
Abstract
Macrophage-colony stimulating factor, matrix metalloproteinase-9, and tissue inhibitor of metalloproteinase-1 may play an important role in malignant processes. The aim of this study was to investigate the diagnostic power of those parameters (serological biomarkers) in comparison to cancer antigen 125 and squamous cell carcinoma antigen in cervical cancer patients and in relation to the control groups. The study included 100 cervical cancer patients, 50 patients with cervical ectropion and 50 healthy women. Plasma levels of tested parameters were determined by enzyme-linked immunosorbent assay, cancer antigen 125, and squamous cell carcinoma antigen by chemiluminescent microparticle immunoassay. Plasma levels of all parameters in the total cancer group showed statistical significance (in all cases p < 0.05). In stage I of cancer only medial supraclavicular fossa and tissue inhibitor of metalloproteinase-1, in stage II all the tested parameters and cancer antigen 125, and in stage III + IV macrophage-colony stimulating factor, matrix metalloproteinase-9, and cancer antigen 125 showed statistical significance when compared to the healthy volunteers group. Macrophage-colony stimulating factor showed the highest value of sensitivity from all tested parameters (I: 56.25%, II: 72.73%, III + IV: 77.14% and 69% in total cervical cancer group). The highest specificity was obtained by matrix metalloproteinase-9 (94%). Positive predictive values were highest also for matrix metalloproteinase-9 (I: 82.35%, II: 84.21%, III + IV: 88% and 94.55% in total cervical cancer group), negative predictive values for macrophage-colony stimulating factor (I: 75.44%, II: 82.69%, III + IV: 87.5% and 58.11% in total cervical cancer group) and tumor markers. In the total cervical cancer group, all tested parameters showed statistically significant areas under receiver operating characteristic curve, but maximum range was obtained for the combination macrophage-colony stimulating factor + squamous cell carcinoma antigen (0.8723). The combined analysis of tested parameters and tumor markers resulted in an increase in sensitivity and areas under receiver operating characteristic curve values, which provides hope for developing new panel of biomarkers that may be used in the diagnosis of cervical cancer in the future.
Keywords
Introduction
Currently, cervical cancer (CC) is the fourth leading cause of cancer death in women worldwide, causing more than 275,000 deaths annually. 1 Treatment of CC is planned depending on the clinical stage of the disease, ranging from surgery alone to a combination of radiation, chemotherapy, and surgery in special situations. The initial screening algorithm of annual cytology proved to be effective in decreasing the incidence of CC.2,3 However, cytology-based cervical screening also has some limitations. The major problem is the low sensitivity of a single smear to detect high-grade precursor lesions (50%–70%), which require frequent testing. 2 In addition, cytology has low reproducibility, leading to variable accuracy. Some researchers have made efforts to individuate cancer markers such as carcino-embryonic antigen (CEA) and squamous cell carcinoma antigen (SCC-Ag). They actually are not used for early diagnosis, but only for evaluation and monitoring of treatments of CC.4,5 Consequently, there is a need for a better primary screening test, and thus a new screening algorithm and furthermore, the survival improvement from early detection of disease relapse has been found.6,7 Early detection of cancer is also important due to risk of premature ovarian failure and infertility. More than 70% of women with a cancer diagnosis are interested in the possibility of having children, which significantly affects their quality of life and psychological well-being. 8
