
Abstract
The body's main fuel sources are fats, carbohydrates (glucose), proteins, and ketone bodies. It is well known that an important hallmark of cancer cells is the overconsumption of glucose. Positron emission tomography (PET) imaging using the glucose analog 18F-fluorodeoxyglucose (18F-FDG) has been a powerful cancer diagnostic tool for many decades. Apart from surgery, chemotherapy and radiotherapy represent the two main domains for cancer therapy, targeting tumor proliferation, cell division, and DNA replication–-all processes that require a large amount of energy. Currently, in vivo clinical imaging of metabolism is performed almost exclusively using PET radiotracers that assess oxygen consumption and mechanisms of energy substrate consumption. This paper reviews the utility of PET imaging biomarkers for the detection of cancer proliferation, vascularization, metabolism, treatment response, and follow-up after radiation therapy, chemotherapy, and chemotherapy-related side effects.
Introduction
Tumor cells consume glucose to produce energy at a much higher level than normal cells and show a remarkable plasticity to evolve, driving their aggressiveness in glucose consumption. Tumor cells transform glucose to pyruvate, then to lactic acid using the anaerobic mode, with or without the presence of oxygen within the cell (Warburg effect). 1 Most cancer cells typically exhibit mitochondrial dysfunction, and this failure will be reflected by an abnormally high level of reactive oxygen species (ROS). 2 The chemical superoxide radical (·O2_), lipid peroxidation, and other molecules that interact with oxygen in the healthy cells are normally regulated during oxidative phosphorylation; however, this is not the case in the tumor cells where the mitochondria are dysregulated. 3 It is commonly believed that the high glucose consumption by tumor cells is used to supply energy, produce complex molecules dedicated to cell division and proliferation, and finally to protect the cell against oxidative stress induced by ROS using the pentose phosphate pathway, which generates nicotinamide adenine dinucleotide phosphate-oxidase (NADPH) to reduce oxidative damage. 4
In oncology, diagnostic imaging tools could be used effectively to characterize key indicators, such as the vascularization and metabolic index of aggressiveness of a specific cancer. Positron emission tomography (PET) imaging could also provide information on the perfusion and energy metabolism of the tumor, while the PET metabolism biomarkers could contribute to cancer detection, treatment response assessment, and follow-up of remission.5,6 This technology has the potential to be used in guiding a personalized treatment plan, providing more effective therapy and reducing tumor recurrences, which in turn may decrease the burden on the already strained healthcare system. Canada will have to deal with close to 200,000 new cancer diagnoses per year and 25% of the Canadian population will die from cancer. 7 Imaging of tumor metabolism could lead to improved knowledge of the basic biologic mechanisms in oncology and generate novel approaches and treatments to fight against these high rates of cancer.
PET Imaging
Unlike magnetic resonance imaging (MRI) or X-ray computed tomography (CT), PET requires the intravenous injection of a radiotracer: a radioactive atom (radioisotope) attached to a molecular probe targeting a specific metabolic pathway in the human body. During its decay, the radioisotope will release a positron that annihilates with a nearby electron, causing the emission of two 511 keV photons in opposite directions. The photons create a line of coincidence recorded by the detectors of the PET camera. These coincidence counts are used in a tomographic reconstruction algorithm to generate quantitative PET images of isotope concentration (Bq/mL). Also, unlike MRI or CT, PET images are always molecular and provide few details about the anatomy. That is why PET-CT is the current standard for hybrid imaging in which the PET technology is used to assess perfusion or metabolism and CT is used to derive anatomical landmarks to aid interpretation. However, it is important to mention that even if the PET-CT is the current standard, there is an increasing use of MRI to help localize the PET radiotracers in the body. 8
PET perfusion and metabolism imaging is commonly performed using the following radioisotopes: carbon-11, fluorine-18, nitrogen-13, oxygen-15, and rubidium-82. 9 Fluorine-18 is the principal isotope source used. Its half-life is close to two hours, meaning that it has an ideal imaging window of one to three hours postinjection. All of these radioisotopes can be incorporated into an energy substrate that is part of the metabolic pathway and is consumed by cells. However, there are two different categories of radiotracers: the first one (eg, 15 O-water) follows and mimics native body compounds, while the second one (eg, the glucose analog 18 F-FDG) closely mimics the native compounds but becomes trapped in the cells after one or two metabolic transformations by the cell enzymes.
