
Abstract
Plasma HIV-1 RNA concentration, or viral load, is an indication of the magnitude of virus replication and largely correlates with disease progression in an infected person. It is a very useful guide for initiation of therapy and monitoring of response to antiretroviral drugs. Although the majority of patients who are not on antiretroviral therapy (ART) have a high viral load, a small proportion of ART naive patients are known to maintain low levels or even undetectable viral load levels. In this study, we determined the rate of undetectable HIV-1 RNA among ART naive HIV positive patients who presented for treatment at the University College Hospital (UCH), Ibadan, Nigeria from 2005 to 2011. Baseline viral load and CD4 lymphocyte cell counts of 14,662 HIV positive drug naive individuals were determined using the Roche Amplicor version 1.5 and Partec easy count kit, respectively. The detection limits of the viral load assay are 400 copies/mL and 750,000 copies/mL for lower and upper levels, respectively. A total of 1,399 of the 14,662 (9.5%) HIV-1 positive drug naive individuals had undetectable viral load during the study period. In addition, the rate of non-detectable viral load increased over the years. The mean CD4 counts among HIV-1 infected individuals with detectable viral load (266 cells/μL; range = 1 to 2,699 cells/μL) was lower than in patients with undetectable viral load (557 cells/μL; range = 1 to 3,102 cells/μL). About 10% of HIV-1 infected persons in our study population had undetectable viral load using the Roche Amplicor version 1.5.
Keywords
Introduction
HIV-1 viral load refers to the number of copies of HIV-1 RNA in one milliliter of plasma. Unlike the virus in the cell, plasma viral load indicates the magnitude of virus replication and often disease progression.1,2 It is therefore a very useful guide for initiation of therapy and monitoring of response to antiretroviral drugs. 3 Plasma viral load also plays a major role in the transmission of HIV 4 as well as response to treatment.5,6 Studies have also shown that a small proportion of patients who are not on antiretroviral therapy (ART) are known to maintain low or even undetectable viral load levels. These groups of individuals have been described as aviremic or elite controllers.7,8 However a great majority of patients who are not on ART have a high viral load.9,10
Several HIV-1 viral load assays are available with varying detection limits.11,12 The Roche Amplicor version 1.5, which is widely used in resource limited countries, has a lower detection limit of 400 copies/mL and upper limit of 750,000 copies/mL. Therefore, HIV-1 RNA undetectable result does not imply absence or clearance of virus but may be due to the inability of the assay to detect the virus in plasma. This may be because the virus level is lower than the detection limit or that a variation in the virus, and hence a “primer mismatch” has occurred, leading to the inability to detect the virus. 13 The ability of a viral load assay to detect every known and unknown HIV-1 subtype is very important in Nigeria, where diverse HIV-1 subtypes have been reported and new variants still being identified.14–18
Wide use of ART in Nigeria began in 2002 when the Federal Government launched the pilot HIV treatment program for 10,000 adult and 5,000 children in 10 tertiary hospitals in the country, including the University College Hospital (UCH).19,20 Soon after, support for more ART and HIV care became available in the country through the USG funded President's Emergency Plan for AIDS Relief (PEPFAR) program and the Global Funds. Presently, over 500,000 patients are on ART in the country.
In developed countries, viral load along with CD4 count estimation are used to make decisions regarding commencement of ART in HIV infected individuals.3,21 In resource limited countries, the WHO recommends initiation and monitoring of treatment response based only on CD4 counts.10,11 However, the tertiary health institutions providing HIV care and treatment under the Harvard School of Public Health led PEPFAR program in Nigeria use both CD4 and viral load values for initiation and monitoring of response of patients to ART. We hereby present data that show increasing rate of undetectable HIV-1 RNA among ART naive HIV positive patients who presented for treatment at UCH from 2005 to 2011.
Materials and Methods
Study Location
This study was carried out in UCH, Ibadan, Nigeria. UCH is a tertiary hospital with 55 weekly specialty clinics and about 1000 bed spaces. Being a Federal Government of Nigeria supported tertiary health facility, patients are referred to UCH from secondary health facilities and private hospitals, mostly from the southwest and also from other regions of the country.
Study Population
The study subjects included all HIV positive patients who attended the ART clinic in UCH and were pre-assessed for initiation of ART from January 2005 to December 2011. The University of Ibadan/UCH ethical review board approved the study protocol and written informed consent was obtained from every patient attending the clinic. Pre-ART initiation assessment for each subject included baseline viral load, CD4 enumeration, liver/renal function tests, full blood counts (FBC), and physical examination.
