
Abstract
With the improvement of cancer therapy, survival related to malignancy has improved, but the prevalence of long-term cardiotoxicity has also increased. Cancer therapies with known cardiac toxicity include anthracyclines, biologic agents (trastuzumab), and multikinase inhibitors (sunitinib). The most frequent presentation of cardiac toxicity is dilated cardiomyopathy associated with poorest prognosis. Monitoring of cardiac toxicity is commonly performed by assessment of left ventricular (LV) ejection fraction, which requires a significant amount of myocardial damage to allow detection of cardiac toxicity. Accordingly, this creates the impetus to search for more sensitive and reproducible biomarkers of cardiac toxicity after cancer therapy. Different biomarkers have been proposed to that end, the most studied ones included troponin release resulting from cardiomyocyte damage and natriuretic peptides reflecting elevation in LV filling pressure and wall stress. Increase in the levels of troponin and natriuretic peptides have been correlated with cumulative dose of anthracycline and the degree of LV dysfunction. Troponin is recognized as a highly efficient predictor of early and chronic cardiac toxicity, but there remains some debate regarding the clinical usefulness of the measurement of natriuretic peptides because of divergent results. Preliminary data are available for other biomarkers targeting inflammation, endothelial dysfunction, myocardial ischemia, and neuregulin-1. The purpose of this article is to review the available data to determine the role of biomarkers in decreasing the risk of cardiac toxicity after cancer therapy.
Introduction
With new drugs and more aggressive protocols for the treatment of cancer, survival of patients with malignancy has improved but the prevalence of long-term cardiac effects of those therapies has also increased. The cardiac side effects of these drugs have been shown to affect the quality of life and overall survival, regardless of the prognosis related to the cancer. In fact, the risk of cardiovascular death can become higher than the risk of tumor recurrence. 1 Cancer therapies with known cardiac toxicity include anthracyclines, biologic agents such as trastuzumab, and multikinase inhibitors such as sunitinib. Cardiac toxicity can result in different clinical manifestations including arrhythmias, myocardial ischemia, hypertension, acute heart failure (HF), and late-onset ventricular dysfunction with reduced (dilated cardiomyopathy) or preserved ejection fraction. 2 Among these presentations, dilated cardiomyopathy presents the poorest prognosis, especially if refractory to conventional HF therapy, with a two-year mortality of 60%. 3
Detection and monitoring of cardiac toxicity are currently performed by the assessment of left ventricular ejection fraction (LVEF) using echocardiography, radionuclide ventriculography, or magnetic resonance imaging at the beginning of cancer therapy, once half of the cumulative dose has been administered, before every subsequent dose, and 3, 6, and 12 months after completion. 4 Because a significant amount of myocardial damage is needed to result in a decrease of LVEF, the detection of cardiac toxicity can be delayed, leading to irreversible cardiac damage, late introduction of HF therapy, and suboptimal recovery. Accordingly, complete cardiac recovery is achieved in only 42% of patients with cardiac toxicity, despite optimal HF therapy. 5
Interobserver variability of LVEF measurement also limits early detection of cardiac damage. This contributes to the impetus to find more sensitive and reproducible biomarkers of cardiac toxicity during and after cancer therapy. Different biomarkers have been proposed to that end, the most studied ones included troponin release resulting from cardiomyocyte damage and natriuretic peptides reflecting elevation in left ventricular (LV) filling pressure and wall stress. Other biomarkers targeting inflammation (high-sensitivity C-reactive protein
[hs-CRP], interleukin-6, myeloperoxidase, and total anti-oxidant status), endothelial dysfunction (plasminogen activator inhibitor [PAI], tissue-type plasminogen activator [t-PA], and soluble intercellular adhesion molecule-1 [ICAM-1]), myocardial ischemia (fatty acid binding protein [FABP] and glycogen phosphorylase BB [GPBB]), and neuregulin-1 (NRG-1) have been studied. The purpose of this article is to review the available data and discuss the role of biomarkers in decreasing the risk of cardiac toxicity after cancer therapy.
