
Abstract
Background
Individuals with human T-cell lymphotrophic virus type-1 (HTLV-1)/HIV-1 coinfection have been demonstrated to undergo CD4+ lymphocytosis even in the face of immunodeficiency and increased vulnerability to opportunistic pathogens that can lead to poor prognosis.
Objective
This study investigated the prevalence as well as the effects of HIV-1/HTLV-1 coinfection on CD4+ cell counts, routine hematology, and biochemical parameters of study participants.
Materials and Methods
This prospective cross-sectional study involved 184 blood samples collected from HIV-1-seropositive individuals attending HIV-special clinic of the University of Abuja Teaching Hospital, Gwagwalada, Nigeria. These samples were analyzed for anti-HTLV-1/2 IgM antibodies using enzyme-linked immunosorbent assay, CD4+ cell counts, and some routine hematological and biochemical parameters. All samples were also tested for HTLV-1 provirus DNA using real-time polymerase chain reaction (PCR) assay.
Results
Of the 184 subjects studied, 9 (4.9%) were anti-HTLV-1/2 IgM seropositive; however, upon real-time PCR testing, 12 (6.5%) had detectable HTLV-1 provirus DNA. The CD4+ cell count was significantly high in HTLV-1-positive (742 ± 40.2) subjects compared to their HTLV-1-negative (380 ± 28.5) counterpart (
Conclusion
All subjects (100%) who were HTLV-1/HIV-1-coinfected had normal CD4+ counts. This gives contrasting finding on the true extent of immunodeficiency of subjects. So it is suggested to be very careful in using only CD4+ counts to monitor disease progression and as indicators for antiretroviral therapy (ART) in resource-limited settings. In such conditions, there may be a need to test for HTLV-1 alongside HIV viral loads in order to begin appropriate ART regimens that contain both pathogens.
Introduction
Human T-cell lymphotrophic virus type-1 (HTLV-1) was the first human retrovirus to be identified, and it is structurally related to other viruses of the Retroviridae family. 1 Since its discovery in 1979, three additional deltaretroviruses (ie, HTLV-2, HTLV-3, and HTLV-4) were subsequently discovered, but only HTLV-1 and HTLV-2 have been associated with human diseases. 1
The HTLV-1 was first isolated from a patient with a rare type of adult T-cell leukemia (ATL). The virus was later established to be associated with a neurological disease, HTLV-1-associated myelopathy (HAM)/tropical spastic paraparesis. 2 Other pathologies that have also been linked to HTLV-1 included poliomyositis, polyarthritis, uveitis, and infective dermatitis in children. ATL was first described in Japan by Uchiyama et al 3 and has since been reported in many other parts of the world.
Epidemiologically, areas are characterized as endemic when the prevalence of HTLV-1 falls within 0.5%–20% of the population (depending on age and gender) and characterized as nonendemic when the prevalence is <0.1%. 4 The seroprevalence rates tend to increase with age, and they are higher in females than males. 4 Areas of high prevalence for HTLV-1 include Japan, Sub-Saharan Africa, Caribbean basin, South America, Melanesia, and the Middle East. 4 HTLV-1 has been exhaustedly studied in different subjects, especially, blood donors, injection drug users, thalassemia patients, and HIV-infected individuals.5–7
In Nigeria, most previous serological surveys were conducted on blood donors. Williams et al 8 reported a seroprevalence of 7.0% among blood donors in Ibadan, Fleming et al 9 reported an overall prevalence of 3.7% in Zaria city of Northern Nigeria, and Analo et al 10 reported a prevalence of 0.7% among blood donors in Lagos city of south-western Nigeria. Surprisingly, in 2015, none of the 300 blood donors studied had HTLV-1 antibody. 7 However, there are no recent representative data regarding prevalence of HTLV-1 in the general Nigeria population or specific patient subgroups, particularly, the HIV-infected individuals.
