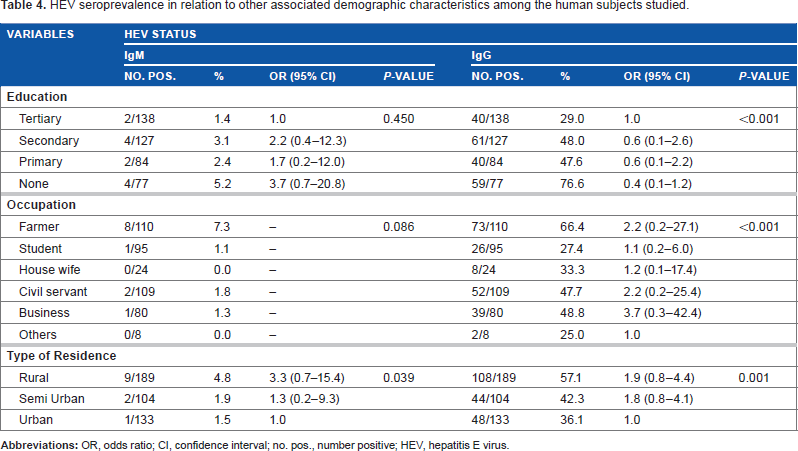
HEV seroprevalence in relation to other associated demographic characteristics is presented in Table 3. It revealed that subjects with no formal education accounted for the highest prevalence, whereas those who had attained tertiary education level had the lowest prevalence. A significant difference was recorded with regard to IgG (
Seroprevalence distribution in relation to associated demographic characteristics among human subjects.
Occupation was significantly associated with IgG seropositivity (
Residential dwelling was significantly associated with HEV seropositivity with IgG (
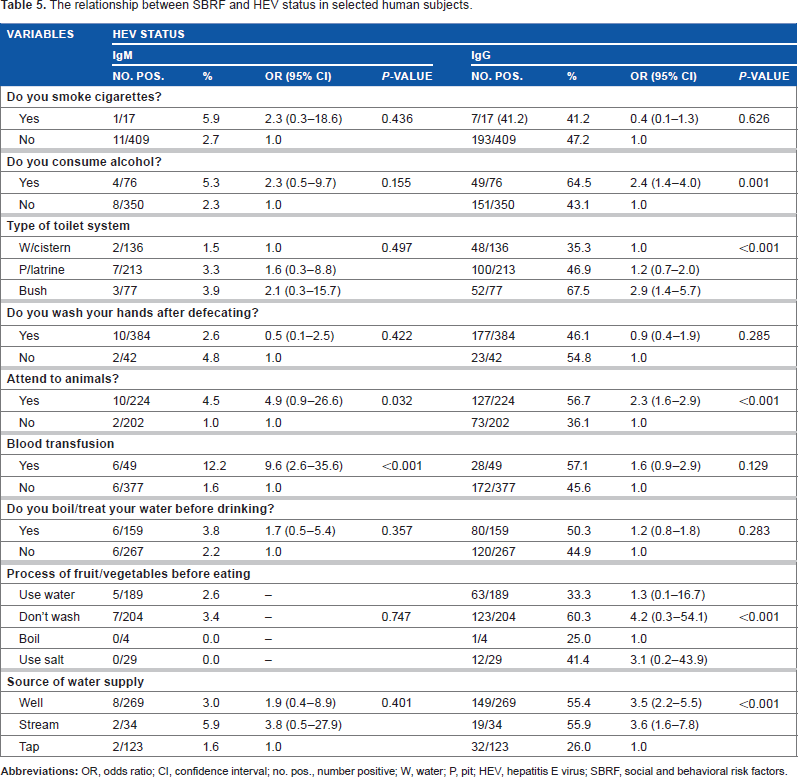
Social and Behavioral Risk Factors (SBRF)
Alcohol consumption engendered a significant association with HEV IgG seropositivity (
HEV seroprevalence in relation to other associated demographic characteristics among the human subjects studied.
