
Abstract
This study is aimed at describing a novel method for treating patients with chronic complete spinal cord injuries (SCIs) by utilizing autologous, purified CD34+ and CD133+ stem cells (SCs). The study focuses on the safety and efficacy of transplanting unmanipulated, autologous, purified stem cells in treated patients during a 5-year follow-up period. In this report, 19 patients were included (16 males and 3 females) who presented with a complete SCI (ASIA-A) in the thoracic region. The patients' endogenous cells were mobilized with subcutaneous granulocyte-colony-stimulating factor (G-CSF) for 5 days. We utilized the CliniMACS magnetic separation system to purify leukapheresis-derived CD34+ and CD133+ SCs. Purified SCs were directly transplanted into the SCI site. Patients were then monitored and followed for up to 5 years. On average, 76 × 106 purified SCs were obtained from each patient, with 95.2% purity and >98% viability. SC transplantation into the cyst cavity or the subarachnoid space was successful and well tolerated in all 19 patients and did not cause any allergic or inflammatory reactions within the CNS in the early or late periods after transplantation. Ten patients (53%) showed no improvement after 42–60 months (ASIA-A), while seven patients (37%) demonstrated segmental sensory improvement (ASIA-B), and the remaining two patients (10%) had motor improvement (ASIA-C). This study presents a safe method for transplanting specific populations of purified autologous SCs that can be used to treat SCIs in a clinical setting. The results may be utilized as a stepping-stone for future investigations in the field of regenerative medicine for treatment of SCIs and other neurological diseases. This manuscript is published as part of the International Association of Neurorestoratology (IANR) special issue of Cell Transplantation.
Introduction
Spinal cord injury (SCI) leads to apoptosis of oligodendrocytes at the injury site resulting in demyelination and neuronal degeneration. This degeneration causes severe functional, sensory, and motor mutilations that remain an immense challenge to physicians and in which stem cell (SC) transplantation represents a viable alternative (8). A number of recent studies have focused on the regeneration of damaged neurons, injured axons, and lost neural cells to possibly treat SCI using a variety of SC types (19,21). These studies have proposed that SC therapy (SCT) could improve motor and sensory functions in SCI following transplantations (1). During recent years, researchers have discovered the ability of bone marrow-derived SCs (BMSCs) and specific populations of hematopoietic SCs (HSCs) to differentiate into neurons and glial cells under specific experimental conditions (7).
Transplanted HSCs and BMSCs were found to improve neurological conditions at injured sites of the central nervous system (CNS), through generating neural cells or myelin-producing and supporting cells (24). Furthermore, transplanted SCs may produce cytokines that can assist in the neuroprotection process (14). Yet, some factors need to be taken into consideration in the utilization of SCs for SCI, including their availability in sufficient numbers, the genetic stability of the injected cells, rejection in the host, the ability to purify specific types of SCs with their differentiation capability into neuronal cell lineages, and the development of safe and efficacious delivery methods into the CNS (12,16,18,20). Additionally, there are ethical, safety, and efficacy concerns, which may limit the application of SC transplant in patients with SCI (9). Most important when considering the repair of a SCI using SCs is that the CNS is an immune-privileged organ that is segregated from the blood by the blood–brain barrier (BBB) (6). Any compromise in BBB integrity due to the introduction of unpurified SCs that may contain white blood cells (WBCs) could lead to severe neurological damages, including impairment of oligodendrocyte function, autoimmune diseases, neurodegeneration, demyelination of myelin sheaths, and neuronal axon dysfunction (4).
In this study, we describe a method for the treatment of SCI using autologous SCs that have been purified to increase their concentration and to remove contaminating WBCs. We emphasize in the present report the effectiveness of the SC purification method to obtain specific populations of highly viable and purified cluster of differentiation 34-positive (CD34+) and CD133+ SCs. We also present an evaluation of patients, while focusing on the safety and feasibility of SCT in 19 patients with chronic and complete spinal cord injury [American Spinal Injury Association (ASIA)-A].
Materials and Methods
Formulation of the Treatment Protocol
The design of our protocol for the treatment of SCI patients by SCT was carefully planned depending on several factors. Patient safety considerations were the most important factor in determining each step of the procedure. All steps pertaining to patient handling and SC processing were carefully reviewed and planned according to the availability of clinically approved protocols and reagents. SC mobilization, collection of leukapheresis, processing of leukapheresis products (LPs), SC purification, and conditioning prior to transplantation were carried out according to a well-defined protocol as outlined in Figure 1.

Outline of our protocol used in SC transplantation in SCI patients. The figure outlines patient handling before SC transplantation, SC mobilization, collection, processing, purification, conditioning, and transplantation, in addition to patient follow-up, as described in Materials and Methods.
