
Abstract
For many years, transfusion of allogeneic red blood cells, platelet concentrates, and plasma units has been part of the standard therapeutic arsenal used along the surgical and nonsurgical treatment of patients with malignancies. Although the benefits of these blood products are not a matter of debate in specific pathological conditions associated with life-threatening low blood cell counts or bleeding, increasing clinical evidence is nevertheless suggesting that deliberate transfusion of these blood components may actually lead to negative clinical outcomes by affecting patient's immune defense, stimulating tumor growth, tethering, and dissemination. Rigorous preclinical and clinical studies are needed to dimension the clinical relevance, benefits, and risks of transfusion of blood components in cancer patients and understand the amplitude of problems. There is also a need to consider validating preparation methods of blood components for so far ignored biological markers, such as microparticles and biological response modifiers. Meanwhile, blood component transfusions should be regarded as a personalized medicine, taking into careful consideration the status and specificities of the patient, rather than as a routine hospital procedure.
Keywords
Introduction
While perioperative mortality in complex surgical interventions and, in particular, cancer surgeries has decreased significantly over the last few decades as a result of better surgical techniques and anesthesia, morbidity remains an important challenge.1–3 Blood loss is an inherent risk with long and complicated surgical interventions,4–6 where allogeneic blood transfusions (BTs) are often needed and considered as an indispensable choice in many instances. In fact, of the 15.7 million blood component units transfused in the USA in 2011, 19.8% were for patients undergoing surgical procedures. 7 In the absence of clear guidelines, however, it seems that there is dramatic hospital variability in perioperative transfusion thresholds and rates among patients undergoing major noncardiac surgery at different academic centers. While BT, by improving oxygen delivery and tissue perfusion, can be lifesaving, it can also result in an altered immune response and may lead to transfusion-related acute lung injury or thrombosis and adversely affect the outcome in cancer patients.4,8–10
On the short-term perspective, a large study on 38,926 patients who underwent cancer surgeries demonstrated that intraoperative BT seemed to adversely impact outcomes across all age groups and in those with low-to-normal hematocrit levels. 11 Furthermore, BT has been shown to have a negative impact on the postoperative cancer survival rates, an observation that was repeatedly confirmed for colorectal carcinoma after surgery12–15 and also recognized for other types of cancers.16–19 When the incidence of recurrence of tumors was examined retrospectively in patients who had undergone potentially curative operations for cancer of the colon and after adjustment for other baseline prognostic factors, transfusion alone was found to be significantly associated with a short time to recurrence. Therefore, perioperative transfusion may confer a significant risk factor in the prognosis of cancer of the colon, 20 with the number of units transfused strongly correlating with a poorer outcome. 21
Cancer patients are also often transfused with red blood cell (RBC) concentrates in the context of chemotherapy to keep an acceptable hemoglobin level, and ~15.1% of the blood resources in the USA are allocated to hematology/oncology patients. 7 Therefore, it was noted that transfusion of blood components can possibly be related to worse long-term outcomes in the oncology world.22,23 In general, liberal transfusion triggers for major cancer surgeries are more commonly adopted than restrictive practices. Several randomized controlled trials have looked into minimizing patient exposure to unnecessary transfusions and have advocated for a restrictive red cell transfusion strategy as safe and effective alternative to more liberal transfusion approaches.5,24–29 Patients with restrictive transfusion triggers do not have increased risk for complications when compared to patients transfused liberally. 30
Blood component therapy and particularly platelet transfusions or plasma' which contain multiple blood cell-derived microparticles (MPs; or microvesicles),31,32 are also frequently used in the context of cancer and its related surgeries and are known to negatively affect the outcome of cancer.33–37
In the current review, we will look into the evidence of the risks/benefits of red cell or blood component transfusions in the context of cancer and cancer-related surgeries and the mechanisms through which transfusion may negatively affect the outcome in malignancy.
