
Abstract
Cytomegalovirus (CMV) is a significant pathogen causing disease in renal transplant patients. The highest incidence of CMV disease occurs during the first 3 months post-transplant and is most problematic in CMV-naïve transplant recipients. In this study, we conducted a retrospective review of two databases, the Australia and New Zealand Dialysis and Transplant Registry (ANZDATA) and the National Hospital Morbidity Database, from the Australian Institute of Health and Welfare (AIHW), to examine CMV in renal transplant recipients. The first source looked at CMV serostatus at the time of transplantation and the second recorded hospital admissions for recipients with invasive CMV disease.
From the ANZDATA registry, we obtained information from 13,530 renal transplants recipients from 1980 to 2004. Of these recipients, 7808 had a known CMV serostatus, of which 65.7% (5134/7808) had a positive sero antibody status and 34.2% (2674/7808) had a negative sero antibody status. In univariate analysis, factors significantly associated with renal rejection were being male, recipient age <50 years, being diabetic, being diagnosed with cancer at some point and having a positive EBV status. Positive CMV serostatus was not a contributing factor. Between 1993 and 2001 there were 1445 renal transplant recipients hospitalized in Australia with a diagnosis of CMV disease, of which 38% (554/1445) had CMV disease as a principal diagnoses. The average annual rate of admissions with any diagnosis was 3871 episodes per 100,000 people living with a functioning graft.
Preventative strategies for CMV in renal transplant recipients should be a priority. New vaccines for CMV may soon be available and renal transplant recipients would be a suitable target group for vaccination.
Keywords
Introduction
Currently, cytomegalovirus (CMV) is a common cause of morbidity and mortality among patients receiving chronic maintenance immunosuppression [1] and is often considered the most important infection in renal transplantation [2]. Recurrent CMV disease has been reported to occur in 6%–59% of solid organ transplant recipients [3].
Generally, the highest incidence of CMV disease occurs during the first 3 months post-transplant [4], and is most severe in CMV naïve (CMV seronegative) recipients who receive an organ from a CMV seropositive donor (D+/R–) [5]–[8]. Other risk factors for CMV disease include graft rejection and increased levels of immunosuppressive therapy, including anti-lymphocyte therapy, high dose corticosteroids, and mycophenolate mofetil [9]–[11]. Severe graft rejection and increased immunosuppression may cooperatively stimulate the development of active CMV infection in renal transplant recipients and CMV may activate the immune response to the graft [12].
Although the impact of CMV disease is well documented in this population, the disease burden has not been well established in the hospital setting. As single centers may be subject to referral bias and may either inflate, or miss episodes treated in other centers and deflate, the true rate of disease in renal transplant recipients, we retrospectively examined two national registries: the Australian and New Zealand Dialysis and Transplant Survey [13] and the Australian Institute of Health and Welfare [14] hospitalization database. Our objectives were to analyze the burden and patient survival associated with CMV disease affecting renal transplant recipients in Australia and New Zealand.
Methods
Data Sources
Information from the Australia and New Zealand Dialysis and Transplant Registry (ANZDATA) [13] was chosen as the first source of information for this retrospective study. The ANZDATA registry collects information every 6 months from all renal transplant units throughout Australia and New Zealand about all patients receiving chronic renal replacement therapy (RRT). All patients who begin RRT with a diagnosis of chronic renal failure and in whom RRT was intended to be a chronic and indefinite treatment are included on the registry. Full details regarding the structure and methods of this registry are reported elsewhere [15]. The collection is complete from the first RRT in Australia and New Zealand in 1963 and includes all renal units in both countries. The registry relies on the voluntary contribution of renal unit staff for the completion and return of data forms. Quality of reported data, data entry and consistency are routinely monitored for all data held in ANZDATA. If transplanted, patient records are also crosschecked with the Australian and New Zealand Organ Donation Registry and Tissue Typing Centres.
The collected data consists of information about the underlying cause of end-stage renal disease, demographic details (age, sex and racial origin), a limited range of comorbidities (e.g. the presence of coronary artery disease, peripheral vascular disease, cerebrovascular disease, chronic lung disease, treated hypertension, and smoking), acute rejection (biopsy proven), the type and dose of dialysis treatment and details about renal transplantation. For this study, a number of variables were created for specific analysis including specific age groups (older recipients (≥50 years) vs. younger recipients (<50 years) and Indigenous status (Aboriginal/Torres Strait Islander or Maori racial origin).