Macrophage-colony stimulating factor (M-CSF) is a hematopoietic growth factor that stimulates the proliferation and differentiation of monocytes to macrophages. In inflammation, M-CSF induces macrophages to secrete cytokines and proteases, thereby enhancing the macrophages’ ability to combat microbial infections. 9 Increased expression of M-CSF and its receptor are correlated with poor prognosis in breast, ovarian, and prostate cancer.10–16 M-CSF has mainly been studied in breast carcinomas where it is commonly expressed.17,18
Several other candidate tumor markers have also been implicated especially these involved in tumor invasion such as matrix metalloproteinases (MMPs). It was demonstrated that MMPs play a critical role in tumor invasion and metastasis due to their proteolytic capacity against basement and extracellular matrix (ECM) proteins.19,20 So far, more than 20 MMPs have been identified, among which, matrix metalloproteinase-9 (MMP-9) expression has been found to be activated or enhanced by oncogenic proteins and elevated in many cancer types, such as breast cancer, prostate cancer, bladder cancer, and pancreatic cancer.21,22 Besides degradation of ECM, MMP-9 also appears to be active in releasing tissue-bound fibroblast growth factor (FGF) and vascular endothelial growth factor (VEGF) from ECM and stimulating neovessel formation. 23
Normal tissue remodeling is a consequence of the dynamic balance between MMPs and tissue inhibitor of metalloproteinases (TIMPs) activities and its disruption may lead to diseases of uncontrolled ECM component formation including cancer.23–25 TIMPs are endogenous inhibitors that bind specifically and inhibit MMPs activation. Four types of TIMPs (TIMPs 1–4) have been identified; these proteins share an analogous structure which fits into the active site of the MMP catalytic domain.26,27 For example, TIMP-1 inhibits MMP-9 with a high affinity. TIMP-1 has been shown to be increased in primary tumor in advanced breast carcinoma and high TIMP-1 levels would therefore be associated with a worse prognosis.26,28
The aim of this study was to determine the plasma levels of M-CSF, MMP-9, TIMP-1, and the commonly accepted tumor markers (cancer antigen 125 (CA 125), SCC-Ag) in CC patients in relation to the group with ectropion and to healthy controls. We compared the plasma levels of the potential tumor markers with the stage of CC. In addition, we defined the diagnostic criteria (sensitivity (SE), specificity (SP), positive predictive value (PPV), and negative predictive value (NPV)) and receiver operating characteristic (ROC) curve for the tested parameters and in combination with both tumor markers. The data obtained in this work may be helpful in the determination of the usefulness of the analyzed parameters (separately and together) in diagnosis of CC.
Material and methods
Human subjects
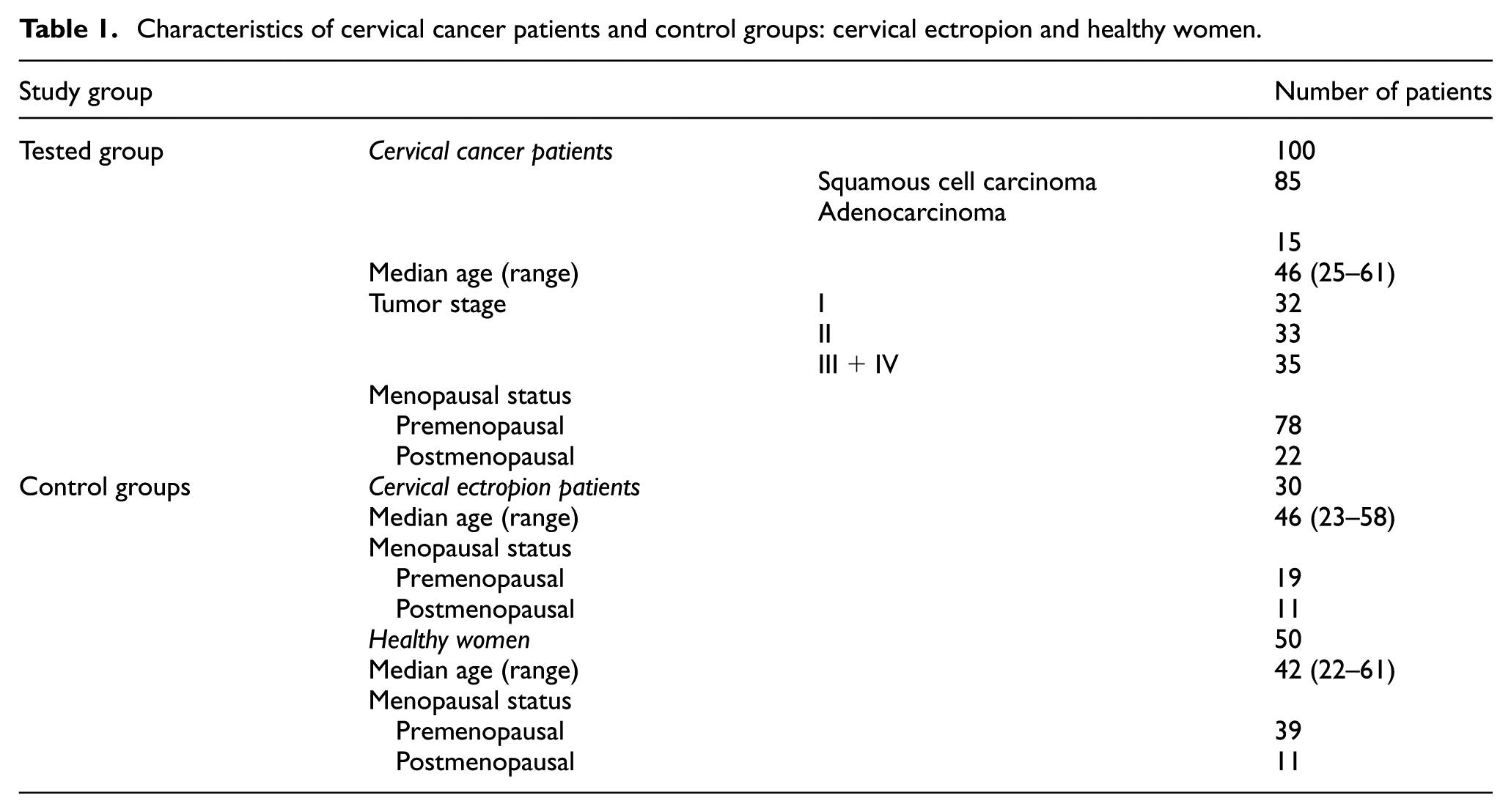