HTLV is transmitted via sexual contact, breast-feeding, blood transfusion, and among intravenous drug users, in a similar fashion to the pandemic HIV. 11 Coinfection of the same cell by HTLV-1 and HIV is possible. 12 Some studies suggest a more severe clinical course with shortened survival for AIDS patients coinfected with HTLV-1, whereas others demonstrated no detrimental effect of HTLV-1 upon progression of HIV infection. 12
Like other human retroviruses, HTLV-1 causes a lifelong infection of T-lymphocytes, in particular, CD4+ cells. However, unlike HIV, the immunological hallmark of HTLV-1-infected individuals is a sustained proliferation of T-cells driven by the HTLV-1-encoded Tax protein. 13 The subsequent transactivation of cellular genes by the Tax-encoded region can result in malignant transformation, although this is rare. 14 In the majority of cases, cytotoxic T-cells effectively control the virus by lysis of infected lymphocytes, which in turn results in the release of inflammatory cytokines that can be pathogenic.13,14
On account of these various pathophysiological mechanisms, HTLV-1 is associated with a diverse range of pathologies, including malignant disease, inflammatory syndromes, and infective complications.13,14 Whether HIV-1 coinfection with HTLV-1 is associated with a faster progression to AIDS remains a contentious issue, although a number of studies have suggested as much. 15 What is, however, less controversial and perhaps of greater relevance is the effect of HTLV-1 on T-lymphocytes, and in particular, its association with CD4+ lymphocytosis in HIV-1-coinfected patients. 16
It was once asserted that a CD4+ lymphocyte count cannot always be considered to be a reliable marker of immunological competence in HIV-infected people, especially in patients coinfected with HTLV-1.1,16 Normal or high CD4+ cell counts in such persons can be on account of reactive or clonal expansion of T-lymphocytes and can confound HIV diagnosis and delay initiation of chemoprophylaxis and highly active antiretroviral therapy (HAART).1,16 Conversely, high CD4 count could be attributable to increased macrophage population especially in early HIV infection since HIV bind, enter, and infect host cells via CCR5 and CD4 cells on macrophages. 17
The prognosis of ATL and HAM is poor due to the rapid course of the disease, difficulty of confirming the diagnosis, and undetected occurrence of ATL/HAM. The current diagnosis of HTLV-1 infection is based on the search of specific antibodies; nevertheless, several studies conducted pointed deficiencies of the commercially available enzyme-linked immunosorbent assay (ELISA) kits in detecting HTLV-1, especially in HIV/AIDS patients. In view of this, we sought to search for the presence of HTLV-1 provirus DNA from 184 consented HIV-1-infected individuals attending HIV-special clinics of the University of Abuja Teaching Hospital (UATH), Gwagwalada, Nigeria.
Materials and Methods
Study Design
This was a prospective cross-sectional study carried out on blood samples of 184 ART naïve HIV-1-infected individuals. They were screened and confirmed HIV-1 seropositive using Uni-Gold™, Determine™, and Multispot™ HIV-1/HIV-2 test strips. These samples (80 males and 104 females) were collected at the HIV-special clinic of the UATH, Gwagwalda, FCT Abuja, Nigeria. Informed consent was obtained from all participants. Their mean age was 34 years (range 18–60 years). All subjects were screened using rapid diagnostic test in order to be sure that they were seronegative to hepatitis-B and -C viruses. They were also screened to ascertain no history of pulmonary tuberculosis.
Study Area
This was a hospital-based study carried out at UATH, a tertiary hospital located in the federal capital territory of Nigeria. It is a center for President's Emergency Plan for AIDS Relief interventions. The center diagnoses new cases of HIV infections and monitors those on therapy. Our subjects were recruited at this center. All laboratory parameters were analyzed at the Immunology Laboratory of UATH except the molecular detection of HTLV-1 provirus DNA, which was conducted using real-time polymerase chain reaction (PCR) at DNA Laboratory and Molecular Diagnostic Center at Kaduna state, Nigeria.