Serologic testing for CMV and Epstein-Barr virus (EBV) has increased over time, with serum CMV and EBV immunoglobulin G (IgG) recorded by the ANZDATA Registry. However, the registry does not collect follow-up CMV or EBV serology after transplantation. CMV serology for cadaveric donors has also been recorded since 1989 and EBV serology since 1998 by the Australia and New Zealand Organ Donor Registry (ANZOD) [16], but serology for living kidney donors has not been collected on a systematic basis until very recently. Analyses included all patients in Australia who received a transplant after January 1, 1980.
The second source of information for this study was data drawn from the National Hospital Morbidity Database (NHMD) complied by the Australian Institute of Health and Welfare [14]. A retrospective review of hospital discharge records for the period of July 1993 to June 2001 was conducted. The NHMD is a collection of electronic confidentialised summary records for admitted patients dying/discharged from public and private acute and psychiatric hospitals as well as private freestanding hospital facilities in Australia. As CMV, disease mainly occurs in high-risk populations and usually results in hospitalisation; this data represents an appropriate source of information on the epidemiology of clinically relevant disease.
All patients whose records contained a diagnosis with the specific CMV code ICD 9: 078.5, 996.81 for the period 1993–1998, or ICD-10: Z94.0 T86.1 and B25x for the period 1999–2001, in any of the diagnosis fields were included. The principal diagnosis was defined as “that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care” [17]. However, patients with a non-principal diagnosis were also included to get a more complete picture of the burden of disease attributable to CMV.
Discharge records include such information as diagnoses and procedure codes, length of stay (LOS), patient demographics (e.g. sex, age group, state), year and separation mode, and hospital attributes. The age groups were divided into 0–4, 5–9 and further 5-year-classes until 85 years and above. We were unable to obtain information regarding the use of antibiotics, alcohol, tobacco, and the results of microbiologic or radiology procedures and time since transplantation.
Statistical Methods
Average annual rates of hospitalisation and the average rate by sex and age group were calculated using the renal recipient population data collected by ANZDATA. All analysis was done using EPI-INFO (CDC, Version: 3.4.1, 2007) and Egret (Cytel Software, Version: 2.0.31, 1999). Statistical significance was defined as p < 0.05. Variables with p < 0.10 in univariate analysis for a relationship with CMV serostatus were entered into multivariate logistic regression analysis as covariates.
Results
Renal Transplant Notifications in Australia and New Zealand
Between 1980 and 2004, there were 13,982 transplant operations performed in Australia and New Zealand. In Australia, by the end of December 2004, there were 14,221 patients receiving RRT. Of these, 6,269 had a functioning kidney transplant. The median age of transplant recipients was 47.6 years (range was 2.9–74.8 years). In New Zealand, during 2004 there were 105 transplant operations performed. As in Australia, the rate of transplantation for New Zealand patients was highest amongst those less than 14 years old and declined with age thereafter.
From the ANZDATA registry, we were able to obtain information from 13,530 renal transplants recipients between 1980 and 2004. Out of these, 7808 recipients had a known CMV antibody status, of which 65.7% (5134/7808) was CMV seropositive and 34.2% seronegative (2674/7808). Comparison of factors between recipients who were seropositive, seronegative or who had an unknown serostatus is shown in Table 1. For some of the documented co-morbidities such as EBV, the distribution of cases in the unknown serostatus group was slightly lower than the number recorded for recipients with known CMV serostatus.
Demographic factors from ANZDATA assessed in renal transplant recipient.