Table 1 shows the tested groups. The study comprised 100 patients with invasive primary carcinoma of the uterine cervix who were referred to the Department of Gynecology, Białystok Medical University Teaching Hospital, Poland, between 2006 and 2012. Clinical stages and histological classification based on the criteria of the International Federation of Gynecology and Obstetrics (FIGO) were established in all cases. Written consent including participants’ own statements regarding their medical history (i.e. data related to reproductive history, personal or family history of cancer, general health issues—hospitalization or surgery, use of medication) and lifestyle habits including smoking were obtained from all the subjects. None of the patients had received chemotherapy or radiotherapy before blood sample collection. Pretreatment staging procedures included physical and blood examinations, ultrasound scanning, and chest X-rays. In addition, computed tomography (CT) scans or magnetic resonance imaging (MRI) were performed when necessary. The control group included 50 healthy, untreated women and 30 women with ectropion lesions. In these women, before blood collection, cervical smear has been examined by gynecologist. They were not referred from other medical centers. All subjects had undergone annual check-ups (laboratory tests, chest X-ray, cervical cytology screening, mammography). The study was approved by the local Ethics Committee (R-I-003/265/06 and R-I-002/239/2014) and all the patients gave their informed consent for participation in the study.
Characteristics of cervical cancer patients and control groups: cervical ectropion and healthy women.
Plasma collection and storage
Venous blood samples were collected from each patient. Blood was collected into a heparin sodium tube, centrifuged 3500 r/min for 20 min to obtain plasma samples, and stored at −85°C until assayed.
Measurements (M-CSF, MMP-9, TIMP-1, CA 125, and SCC-Ag)
The tested parameters (M-CSF, MMP-9, and TIMP-1) were measured with enzyme-linked immunosorbent assay (ELISA) (Quantikine Human M-CSF Immunoassay; R&D Systems Inc., Minneapolis, MN, USA) and commonly used tumor markers were determined by chemiluminescent microparticle immunoassay (CMIA) (CA 125 and SCC-Ag; Abbott, Chicago, IL, USA), according to the manufacturer’s protocols. The intra-assay coefficient of variation (CV) of M-CSF is reported to be 3.4% at a mean concentration of 227 pg/mL, standard deviation (SD) = 7.7; MMP-9 to be 1.9% at a mean concentration of 2.04 ng/mL, SD = 0.039; TIMP-1 to be 3.9% at a mean concentration of 1.27 ng/mL, SD = 0.05; CA 125 to be 2.4% at a mean concentration of 43.5 U/mL, SD = 1.10; SCC-Ag to be 4.3% at a mean concentration of 1.97 ng/mL, SD = 0.085. The inter-assay CV of M-CSF to be 3.1% at a mean concentration of 232 pg/mL, SD = 7.3; MMP-9 to be 7.8% at a mean concentration of 2.35 ng/mL, SD = 0.184; TIMP-1 to be 3.9% at a mean concentration of 1.28 ng/mL, SD = 0.05; CA 125 to be 3.9% at a mean concentration of 43.5 U/mL, SD = 1.7; SCC-Ag to be 5.1% at a mean concentration of 1.97 ng/mL, SD = 0.1. The value of intra- and inter-assay CVs were calculated by the manufacturers and enclosed in the reagent kits. The assay does not exhibit cross-reactivity or interference with numerous human cytokines and other growth factors. Duplicate samples were assessed for each patient.