Radiotracer uptake assessment is commonly performed using a semiquantitative metric: the standard uptake value (SUV), which accounts for the weight of the subject and the injected tracer activity. The SUV (g/mL) will be generally assessed using static images at a point in time between the injection of a radiotracer into the blood and when the bio-distribution is deemed optimal. Comparatively, PET kinetic analysis is the study of the radiotracer behavior over time within the living organism. Kinetic analysis generally requires knowledge of the input function (the course of the radiotracer in the blood over time) and of the response of the target organ or area to the radiotracer. Those two components (input and target) will drive the interpretation of the biologic mechanisms occurring in the target, allowing the description of perfusion, metabolism, and anaplerotic processes within the cell. In this paper, we review the ability of PET and targeted tracers to detect the tumor vascularization, as well as energy metabolism, important factors in characterizing cancer (Fig. 1), and describe the mechanisms of the radiotracers available for cancer detection, assessment of tumor treatment response, and evaluation of therapy-related adverse effects.
Schematic of the uptake mechanisms of the principal PET radiotracers targeting tumors used for the assessment of blood flow (MBF;
15
O-water,
13
N-ammonia, 82Rubidium,
11
C-acetate), metabolism (
18
F-FDG,
11
C-glucose,
18
F-FTHA,
11
C-palmitate,
11
C-acetate,
18
F-FGln, and
11
C-acetoacetate), and key markers (
18
F-FAZA,
18
F-FLT,
18
F-FET,
18
F-FCh, and
11
C-choline). Fluorodeoxyglucose (FDG), glucose transporters (GLUT), 18-fluorodeoxyglucose-6-phosphate (
18
F-FDG-6-P), monocarboxylate transporter (MCT), 14(R, S)-fluoro-6-thia-heptadecanoic acid (FTHA), fatty acid transport protein (FATP), fluoroglutamine (FGln), fluorothyminide (FLT), fluoroehtyltyrosine (FET), fluoromethylcholine (FCh), choline transporter (ChT), l-amino acid transporter 1 (LAT1), acetyl-coA synthetase short-chain family member 2 (ASCT2), fluoroazomycin arabinoside (FAZA).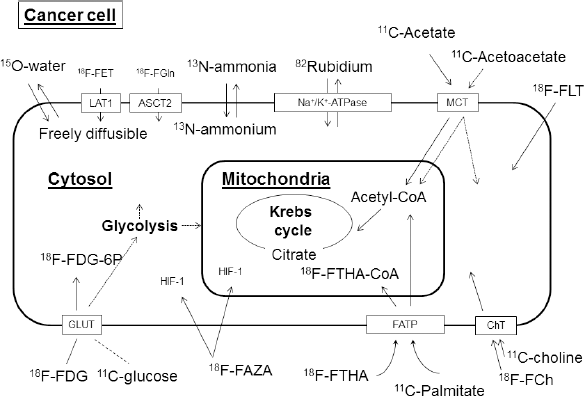
PET Perfusion and Tumor Blood Flow
An ideal tumor blood flow radiotracer will be able to diffuse freely throughout the vascular system and across tumor cell membranes. It will possess high first-pass extraction from the blood into the cell, where it should be retained, and, afterward, it will be rapidly and completely cleared from the blood to permit high-contrast visualization of the tumor uptake. Intravenous PET radiotracers available are 15 O-water, 13 N-ammonia, and 82Rb-chloride; all possess a number of these aforementioned properties.10–14 In brain, kidney, and pulmonary tumors, blood flow has been used primarily to discriminate between nonneoplastic and neoplastic lesions and to grade the aggressiveness of the tumor focus. For example, a focal lesion showing hypometabolism with 18 F-FDG PET could be further defined using a radiotracer to evaluate blood flow, such as those mentioned previously. 12 During cancer treatment, chemotherapy can be targeted to damage the microvascular system of the tumor, an effect that can be assessed by measuring tumor blood flow. 14 After radiation therapy, radiation necrosis could be misinterpreted as recurrence; therefore, measuring vascularization could provide an index of the treatment response. Evaluation of the vascularization and energy metabolism could increase the accuracy of the diagnosis. In summary, tumor blood flow could be used in the initial diagnosis, assessment of treatment response, or follow-up evaluation.