Incidence of Cardiac Toxicity after Cancer Therapy
Different classifications of cardiac toxicity have been proposed. The first classification focuses on pathophysiology and distinguishes irreversible myocardial injury, caused by damage to the microstructure of cardiac myocytes leading to cell death via necrosis or apoptosis (type 1), from reversible cardiac myocyte dysfunction without microstructural damage (type 2). 6 The second approach is temporal and categorizes cardiac toxicity as acute or subacute when it appears within two weeks of completion of chemotherapy (this less-frequent presentation includes arrhythmias, acute coronary syndrome, acute HF, pericarditis, and myocarditis) and as chronic beyond that time point, which can be further subdivided into early or late presentation (the latter is more than one year after treatment has ended) and manifests as asymptomatic systolic and/or diastolic dysfunction or symptomatic congestive HF. 7
Anthracyclines, such as doxorubicin and epirubicin, are chemotherapeutic agents frequently used for the treatment of breast cancer and hematologic neoplasms. The main mechanisms leading to the efficacy of anthracycline are related to DNA damage inducing rapid death of dividing cancer cells, and the cardiac toxicity is induced by free radical formation caused by its metabolism. 8 In a recent meta-analysis, 6% of patients receiving the anthracycline doxorubicin presented with clinically relevant cardiotoxicity and 18% had subclinical cardiotoxicity. 9 Cardiac toxicity induced by anthracyclines is dose dependent, with an increased risk and severity of cardiomyopathy with higher doses. The risk of cardiac toxicity begins at a dose of 200 mg/m2 doxorubicin and radically increases at doses more than 550 mg/m2. 10 Indeed, cardiac toxicity was observed in 3%–5% of patients having received doxorubicin at 400 mg/m2 and in 18%–48% of those at a dose of 700 mg/m2. 11 Moreover, anthracyclines have a synergistic effect with radiation and trastuzumab in terms of cardiac toxicity. 12
Trastuzumab is an inhibitor of the HER2 receptor and is used for the treatment of breast and gastric cancers. The mechanism of cardiac toxicity is not completely understood, but it is probably directly related to HER2 blockade. 13 There are two different patterns of cardiac toxicities associated with this agent, depending on concomitant (or absence of) administration of anthracycline therapy. In patients treated exclusively with trastuzumab, cardiac toxicity is not dose dependent and is reversible (type 2) with HF therapy and discontinuation of cancer treatment. After adequate myocyte recovery, rechallenge is generally well tolerated. 14 In contrast, in patients treated with an anthracycline concomitantly or within 90 days, cardiac toxicity and symptomatic HF can occur in 28% 15 and 27% of patients, respectively. 16 The risk of cardiac toxicity decreases with longer time intervals between both therapies, with an incidence rate of 4.3% when the interval is more than 90 days. 17
Sunitinib is a tyrosine kinase inhibitor used for the treatment of renal cell carcinoma, and cardiac toxicity is probably caused by mitochondrial injury and cardiomyocyte apoptosis. 18 The reported incidence of cardiac toxicity with this agent has ranged from 4.1% to 33.8%.18–20 Cardiac toxicity that is reversible with HF therapy (type 2) has most often been described with sunitinib. 20
Biomarkers Associated with Cardiac Toxicity
There are potentially important benefits of using biomarkers to unmask cardiac toxicity related to cancer therapy.7,21,22 The first one is the possibility to identify patients at high risk of developing cardiac toxicity, to use targeted preventive pharmacologic strategies only in those selected patients, and to avoid exposing others to unnecessary side effects. 23 Also, compared with the use of LVEF measurement, early detection of cardiac toxicity with biomarkers can lead to the initiation of prompt HF treatment with higher likelihood of complete recovery.
Marker of myocardial damage: cardiac troponins
Biomarker of myocardial damage: cardiac troponins.