Statistical analysis
Statistical analysis was performed using STATISTICA 12.0 (StatSoft, Tulsa, OK, USA). The preliminary statistical analysis (using the Shapiro–Wilk test) revealed that the tested parameters and tumor marker levels did not follow normal distribution. Consequently, statistical analysis between all groups was performed using the Mann–Whitney U test, the Kruskal–Wallis test, and a multivariate analysis of various data by the post-hoc Dwass–Steel–Critchlow–Fligner test. Diagnostic SE, SP, PPV, and NPV were calculated using the following cut-off value. The cut-off values were calculated by Youden’s index and for each of the tested parameters was as follows: M-CSF—396.66 ng/mL; MMP-9—316.80 ng/mL; TIMP-1—104.23 pg/mL; CA 125—13.40 U/mL; and SCC-Ag—0.85 ng/mL. We have defined the ROC curve for all the tested parameters and tumor markers. The construction of the ROC curves was performed using GraphRoc program for Windows (Windows, Royal, AR, USA) and the areas under receiver operating characteristic curve (AUC) were calculated to evaluate the diagnostic accuracy and to compare AUC for all tested parameters separately and in combination with commonly used tumor markers (CA 125 and SCC-Ag). Statistically significant differences were defined as comparisons resulting in p < 0.05. In case of analyses of diagnostic performance (SE, SP, PPV, and NPV) and ROC curve, only healthy subjects were used as a control group.
Results
Table 2 shows the plasma levels of tested parameters and tumor markers in patients with CC and in control groups. Plasma levels of all parameters in total cancer group were statistically significantly higher (only in case of TIMP-1 statistically significantly lower) when compared with healthy women group (in all cases p < 0.05). In stage I of cancer only M-CSF and TIMP-1, in stage II all tested parameters and only one of commonly used tumor markers (CA 125), and in stage III + IV two of tested parameters (M-CSF and MMP-9) and CA 125 showed statistical significance when compared to healthy volunteers group (in all cases p < 0.05).
Plasma levels of tested parameters, CA 125 and SCC-Ag in patients with cervical cancer and in control groups.

CA 125: cancer antigen 125; SCC-Ag: squamous cell carcinoma antigen; M-CSF: macrophage-colony stimulating factor; MMP-9: matrix metalloproteinase-9; TIMP-1: tissue inhibitor of metalloproteinase-1; CC: cervical cancer.
Statistically significant when patients with CC compared with healthy women (p < 0.05).
Statistically significant when patients with CC compared with cervical ectropion group (p < 0.05).
Statistically significant when patients with CC stage III or IV compared with patients with CC stage I (p < 0.05).
Statistically significant when patients with CC stage III or IV compared with patients with CC stage II (p < 0.05).
Statistically significant when patients with cervical ectropion compared with healthy women (p < 0.05).
As MMP-9 in all stages of cancer showed statistically significantly higher values (p < 0.05) when compared to ectropion lesions (also TIMP-1 and CA 125, but only in stage III + IV), it gives a possibility to use this parameter in distinguishing between cancer and ectropion cases. In case of SCC-Ag, we can also observe statistically significantly higher values and in case of TIMP-1, we can also observe statistically significantly lower values when compared ectropion lesions to healthy volunteers (in all cases p < 0.05). This demonstrates the chance of using these parameters in differentiation between ectropion lesions and healthy women.
Tables 3 and 4 show the SE, SP, PPV, and NPV of the investigated parameters and tumor markers. We indicated that the SE of all tested parameters in the total cancer group was the highest for M-CSF (69%), but lower than routinely used tumor markers CA 125 (78%) and SCC-Ag (77%). Among all parameters, the highest SE from tested parameters in stages I, II, and III + IV of cancer was observed also for M-CSF (56.25%, 72.73%, 77.14%, respectively), but it was lower than commonly used tumor markers. The diagnostic SP of the tested parameters was the highest for MMP-9 (94%) in total group of CC patients.