PET Metabolic Biomarker and Cell Metabolism
To understand tumor behavior and oncology treatments (radiotherapy and chemotherapy), we will do a brief overview of the cell metabolism. There is storage of adenosine triphosphate (ATP) in the cell, and this energy reserve is available at two levels: first for subsistence–-meeting primary and structural needs (survival)–-and second, when those subsistence needs are filled, for normal cell operations that are, for tumor cells, division and proliferation.15,16 Tumor cell energy metabolism seems to be different from that of normal cells, and this could be reflected in the consumption of a number of energy substrates. The human body constantly requires energy substrates, with the principal energy sources being fatty acids, glucose, ketone bodies, lactate, pyruvate, and amino acids. In a normal cell, this energy will be provided from beta-oxidation of the fatty acids and pyruvate, from glycolysis and then through oxidative phosphorylation to generate ATP (Fig. 2). Tumor cells, however, rely excessively on anaerobic glycolysis to produce ATP.
16
Schematic of the main interactions of glucose fatty acid oxidation. The FFA enters the cell through FATP 1 and 6, is converted to FFA-CoA in the cytosol, then it moves to the mitochondria through CPT I and II and acylcarnitine translocase. Inside the mitochondria, the acyl-CoA is transformed into acetyl-CoA to enter the Krebs cycle. Glucose enters the cell through the GLUT transporters and is converted to glucose-6-phosphate (glucose-6-P) in the cytosol. Glucose-6-P is converted to pyruvate and enters the mitochondria. Pyruvate is transformed into acetyl-CoA to enter the Krebs cycle. The glucose fatty acid oxidation cycle is the predominant regulator of the consumption of energetic substrates in the cell. Drug key enzymes (dichloroacetate, metformine, statins, and 2-tetradecylglycidic acid) could be used to favor an investigated pathway of energy metabolism.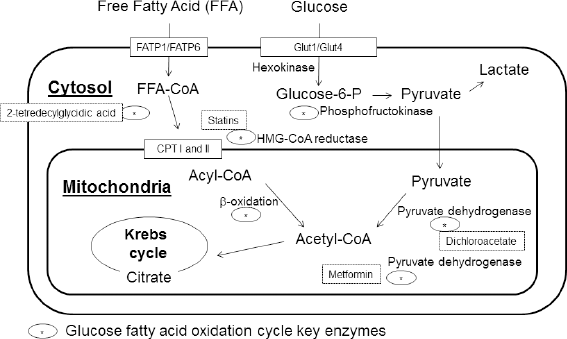
Glucose metabolism
Through glycolysis, glucose is converted to glucose-6-phosphate, then to pyruvate. Pyruvate is converted into acetyl-CoA in the mitochondria for glucose oxidation through the Krebs cycle, under aerobic conditions, to generate energy. Glucose oxidation is favored in the normal cell, whereas lactate instead of pyruvate is produced under aerobic or anaerobic conditions in the tumor cell (Warburg effect). 1 The enzyme phosphofructokinase-1 (PFK-1) is an important glycolytic factor; it is the first irreversible step and the tumor cell activates the complex PFK-1 enzyme by modulating the level of 6-phosphofructo-2-kinase/fructose 2,6-bisphosphatase to upregulate this pathway.4,17 It is noteworthy that many other factors will regulate the glycolytic pathway in both situations and will influence glucose consumption, including insulin, insulin-like growth factor, glucagon, and several other hormones. Hence, it is important to understand pathways and metabolism using in vivo imaging tools. 9
Primarily, the glucose analog 18 F-FDG and to a lesser degree 11 C-glucose are the most commonly used PET tracers to assess glucose metabolism. 18 F-FDG will cross the cell membrane in the same way as glucose and is metabolized through hexokinases for phosphorylation into 18 F-FDG-6-phosphate. When 18 F-FDG is phosphorylated, it is trapped and the next enzyme is not able to metabolize it; thus, the glucose analog remains within the cell. Therefore, 18 F-FDG reflects the uptake of glucose within the cell. 18
The accumulation regions are well defined, and for imaging applications in oncology, it is possible to use the semi-quantitative SUV values to interpret the images and aid in the diagnosis of tumor malignancy.