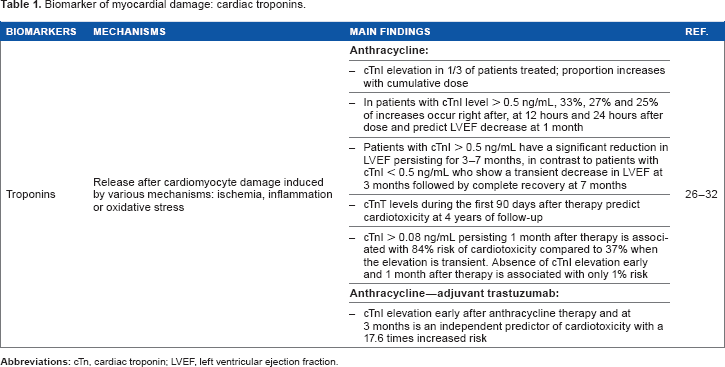
cTnI elevation is present in one-third of patients treated for hematologic or breast cancer with a high-dose anthracycline and is associated with the degree of LV dysfunction.26,27 The proportion of patients with cTnI elevation has also been shown to increase with the cumulative dose of anthracycline. 28 In patients with cTnI levels above 0.5 ng/mL, 33%, 27%, and 25% of increases occur, respectively, right after, at 12 hours, and 24 hours after anthracycline administration, and these were predictive of LVEF decrease at 1 month. 29 Interestingly, in a cohort of 204 patients, there was a significantly different pattern of LVEF changes according to cTnI levels, with patients reaching values above 0.5 ng/mL showing significant and persistent reductions in LVEF, whereas others (those with cTnI less than 0.5 ng/mL) presented a transient decrease in LVEF at 3 months and complete recovery at 7 months. Of note, elevations in cTnI occurred soon (within 12 hours) after the termination of anthracycline administration in 53% of patients. Also, all patients with significant cardiac toxicity and decrease in LVEF more than 30% had a cTnI elevation >0.5 ng/mL. 28 Based on these data, measurement of troponin in the first 24 hours after anthracycline dose is highly efficient to predict early chronic cardiac toxicity, leading to LV dysfunction between 1 and 7 months of follow-up. Moreover, elevation of cTn has also been shown to predict late chronic cardiac toxicity. cTnT levels measured in children with acute lymphoblastic leukemia during the first 90 days after anthra-cycline have indeed been shown to predict the development of cardiac toxicity at 4 years of follow-up. 30
Even if early elevation of cTn after anthracycline is predictive of chronic cardiac toxicity, the pattern of this elevation can add prognostic information. In a cohort of 703 patients, a persistent cTnI elevation (>0.08 ng/mL) 1 month after cessation of anthracycline was associated with a greater incidence of cardiac events compared with transiently high levels (84% versus 37%) during a mean follow-up of 20 months. On the other hand, absence of detectable cTnI level early and one month after anthracycline was associated with a low risk of cardiac events (1%), suggesting that long-term follow-up of these patients may not be necessary. 26 Also, in patients treated with anthracycline followed by trastuzumab for breast cancer, elevations of cTnI measured at the completion of therapy and their persistence at 3 months were independent predictors of future cardiotoxicity.27,31 Elevation of cTnI during administration of trastuzumab has also been demonstrated to be associated with a 17.6 times increased risk of cardiotoxicity. 32
Marker of elevated LV pressure: natriuretic peptides
Biomarker of elevated left ventricular pressure: natriuretic peptides.
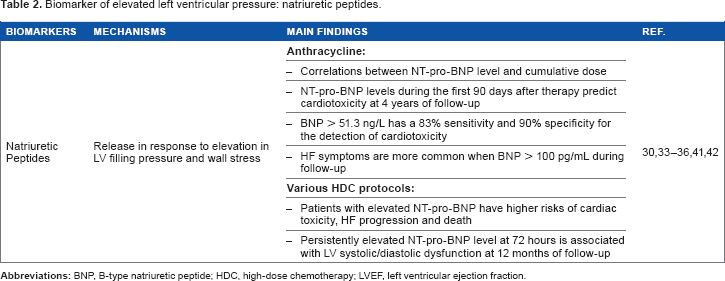
The predictive value of NT-pro-BNP levels before chemotherapy administration has also been evaluated. Patients with elevated prechemotherapy NT-pro-BNP levels had a higher risk of cardiac toxicity with HF progression and death from all causes. 35 Therefore, identification of more vulnerable individuals by unmasking preexisting subclinical disease appears to be possible, and appropriate introduction of HF therapy in such patients may limit the progression of HF. As reported with cTn, measurement of natriuretic peptide level in the first days as well as 3 months after chemotherapy administration may predict the occurrence of late chronic toxicity. In a cohort of 52 patients treated with high-dose chemotherapy, persistently elevated NT-pro-BNP levels [male > 88 ng/L (≤50 years); >227 ng/L (>50 years); female > 153 ng/L (≤50 years); > 334 ng/L (> 50 years)] were observed in 33% of patients at 72 hours and strongly associated with development of systolic (decrease of LVEF from 62.8% to 45.6%) and diastolic dysfunction; in contrast, those with transient elevations (36% of patients) or no elevations (31% of patients) showed no significant LVEF changes during 12 months of follow-up. 36 The lack of association between transient increases in NT-pro-BNP and development of cardiac dysfunction has also been reported by other investigators. 25 NT-pro-BNP levels during the first 90 days after anthracycline have also been shown to predict the development of LV remodeling at 4 years of follow-up. 30