Diagnostic criteria of tested parameters, CA 125 and SCC-Ag in patients with cervical cancer.

CA 125: cancer antigen 125; SCC-Ag: squamous cell carcinoma antigen; M-CSF: macrophage-colony stimulating factor; MMP-9: matrix metalloproteinase-9; TIMP-1: tissue inhibitor of metalloproteinase-1; SE: sensitivity; SP: specificity; PPV: positive predictive value; NPV: negative predictive value.
Diagnostic criteria of combined parameters in patients with cervical cancer.

CA 125: cancer antigen 125; SCC-Ag: squamous cell carcinoma antigen; M-CSF: macrophage-colony stimulating factor; MMP-9: matrix metalloproteinase-9; TIMP-1: tissue inhibitor of metalloproteinase-1; SE: sensitivity; SP: specificity; PPV: positive predictive value; NPV: negative predictive value.
The predictive value of a positive test result (PPV) in the total group of CC patients was the highest for MMP-9 (94.55%) from both tested and comparable parameters. Among all the tested parameters, the highest PPVs in stages I, II, and III + IV of cancer were observed also for MMP-9 (82.35%, 84.21%, 88%, respectively).
The predictive value of a negative test result (NPV) in the total group of CC was the highest for M-CSF (58.11%), but slightly lower than CA 125 and SCC-Ag. The highest NPV in stage I of CC was observed for SCC-Ag and M-CSF (82.22% and 75.44%, respectively), in stage II was M-CSF, CA 125, and SCC-Ag (82.69%, 82.93%, 84.09%, respectively), and in stage III + IV was M-CSF and CA 125 (87.5%).
Combined analysis of tested parameters and CA 125 or SCC-Ag resulted in increase of SE and NPV in all cases. The most favorable combination revealed to be M-CSF + SCC-Ag and M-CSF + CA 125 in total group of CC (SE = 91%; SP = 66%; PPV = 84.26%; NPV = 78.57%, both).
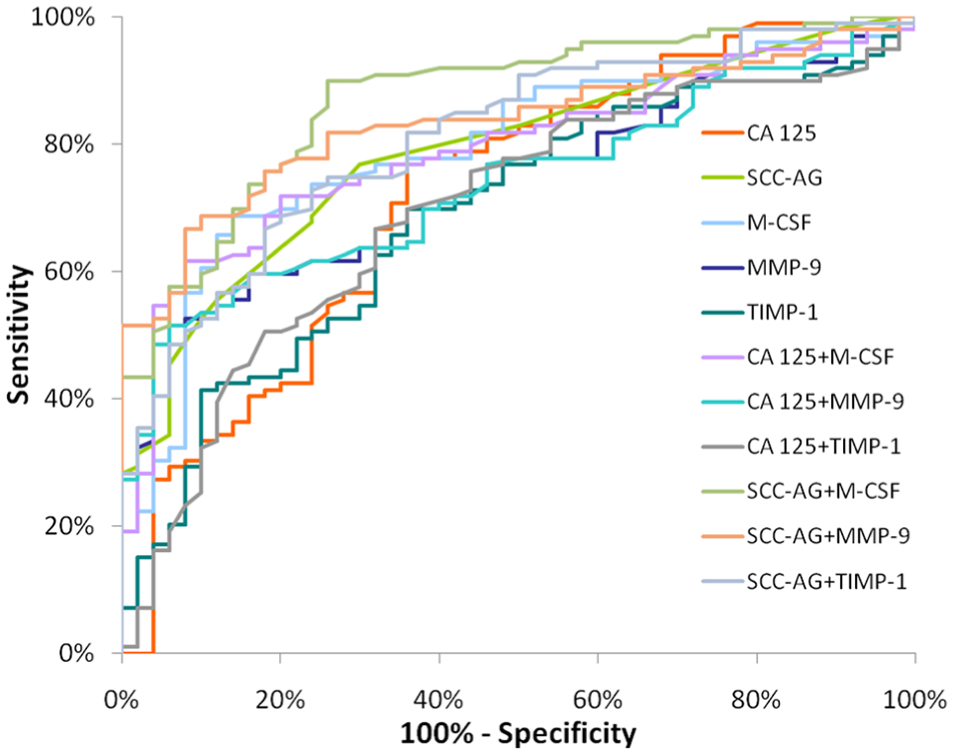
The relationship between the diagnostic SE and SP is illustrated by the ROC curve. The area under the ROC curve (AUC) indicates the clinical usefulness of a selected parameter and its diagnostic power. All data relating to the AUCs in total group of CC are included in Table 5. Graphical versions of the ROC curve for all tested parameters and their combinations with commonly used tumor markers (CA 125 and SCC-Ag) in the whole group of CC are shown in Figure 1. We noted that the M-CSF area under the ROC curve (0.7931) in the total group of CC was highest from all single parameters. Combined analysis of tested parameters and CA 125 or SCC-Ag resulted in increase of AUC in almost all cases. The most favorable combinations in total cancer group revealed to be M-CSF + SCC-Ag (AUC = 0.8723). The AUCs for the tested parameters, similarly as for commonly used tumor markers, were statistically significantly larger in comparison to AUC = 0.5 (borderline of the diagnostic usefulness of the test) (p < 0.05 in all cases).