18 F-FDG PET-CT represents the quasi-totality of the PET clinical applications in oncology. It is used for initial staging of the disease as well as to assess the malignancy of the lesion foci, lymph node involvement, or presence of metastasis. After the initial diagnosis, 18 F-FDG can be used for response evaluation, restaging after treatment, and follow-up to detect cancer recurrence. 19 Because of this versatility, 18 F-FDG assessment of glucose metabolism finds applications in many cancer types. Notably, 18 F-FDG is at the front line of investigation and follow-up for lung as well as head and neck cancer, while for cervical, ovarian, and breast cancer as well as melanoma, it is used to assess node involvement and metastasis for improved initial staging. 20 Also, in pancreatic cancer, 18 F-FDG guides the decision when choosing between a curative and a palliative approach, whereas, in colorectal cancer, it is used to improve the diagnosis when the initial staging is uncertain. Finally, in lymphoma diagnosis, 18 F-FDG improves initial staging when compared to other conventional imaging modalities. Indeed, 18 F-FDG is known to upstage nearly one-third of cases initially assessed by other conventional methods. 21
The high prevalence of 18 F-FDG in oncology PET imaging is explained by near-ideal radiotracer qualities: the avidity of cancer cells for glucose, its high retention within the cells during the imaging period and its rapid subsequent elimination from the body (within ~1 day). All of these make it a reliable and robust tool in oncologic imaging. However, 18 F-FDG is not without flaws: false-negative and false-positive findings can occur. For example, 18 F-FDG uptake is important in granulocytes and mononuclear cells of the immune system during infectious or inflammatory processes because of high energy demands. 22 Radiation therapy will also cause an uptake of 18 F-FDG in the treatment region. 23 On the other hand, tumors with low metabolic rates, such as the mucinous adenocarcinomas, or weak glucose avidity, such as some prostate cancers, can be associated with equivocal or negative scans.24,25 Also, it is impossible to discriminate between the glucose oxidative pathway and anaerobic consumption when using 18 F-FDG because it is not metabolized beyond phosphorylation. 11 C-glucose could be used as an alternative to follow the anaerobic and oxidative pathways, but PET imaging only detects the presence of radioactivity and not the type of carrier; therefore, it cannot differentiate between the native radiotracer and its metabolites. 26 One way to distinguish pathways is to use a drug inhibiting the activation of a specific path, such as dichloroacetate, an inhibitor of the pyruvate dehydrogenase kinase. 27 Dichloroacetate will reduce lactate production driving the system to use glucose oxidation. Inhibitory drugs could be useful in providing an index of aggressiveness of the tumor, but a clinical research application could be a major challenge.
Fatty acid metabolism
The transport rate of free fatty acids (FFA) in the brain, heart, and tumor is different and usually linked to the FFA concentration in the blood. FFA in the blood will diffuse freely or use facilitated transport through the fatty acid transporters FATP1 and FATP6 to enter the cell. FFA within the cell will be oxidized through the Krebs cycle to generate ATP. However, tumor mitochondria failure produces an excess of ROS within the cell and the consumption is reduced as compared to normal cells for this energy production pathway.28,29 FFA within the cell could form tri-glycerides, sterols, or be transported into the mitochondria for energy. The complex carnitine palmitoyltransferase I and II (CPT I–II) will transport fatty Acyl-CoA from the cytosol into the mitochondria and β-oxidation will generate acetyl-CoA for the Krebs cycle to produce energy. In the cytosol, acetyl-CoA carboxylase (ACC) inhibitors will convert acetyl-CoA to malonyl-CoA, slowing down the complex CPT activity to transport the FFA in the mitochondria. FFA oxidative metabolism is the major pathway of energy production in the normal cell, whereas the tumor cell will favor glucose energy production and FFA phospholipids and sterols production. Fatty acid synthesis is increased in tumor cells in response to the demands of cell proliferation and survival. 11 C-choline or 18 F-fluoromethylcholine has been used extensively in prostate cancer and, to a lesser degree, in brain 30 and lung 31 cancer investigation. 