Confirmation of HIV Infection
Patients who have been tested and found to be HIV positive are regularly referred from various primary and secondary hospitals, as well stand-alone HCT centers, to the UCH ART clinic for management. HIV infection status of the patients was confirmed by Western Immunoblot (Qualicode HIV-1/2, Immunetics, USA), a qualitative immunoblot assay with a nitrocellulose membrane containing 8 HIV-1 proteins (gp160, gp120, p66, p56, gp41, p36, p24, p17) and a recombinant HIV-2 specific envelope antigen (gp36). Briefly, the nitrocellulose strip containing the HIV-1 and 2 proteins were reacted with 10 μL of serum/plasma specimen and washed to remove unbound antibody. Human immunoglobulin specifically bound to HIV-1 or HIV-2 proteins/antigen is visualized after reaction with goat antihuman immunoglobulin-alkaline phosphatase conjugate and BCIP/NBT substrate. The bands on the test strips are identified by comparing them to the bands on the positive control strip and results interpreted as follows: No band present (HIV-1 and HIV-2 negative), any two or more of the following bands present: p24, gp41, gp120/gp160 (HIV-1 positive), any band pattern not matching the criteria for positive HIV-1 result (indeterminate), HIV-2 band present (HIV-2 positive). Only individuals with positive Western blot results were pre-assessed for ART initiation.
HIV-1 RNA (Viral Load) Determination/ Quantification
Five milliliters of blood was collected from each patient into EDTA tube. Each blood sample was spun immediately after collection at 3500 rpm for 25 minutes and plasma separated into 2 mL cryovial and stored at −80°C until tested.
The Roche Amplicor® HIV-1 version 1.5 was used to quantify plasma HIV-1 RNA from 200 μL of plasma. The procedure of the assay included RNA extraction from 200 μL of plasma, reverse transcription of target RNA to cDNA, PCR amplification of cDNA using specific primers, hybridization of the amplified product to oligonucleotide probe specific to the target region of HIV-1 genome, and detection of probe-bound amplified product by colorimetric determination using an ELISA reader.
The lower and upper detection limits of the assay are 400 copies/mL and 750,000 copies/mL of plasma respectively. Sample with values less than the 400 copies/mL were considered non-detectable while those with values greater than 750,000 copies/mL were titrated, retested, and the actual value was calculated by multiplying with the dilution factor.
CD4 Cell Enumeration
The CD4 easy count kit (Partec GmbH, Munster, Germany) based on the no-lyse no-wash principle was used for CD4+ T-cell enumeration. Twenty microliters of blood collected in EDTA anticoagulant was transferred into a Rhone tube and 20 μL of CD4 monoclonal antibody tagged to PE (CD4 mAb-PE) added and incubated for 15 minute in the dark. Thereafter, 800 μL of no lyse buffer was added and mixed gently and properly. The Rhone tube containing 840 μL of processed blood sample was then analyzed using the Cyflow Counter. The number of CD4+ cells is displayed automatically on the monitor of the counter using the Flow max software as CD4+ T-cells/μL of whole blood.
Results
Data from a total of 13,263 ART naive patients who had baseline HIV viral load were analyzed. Enrollments increased from 2005 to 2007 after which it decreased gradually (Table 1). The mean baseline CD4 lymphocyte count for the 14,662 patients enrolled in the study was 238 cells/μL with a range of 1 to 3102 cells/μL.
HIV RNA was not detected in 1,399 (9.5%) of the 13,263 naive patients included in the study. The proportion of HIV-1 positive patients with undetectable viral load increased over time (Table 1). A mean CD4 count of 266 cell/μL (range = 1 to 2,699 cells/μL) among individuals with detectable viral load was lower than in patients with undetectable viral load (557 cells/μL; range = 1 to 3,102 cells/μL) (
Baseline characteristic of patients.
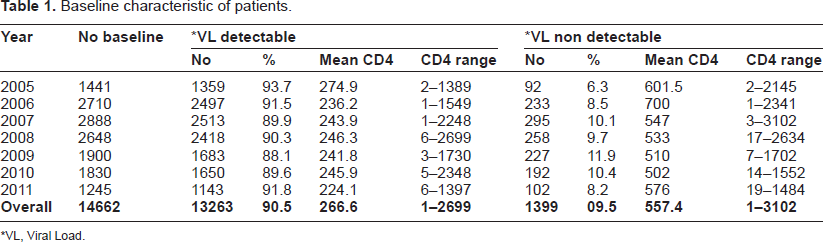
VL, Viral Load.
Stratifications of individuals with detectable and undetectable viral load by CD4 count values are shown in Figure 1. Overall, a large number (62.3%) of patients with detectable viral load had CD4 of less than 250 cells/μL, while most (56.3%) of those with undetectable viral load had CD4 of 500 cells/μL or above. However, 18.7% of individuals with undetectable viral load had CD4 count of less than 250 cells/μL, and about 12% of individuals with detectable viral load had CD4 greater than 500 cells/μL.