BNP levels have been shown to correlate significantly with LVEF in only some of the published reports.37–40 In a study of 79 women treated for breast cancer with anthracycline, BNP levels >51.3 ng/L predicted the development of cardiac toxicity with a sensitivity of 83% and a specificity of 90%. 41 Also, HF symptoms were more common if BNP levels reached 100 pg/mL at least once during follow-up. 42
There remains some debate regarding the clinical usefulness of the measurement of natriuretic peptides in this setting. In two cohorts of patients in which TnT levels were predictive of cardiac toxicity, natriuretic peptides were not.43,44 Also, in patients treated with anthracycline followed by trastuzumab, NT-proBNP levels measured at the time of anthracycline treatment completion and at three months were not predictive of cardiac toxicity in contrast to cTn.27,31 Those results are probably explained at least in part by the difficulty in interpreting natriuretic peptide levels using different laboratory methods and cutoff values.7,23
Markers of inflammation
Novel biomarkers for prediction of cardiac toxicity.
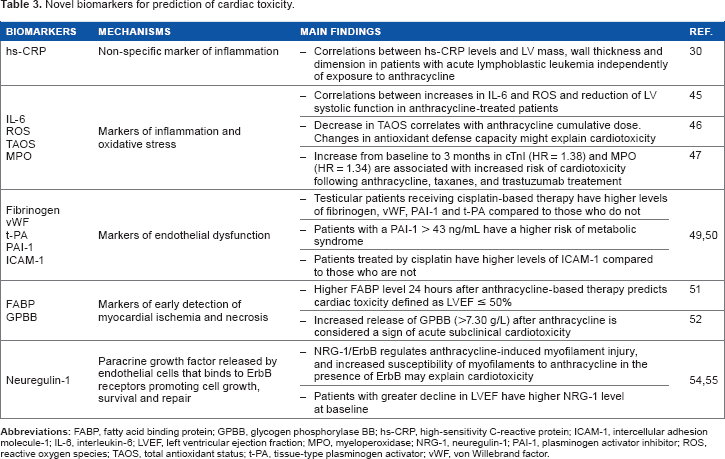
Increases in interleukin-6 and reactive oxygen species (Table 3) were significantly correlated with the reduction of LV systolic function assessed by tissue Doppler imaging in a small study of 16 patients treated with 200 mg/m2 of epirubicin. 45 In another small cohort of 29 children treated with anthracyclines for acute lymphoblastic leukemia, total antioxidant status was significantly lowered after treatment and this decrease was correlated with cumulative dose. Although direct correlation with cardiotoxicity was not reported, the authors speculated that the changes observed in the antioxidant defense capacity might play a role in anthracycline-induced cardiotoxicity. 46 Finally, in a cohort of 78 women with breast cancer undergoing anthracycline and trastuzumab therapy, increases from baseline to three months after anthracycline treatment in cTnI (hazard ratio [HR] = 1.38) and myeloperoxidase (HR = 1.40) were associated with increased risk of subsequent cardiotoxicity, with additive value for both biomarkers. 47
Markers of endothelial dysfunction
Endothelial activation can lead to vascular dysfunction and accelerated atherosclerosis. 48 In a cohort of 90 patients treated with cisplatin for testicular cancer and followed up for a median of seven years, patients who received chemotherapy had higher levels of fibrinogen, hs-CRP, von Willebrand factor (vWF), PAI-1, and t-PA compared with 44 patients treated with orchiectomy only and 47 healthy men (Table 3). Also, those with a PAI-1 > 43 ng/mL had higher triglyceride levels, body mass index, insulin-to-glucose ratio, and blood pressure, as well as decreased carotid artery distensibility and increased stiffness, compared with controls. 49 Additionally, in another similar cohort followed up for five years, higher levels of ICAM-1 have been found in patients treated with chemotherapy compared with those who were not. 50 Given that increased levels of markers of endothelial dysfunction have been identified many years after cancer therapy, suggesting an increased risk of accelerated atherosclerosis, monitoring of these markers may potentially help in cardiovascular risk stratification. Additional work is required to better evaluate the use of this strategy with these biomarkers.