RBC Transfusion and Cancer
In general, patients undergoing cancer therapy with a curative intent should be transfused similarly to other medical patients, with transfusion for symptoms and consideration of a threshold of 70–80 g/L of hemoglobin in the absence of symptoms. In the absence of randomized trials, small observational studies have shown that transfusion offers symptom relief to patients with advanced cancer.38,39
Colorectal cancer seems to be the prototype that was used by many researchers to investigate the implications of BT on outcome. As early as 1988, Tartter alluded to the possible immunosuppressive effects of perioperative BTs, resulting in an increased incidence of postoperative complications and infections, where of the 134 patients who received RBC transfusions, 33 patients (24.6%) developed infectious complications compared with 9 (4.3%) of the 209 patients who were not transfused (P < 0.0001). 40
Intraoperative red cell BT (RBT) was shown to adversely impact short-term operative cancer surgery outcomes across all age groups and in those with low-to-normal hematocrit levels. 11 The long-term outcome seems poorer with more disease recurrences in patients who received intraoperative transfusions.12–15
Furthermore, in 292 patients undergoing liver resection for colorectal liver metastases, allogeneic RBT was significantly associated with reduced recurrence-free survival (RFS; 32 vs. 72 months; P = 0.008). 41 In another series involving 483 similar patients subjected to resection, 27.5% received RBT. Five-year overall survival (OS) was inferior in red cells transfused patients (45.9% vs. 61.0%; P < 0.0001). Five-year RFS was decreased with RBTs (15.5% vs. 31.6%; P < 0.0001). After adjustment for prognostic factors, BT was independently associated with decreased OS (hazard ratio [HR], 2.24; 95% confidence interval [CI]: 1.60-3.15) and RFS (HR, 1.71; 95% CI: 1.28–2.28). 42 Conversely, a propensity score-based analysis suggested that poor oncological outcomes after curative colon cancer resection in patients receiving perioperative BTs are due to clinical circumstances requiring transfusions rather than being due to the BTs. 43
The negative effect of RBT seems to extend to a large spectrum of malignancies. In esophageal cancer patients, patients with BT experienced significantly shorter OS (univariate HR, 2.50; P = 0.0006) and disease-free survival (DFS; univariate HR, 1.71; P = 0.016) than patients without BT. Similar results were observed in gastric cancer patients (OS: univariate HR, 3.35 and P = 0.0001; and DFS: univariate HR, 3.18 and P < 0.0001). Furthermore, perioperative BT may be an independent prognostic factor in esophageal cancer patients (multivariate HR, 2.07; P = 0.026). Interestingly, age at surgery significantly affected the influence of BT on patient outcome in esophageal cancer patients (P for interaction = 0.022), where the negative effect of BT is particularly evident among younger patients. 44 Dose-response meta-analysis revealed that all-cause mortality was significantly lower in patients with gastric carcinoma transfused with ≤800 mL of blood than those transfused with more (odds ratio [OR], 0.58; 95% CI: 0.37–0.92; P = 0.02; I2 = 54%) in the context of a curative intent surgery. BT was also associated with increased cancer-related mortality (OR, 2.57; P = 0.011) and recurrence (OR, 1.52; P = 0.017) in gastric cancer. 45 In hepatocellular carcinoma, a meta-analysis demonstrated that BT was associated with adverse clinical outcomes for patients undergoing surgery, including increased death, recurrence, and complications. 46
Similar observations with a poor outcome in BT recipients were made in the context of surgeries for urothelial malignancies.47–50 The association between a poor outcome and BT was again documented when Cox regression showed that transfused subjects with advanced ovarian carcinoma had shorter median times to recurrence and mortality after adjusting for age and tumor grade. 51 Furthermore, allogeneic BT given before radiotherapy may be associated with higher incidence of distant metastases and decreased survival in patients with stage IIB cervical cancer, 52 but not for stage Ib. 53 BT of three or more units also might confer a worse prognosis in patients undergoing primary surgery for oral and oropharyngeal squamous cell carcinoma. 54