The type of toilet system used was associated with HEV seroprevalence. Results indicated that those who use open field (bush) for defecation accounted for the highest IgG seroprevalence (
Although results portray no statistically significant association with washing of hands after defecation and seropositivity
Table 4 shows that attending to or handling of animals was significantly associated with HEV infection. The results were statistically significant at
The risk of infection with HEV through blood transfusion was assessed, and the results revealed a significant difference between those that have had and those that have not and association of HEV IgM seroprevalence with blood transfusion (
Considering any relationship between processing of fruits and vegetables with contracting HEV infection, the results showed there was such association and a significant difference with IgG seropositivity (
Source of drinking water as a risk factor was associated with HEV seroprevalence with a high significant difference (
The relationship between SBRF and HEV status in selected human subjects.
Discussion
Prevalence of HEV
The finding in this study of overall seroprevalence rate of 45.5% in the human population is comparable with previous finding in Indonesia (50% prevalence rate in a cross-sectional population study), 11 Albania (36.6% prevalence rate in a case–control study), 12 and Sudan (34% prevalence rate reported by Guthmann et al), 13 among the population. Apart from the similarity in study population used in these studies, there appeared to be a display of homogeneity in cultural and socioeconomic conditions across the African and Asian regions. However, the observed rate is still much lower when compared to hospital-based and outbreak studies done in Africa and Asia.14–17 The marked difference between the compared studies and the current study may be explained in part by the fact that the hospital-based and outbreak studies are likely to record higher rates because the subjects were already symptomatic. Furthermore, the disparity could be accounted for by the current study targeted at specific diverse subjects (apparently healthy persons, animal handlers, pregnant women, and HIV positive patients).
This study, however, recorded a much higher prevalence when compared to other cross-sectional population studies carried out in Europe.18–23 These discrepancies in prevalence rates are likely to be related to the rural urban differences in study areas. Other reasons may lie in the differences in socioeconomic, cultural, hygienic, and climatic factors across geographical divides as these low prevalence rate countries are developed with high socioeconomic status and much cleaner environmental sanitary conditions, when compared to Nigeria, a developing country of much lower economic status and poorer sanitary conditions. Evidence of significant geographic heterogeneity has been noted elsewhere24,25 and also in this study. Evidence from studies conducted in northern Asia emphasizes that HEV is endemic and tends to accumulate in developing countries. 26 The high prevalence in this study suggests that autochthonous HEV is circulating in Nigeria, and the infection shows under diagnosed endemicity.
Prevalence among Animal Handlers
Animal handlers accounted for the highest prevalence in the current study with 66.7%, which is comparable to 51% reported by Drobeniuc et al. 27 However, much lower rates were reported, when compared to other studies carried out in Europe.28,29 The reason for the lower rate among the European animal handlers may be explained on the basis of their better scientific approaches to farming and observance of strict biosecurity (eg shower-in/shower-out) practices. This leads to reduced infection rates unlike in developing countries. The high prevalence recorded in this study may be attributed to the fact that in countries like Nigeria, most rural people are farmers, who may be more exposed to contamination by HEV. Growing evidence suggests that individuals who work in contact with swine such as pig farmers, veterinarians, and slaughterhouse workers are at increased risk of acquiring HEV infection.14,30 The finding of higher HEV antibody among persons who work with animals is consistent with literature and is widely attributed to work-related behaviors practiced on farm settings. However, transmission of HEV has also been documented among individuals outside the farm setting and persons who are not occupationally exposed to pigs.31,32