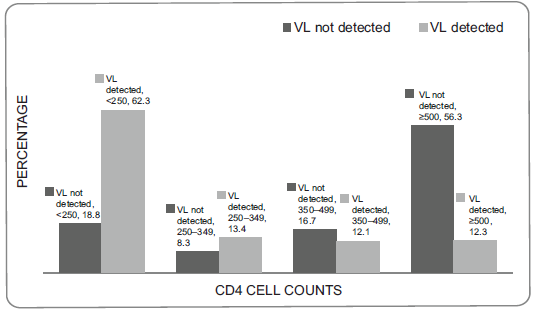
Stratification of CD4 cell count among individuals with detectable and non-detectable viral load (VL).
Discussion
Antiretroviral drugs became widely available Nigeria at little or no cost to HIV positive patients in 2004 through the PEPFAR and Global Fund programs. The number of patients enrolled at the antiretroviral clinics therefore increased as information on the availability of drugs became available to people living with AIDS. This thus explains the increasing rate of patient enrollment reported in this study.
Most HIV positive individuals who are not on ART are known to have high viral load while a few maintain very low or even undetectable levels of viral RNA. The proportion of HIV positive ART naive individuals found in this study is relatively high when compared with reports from other countries.9,22,23 Brun-Vezinet et al 9 reported a lower rate of 2.0% in the Delta trial study. In addition, the proportion of HIV positive individuals with undetectable viral load among drug naive individuals found in this study increased over the years. This may be due to improvement in health seeking behavior among persons living with HIV in Nigeria. It is known that as stigma against HIV positive individuals reduces, there is the tendency for people to know their HIV status earlier and seek medical attention early, unlike during the era of ‘no’ or ‘limited’ ART and high stigma and discrimination in the country. On the other hand, the observed trend may be due to presence and increase in the proportion of variants of HIV-1 that the Roche Amplicor (version 1.5) kit for viral load assay is unable to detect. Studies have shown that variation in the target region of HIV-1 is a major cause of false negative results in PCR based assays due to primer mismatch. 13 This is especially the possibility in a country like Nigeria, where multiple subtypes of the virus have been reported in high proportions and new ones are still being identified.14–18 In a study in China, Wang and colleagues have showed that clade types are most likely to impact on HIV viral load quantification. 24
Some individuals have been described as “elite controllers” because they spontaneously control virus replication without antiretroviral drugs to levels below the limit of detection by commercial assays or with very low level of viremia.7,8 These groups of individuals have not been reported from Nigeria. A follow up study of cohorts of individuals with undetectable viral load in this study, as well as use of more sensitive assays with lower detection limit, may provide more information to determine if these individuals are “elite controllers” or not. In a study on level of viremia in HIV-1 elite controllers, Pereyra et al 13 found PCR mismatch of 11%.
It is interesting to note that the mean viral load of 450,370 copies/mL obtained among the drug naive individuals with detectable viral RNA is higher than values reported from some western countries 1 but similar to report from some other African countries.25,26 This difference may be the result of recurrent infections in HIV infected individuals in Africa, especially malaria and some bacterial infections.27–29
Most (56.3%) of the individuals with undetectable viral RNA had CD4 counts of over 500 cells/μL. Because CD4 cell value is generally inversely related to disease progression,30,31 it is possible that these individuals presented early for care and hence diagnosed of the early stage of the infection. However, 18.8% of this group of individuals had low level of CD4 that qualifies them for ART initiation. The national guideline for commencement of ART in Nigeria during the period covered in this study included a criterion of CD4 less than 250 cell/μL. This initiation criterion was changed, however, to CD4 cells of less than 350 cells/μL in 2012. With the new guideline, over 27% of these individuals will qualify for ART implying that the virus in these individuals are replicating and destroying CD4 cells. However, why the virus is not detectable using the Roche Amplicor 1.5 assay is not clear and requires further investigation. On the other hand, the finding that large number (62.3%) of the individuals with detectable viral load had CD4 cell values of less than 250 cells/μL and that only 12.3% of them had CD4 cell greater than or equal to 500 cells/μL, is similar to previous reports from other African countries.3,32
Conclusion
About 10% of HIV-1 infected persons among our study population had undetectable viral load using the Roche Amplicor version 1.5. Some of these patients also had low CD4 cell count, indicating virus replication in the persons. It is therefore important to carefully study the extent of HIV diversity circulating in different parts of Africa with particular reference to diagnostics, therapy, and vaccine design.
Author Contributions
Conceived and designed the experiments: GNO, DOO. Analyzed the data: GNO, IFA, DOO. Wrote the first draft of the manuscript: GNO. Contributed to the writing of the manuscript: IFA, DOO. Agree with manuscript results and conclusions: GNO, IFA, DOO. Jointly developed the structure and arguments for the paper: GNO, DOO. Made critical revisions and approved final version: DOO. All authors reviewed and approved of the final manuscript.
Funding
The ART program at the University College Hospital is supported by USG PEPFAR program through a Cooperative Agreement (No: 1U2GPS001058) from the Centers for Disease Control and Prevention. The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
Competing Interests
Authors disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgements
We are grateful to all the staff of the ART clinic and Virology laboratory for patient enrolment and laboratory analysis. We thank immensely our patients who participated in the study.