
Abstract
Cancer is associated with hypercoagulopathy and increased risk of thrombosis. This negatively influences patient morbidity and mortality. Cancer is also frequently complicated by the development of venous thromboembolism (VTE). Tumor-derived tissue factor (TF)-bearing microparticles (MPs) are associated with VTE events in malignancy. MPs are small membrane vesicles released from many different cell types by exocytic budding of the plasma membrane in response to cellular activation or apoptosis. MPs may also be involved in clinical diseases through expression of procoagulative phospholipids. The detection of TF-expressing MPs in cancer patients may be clinically useful. In lung and breast cancer patients, MPs induce metastasis and angiogenesis and may be indicators of vascular complications. Additionally, MPs in patients with various types of cancer possess adhesion proteins and bind target cells to promoting cancer progression or metastasis. Overexpression of TF by cancer cells is closely associated with tumor progression, and shedding of TF-expressing MPs by cancer cells correlates with the genetic status of cancer. Consequently, TF-expressing MPs represent important markers to consider in the prevention of and therapy for VTE complications in cancer patients.
Microparticles and Cancer
Many individuals with cancer are also in a hypercoagulable state, and the elevated risk of thrombosis conferred by hyper-coagulativity increases patient morbidity and mortality.1,2 Cancer patients frequently develop venous thromboembolism (VTE).3–8 Various potential predictive biomarkers have been examined for association with VTE in cancer progression. For example, analysis of blood cells can effectively predict the risk of VTE development. 9 Additionally, measurement of D-dimer, prothrombin fragment 1 + 2, and soluble P-selectin levels can accurately predict VTE risk. 10 Recently, microparticle (MP) level has emerged as an accurate marker of VTE risk.11–13
MPs are small membrane vesicles that are released from many cell types by exocytic budding of the plasma membrane in response to cellular activation or apoptosis.14–16 MPs disseminate various bioactive effectors originating from the parent cells. Therefore, MPs can alter vascular functions and may induce biological responses involved in vascular homeostasis.
17
Although most MPs in human blood originate from platelets, MPs are also released from leukocytes, erythrocytes, endothelial cells, smooth muscle cells, and cancer cells (Fig. 1).18–23 MPs have been documented in almost all thrombotic diseases occurring in venous and arterial beds.24–27 Tissue factor (TF)-MPs are related to cancer and exhibit increases in patients with certain cancers such as pancreatic cancer and breast cancer.
23
Origin of microparticles (MPs). MPs disseminate various bioactive effectors originating from the parent cells. Although most MPs in human blood originate from platelets, MPs are also released from leukocytes, erythrocytes, endothelial cells, smooth muscle cells, and cancer cells.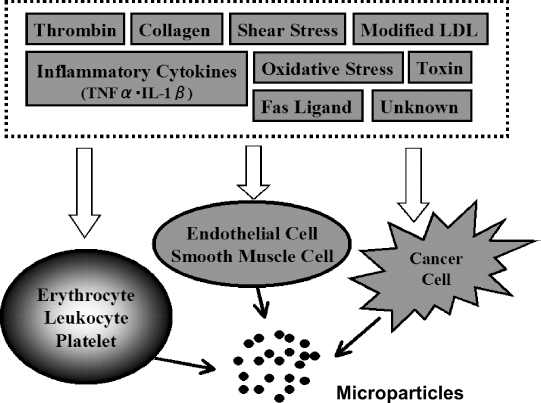
Definition of MPs
MPs can range in size from 0.1 to 1.0 μm.14–16 The membrane composition of MPs reflects the membranous elements of the cell of origin.14–16 MPs contain functional cytoadhesions, bioactive phospholipids, cytoplasmic components, and various antigens that are characteristic of the state of the originating cell and the type of stimulus.28,29 Some studies have analyzed the proteome of MPs and identified hundreds of proteins.30,31 Such proteins may be useful biomarkers for various disease processes. 31
MPs are constitutively released from the surface of cells, and their formation can be upregulated by cellular activation and apoptosis.32,33 Plasma membranes contain various types of phospholipids. Although uncharged phospholipids are mainly present in the outer leaflet of the membrane bilayer, the inner leaflet contains negatively charged aminophospholipids such as phosphatidylserine (PS). During activation or apoptosis of cells, the normal lipid bilayer undergoes an alteration by “flipping” internal PS to the external surface. As a result, PS-exposing MPs may be released from cells. 34
MP Functions
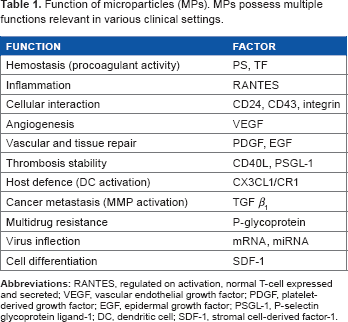
Function of microparticles (MPs). MPs possess multiple functions relevant in various clinical settings.