The results obtained in this study support the link between the presence of anti-HEV antibodies and direct contact with swine, as reported by several authors.18,27,31,33,34 In contrast, studies in Sweden 29 found no significant differences between those exposed (13%) and unexposed to swine (9.3%). These differences may reflect varying levels of hygiene and local sanitation infrastructure. In the Moldova study, for example, seropositivity was significantly associated with absence of a running water supply at home. 33 The high variation among the prevalence described above might be caused by differences in sample size, country of origin, and the diagnostic assay used. In this context, it has been described that there are significant sensitivity variations in developed countries depending on the type of ELISA kit used as well as immunoblotting confirmation of the ELISA-positive samples. 35 HEV has been suggested to be a zoonotic infection where pigs play an important role in the spreading of the disease. HEV is capable of crossing the species barrier, as has been shown by means of experimental infections in pigs with a human HEV strain and in non-human primates with a swine HEV strain. 36 This supports the hypothesis that HEV reservoir may exist in animals. 37
Prevalence among Apparently Healthy Subjects
Apparently healthy subjects followed closely with a prevalence rate of 47.9%, which is comparable with the findings of Amer et al 38 in Egypt (38.9%) among apparently healthy adolescent females. The observed similarity in prevalence rate may be related to the similarity in cultural practices and socioeconomic status of populace in both countries, but the difference in rate may not be unconnected with the difference in sample population. However, the observed rate in the current study is still much higher when compared to the studies carried out in Taiwan (11%), 39 Mongolia (11%), 40 and Indonesia (20%). 41 The observed difference in comparison with the present study may be explained by differences in socioeconomic, cultural, hygienic, and climatic factors across geographical divides. This indicates that prevalence rates of HEV infection among apparently healthy individuals differ from one country to another. The high rate recorded in this study suggests that HEV infection has been autochthonously circulating, thereby resulting in subclinical infection in the population. Reasons for the lack of clinical hepatitis remain unclear but could be the result of early childhood HEV exposures, producing long-lasting immunity and/or modifying subsequent responses to exposure. 42 Alternatively, the predominant HEV strain(s) in Nigeria is(are) less virulent than those in South Asia.
HEV and Pregnancy
Pregnant women accounted for 42.6% prevalence, which is consistent and comparable with 45, 47.4, and 37% reported by Kumar et al, 43 Beniwal et al, 44 and Singh et al, 45 respectively, in India. A likely explanation may lie in the similarity in socioeconomic status as well as cultural and hygiene practices. Furthermore, most of the subjects from the studies similarly had rural lineage with its attendant influential factors. A lower prevalence was reported in Gabon (14.1%), 46 Ghana (28.6%), 47 and Central African Republic (33 %) 48 when compared to that of the current study. The reason for this disparity may be that these other nations are smaller in terms of population and hence less crowded. As the pressure on water and sanitary facilities are likely to increase in heavily populated nations, epidemic diseases related to water may arise. It is likely that there may be less pressure on health services, dealing with fewer populations with its consequence on provision of social amenities. These may include potable drinking water and exposure to other risk factors in contrast to that obtained in the current study area. Densely populated areas are associated with many problems such as lack of basic facilities and amenities, dependence for food supply, and municipality failing to solve the urban management problems such as provision of clean drinking water, waste disposal, and housing issues, with the demand for social amenities exceeding supply. 49 However, much higher rates were reported elsewhere in Asia and Africa.42,50–53 A possible reason for the marked difference compared to that of the current study may be connected to demography. As observed from these studies, majority of the pregnant women live and work in densely populated rural areas, with its attendant problems. Furthermore, domestic animals share habitat with humans; these areas are also highly prevalent for HEV. The discrepancies in prevalence are likely to be related to the rural urban differences in study areas. Other reasons may lie in the differences in socioeconomic, cultural, hygienic, and climatic factors across geographical divides in developing countries.