Diagnostic criteria of ROC curve for tested parameters, CA 125 and SCC-Ag in total stage of CC.

ROC: receiver operating characteristic; CA 125: cancer antigen 125; SCC-Ag: squamous cell carcinoma antigen; CC: cervical cancer; M-CSF: macrophage-colony stimulating factor; MMP-9: matrix metalloproteinase-9; TIMP-1: tissue inhibitor of metalloproteinase-1; AUC: areas under receiver operating characteristic curve; SE: sensitivity.
p statistically significantly larger AUCs compared to AUC = 0.5.
Diagnostic criteria of ROC curve for tested parameters and in combination with commonly used tumor markers in total group of CC.
Discussion
Worldwide, CC is one of the major causes of cancer-related death in women. 29 Cytokines play an important role in tumor–stroma interaction, thus facilitating tumor progression and aggressiveness. Recombinant human M-CSF induces angiogenesis through macrophages by promoting VEGF-A expression. 30 We have previously found increased concentrations of M-CSF in the plasma of patients with endometrial, 31 breast, 32 and ovarian cancer. 33 MMP-9 and its tissue inhibitor (TIMP-1) have been also recently suggested as potential tumor markers of ovarian and breast cancers.34,35
In this particular study, we have investigated the usefulness of M-CSF, MMP-9, and TIMP-1 separately and in combination with CA 125 and SCC-Ag (as a commonly used tumor markers) in CC patients not only in total group of patients but also in differentiation on less and more advanced stages (I, II, and III + IV) and in comparison to two control groups (ectropion patients and healthy subjects).
Our results showed statistically significantly higher concentrations of M-CSF and MMP-9 (as tested parameters) and statistically significantly lower concentrations of TIMP-1 when compared total group of CC patients to healthy subjects. We have found comparable results concerning plasma levels of MMP-9 in the study of Yang et al., 36 but they have compared their results only to healthy subjects and in the paper of Li et al., 29 but they have observed significantly higher expression of MMP-9 in CC tissues. Our previous findings about breast cancer11,17 with use of the same parameters and commonly used in this type of cancer tumor marker also showed that M-CSF, MMP-9, and TIMP-1 have high statistical significance.
Interestingly, low concentrations of TIMP-1 as an inhibitor of MMP-9 indicate a dependence—an increase in metalloproteinase concentration and a decrease in inhibitor concentration, which further confirms the hypothesis that production of TIMP-1 in low (physiological) amounts by healthy cells is unable to inhibit large amounts of produced by cancer cells metalloproteinases, which decomposes type IV collagen and contributes to the degradation of ECM.