Sample Size Calculation
Prior to this study, HTLV-1 infections in HIV patients have never been conducted in Nigeria; hence, the sample size was determined using data from a prevalence rate conducted by Galetto et al 18 in Brazil with a prevalence of 1.9% in HIV subjects using PCR; therefore, the minimum sample size at 95% confidence level was 30. However, statistical credence was given to the study by increasing the sample size by sixfold. Thus, 184 subjects who voluntarily consented to participate were recruited for the study.
Sample Collection and Preparation
Samples were collected between October 2014 and January 2015. Using new sterile syringes, 5 mL of blood was collected aseptically, 3 mL of which was gently and carefully dispensed into ethylenediaminetetraamine acid (EDTA) container, while the remaining 2 mL was dispensed into plain vacutainer tubes. The tubes were then appropriately labeled with participants' study number. Sera from these blood samples in plain tubes were separated by allowing the blood to clot at room temperature and centrifuged at 2500 rpm for 10 minutes. The sera were then separated and transferred using clean Pasteur pipettes into serum containers and stored at −4°C until laboratory analysis. Whole blood samples for CD4+ cell count and hematology/biochemical and buffy coats for HTLV-1 provirus DNA tests were analyzed within six hours of collection. However, serum samples for ELISA were stored at −20°C and later analyzed within 48 hours of collection.
Analytical Procedures
Determination of Hematological Parameters
We made use of Sysmex™ 300 automated hematology analyzer for total white cell count, monocyte, lymphocyte differentials, and hemoglobin concentration. Red blood cells (RBCs), white blood cells, and differentials were counted using direct current detection method with coincidence correction. Automatic discriminators separated the cell populations based on complex algorithms. The intensity of the electronic pulse from each analyzed cell was proportional to the cell volume. The Packed Cell volume (PCV) was directly determined based on the red cell count and volume detection of each individual RBC. Hemoglobin was determined using methemoglobin method.
Determination of Serum Biochemical Analytes
We made use of Vitrox-360™ automated chemistry analyzer for serum potassium, sodium, biocarbonate, urea, and creatinine concentrations. After the tray was loaded with samples, a pipette aspirated 100 μL aliquot of samples and discharged it into the reaction vessel. Reagents were dispensed into the reaction vessel. After the solution was mixed, it was passed through a colorimeter that measures its absorbance, while it is still in the reaction vessel. The analyzer then calculated the concentration of the analyte. The Vitrox-360 ran five serum biochemical of 10 samples at a time (10 minutes).
Determination of CD4+ Cell Count
Cluster of differentiation-4+ cell count in whole blood was determined using Partec™ Cyflow analyzer model SL3 based on manufacturer's instruction. It worked on the principle of light scatter (due to different size or granularity of the cell) combined with fluorescence of cells after staining with monoclonal antibodies to cell surface markers tagged to fluorescent dyes. Population of interest were then identified and gated. Absolute CD4+ cell counts were then determined using single-platform methodology.
IgM ELISA
Serum samples were analyzed by ELISA using anti-HTLV-1/2 IgM ELISA kit, lot number 8196-12, Diagnostic Automation, Inc. All samples and reagents were brought to room temperature. The test was performed according to manufacturer's instructions. This was an antigen “sandwich” ELISA method that used polystyrene microwell strips precoated with recombinant HTLV antigens expressed in
Real-Time PCR
To detect HTLV-1 provirus in peripheral blood cells, DNA was extracted from 200 μL blood buffy coat using the High pure extraction kit (Roche Diagnostics GmbH). Quantitative determination of the amplified products was done with the Rotor Gene 6000 (Corbett Research). Real-time detection system was in accordance with the manufacturer's instructions, which was subjected to PCR with a Maxima probe qPCR Master Mix (2X) kit (Fermentas). Briefly, as previously described by Gabet et al, 19 the primer set for the HTLV-1 tax gene was PXF (5'-CAAACCGT-CAAGCACAGCTT-3') positioned at 7163–7182 and PXR (5'-TCTCCAAACACGTAGACTGGGT-3') positioned at 7385–7364 and the probe for HTLV-1 tax gene was PXT (5'-TTCCCAGGGTTTGGACAGAGTCTTCT-3') positioned at 7331–7355. The thermal cycler profile was optimized and validated with heat activation (15 minutes at 95°C) of hot-start Taq polymerase, followed by 40 cycles of denaturation (30 seconds at 95°C), annealing (30 seconds at 50°C), and extension (30 seconds at 72°C). Each sample was analyzed in duplicate using 150 ng of DNA for tax. An uninfected DNA sample and water served as negative controls.