MPs support coagulation by factor VII/TF-dependent and -independent pathways. 38 During vascular damage, blood contacts extravascular TF, resulting in the activation of extrinsic coagulation and the formation of fibrin. Indeed, TF can become active upon adhesion and fusion of MPs with activated platelets. While TF is exposed by endothelial cell-derived MPs (EDMPs), TF activity is markedly inhibited by MP-associated TF pathway inhibitor (TFPI). In storage-induced PDMPs, 10% of which contain TF, TF-dependent thrombin generation is only observed in plasma with neutralization by TFPI. 39 A balance between TF and TFPI at the MP surface is likely to be crucial for the initiation of blood coagulation, and higher levels of MPs containing TF may overcome the TFPI anticoagulant pathway. 40
Identification of MPs in a Clinical Setting
An identification method for MPs is important for clinical studies. Appropriate sampling conditions, processing, and sample storage are essential. 14 MPs can be directly quantified in platelet-poor plasma obtained by serial centrifugation of citrated whole blood. Alternatively, washed MPs can be isolated from platelet-poor plasma by ultracentrifugation before resuspension and analysis.
The most widely used method for studying MPs is flow cytometry because of its simplicity and the wealth of information that can be obtained from the population of interest. 41 Platelet-poor plasma or MP suspensions are labeled with fluorescently conjugated monoclonal antibodies. The major advantage of flow cytometry is double staining of MPs to determine the origin/cellular source of the MPs. Annexin V binding is used to confirm the phospholipid properties of MPs, although most endothelial MPs do not contain this antigen. Antibodies against specific surface antigens expressed on the cells of origin are used to identify the MP subtype. Flow cytometry also allows the criterion of size to be applied to MP analysis by assessment of the forward light scatter of MPs. Identification of events of a specific size is most accurately performed using calibration beads of a known diameter for comparison.14,16,42 Additionally, a variety of cell-specific antibodies have been applied to MP analyses, and their specificity is likely to influence the results.
Several studies have applied flow cytometry to detect TF-expressing MPs (TF-MPs) in cancer patients.43–45 A recent report showed that the level of TF-MPs measured by functional TF activity in an MP assay correlated with the development of VTE in cancer patients, whereas no correlation was found using flow cytometry to measure TF-MPs. 46 Therefore, further investigations should consider TF-MP analysis by flow cytometry.
Various MPs and Blood Cell-derived MPs in Cancer Patients
Cancer patients possess high levels of circulating procoagulant MPs and an increased risk of thrombosis (Table 1).44,47–52 These procoagulant MPs may originate from various cell types and can be produced by fusion between MPs of different origins.47,52 MPs frequently detected in cancer patients include PDMPs, monocyte-derived MPs (MDMPs), and EDMPs (Fig. 1).53–55 PDMPs promote metastasis and angiogenesis in lung cancer patients and accelerate breast cancer progression by enhancing the invasive potential of cancer cells.53,54 Additionally, PDMPs enhance chemotaxis in response to stromal cell-derived factor-1, leading to cancer progression or metastasis. 55 Collectively, these results suggest that PDMPs may be a useful biomarker of cancer. Consistently, the concentration of circulating PDMPs differs by cancer stage. 56 Kanazawa et al 57 reported that the number of PDMPs and MDMPs in patients with non-small cell lung cancer is significantly higher than those in patients with small cell lung cancer. They concluded that elevated MDMPs are a sign of vascular complication in lung cancer patients, particularly those with non-small cell lung cancer. On the other hand, EDMPs also play an important role in patients with various types of cancer. A pilot study concerning hepatocellular carcinoma showed that the levels of EDMPs in liver transplant patients are altered after surgery and correlated with the clinical outcome. 58 Recently, some reports have suggested that circulating levels of EDMPs are significantly associated with one-year mortality in patients with end-stage non-small cell lung cancer.59,60 Furthermore, Reynés et al 61 reported that EDMPs have a prognostic value in patients with glioblastoma. The exact production mechanism of these blood cell-derived MPs in cancer patients is unknown. However, these MPs may participate in the generation of TF-MPs.