32 In prostate cancer diagnosis, choline circumvents some limitations of 18 F-FDG, which are attributed to slow tumor progression and difficulty evaluating the pelvic region due to high bladder activity caused by renal excretion. Choline is a component of the lipid membrane; therefore, uptake of the radiotracer is an index of cell proliferation and division. Low choline uptake in normal cells is also exploited for the imaging of brain tumors where, once again, high 18 F-FDG uptake in normal tissues produces a very high and nonspecific background. 30 Choline PET radio-tracers have been shown to improve clinical diagnosis in a small specific cohort of patients: those who presented with high Gleason scores (8–10) and prostate-specific antigen (PSA) >20 ng/mL at initial staging and with double initial PSA levels (>1 ng/mL) at restaging within 3–6 months, combined to an initial staging of positive nodes. 33
On the other hand, 11 C-acetate, an oxidative metabolism marker, seems to be the radiotracer of choice to assess fatty acid consumption.32,34,35 Oxidative metabolism has been intensively studied with 11 C-acetate, and washout of the radiotracer is an index of the Krebs cycle activity. This small molecule is transported into the normal cell through the monocarboxylate transporter (MCT) and then into the mitochondria to generate energy. 36 In the tumor cell, fatty acid metabolism is different and will be favored for synthesis of lipid membranes or signaling molecules instead of energy metabolism. Acetate within the cell is converted to acetyl-CoA by the acetyl-CoA synthase (ACeS) present in the cytosol and mitochondria in response to the metabolic needs. Fatty acid synthase, a key enzyme used in oxidative metabolism and fatty acid synthesis pathways, can be monitored using 11 C-acetate PET. 37 11 C-acetate has been used clinically for diagnosis of prostate, renal, brain, and hepatocellular tumors and treatment response assessment in cases where 18 F-FDG showed previously mentioned limitations. Even though radiotracers using 11 C are limited to PET centers with on-site cyclotron facilities and this specific tracer is known for its low tumor to normal tissue ratio, it has an undeniable potential for cancer diagnosis improvement. 37 Furthermore, 11 C-acetate could have a dual function: it could act primarily as a metabolic tracer and secondarily as an index of blood flow, making it a very interesting bifunctional marker. The first-pass extraction of 11 C-acetate in the cells is good and methods have been used to assess myocardial blood flow, but further investigation is needed to clearly establish this radiotracer as a reliable index of tumor blood flow. 38
The fatty acid analog 14-(R, S)- 18 F-fluoro-6-thiaheptadecanoic acid ( 18 F-FTHA) is another radiotracer to assess fatty acid metabolism. Similar to 18 F-FDG, 18 F-FTHA is trapped after a few steps: it remains inside the mitochondria after initial β-oxidation.39,40 18 F-FTHA is blocked by sulfur addition, and we are not able to distinguish between β-oxidation and esterification. 18 F-FTHA has the potential to be used in the investigation of tumor fatty acid metabolism, but 11 C-palmitate may be preferable because, like 11 C-glucose in glucose metabolism, 11 C-palmitate will follow the entire pathways of FFA. However, tumor analysis has not yet been performed with this radiotracer. 41 Again, to discriminate between metabolic pathways, an inhibitory drug, such as 2-tetradecylglycidic acid, can be used. This drug blocks the CPT complex pathway, giving a better evaluation of the esterification process.
Glucose and fatty acid oxidative energy production is controlled by hormones, enzyme inhibition or activation, and reversible enzyme phosphorylation (Randle cycle). 42 Malonyl-CoA, phosphofructokinase (PFK), ACC, citrate, and AMP-activated protein kinase are key enzymes in this mechanism and further investigation of energy metabolism imaging is needed. In the tumor, FFA oxidation is reduced and, in return, glucose anaerobic consumption is increased. Therefore, fatty acid synthase-activated fatty acid synthesis and energy metabolism analyses could provide important information to aid initial diagnosis or follow-up on treatment response. 43
Ketone body metabolism
The normal cell will use ketone bodies in proportion to their concentration in the blood. Under normal conditions, the amount of ketone bodies in the blood is low and they contribute very little to energy production. During intense and prolonged exercise, fasting, or fever, the levels of ketone bodies in the blood can increase substantially, increasing cell metabolism involvement.44–46 Normal cells will consume FFA and ketone bodies (eg, acetoacetate and beta-hydroxybutyrate) to efficiently generate energy, whereas, in tumor cells, energy production using these substrates will be of limited amount and efficiency.