A unique feature associated with HEV infection is the relatively high mortality rate in infected pregnant women, which can reach up to 28%, 54 and death of the mother and fetus, abortion, premature delivery, or death of a live-born baby soon after birth are common complications of hepatitis E infection during pregnancy. 55 This underscores the importance of the high HEV prevalence recorded among pregnant women in the current study, because Nigeria is listed as one of six countries that account for 50% of global estimates of maternal deaths. 56
Prevalence among HIV Positive Subjects
The prevalence of 31.1% recorded for HIV positive subjects in this study is similar to that reported from work carried out in Russia (38.1%) among AIDS patients. 57 However, this rate is much higher than the results obtained from studies done in France (1.5 and 4.4%)58,59 and Argentina (6.6%). 60
A closer observation of the data from the current study and those reported from other studies shows that HIV patients in the current study area have higher prevalence than those in developed countries. This disparity might be as a result of (i) higher standard of living in developed than in a developing country like Nigeria, (ii) better medical and socioeconomic facilities in those countries than Nigeria, and (iii) lower risks of exposure and infection with HEV and HIV because of higher level of awareness and literacy in developed countries than in Nigeria. HEV infection may have common transmission mechanisms (risk factors) with HIV infection rather than represent an additional opportunistic infection in AIDS. 57 Data have shown that chronic infection with HEV may occur in patients with HIV infection and is associated with active hepatitis. 61
Demography and Associated Risk Factors
Age
The antibody positivity rates appeared to increase with age, and increase was marked at age >60 years with the highest prevalence. The lowest prevalence was among subjects of 20–40 years. This agreed with results from a similar study by Dong et al, 62 who reported that the prevalence of anti-HEV IgG antibodies was seen to increase significantly with age from 7.92% in children (<10 years old) to 21.48% among older persons (>60 years old). This finding is also consistent with other studies carried out in Indonesia, 11 Taiwan, 39 Mongolia, 40 Egypt, 42 Spain, 21 Albania, 12 USA, 63 India, 64 Central African Republic, 14 Germany, 23 and China 65 but contrary to the report by Adesina et al 66 who observed the prevalence of anti-HEV antibodies to be highest in ages 20–40 years. Low numbers of pediatric cases seen during HEV outbreaks further strengthen the hypothesis that children are, for unidentified reasons, less likely to be infected than adults. 67 The increase in positivity with age seen in the study area may be attributed to the high exposure of most elderly people, who are in the majority especially in rural areas, to possible risk factors, such as animal handling and fecal disposal, compared to the young and middle-aged groups who are mostly in the cities for economic reasons. Therefore, it is assumed that age is a very significant independent predictor of anti-HEV status.
It is still not clear how long HEV antibodies persist after exposure, but some studies have reported that they have a short life. 68 However, the finding from the current study that HEV IgG seroprevalence was independently associated with age >60 years could potentially be explained by a long-term persistence of HEV antibody and a consequently higher seroprevalence among older individuals. 69
A previous study detected HEV IgG in 47% of persons 14 years after acute HEV infection. 70 A follow-up study conducted by Rapicetta et al 71 among the general population reported that antibody persisted in only 37% of seropositive subjects after five years. As a consequence, the past spread of HEV infection cannot completely explain the significant trend in HEV prevalence by age.
Gender
Although no statistically significant difference was observed with regard to gender, the current study recorded proportionately higher prevalence among males than females. This is basically consistent with what had been found in other studies.14,21,63,65,72 A logical reasoning could be that in the current study area, generally, most men are more exposed to HEV infection risk factors such as irrigation farming using contaminated river water, working in animal farms, and disposal of human and animal waste. The men are also commonly involved with other environmentally related works locally considered as men's job, spending much time with the animals, and handling animals at home among others. Takahashi et al
40
in Mongolia reported a positivity rate of 11% in both sexes for IgG anti-HEV, indicating that individuals of both sexes are at equal risk of HEV infection. However, in contrast, Corwin et al
11
in Indonesia reported a higher prevalence among females than males (55 versus 47%,
Marital Status
The current study significantly associated marital status with the risk of HEV IgG seropositivity. Those who were married ran a significantly higher risk of HEV IgG seropositivity than the unmarried (
A logical explanation why marital status predisposes individuals to HEV infection (IgG;
Location and Type of Residence
Subjects who resided in southern Plateau had the highest prevalence significantly associated with IgG antibodies (63.4%) but least in northern Plateau (40.4%) (
The reason for this difference, regarding location, may be similar to the likely factors influencing prevalence with regard to type of residence. The current study significantly associated seroprevalence with type of residence. The findings revealed that rural dwellers were more at risk of infection than urban dwellers. This is consistent with the findings of Stoszek et al 42 in Egypt, Dong et al 62 in eastern China, and Labrique et al 72 in Bangladesh, which showed that prevalence was significantly higher in persons living in rural neighborhood than those in urban settings. Contributory factors may be attributed to the tropical nature of the region and possibly poor hygienic conditions of the people, and lack of potable water supply in our rural settlement. In contrast to the current findings, studies in India reported a significantly higher prevalence in urban children and population in comparison to rural subjects.64,74 This suggested that urban populations with higher density and common water supplies may be at greater risk of HEV infection. Furthermore, higher exposure of urban than rural children because of poor sanitation in urban slums is likely. Also, the probability of exposure to HEV during childhood was higher in urban than rural population. This may be because of the large numbers of people found in the urban areas leading to overcrowding in such places. This suggests that person-to-person contact is probably a major transmission factor in urban, as opposed to rural, settings. Overcrowded areas carry the risk of poor sanitation conditions and low standard of lifestyle. 75
Occupation
The current study significantly associated farming (occupational exposure) with HEV anti-IgG prevalence. This is consistent with other documented reports of occupational exposure with direct contact with animals as one of the most common possible risk factors for acquiring HEV.8,14,18,28,31,33,76,77 Galiana et al 28 further stressed from their study that people exposed to swine were 5.4 times at risk of having anti-HEV IgG antibodies than others.