Ethics Statement and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the ethical research committee of the UATH (ethical approval number: FCT/UATH/HREC/PR/347). The study was appropriately explained to all participants and thereafter, they individually gave verbal and/or written consent for inclusion before they voluntarily participated in the study. All data were analyzed anonymously throughout the study.
Statistical Analysis
Data were systematically analyzed as appropriate. Mean ± standard deviation of mean (SD) were derived, and Student's
Results
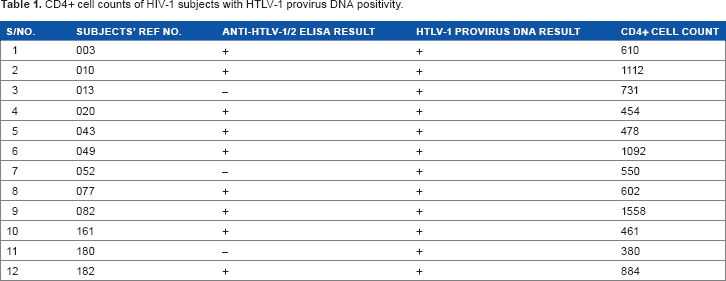
A total of 184 subjects participated in this study. The seroprevalence of anti-HTLV-1/2 IgM antibodies was 4.9% (Table 1); however, 12 (6.5%) subjects were HTLV-1 provirus DNA positive. The CD4+ cell count in those with HTLV-1 and HIV-1 coinfection was significantly higher than those with HIV-1 monoinfection (
CD4+ cell counts of HIV-1 subjects with HTLV-1 provirus DNA positivity.
HTLV-1 positivity distribution across some hematological parameters studied.
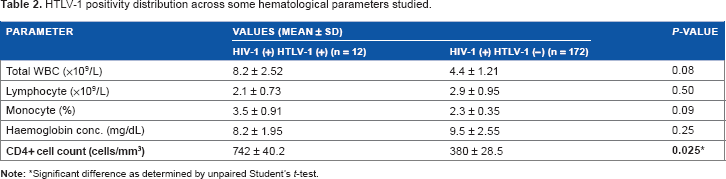
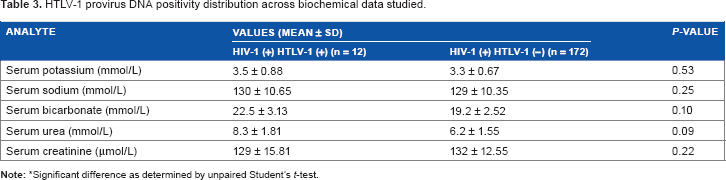
Significant difference as determined by unpaired Student's
HTLV-1 provirus DNA positivity distribution across biochemical data studied.
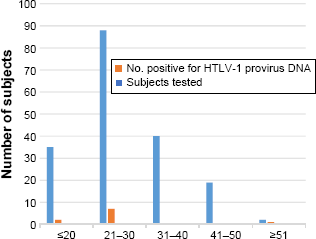
Age distribution of HTLV-1 provirus DNA positivity among HIV-1 subjects.