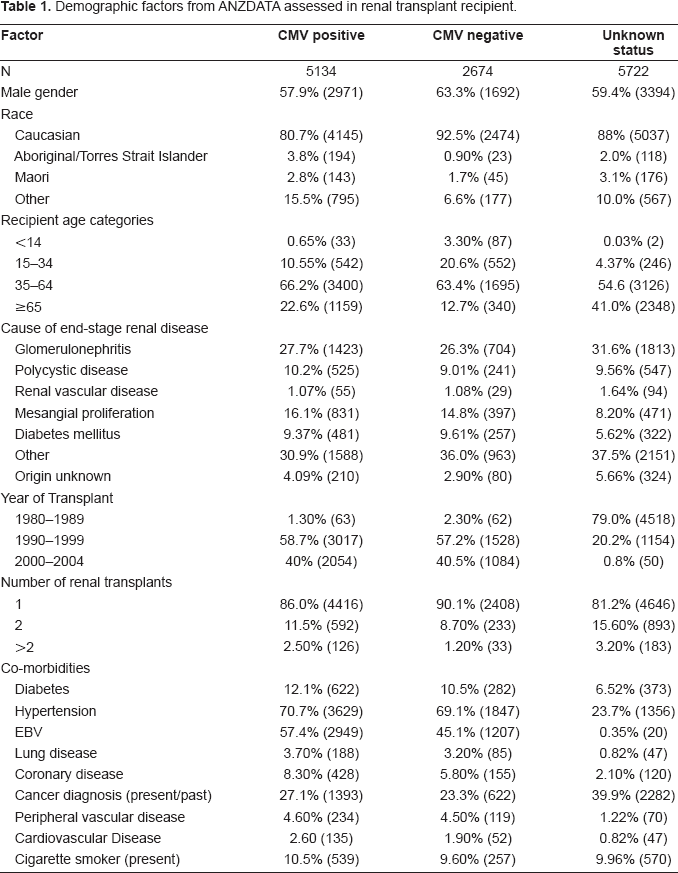
Figure 1 compares the rate of CMV serostatus in renal recipients from ANZDATA to results obtained from a large, nationally representative CMV serosurvey. The sera for that survey were opportunistically collected from public and private laboratories in all Australian States and Territories and a representative sample by age and gender were tested for CMV antibody. The complete methods of the serosurvey are documented previously [18].
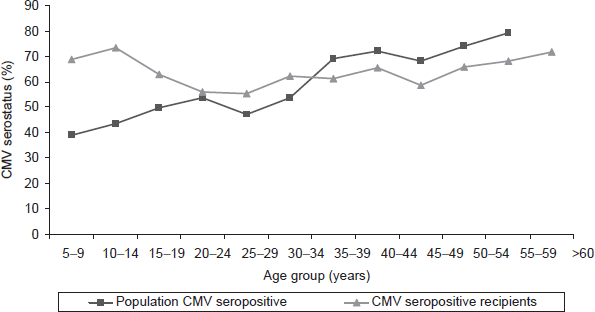
CMV seroprevalence by age group of general population vs. CMV seropositive renal transplant recipients, Australia.
The results of the serosurvey showed that firstly the population-weighted rate of CMV seropositive subjects aged between 1 and 59 years was 57% (95% CI: 55.2%–58.6%) and secondly, that the seroprevalence continued to rise with age from 50% (95% CI: 48.5%–58.7%) in 20–24 year olds to 79% (95% CI: 72.7%–84.7%) in 50–59 year olds. By comparing the CMV seropositive recipients to the general population, it is observed that in some age brackets, there were a higher percentage of transplant recipients documented as seropositive. Unlike the trend for CMV seroprevalence in the population, which gradually rose with increasing age, the rates of seroprevalence for the recipients were high for those patients aged ≤ 15 years and over 50 years. Recipients aged 20 to 29 years documented the lowest CMV seropositive prevalence rates of all the transplant recipients tested, with little over half of the recipients being positive.
In univariate analysis, factors significantly associated with having a previous rejection episode were male sex, recipient age ≤50 years, being diabetic, being diagnosed with cancer at some point and having a positive EBV status. However, having a positive CMV status was not a contributing factor. In multivariate analysis with logistic regression analysis (Table 2), factors independently associated with having a previous rejection episode were CMV seropositivity, age <50 years, having coronary heart disease or hypertension and having a positive antibody status to EBV. The strongest risk factor for rejection was being aged ≤50 years and having hypertension. In univariate analysis, factors significantly associated with death after transplantation were recipient age ≤50 years, being diabetic, being diagnosed with cancer at some point, having cardiovascular disease or having a positive CMV or EBV status. In multivariate logistic regression analysis, factors independently associated with death for this cohort were CMV positive serostatus, aged <50 years, male recipient, being Caucasian, having cardiovascular disease or diabetes and having been diagnosed with cancer at some point.
Multivariate analysis (by logistic regression) of factors associated with renal rejection.