Markers of myocardial ischemia
FABP and GPBB are new markers for the early detection of myocardial ischemia and necrosis (Table 3). In a cohort of 40 patients treated with a cumulative anthracycline dose of 300 mg/m2 for non-Hodgkin's lymphoma, higher FABP levels within 24 hours after treatment was predictive of subsequent cardiac dysfunction defined as an LVEF ≤ 50%. 51 In another study of 24 patients treated with a cumulative anthracycline dose of 463 mg/m2 for acute myeloid leukemia, GPBB increased above the cutoff” level (7.30 g/L) in four (16.7%) patients after the first cycle, in five (20.8%) patients after the last cycle, and remained elevated in five (20.8%) patients within six months after therapy. Increased release of GPBB from cardiomyocytes after administration of an anthracycline could be a potential sign of anthracycline-induced cardiotoxicity. 52
Neuregulin-1
Neuregulin-1 (NRG-1) is a paracrine growth factor (Table 3) released by endothelial cells that bind to ErbB (HER-2 Neu) receptors of cardiac myocytes, promoting cell growth, survival, and repair essential to maintain cardiac function. 53 It has been demonstrated that NRG-1/ErbB signaling regulates anthracycline-induced myofilament injury in cardiomyocytes. The increased susceptibility of myofilaments to anthracyclines in the presence of antibody to ErbB may explain the contractile dysfunction seen in patients receiving concomitant trastuzumab and anthracycline therapy. 54 Accordingly, in a prospective study of 78 women treated for breast cancer with anthracycline followed by trastuzumab, NRG-1 levels were measured before and after completion of anthracycline therapy; a significant decrease in NRG-1 levels was noted, suggesting a loss of cardioprotective growth factor. 55 Also, a higher baseline NRG-1 level was observed in patients with greater decline in LVEF, supporting that NRG-1 could be a potential prognostic marker of chemotherapy-induced cardiotoxicity. 55 Further research to better understand the biologic role of NRG-1 and its response to cardiotoxic chemotherapy is warranted, as it could lead to the development of a new pharmacologic strategy for cardioprotection. 56
Conclusion
With the improvement of cancer therapy, survival related to malignancy has improved but long-term cardiotoxicity has also increased with a significant impact on the quality of life and cardiovascular morbidity and mortality. Current guidelines recommend the assessment of cardiac toxicity using cardiac imaging and LVEF measurement, which requires a significant amount of myocardial damage to unmask cardiotoxicity. Accordingly, more sensitive and reproducible biomarkers predictive of cardiac toxicity should be included in routine monitoring to allow early detection, prevention, prompt treatment, and ultimately optimal recovery. The most studied biomarkers include troponin and natriuretic peptides, but other markers addressing inflammation, endothelial dysfunction, myocardial ischemia, and NRG-1 are also promising. Many studies have demonstrated the effectiveness of troponin measurement to predict early and chronic cardiac toxicity. Therefore, we believe that biomarkers, especially troponin, may complement cardiac imaging for detection and monitoring of cardiac toxicity during anthracycline-containing chemotherapy. However, standardization of the assessment of cardiac toxicity using routine measurement of troponins and other biomarkers is needed and further studies are required before establishment of clear recommendation.
Author Contributions
Wrote the first draft of the manuscript: CH. Contributed to the writing of the manuscript: CH, TH, JCT. Agree with manuscript results and conclusions: CH, TH, JCT. Jointly developed the structure and arguments for the paper: CH, TH, JCT. Made critical revisions and approved final version: CH, TH, JCT. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
Dr. Tardif holds the Canada Research Chair in translational and personalized medicine, and the University of Montreal endowed research chair in atherosclerosis.