Ketone bodies use the MCTs to enter the cell. Beta-hydroxybutyrate and acetoacetate within the cell can be transformed into acetoacetyl-CoA through acetoacetyl-CoA synthetase (cytosol) or succinyl-CoA 3-oxoacid CoA transferase (mitochondria) and be driven, respectively, into lipogenesis or the Krebs cycle for energy production. 46 Some types of brain tumors, such as the glioblastoma multiform, will moderately consume ketone bodies and this presence as an energetic substrate will slow down cell progression.47–50 On the other hand, ketone bodies in normal cells could be used in lipogenesis, mitochondrial and cell membrane damage repair or as energy, and could even protect against ROS. 51
11 C-acetoacetate is an emerging radiotracer designed to investigate the ketone bodies pathway. It has been studied in the heart, in the aging or diseased brain, and in oncology.45,46,52 Uptake in xenograft prostate cancer cells has been demonstrated in the mouse. Also, similar to 11 C-acetate, this ketone body is not excreted by kidneys, which eliminates the normal background associated with the bladder. 52 In another study, 11 C-acetoacetate has shown different uptake and washout patterns in subjects suffering from early-stage heart failure, secondary to doxorubicin toxicity, as compared to controls.46 11C-acetoacetate washout from cells has the potential to estimate energy production or anabolic production. This radiotracer could be helpful in identifying adaptive cell metabolism related to the energy substrate available. As take-home message: normal and cancerous cells differ in their energy metabolism; therefore, modification of the energy substrate through increased levels of ketone bodies could lead to a successful treatment that could in turn be followed using PET metabolism biomarkers.
Cell metabolic imaging may be used to assess the interactions between glucose and FFA metabolism or other substrate interactions. All of the aforementioned radiotracers have the potential to reveal the energy metabolism of cells. Oncology treatments and cardiac toxicity alter metabolism and cell integrity. Further investigation is required to develop early detection methods and to improve management of the treatment response or chemotherapy-related side effects.
Amino acid metabolism
Tumor cells show increased levels of protein synthesis for survival, replication, and invasion. There are 20 primary amino acids required for protein synthesis and nearly half of those are derived from food. The high metabolic activity of tumors increases both nutrient demand and amino acid transporter expression, making it a very attractive pathway to exploit. Most amino acids have been radiolabeled and can be used to assess the expression of their respective transporters by PET. For example, 11 C-methionine and 11 C-tyrosine have shown uptake in brain tumors.5,53 There is also good potential for 18 F-fluoroethyltyrosine ( 18 F-FET) and 18 F-dihydroxyphenylalanine ( 18 F-DOPA), two radiotracers targeting the large amino transporter (LAT1).5,8 LAT1 is associated with poor prognosis and is overexpressed in several cancers such as astrocytoma as well as renal, pancreatic, and lung carcinomas. 18 F-FET is accurate for glioblastoma staging or as an index of tumor treatment response. 18 F-fluorocyclobutanecarboxylic acid (FACBC), a radiotracer used in prostate cancer, is also transported through the LAT1 as well as by the ASC amino acid transporter 2 (ASCT2), which is primarily involved in the transport of glutamine. 54 As for 18 F-fluoroglutamine ( 18 F-FGln) and 18 F-fluoropropyl-glutamine ( 18 F-FPGln), they are designed to image glutaminolysis.5,55
Nucleoside metabolism
Cell division and DNA replication are hallmarks of cancer cells. Cell proliferation can be imaged using radiolabeled versions of the nucleoside thymidine. The first radiotracer used for this purpose was 11 C-thymidine, followed by 18 F-fluorothymidine ( 18 F-FLT).56 18F-FLT, like 18 F-FDG, will be monophosphorylated by kinases and trapped within cells, but, unlike 18 F-FDG, it will not accumulate in inflammatory foci. 18 F-FLT correlates with Ki-67, an index of proliferation, and has proved useful in the staging of lung, breast, and colon cancers, as well as lymphoma. 18 F-FLT uptake remains lower than that of 18 F-FDG and should not be used for disease staging, but rather as an index of tumor treatment response. This assessment of tumor response has been evaluated in breast and lung cancer patients. 57
Radiotherapy Treatment
Radiotherapy treatment (RT) is based on DNA damage inflicted to the tumor cell in order to induce cellular death. RT is usually fractionated to target the fast-proliferating tumor cells as opposed to the slow-proliferating normal cells, allowing more time for DNA repair and better survival of normal cells. It is observed that tumor foci having higher glucose consumption are more resistant to radiation damage. 47 There are two main categories of factors responsible for radioresistance: environmental factors (growth factors, hypoxia, and lactate) and intrinsic factors (antiapoptotic factors, proliferation, and invasiveness). Hypoxic tumor foci and glucose consumption can be assessed by PET tumor blood flow and glucose consumption. Furthermore, this analysis can be combined with a hypoxia marker, for example, 18 F-fluoroazomycin arabinoside ( 18 F-FAZA), which provides an index of the radiore-sistance or the tumor response to treatment.58,59
Chemotherapy Treatment
Apart from surgery, chemotherapy and radiotherapy are the main types of cancer treatment. Chemotherapy is cytotoxic and targets cells with fast division rates. Inhibition of DNA replication with alkylating agents, antimetabolites, and anti-microtubule agents, inhibitors of the transcription system, or inhibitors of cell division are all targets of chemotherapeutic agents.60–62 Briefly, chemotherapy treatments will use different mechanisms on tumor cells, and this will be reflected in their toxicity on healthy cells.