In stage I of cancer, we have observed statistical significance only in concentrations of M-CSF and TIMP-1 when compared to healthy subjects. This is consisted with our previous results in other type of cancer. 17 What is very important, none of commonly tumor markers has shown any significance. Our findings are in oppose to those described by Takeda et al. 37 where authors have shown that the levels of SCC-Ag and CA 125 have been shown to be related to the stage of the disease, and that elevated levels of those tumor markers have predictive value for cancer prognosis. Interestingly, another research groups have shown similarly to our findings that serum level of SCC-Ag showed no independent prognostic value in early stages of CC 38 and in other publication, 39 that in only 30% of patients, both of commonly used tumor markers give positive results. Therefore, the search for new candidates as tumor markers, which already at the earliest stage of cancer would show the presence of tumor progression, is so important and still needed.
In stage II of CC all tested parameters and CA 125, and in stage III + IV two of tested parameters (M-CSF and MMP-9) and CA 125 showed statistical significance when compared to healthy volunteers group. What is very important, one of all tested parameters (MMP-9) showed statistically significantly higher concentrations in all stages of cancer, when compared to ectropion lesions. It gives a possibility to use this parameter in distinguishing between cancer and ectropion cases, which is very important during medical diagnosis carried out by oncologist. This contributes to the choice of treatment, both pharmacological and surgical, affecting the quality and length of patients’ survival.
TIMP-1 has also revealed statistically significantly lower concentrations when compared ectropion lesions to healthy volunteers. This demonstrates the chance of using these parameters in differentiation between ectropion lesions and healthy women. It is also very important for both the patient and oncologist, to determine the use of additional (also much more expensive) diagnostic methods (e.g. CT), the need for other studies such as biopsies. Those findings, to our knowledge are the first indicating the utility of this parameters in the differentiation between ectropion lesions and CC or healthy subjects.
SE measures the proportion of positive results that are correctly identified. In all stages of CC, SE values were highest for M-CSF. This is in accordance with our previous work in breast cancer, where M-CSF has also highest results from the same tested parameters. 17
SP measures the proportion of negative results that are correctly identified. In this study, the highest SP for all CC group has MMP-9 (94%). In our previous study concerning CC, MMP-9 has obtained similar results (91.67%). 40 The same results we have obtained in breast cancer (94%). 34
Our results show that MMP-9 has the highest PPVs from all tested parameters in all groups of CC patients. As previously highlighted in our research, the PPV for MMP-9 was also very high. 40
The predictive value of a negative test result (NPV) in the total group of CC was highest for M-CSF, but slightly lower than commonly used tumor markers. The highest NPV in stage I of CC was observed also for SCC-Ag and M-CSF, in stage II of CC was M-CSF and both tumor markers, and in stage III + IV of CC was M-CSF and CA 125. Other researches such as Vasiliades et al. 41 observed lower NPV for M-CSF in pancreatic cancer. We also observed higher NPVs in all stages of cancer for M-CSF.
Combined analysis of tested parameters and CA 125 or SCC-Ag resulted in increase of SE and NPV in all cases. The most favorable combination revealed to be M-CSF + SCC-Ag and M-CSF + CA 125 in total group of CC. To our knowledge, this report is the first to evaluate such a wide statistical analysis with use not only the tested parameters but also combined analysis with CA 125 and SCC-Ag in both CC and other cancers.
The AUC represents the overall accuracy of a test, with a value approaching 1.0 indicating perfect SE and SP. According to this study, the ROC area of M-CSF (0.7931) was the largest of all the tested parameters (even higher than commonly used tumor markers) in the total group of CC. It is with concern to our previous studies in breast cancer, where M-CSF has reached AUC = 0.7955. 17 The most favorable combination in total cancer group revealed to be M-CSF + SCC-Ag (AUC = 0.8723). This report is also the first to evaluate such a statistical analysis with use of combined analysis of tested parameters with CA 125 and SCC-Ag in CC and other cancers. Unfortunately, we could not compare our data with other authors. Most of results are concerning on tissue expression or different evaluations of these parameters.
Conclusion
In summary, to the authors’ knowledge, our report is the first to evaluate the diagnostic usefulness of such an extensive analysis of M-CSF, MMP-9, TIMP-1, CA 125, and SCC-Ag in CC and ectropion patients, not only independently, but especially in combination with both established cervical tumor markers. The results of this study suggest that combining M-CSF + SCC-Ag measurements might enable the improved, early detection of CC when compared with the use of either marker alone.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the local Ethics Committee of the Medical University of Białystok (R-I-003/265/06 and R-I-002/239/2014).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.