From the current study, the reasonable explanation for farmers being at the highest risk compared to other occupational groups could be that they are predisposed to be in frequent direct contact with their livestock. This view was supported by Galiana et al 28 who even suggested that HEV be seen as vocational illness of swine workers. Use of contaminated water for irrigation farming and animal feces as source of manure (as the low economic status of most rural farmers renders them unable to purchase organic fertilizer) is other likely associated factors. It is of interest to note that most farms in the study area were situated close to the homes, whereas domestic animals most especially pigs, sheep, and goats and the human owners, of course, share the same habitat.
Our data contribute to the accumulating evidence that hepatitis E may be a zoonosis and specifically to the concept that it is an occupational infection of livestock workers. It appeared that the probability of exposure and reinfection to HEV is higher in farmers than in the other occupational groups in the present study. The poor environmental sanitary conditions on the farms coupled with socioeconomic status of the subjects could be other potentiating factors. 76
Attending to Animals
Consistent with other studies,15,19,36,63 the current study found statistically significant evidence that HEV IgG and IgM seropositivity was positively associated with having pets and other animals in the household of the study population. Antibody to HEV has been detected in a wide variety of animal species, 78 suggesting that exposures to pets and other animals could play a role in HEV transmission cycles. However, detection of HEV RNA in biological samples collected from animals other than swine has not been common. This probably suggests that pets may be accidental rather than primary hosts for HEV. 63
Education Background
Educational status was strongly associated with HEV IgG seropositivity (
Water Supply
The use of stream as a source of water supply was identified as a significant risk factor for HEV IgG seropositivity and proportionately higher IgM seroprevalence. This is consistent with the findings in other studies in Indonesia, 11 USA, 79 France, 80 Spain, 28 and Turkey. 19 It is also likely that all sources of water could function as a vehicle for HEV transmission and that surface water only increased the risk. 13 Contaminated water or water supplies are important sources of HEV infection especially following outbreaks in humans. 13 , 21 , 79 Indeed, Perez et al 81 also reported that the rate of HEV infection is significantly higher in people having their water supply outside rather than those inside the house. The wells were probably contaminated because of the closeness of latrines to water sources. Insufficient drinking water treatment and low standards of sanitation have been implicated in major outbreaks in developing countries where contamination of drinking water with animal or human feces is common. 82 , 83 Poor sanitation and food sources are also integral factors to enteric pathogen exposure. 83 Buisson et al 84 described how residents may be exposed to HEV from contaminated water supplies or uncooked shellfish, which could explain the occurrence of sporadic cases observed throughout the year in the Niger Delta region of Nigeria. This underscores the urgent need for provision of potable drinking water to curb the rate of infection through consumption of contaminated water.
Toilet System Used
The use of open field (bush) as toilet was significantly associated with HEV IgG seropositivity; also high HEV IgM seroprevalence was observed, placing individuals who use bush at the highest risk of infection. Such open fields over time may become highly contaminated, and the risk of contracting infection from such a place may have increased. This is consistent with the findings of Eker et al 19 who reported high rates of seropositivity among people with individual incompatibility to the hygiene rules, and denotes that personal hygiene is an important factor for prevention from HEV infection. The reason for significance of toilet system in the current study may likely be because of the poor personal hygiene and sanitary practice of the individuals. Furthermore, it may also be that this group does not wash their hands with soap and water after visiting such open field for defecation, and before preparing food and eating, considering that the major route of HEV transmission is fecal–oral. 79 The highest prevalence of HEV infection occurs in regions where low standards of sanitation promote the transmission of the virus. 85 Good personal and food hygiene could therefore significantly reduce the risks of infection.