Anthracyclines, such as doxorubicin or epirubicin, are widely used in cancer treatment for the therapy of solid tumors such as breast, ovarian, and lung cancer, as well as leukemia and lymphoma.63,64 In tumor cells, doxorubicin affects the activity of the topoisomerase II and the DNA replication, resulting in inhibition of mitotic activity, which leads to cell death. Doxorubicin and/or epirubicin are the components of many chemotherapy regimens, but their cumulative dose can significantly increase the risk of toxicity. Doxorubicin has been associated with cardiotoxicity in acute, subacute, chronic, and late phases of treatment. However, the mechanisms of this toxicity are not entirely elucidated. Basically, doxorubicin induces morphologic changes in the cardiac cells, including damage to myofibrils, morphologic changes in the sarcoplasmic reticulum and lysosomes–-all leading to heart failure. Doxorubicin and its byproducts induce damage through ROS generation: superoxide radical (·O2–), hydroxyl radical (·OH–), and hydrogen peroxide (H2O2).65–68
Alkylating agents, for example, cyclophosphamide or ifosfamide, are commonly part of chemotherapy regimens such as R-CHOP (cyclophosphamide, doxorubicin, vincristine, rituximab, and prednisolone) used to treat large B-cell lymphoma. Metabolites of alkylating agents interacting with DNA and RNA will inhibit DNA synthesis. 69 In a fashion similar to that of anthracycline-related cardiotoxicity, they can damage the mitochondrial membrane and impair oxidative phosphorylation by oxidative stress.66,69
Some chemotherapeutic agents have the same mechanisms of action in healthy cells and cancer cells, for example, antimicrotubule agents, such as docetaxel, used for adjuvant therapy in breast cancer. Docetaxel stops cell division through microtubule dysfunction by promoting polymerization of tubulin and inhibiting its depolymerization.70,71 Antibody-based treatments and small tyrosine kinase inhibitors primarily target growth factor receptors by competing with ATP and inhibiting the kinase enzyme activity.72,73 The monoclonal antibody-based tyrosine kinase inhibitor, trastuzumab, used in breast cancer targets the overexpression of the human epidermal growth factor receptor 2. 74 Sunitinib, a tyrosine kinase inhibitor, targets nonspecific tyrosine kinase receptors, including vascular endothelial growth factor receptor (VEGFR) and platelet-derived growth factor receptors (PDGFR).75,76 Basically, this emerging kinase-based therapeutic approach targets the epidermal growth factor, the PDGF, and the VEGF. Tyrosine kinase inhibitors are emerging chemotherapeutic agents and have arisen as a result of increased understanding of tumor biology and its mechanisms of progression.
All chemotherapeutic agents have limiting cumulative doses depending on their side effects because their action is cytotoxic, poisoning the tumor to induce cell death. PET tumor blood flow and metabolism biomarkers could drive the development of personalized cancer therapy and help manage the treatment, increasing efficiency and decreasing recurrence.
Chemotherapy-related Side Effects
The major issue shared by all chemotherapeutic agents is the occurrence of side effects. Here, we will make a small incursion into the field of cardiotoxicity and discuss the imaging biomarkers in cancer.65,77–79 Heart failure, ischemia, and vascular problems, such as endothelial dysfunction, represent the major side effects of chemotherapy. The anthracycline family, proteasome inhibitors, antimicrotubule agents, alkylating agents, and tyrosine kinase inhibitors will indirectly affect the heart. Hypertension, endothelial damage, and apoptosis will induce cardiomyopathy, most commonly congestive heart failure. Heart failure is defined as structural or functional impairment that affects the heart contractile function.