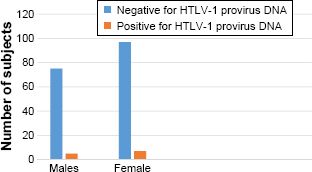
Gender distribution of HTLV-1 provirus DNA positivity among HIV-1 subjects.
Discussion
CD4+ cell count is the most used selection criterion to determine ART eligibility for HIV-infected individuals. However, coinfection with HTLV in these patients may represent an added problem regarding timing to initiate and types of ART combinations especially in sub-Saharan Africa where unavailability of sufficient laboratory reagents/equipment impede diagnosis of most opportunistic viral pathogens in people living with HIV/AIDS. This cross-sectional study has confirmed the elevation of CD4+ cell counts in HIV-1/HTLV-1-coinfected individuals compared to their counterparts with HIV-1 monoinfection in Abuja, Nigeria. To the best of our knowledge, this is the first study in Nigeria that investigated the effects of HTLV-1/HIV-1 coinfection on CD4+ cell counts, routine hematology, and biochemical indices of the study participants.
In this study, we reported an overall 4.9% seroprevalence of anti-HTLV-1/2 IgM in ART-naïve HIV-infected individuals in Abuja, Nigeria. This finding collaborates the previous study conducted by Gudo et al 20 who recorded a seroprevalence of 4.5%, although other studies conducted by Gouhier et al 21 and Cabie 22 reported contrary seroprevalence values (5.4% and 3.4%, respectively). As expected, coinfected individuals presented with normal CD4+ cell counts (742 ± 40.2 cells/mm3) irrespective of whether they progress to AIDS, contrasting with depletion of CD4+ cell counts observed among HIV monoinfected patients over time. This study is in consonance with those of Gudo et al, 20 Van Veldhuisen et al, 23 Casseb et al, 24 Fantry et al, 25 Nadler et al, 26 Scapellato et al, 27 and Schechter et al, 28 who reported that HTLV-1/HIV-1-coinfected patients progress to AIDS irrespective of high and stable CD4+ cell counts and higher levels of activation markers, contrasting with the depletion of CD4+ cell counts observed in HIV monoinfected patients with AIDS. In cases of HTLV-1/HIV-1 coinfection, it has been suggested that HIV-1 viral load alongside clinical presentation, rather than CD4+ cell counts, should be used to monitor HIV disease progression. 29 The anti-HTLV-1/2 IgM ELISA used to detect HTLV infection was not totally consistent with the detection by RT-PCR. This might be due to low serum IgM concentration below detection threshold during early days of HTLV infection due to impaired antibody synthesis due to HIV-1/HTLV-1 coinifection. 29
The predictive value of CD4+ cell count as a marker of HIV-related immunosuppression and disease stage for persons coinfected with HIV-1 and HTLV-1 is not similar for individuals infected with HIV-1 alone. HTLV-1 promotes the clonal expansion of CD4-infected T-lymphocytes causing an elevation of less competent CD4+ T-cells in coinfected persons. 30 When compared to HIV-infected patients with CD4+ cell counts greater than 200 cells/mm3, HIV/HTLV-1-coinfected individuals with similar CD4+ cell counts are at higher risk of developing opportunistic infections.31,32 In addition, cell immortalization and transformation induced by Tax and Rex proteins encoded by HTLV-1 genes constitute major events related to uncontrolled CD4+ T-cell growth and proliferation.33,34 Thus, a high CD4+ cell count in coinfected persons does not necessarily reflect a competent immune system.