Consumption of Fruits and Vegetables without Proper Washing
Improper washing of fruits and vegetables before eating was significantly associated with HEV IgG seropositivity. Those people who consumed fruits and vegetables without washing at all were found to be at the highest risk of infection, and this was substantiated by a similar finding in Turkey. 19 This suggests that contamination of the food items could come from external sources, such as using contaminated irrigation river/stream water for growing vegetables, the wide-spread use of animal fecal waste as manure, and poor and unhygienic handling of fruits. This further emphasizes the importance of proper sanitary practices.
Practice of Hand Washing
It was observed that those who do not wash their hands after defecation appeared at higher risk of HEV infection than those who wash, although no statistical difference between the two groups was recorded. This is similar to the report by Eker et al 19 who also reported no statistically significant difference with reference to the practice of hand washing or otherwise between two groups. However, the results from the current work disagree with that of Stoszek et al. 42 The reason for the discrepancy is not clear and may require further clarification.
History of Transfusion
HEV infection is emerging as a potential new threat to blood safety after several cases of transfusion-transmission were reported from non-epidemic countries.
86
The current study observed a strong significant association of HEV IgM (
Alcohol Consumption
Alcohol intake accelerates the degree of hepatic fibrosis, increases the risk of liver diseases, and worsens the clinical outcome of liver diseases including hepatocellular carcinoma.
90
Regular consumption of alcohol predisposes individuals to higher risk for drug-induced liver injury, independent of viral infections.
91
The current study observed a significant association between alcohol consumption and HEV IgG seropositivity (
Conclusion
This study suggests that a significant number of people in the study area of Plateau State had been exposed to the HEV. The finding of a higher risk for HEV infection in rural areas than in urban areas suggests the presence of local risk factors. Infection increases with increase in age, and males seem to be at higher risk than females. The high rate of prevalence of anti-HEV in healthy subjects indicates that subclinical infection may exist.
Animal handlers, most especially pig handlers, were at risk of HEV infection, irrespective of age, sex, location, and history of blood transfusion. Therefore, pigs and goats rather than sheep or cattle may act as a natural reservoir of HEV infection in the study area. The findings of this study do add to the growing evidence that hepatitis E may be a zoonosis and specifically to the concept of it as an occupational infection of livestock workers.
Findings from this study suggest that socioeconomic status and education is generally the biggest factor behind higher rates of HEV infection irrespective of age, sex, location, occupation, and other factors.
Preventive public health measures should be reinforced among individuals and communities particularly domestic animal handlers and farmers. Redefining of the donor screening policy by blood banks is advocated. Constant monitoring of drinking water should be carried out in rural areas. Government's intervention is solicited for the provision of potable water supply especially in rural communities. HEV remains an under-recognized and significant public health problem in Plateau State, and this calls for further investigation.
Author Contributions
SAJ and SEA conceived and designed the experiments. SAJ and SEA analyzed the data. SAJ wrote the first draft of the manuscript. SEA and KAA contributed to the writing of the manuscript. SAJ, SEA, and KAA agreed with the results and conclusions. SAJ, SEA, and KAA jointly developed the structure and arguments for the paper. SAJ made critical revisions and approved the final version. All authors reviewed and approved the final manuscript.
Footnotes
Acknowledgments
We gratefully acknowledge the immeasurable assistance of the Medical Microbiology Department, University of Cape Town, South Africa. We thank immensely all those who participated in the study. We appreciate the unquantifiable contribution of the following people: Noel Dus, Mrs Lydia N. Ndam, Aloysius Ujah, and Abubakar Ibrahim. We are immensely indebted to Sophia Osawe, Dr Mamadou Kaba, and Dr. Adah Ruth Otelahu for their critical appraisal.