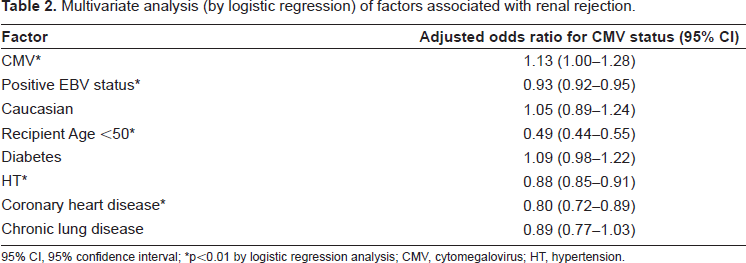
95% CI, 95% confidence interval;
p<0.01 by logistic regression analysis; CMV, cytomegalovirus; HT, hypertension.
CMV disease was the documented cause of death in 72 cases over the last 21 years (1980–2001). Of the deaths, 54% occurred from 1980 to 1989 (39/72), 39% occurred from 1990–1999 (28/72) and only 7% occurred from 2000–2002 (5/72). Out of the recipients who passed away, 84.7% (61/72) had only received one graft and 50% had a functioning graft at time of death (36/72).
Renal Transplant Hospitalizations in Australia
Between 1993 and 2001, 1445 renal recipients were hospitalized with a diagnosis of CMV disease. The average annual rate of CMV admissions for renal recipients was 38.7 episodes per 1000 recipients living with a functioning graft. This rate declined from 69.5 (1995–1996) to 21.5 (2000–2001) episodes per 1000 recipients. Over the eight years, 14,569 bed days (an average of 1821 bed days per year) were recorded for patients diagnosed with CMV. For all patients admitted with CMV disease, the median length of stay was 4 days (range: 1 to 287 days), and 41% of hospitalizations were for 48 hours or less.
Figure 2 shows the number of admissions for CMV disease in transplant recipients versus the number of people living with a functioning graft and the annual intake of new patients in Australia. From the graph, it can identified that both the number of people living with a functioning graft and the number of newly transplanted recipients have been inclining, whereas the number of recipients hospitalized with CMV disease has peaked and then returned to 1993 levels.
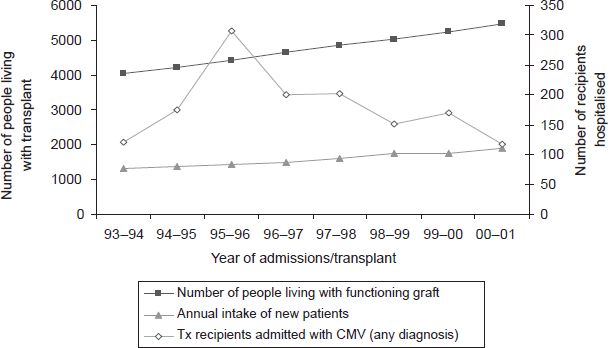
Admissions of CMV, per 100,000 populations, by CMV diagnosis vs. annual intake of new recipients, Australia, 1 July 1993 to 30 June 2001.
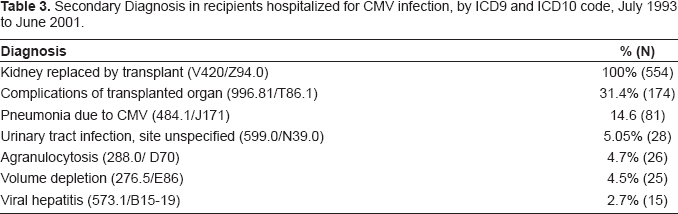
Out of the 1445 admissions, 38% (554/1445) of recipients were hospitalized primarily because of CMV disease (principal diagnosis). The average annual rate of admissions was 14.8 episodes per 1000 people living with a functioning graft. Unlike previous trends, admissions rates (with CMV as the principal cause) were actually increasing again by the end of the eight-year period. The leading secondary diagnoses for patients hospitalized with a principal diagnosis of CMV disease were pneumonia, urinary tract infection, agranulocytosis, and viral hepatitis (Table 3).
Secondary Diagnosis in recipients hospitalized for CMV infection, by ICD9 and ICD10 code, July 1993 to June 2001.