Similar observations were made in the context of high-grade soft tissue sarcomas of the extremities, where the receipt of BTs is associated with increased tumor recurrence and decreased survival in patients. Five-year OS was also substantially decreased in patients receiving RBT (85% compared to 63%; P = 0.0035). A direct relationship existed between the number of transfusions administered and the decrease in DFS and OS; the larger the number of transfusions, the worse the prognosis (P < 0.0001 and P = 0.0001, respectively). 16
On the other hand, such an association was documented neither in the context of radical prostatic surgery for cancer prostate 55 nor in the context of breast cancer surgery with immediate transverse rectus abdominis flap for breast reconstruction. 56
A very interesting observation was published in 2007 where computerized files from the Scandinavian blood banks were analyzed to identify a cohort of 888,843 cancer-free recipients transfused after 1968. During 5,652,918 person-years of follow-up, 80,990 cancers occurred in the transfusion recipients, corresponding to a standardized risk of 1.45 (95% CI: 1.44–1.46). Therefore, the marked increase in cancer risk shortly after a BT may have reflected the presence of undiagnosed occult cancers with symptoms that necessitated the BT or may have, together with the clinical intervention, negatively influenced the recipients' cancer risks through the transmission of biological response modifiers and/or modulation of the immune system, unmasking the occult cancers. 57
The immunomodulatory effect of BT has been described since few decades and is often referred to as transfusion-induced immune modulation (TRIM). 58 A study of the effect of allogeneic BT on specific immunological functions in mice and human subjects 59 has demonstrated decreases in (a) interleukin 2 secretion, 60 (b) natural killer (NK) cell activity and, hence, lymphokine-activated killer (LAK) cell activity and immune surveillance against malignancy, 61 (c) delayed-type hypersensitivity responses,62,63 (d) CD4/CD8 ratios, 64 and (e) macrophage function. 65 Kirkley postulated that the BT-induced immunomodulatory effect is antigen-specific and/or antigen-nonspecific. 59 Antigen-specific response is mediated by B- and T-cell tolerance to transfused human leucocyte antigen (HLA) antigens. The sharing of HLA between donor and recipient cells persists in the recipient (microchimerism state) and therefore induces a specific tolerance 14 or results from the production of anti-idiotype antibodies 66 or is caused by BT-inducing lymphocyte anergy. Antigen-nonspecific response, on the other hand, is mediated by less discriminated changes of the immune system with decreased macrophage function, lower CD4/CD8 ratios, and altered NK cell activity, 59 all contributing directly or indirectly to a reduced immune surveillance, facilitating malignant cell growth, proliferation, tethering, and dissemination. Leukodepletion of red cells does not seem to affect significantly such changes. 14 Figure 1 illustrates TRIM.
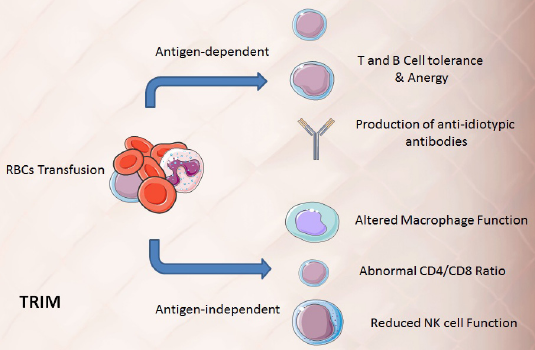
Schematic representation of TRIM; RBC transfusion induces both antigen-dependent T- and B-cell tolerance and enhances the production of anti-idiotypic antibodies, whereas antigen-independent mechanisms involve altered macrophage function, abnormal CD4/CD8 ratios, and reduced NK cell surveillance.
Erythropoietin (EPO) has been a frequently prescribed drug for treatment of cancer-related and chemotherapy-induced anemia in conjunction with iron or autologous transfusion to reduce allogeneic BT need. Paradoxically, recent preclinical and clinical studies indicate that EPO could potentially accelerate tumor growth and jeopardize survival in cancer patients, rendering this approach much less appealing for the correction of anemia in the context of cancer. 67 Therefore, transfusion strategies and thresholds have to be reconsidered with great caution and concerns in patients with known or with potential malignancies particularly if a surgical procedure with curative intent is planned.