When the heart is unable to meet its blood pumping requirements, it will try to adapt by a process of structural remodeling that generally leads to an enlarged ventricular cavity. Heart failure is also associated with hormonal adaptation, ie, elevated norepinephrine levels, that increase the heart rate and contractility in an attempt to improve cardiac output, as well as with an increase in blood pressure via activation of the renin-angiotensin system.66,80 Hypertension increases the afterload on the heart and contributes to its enlargement through increased intraventricular pressure. Progression of heart failure is associated with cardiac remodeling and altered efficiency of oxygen consumption that could be investigated with the aforementioned imaging biomarkers.
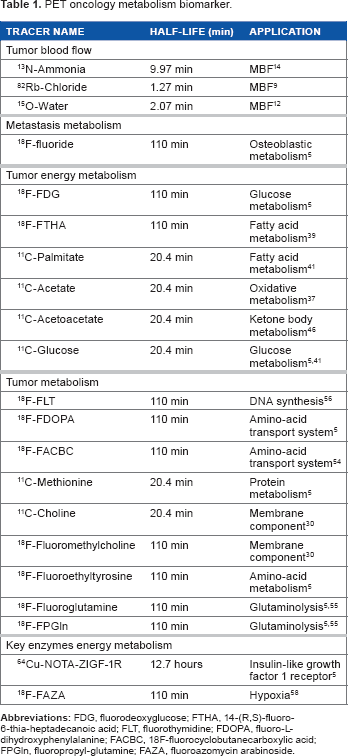
PET oncology metabolism biomarker.
PET Oncology: Blood Flow and Metabolism Biomarkers Perspective
In summary, PET imaging has enormous potential to become a major player in the next generation of cardio-oncologic investigations, mainly via assessment of tumor blood flow and metabolism. These markers can help characterize tumor cells and allow early evaluation of the cancer treatment cardiotoxicity. Precinical animal model experiment (vivo or ex vivo) using drugs to inhibit energy metabolism pathways in order to control the environment, all of these strategies could improve the energy metabolism index analysis. PET imaging is directly translatable to humans using the same radio-tracers to assess tumor blood flow and energy metabolism as used in preclinical development studies. For example, a mouse model of breast cancer could be treated with chemotherapy and the cardiotoxicity of the agent could be evaluated prior to human use. Another example would be RT assessment in a mouse brain tumor model for perfusion and energy metabolism. Tumor cells and toxic effects of chemotherapeutic agents, such as ROS production associated with oxidative stress, could be tracked with 11 C-acetate. 11 C-acetate could also be used to identify mitochondrial failure and cardiotoxicity. 18 F-FDG can be used in conjunction with a pyruvate dehydrogenase kinase (PDH) inhibitor to assess tumor and cardiac metabolism by measuring glycolytic activity. Fatty acid tracers ( 18 F-FTHA and 11 C-palmitate) can be used with statins to evaluate esterification and β-oxidation effects. Finally, the ketone body 11 C-acetoacetate could be used to assess anabolism in oxidative cell damage associated with esterification and mitochondrial membrane repair. 11 C-acetoacetate has the potential to be used in diagnosis and treatment response evaluation as well as detection of early-stage heart failure.
Chemotherapy-related cardiotoxicity, especially if associated with alkylating agents such as cyclophosphamide and ifosfamide that induce primary injury to the endothelium, should be screened using PET myocardial blood flow reserve assessment.
Conclusion
There are a number of positron-emitting radiotracers available for use as imaging biomarkers to investigate tumor vascularization, energy metabolism, and toxic effects of chemotherapy. Each of them may have a specific role to play with respect to the wide-ranging mechanisms used to induce metabolic changes or toxic effects. Further investigation is required to assess PET cancer metabolism biomarkers in order to develop appropriate clinical assessments.
Author Contributions
Conceived and designed the experiments: EC, RAdK. Analyzed the data: EC, RAdK. Wrote the first draft of the manuscript: EC. Contributed to the writing of the manuscript: EC, JMR, MAR, RAdK. Agree with manuscript results and conclusions: EC, JMR, MAR, TDR, FB, RAdK. Jointly developed the structure and arguments for the paper: EC, JMR, MAR, RAdK. Made critical revisions and approved final version: EC, JMR, MAR, TDR, FB, RAdK. All authors reviewed and approved of the final manuscript.