MPs and Multidrug Resistance in Cancer Patients
Multidrug resistance (MDR) is a major obstacle to chemotherapeutic treatment in many cancer patients. 62 Although several mechanisms of MDR acquisition have been identified, the most commonly identified MDR mechanism is overexpression of P-glycoprotein (P-gp).63–64 P-gp is present in cancers and its overexpression is negatively associated with response to chemotherapy.63–65 MPs can transfer MDR between cancer cells by transporting P-gp protein and mRNA in cancer cell-derived MPs (Table 1).66–68 Additionally, inhibitor of apoptosis protein—a negative regulator of cell death—has recently been found to be transported by cancer cell-derived MPs.69,70
Tumor-derived MPs
There is an increasing appreciation for the notion that cancer cells themselves may be a source of procoagulant MPs.71–73 It is highly possible that cancer-derived TF-MPs are a trigger for thrombogenesis in cancer.12,43,44,74,75 The levels of TF-MPs in cancer patients correlate with the activation of coagulation as determined by D-dimer levels. 44 In addition, Tesselaar et al 47 reported a link between TF-MPs and VTE in cancer patients. Furthermore, previous studies have reported a correlation between the levels of TF in pancreatic and brain tumors and VTE.76,77 In particular, cancer-derived TF-MPs might represent a biomarker for poorly differentiated and invasive pancreatic cancer phenotypes as well as poor survival. 78 Therefore, the thrombogenesis in pancreatic cancer, which has one of the highest mortality rates, is a major problem. Wang et al 79 reported interesting experimental results concerning the VTE of pancreatic cancer. They analyzed the expression of TF in four pancreatic cancer-derived cell lines to clarify the mechanism of VTE formation with cancer invasion in vivo. As a result, they found an increase in the expression of TF in two of the four cell lines, and TF-MPs were detected in the culture medium. Moreover, most TF in the culture medium was the TF-combined form. Based on these results, activation of the coagu-latory system through elevation of the thrombin-antithrombin III complex (TAT) suggested a dependence on TF-MPs. It is unknown how TF in tumors activates the coagulating system or participates in thrombogenesis. Wang et al 79 indicated that it is unclear whether TF on the tumor surface and/or soluble TF are directly involved in thrombogenesis. In contrast, cancer-derived TF-MPs appear to participate in triggering thrombogenesis directly and play an important role in the abnormality of the coagulation system in cancer. Consequently, TF-MP is a very important marker in the consideration of prevention or therapy of VTE complication in cancer.13,47,78,80–82
Chemotherapy is known to be associated with an increase in thrombosis.5,83 Cytotoxic chemotherapy agents enhance cellular TF activity and PS exposure, resulting in the release of TF-MPs. 84 An increase in PS expression or the release of PS- or TF-positive MPs has been observed in endothelial and leukemic cells during chemotherapy.85,86 In pancreatic cancer patients, elevated circulating TF antigen levels were found in those receiving gemcitabine chemotherapy, 87 while a detectable rise in plasma TF measured by TF expression levels or MP-associated PCA during chemotherapy was deemed predictive of subsequent VTE events. 51 However, other mechanisms in addition to the increase in the levels of circulating TF-MPs may be involved in thrombosis during chemotherapy, such as the release of nucleic acids and increase in cellular PS exposure.12,52,80
Conclusion
We have summarized the literature to date regarding TF-MPs, highlighting the growing list of cancer types that are associated with elevated MP levels. MPs were initially identified as small particles originating from multiple cell types and possessing PCA. MPs of multiple origins—including cancer cells—may contribute to the increased levels of TF-MPs found in cancer patients, ultimately resulting in cancer-associated coagulopathy (Fig. 2). The PCA of TF-MPs is mediated by expression of TF and the exposure of PS on the MP surface. Adhesion proteins, including CD24 and CD43, have been proposed to be involved in the binding of TF-MPs to target cells.88,89 The utilization of circulating MPs as cancer biomarkers may provide effective and noninvasive methods of cancer diagnosis, prognosis assessment, and disease surveillance to tailor and personalize therapies. However, the functional role played by TF-MPs in cancer patients needs to be understood in greater detail.
Role of TF-MPs in activation of target cells and organs. TF-MPs can carry some substances, such as integrin, cell adhesion molecule, chemokines, phospholipids, and TF. TF mainly contributes to activation of the extrinsic coagulation system.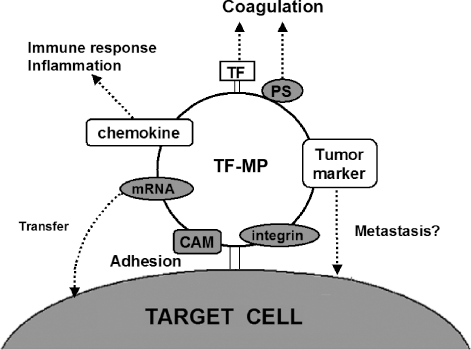
Abbreviations
VTE, venous thromboembolism; MP, microparticle; TF, tissue factor; PS, phosphatidylserine; PDMPs, platelet-derived MPs; PCA, procoagulant activity; EDMPs, endothelial cell-derived MPs; TFPI, TF pathway inhibitor; MDMPs, monocyte-derived MPs; MDR, multidrug resistance; P-gp, P-glycoprotein; TAT, thrombin-antithrombin III complex.
Author Contributions
Conceived and designed the experiments: SN. Analyzed the data: SN and MS. Wrote the first draft of the manuscript: SN and MN. Contributed to the writing of the manuscript: TN and TT. Agreed with manuscript results and conclusion: SN. All the authors reviewed and approved the final manuscript.