Platelet Transfusion and Cancer
Numerical and functional platelet abnormalities have been described in the context of occult and overt malignancy even in the absence of clinically detectable thrombosis.68–71 The interaction between tumors and platelets seems to be bidirectional with tumors activating platelets inviting thrombosis and platelets attracted to tumor sites to fuel their growth and proliferation via their load of growth factors.33–37 The tumor promoter roles of platelet led to the suggestion of an overall benefit of aspirin for a primary prevention of cancer. This was confirmed by population-based data. 72 Furthermore, aspirin was shown to be effective in reducing distant metastasis.71–73 Although there is no randomized data to demonstrate the potential harmful effect of platelet transfusions in cancer patients, one can assume that they will confer a significant risk of disease progression with an increased thrombotic risk attributed to the platelets and their MPs. ASCO set a series of guidelines for platelet transfusion in the context of solid tumors and their related interventions (Table 1). 74
ASCO guidelines for the transfusion of platelets in the context of solid tumors and surgical and invasive procedures in patients with cancer. 74
The postulated mechanisms of interaction between platelets and tumors involve an initial signal by tumor cell-induced platelet activation, activating platelets likely via their P-selectin receptors with the generation of MPs. Platelets attracted to the tumor sites will release their growth factor load of vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and transforming growth factor beta (TGFP), favoring tumor growth and proliferation. Via their P-selectin receptors, platelets will help the intravasation, migration, and extravasation of tumor cells spreading to form distant metastasis.33–37 Activated platelets, and platelet-derived MPs, will also share and mark the first trigger of the thrombotic tendency observed in the context of malignancy. Figure 2 illustrates the interactions between platelets and cancer cells.
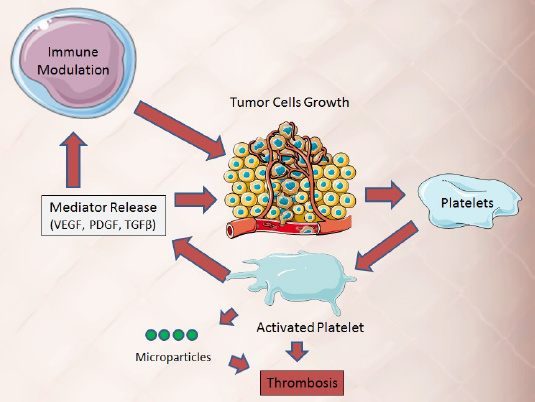
Tumors activate self- and transfused platelets that generate microparticles and mediate the release of growth factors that promote tumor growth and alter the immune response to tumors.
Therefore, it is wise to recommend a great deal of caution when advising for platelet transfusion in the perioperative context of patients with malignancies and in chemotherapy-induced thrombocytopenia pending the availability of prospective and retrospective outcome analysis of cancer patients receiving platelets in the context of their therapy. Thresholds for transfusion should be guided by clinical indications rather than arbitrary numbers.
Fresh Frozen Plasma and Cryoprecipitate Transfusion and Cancer
Fresh plasma and cryoprecipitate are often transfused to patients with cancer in the context of surgeries or to revert warfarin effect or normalize the prothrombin time in anticipation of interventional procedures particularly related to the liver. Plasma, as other blood components, is very rich in MPs, 70–90% of them generated by platelets. 31 MPs are shed from the surface of activated or apoptotic blood cells, and their levels in plasma reflect a balance between cell stimulation, proliferation, and death.37,75 Multiple studies have focused on the role played by coagulation, tissue factor, and platelets and their generated microparticles (PMPs) in the context of cancer, inducing thrombosis.68,76,77 A recent experimental study evidenced that removal of MPs from plasma by a 75-nm nanofiltration step maintains the hemostatic property of plasma proteins but dramatically reduces thrombogenicity. 78 In addition, platelets and their PMPs transfused to patients through plasma can act as tumor promoters.33,37,79 No randomized controlled trials have looked at the evidence of tumor progression or recurrence or shortened survival in plasma transfused cancer patients.
The mechanisms through which plasma delivering their MPs load can affect transfused cancer patients could be direct as they functionally act like liposomes delivering a cargo of growth factors to different tissues primarily aiming at endothelial repair and tissue regeneration.31,75 When released in a tumor microenvironment, mediators will enhance angiogenesis, tumor growth, and metastasis. 34 PMPs' capacity to enhance angiogenesis is mediated through VEGF and tumor-promoting capacity by PDGF, TGFβ-1, and basic fibroblast growth factor that also have proangiogenic activities. 31 VEGF also controls lymphangiogenesis, which is an important contributor to local tumor spread to sentinel nodes. 80 PMPs release their cytokine content in plasma during storage, while some of them may contribute to monocyte cell activation. 81 PMPs may also share through surface receptors in the process of tumor intravasation, migration, and distant seeding. 37
The indirect action played by PMPs on tumor progression is often mediated by their immunomodulatory and inflammatory actions. 31 PMPs polarize resident macrophages toward M2 macrophages. The alternatively activated M2 cells alter the tumor microenvironment and have pro-tumorigenic functions; they suppress NK cells and downregulate T cells and their inflammatory response to tumors.36,82 Figure 3 illustrates the role played by plasma with its MP content in promoting tumor growth.