The average age-specific rate of admission was found to the highest for those aged 15–24 years (96.8 cases per 1000 recipients with a functioning graft), followed by those aged 75–84 (42.7 cases per 1000 recipients) and 45–54 years (40.4 cases per 1000 recipients). The lowest average age-specific rate of admission was recorded for 55–64 years (23.3 cases per 1000 recipients). Over the eight years, there were 133 admissions for children/adolescent recipients with a diagnosis of CMV disease. There were no admissions documented in children under the age of 4 years. Over the eight-year period, male transplant recipients accounted for 65% of admissions with CMV disease.
Discussion
This study describes the epidemiology of hospitalisation for CMV disease in kidney transplant recipients in Australia between 1993 and 2001, as well as trends in CMV seroprevalence between 1980 and 2004. Over the decades, the incidence of CMV infection has changed. In the late 1970's, it was estimated that two-thirds of transplant recipients would show evidence of CMV infection and that 30% of these would develop clinical disease [19]. With the introduction of ganciclovir in the late 1980's, the clinical pattern of CMV disease changed. One study, which examined transplant recipients between 1987 and 1995, found that 25% developed CMV disease after kidney or simultaneous kidney-pancreas transplantation and that 60% went on to develop tissue-invasive CMV disease [20].
A previous Australian study [21] on CMV status and its affect on graft loss and patient mortality, examined data on 5507 patients who had received a primary deceased kidney transplant since the beginning of 1995. They found that for graft loss and patient mortality, outcomes in CMV -ve/+ve, +ve/-ve and +ve/+ve donor/recipient combinations were similar. In univariateanalysis, graft loss varied significantly with matching CMV serology (CMV +ve recipients, i.e. inferior survival). In multivariate analysis, no significant effect was found. For patient mortality, among those not given T lymphocyte depleting antibodies (TLDA), there were poorer outcomes in CMV +ve recipients, whereas among those given TLDA there was no difference. The difference in patient mortality suggests that positive CMV IgG in recipient or donor is a risk factor for patient survival among those who not receive TLDA. The recommendations from the study were that strategies to reduce CMV should be considered for all CMV +ve recipients. In our study, we found that CMV serostatus was independently associated, in multivariate analysis with logistic regression analysis, with having a previous rejection episode and with mortality. These findings correlate with the results from the previous study. However, it must be noted, that donor/recipient matching could not be taken into account in these calculations.
This study represents the first attempt to examine rates of hospitalisation for CMV disease in the Australian transplant setting. Previously, Bock et al. [22] performed a retrospective analysis of the incidence, clinical manifestations, and sequelae of CMV disease in a large group of paediatric renal transplant recipients. Using data from the North American Paediatric Renal Transplant Cooperative Study registry (NAPRTCS), the authors screened 2517 renal transplants performed at 51 centres in the United States and Canada. Over a 12-month period, they identified 142 patients hospitalised with CMV infections, the majority of which included major organ involvement. On examination of data, the authors found that in recent years there has been an increase in the incidence of CMV hospitalisation. During the period 1990 through 1992, 7.7% of the contributing centres’ transplanted patients were hospitalised with CMV infections compared with 4.0% during the period 1987 through 1989. No significant trend of recipient age, allograft source, or changing antiviral prophylaxis strategy correlated with this increase. The authors of the study could not account for the increased incidence of CMV hospitalisation; however, they felt that it was unlikely to be the result of changes in diagnostic capability or clinical practice. A second study [23], which examined CMV disease after renal transplantation, used data from the United States Renal Data System (USRD) to observe the rate, risk factors and patient survival associated with adult hospitalisations for CMV diseases. The authors reported that the incidence density of hospitalisation with a primary diagnosis of CMV disease during their entire study was 1.26 events per 100 person years and that the mean length of stay was 8.57 ± 6.56 days (range 1–78 days). However, unlike the first study, they did not report on changes in the incidence over a period. Whereas, they did find that the leading manifestations of infection specified in secondary diagnosis for hospitalised CMV infections were pneumonia, hepatitis, gastrointestinal, agranulocytosis, and urinary tract infection, which was in correlation with what was reported in this chapter.