On the contrary, in consideration of the clinical significance of CD4+ cell counts for HTLV patients, the 2012 study conducted by Gudo et al on the performance of absolute CD4+ cell count in predicting coinfection with HTLV-1 in ART-naive HIV-infected patients in Maputo, Mozambique, reported that the presence of high absolute CD4+ cell counts proved to be a good predictor of HIV/HTLV coinfection among HIV symptomatic group patients in their setting. This team of researchers applied the receiver operational characteristics curve analysis to determine the best cutoff points of absolute CD4+ cell counts to predict coinfection. The best performance was achieved at the cut-off value of 500 cells/mm3 at which the sensitivity, specificity, positive predictive value, and negative predictive value were 54.2%, 87.2%, 24.0%, and 96.2%, respectively. Their data demonstrated that CD4+ cell counts as a parameter could predict ~50% of HTLV-1 coinfections occurring in symptomatic ART-naïve HIV patients and provide clinicians and stakeholders with evidence on the performance of CD4+ cell counts in predicting coinfection. This information was particularly vital in resource-limited countries for developing guidelines on addressing HTLV-1/HIV-coinfected patients.
In our study, HTLV-1/HIV-1 coinfection was most detected in the age group of 21–30 years, 7 (53.3%), and none in those aged 31–50 years. This was in consistence with earlier study by Gudo et al 16 on the basis of the patients' age and their HAART naïve status. They believed that HTLV-1 infection preceded HIV infection. Considering that individuals chronically infected by HTLV-1 progress with immune activation, it is believed that these patients acquired HIV-1 infection in a preactivated immune milieu, and the presence of immune hyperactivation turns them more susceptible not only to acquire HIV but also to progress faster to poor prognosis. The age-stratified distribution in this study was not in consonance with previous studies that showed that the prevalence of HTLV-1/2 increases markedly in participants aged 30 years or over.35–38 The disparity between our findings and those of previous studies could be as a result of differences in socioeconomic lifestyles and predominant risk factors (especially increased sexual activities and sharing of sharp objects) in youths of 21–30 years group. These lifestyles tend to lessen with increase in age.
HTLV-1 positivity in this study was more among females than male counterparts. It was previously reported that there was no association between HTLV infections and gender predilection. However, some authors argued that biological factors could be used to explain the higher efficiency of HTLV transmission in females particularly due to changes in the vaginal mucosa in women with high-risk behavior, such as, sex work.39,40 Due to the low number of HTLV-1-positive cases in this study (
Findings from our study revealed that HTLV-1/HIV-1-coinfected individuals had higher but statistically insignificant total leukocyte counts (mean: 4.8 versus 4.4 × 10
3
cells/L,
Findings from the serum biochemical investigations in this study revealed that HTLV-1/HIV-1-coinfected individuals had higher but statistically insignificant parameters for potassium concentration (mean: 3.5 versus 3.3 mmol/L,
Conclusion
CD4+ T-cell count in persons coinfected with HIV-1 and HTLV-1 may mask immunosuppression, if used as an indicator for determining immunodeficiency, it may delay ART, which will result in missed opportunity to reduce HIV progression to AIDS and increases the risks of contracting opportunistic infections and complications related to chronic immune activation.
Recommendations
It is suggested to be very careful in using only CD4+ counts to monitor disease progression and as indicators for ART in resource-limited settings, such as, Africa. In HTLV-1/HIV-1 coinfection, there may be a need to test for HTLV-1 alongside HIV viral loads in order to begin appropriate ART regimens that contain both pathogens.
It is recommended to also look at HIV-1 proviral DNA, as well as to test viral loads of HTLV-1 and HIV-1, both in the sera and in the cells. This will provide insight on whether HTLV-1 infection supports HIV-1 latency, the main barrier toward HIV-1 eradication. As HIV-1/HTLV-1 coinfection results in poor prognosis of patients, although the CD4+ cell number remains high, it may be useful to look at some known immune cells exhaustion markers such as programmed cell death protein 1 in these patients.
Author Contributions
Conceived and designed the experiments: IAN. Analyzed the data: AEA. Wrote the first draft of the manuscript: AUE. Contributed to the writing of the manuscript: MSS. Agree with manuscript results and conclusions: JTM and AB. Jointly developed the structure and arguments for the paper: IAN and AEA. All authors reviewed and approved of the final manuscript.