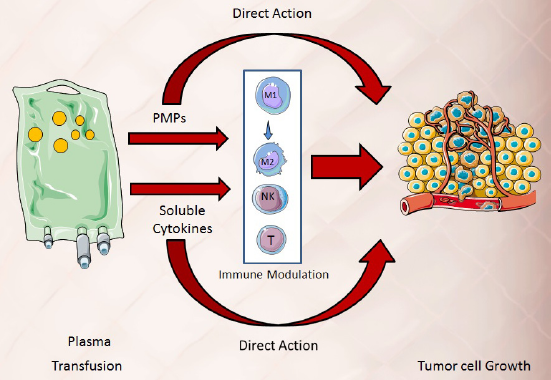
Plasma for transfusion contains PMPs and cytokines that directly or indirectly promote tumor growth.
Furthermore, plasma may contain tumor promoter cytokines released during its preparation, a phenomenon noted in plasma derived from whole blood donation and more pronounced with prolonged storage. Monocyte chemoattractant protein-1 (MCP-1) levels increased with storage time in leukocyte-reduced (LR) blood (P = 0.007) and non-leukocyte-reduced (NLR) blood (P = 0.02). RANTES levels are lower in LR compared to NLR stored blood (P < 0.001), but similar in Day 1 blood, 13.8 ± 1.8 pg/mL in LR vs. 12.0 ± 1.6 pg/mL in NLR. Angiogenin levels were different between LR and NLR blood, 0 pg/mL (undetectable) vs. 44.2 ± 3.7 pg/mL (P < 0.001). Tumor necrosis factor-alpha (TNF-α) level was not different between LR and NLR blood, and there was no storage time effect on concentration. EGF and PDGF levels increased with storage time in NLR blood only. 83
Pro-cancer cytokines and soluble factors as well as MPs may represent possible therapeutic targets to offset the negative effects of plasma transfusion. Despite the absence of clinical studies in humans, evidence of the negative effects of the plasma compartment of stored RBCs was noted in animals 84 and efforts are needed to reduce transfusion requirements and reduced transfusion thresholds in cancer patients.
Fractionated Plasma Products
Not infrequently, patients with malignancies receive industrially processed plasma-derived products, such as albumin, intravenous immunoglobulins (IVIGs), or plasma-derived coagulation factors for replacement. None of the processed protein products, which are free of blood cells and blood cell-derived MPs, seems to affect cancer growth. IVIGs are frequently used to treat immune paraneoplastic diseases, whereas only anecdotal reports allude to a beneficial effect of IVIG in preventing tumor cell migration.85–87
Conclusion
Transfusion is often a needed evil in the surgical and nonsurgical management of cancer patients. A lot of evidence is building up suggesting that red cell, platelet, or plasma transfusion may adversely affect the outcome in patients with cancer, favoring tumor growth, tethering, and dissemination. It is not clear from the published evidence that a specific dose, threshold, or that the leukodepletion of RBT can be recommended, although one can assume that leukodepletion may reduce the risk of TRIM. In the absence of clinical outcome studies and in the presence of significant scientific evidence correlating platelet transfusion and cancer progression, it is important to stick to the minimum current platelet transfusion studies and avoid any unnecessary transfusions.
Large retrospective data analysis and well-designed prospective studies are needed to highlight the amplitude of the problems. Preclinical and clinical research is also needed to control the content and type of MPs and biological response modifiers present in transfused blood components, to check their specific physiological impacts in cancer patients and potentially introduce new quality parameters or manufacturing processes. In the meantime, transfusions should be considered with great caution in such a population. Large bodies should reconsider transfusion thresholds, provide guidelines, and look into safe potential transfusion alternatives.
Author Contributions
Wrote the first draft of the manuscript: HAG. Contributed to the writing of the manuscript: TB. Jointly developed the structure and arguments for the paper: HAG and TB. Made critical revisions and approved the final version: ME-E, JS, MR, and ME. All the authors reviewed and approved the final manuscript.