Risk factors associated with hospitalisation for CMV have also been examined in a number of studies. A previous study [22] found that the risk of CMV hospitalisation was highest among those with a CMV+ donor, regardless of the recipient CMV antibody status prior to transplantation. The risk of CMV hospitalisation was not associated with any identified demographic parameter, including recipient age, race, graft type, use of induction therapy, or dosage of cyclosporine during the first post-transplant month. A second study found that apart from donor CMV seropositivity, prolonged pre-transplant dialysis was the strongest risk factor for hospitalisation for CMV disease. This implied that prolongation of the chronic uremic state might be associated with greater susceptibility to CMV disease. The authors went on to report the following factors as significantly associated with hospitalisation; cadaveric donation, older donor age, recipient age >65, dialysis in the first week post transplant, rejection, maintenance mycophenolate mofetil and CMV serology's [23].
As reported in this study, the mortality from CMV infection and disease was not significantly high in the recipient population studied. Previous studies examining the mortality of recipients hospitalised with CMV disease, found that the all-cause mortality from CMV disease was 13.1% for hospitalised CMV patients compared to 8.7% for other non-infected renal transplant recipients. Whilst the mortality of hospitalised recipients with CMV was significantly higher when compared to other recipients, it was still lower than other hospitalised infections, which have been studied in the same population. For example, in renal transplant recipients hospitalised with fungal infection, the 2 year all-cause mortality was 37.4% vs. 9.6% in all other recipients [24], whilst for renal transplant recipients hospitalised with septicaemia the 2 year all-cause mortality was 24.8% vs. 11.7% in all other recipients [25]. The relatively low risk of mortality in Australia may reflect success in reducing patient mortality using prophylactic and preemptive antiviral therapy. All units in Australian and New Zealand use prophylaxis for CMV -ve recipients of CMV +ve renal transplants, and after T lymphocyte depleting antibodies (TLDA); whilst 10 of 17 units also use it for all CMV +ve recipients.
Conventional wisdom suggests that a successful kidney transplant with a functioning graft is less costly than dialysis [26]. Transplantation may be viewed as an investment to avoid the costs associated with dialysis, which amount to nearly US$70,000 per year [27]. A cost saving from kidney transplantation is achieved about five years after the transplant, when the savings in dialysis costs exceed the initial and ongoing costs associated with the transplant [26]. However, transplant recipients who develop CMV diseases incur further costs associated with hospitalizations, diagnostics and multiple physician visits. In a case-control study of the cost impacts of CMV disease in renal transplant recipients, McCarthy et al. estimated that institutional health care costs were 2.5 times higher in patients with CMV disease than in those without, reflecting a difference in ward and laboratory costs, radiology and pharmacy costs [28]. More recently, studies have confirmed the importance of this infection as a critical cost-driver and risk for hospitalisation [23], [29], and have emphasised the cumulative indirect costs of co-infection and graft loss [27]. These studies have also reported that CMV disease is also associated with increased resource utilization and a longer aggregate length of hospital stay in the first post-transplant year compared to the recipients with no CMV disease (59 vs. 22 days) [30].
The limitations of this study are similar and common to any retrospective study. Findings are associative, not causative. We acknowledge this as a significant and unavoidable shortcoming of the present analysis. The databases examined in this study were the only sources available that would allow assessment of CMV disease in virtually the entire renal transplant population. Until better reporting systems for CMV disease become available, this data is the best that can be obtained. Population-based registries have an important role in nephrology, informing understanding of risk factors, complications and outcomes, clinical care and policies. When addressing infrequent but clinically important events occurring, the advantages of analysing large registries are clearly apparent. Randomised trials, restricted by period and sample size, are not powered to detect differences, and cohort studies from single centres lack sample size to adjust adequately for all potential confounders.
While previous studies have shown that the benefits of renal transplant are clear [31], these data confirm that, despite advances in prophylaxis and improved surgical technique, renal transplant patients still remain at risk of CMV disease. The presence of CMV disease increases the total cost of renal transplantation as well as reduces its effectiveness, thus dramatically diminishing the cost-effectiveness of renal transplants.
Disclosure
The authors report no conflicts of interest.
Footnotes
Acknowledgements
The data reported here have been supplied by the Australia and New Zealand Dialysis and Transplant Registry. The interpretation and reporting of these data are the responsibility of the Authors and in no way should be seen as an official policy or interpretation of the Australia and New Zealand Dialysis and Transplant Registry. The National Center for Immunization Research and Surveillance (NCIRS) funded this study. NCIRS is supported by The Australian Government Department of Health and Ageing, the NSW Department of Health and The Children's Hospital at Westmead.