Patient Recruitment
Careful selection and screening of patients to be included in this study was carried out to limit variation in patient samples. Inclusion criteria were patients with complete spinal cord injuries (ASIA-A) in the dorsal region, chronic injuries ranging from 1–5 years, ages 20–49 years old, both males and females, causes of injury due to falling down (FD) or road traffic accidents (RTAs) only, and patients who have had continuous physiotherapy since the time of injury. Table 1 describes the characteristics of the 19 patients included in this study. Nineteen patients (16 males and 3 females) with complete SCI (ASIA-A) were included in this study to undergo transplantation of autologous purified SCs. The patients' ages ranged from 21 to 42 years (mean 31.5 ± 4.97 SD). The age of the injury at the time of SCT ranged from 12 to 48 months (mean 22 ± 11.25 SD). The dorsal spine was the site of injury in all 19 patients included in this study. Causes of injuries were RTAs in 15 patients and FD incidents in four patients. All patients had new magnetic resonance imaging (MRI) (Siemens AG, Erlangen, Germany) of the injured site before the procedure to precisely identify the site of spinal cord damage and the status of the canal and cord. Analyses of neurological status was performed by an independent neurologist using the ASIA scoring system, which confirmed that all patients were ASIA-A. Informed consent was obtained from each patient, and a permit from the Jordanian Ministry of Health was obtained to perform the study. Exclusion criteria were injuries less than 12 months old or more than 48 months old, nontraumatic injuries (SCI due to inflammation, autoimmune diseases) or injuries due to gunshots, patients less than 20 or older than 50 years, presence of any chronic neurological diseases or diabetes mellitus, and cases that required surgical intervention. The patients did not pay for their inclusion or treatment in this study.
Characteristics of Patients Who Underwent SC Transplantation
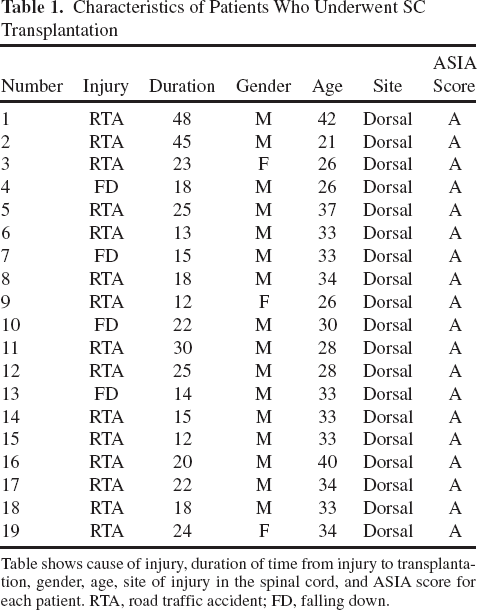
Table shows cause of injury, duration of time from injury to transplantation, gender, age, site of injury in the spinal cord, and ASIA score for each patient. RTA, road traffic accident; FD, falling down.
The procedure was thoroughly discussed with the patients and their families, and a signed consent form was obtained from each patient prior to starting the treatment. Since all the materials and chemicals used for SC collections and separations are clinically approved for human use in patients with specific hematological disorders, the procedure was permitted by the Jordanian Ministry of Health, which is the highest healthcare monitoring agency in the country that has the authority to approve or reject any patient-related treatments in Jordan.
Stem Cell Mobilization
All patients received 10 μg/kg/day granulocyte-colonystimulating factor (G-CSF; Neupogen, Amgen, Thousand Oaks, CA, USA) by subcutaneous injections for 5 days prior to leukapheresis and SC transplantation (from day −5 to day −1). Complete blood counts (CBCs) using a Mindray BC-300Plus hematology automated counter (Nanshan, Shenzhen, P.R. China) were performed on all days during mobilization (days −5 to −1) and on the day of collection of leukapheresis (day 0) to monitor the elevation of WBC counts. Flow cytometry analyses were performed on days −2, −1, and 0 using anti-CD34 and anti-CD133 monoclonal antibodies (Miltenyi Biotec, GmbH, Bergisch Gladbach, Germany), and anti-CD45 monoclonal antibody (BD Biosciences, San Jose, CA, USA). Analyses were carried out using a BD FACS Calibur (BD Biosciences) to evaluate the percentages of CD34+ and CD133+ SCs in the peripheral blood (PB).
Collection of Mononuclear Cells
On day 0, mononuclear cells (MNCs) were collected from the PB using the Cobe® Spectra Apheresis System (Ceridian BCT, Lakewood, CO, USA) and following the manufacturer's defined protocols. Collection of LPs was performed at the Apheresis Unit at Al-Khaldi Medical Center (KMC), Amman, Jordan. An average of 202 ml of LP was collected from each patient that contained on average 28.5 × 109 total MNCs.
Stem Cell Purification
To purify specific populations of SCs from LPs, we used the CliniMACSPLUS® Cell Purification System, together with a Conformité Européenne (CE)-marked, clinical-grade CliniMACS tubing set (TS), CD34 and CD133 microbead reagents, and other accessories (Miltenyi Biotec, GmbH), according to the manufacturer's defined protocols. Some modifications were made to the manufacturer's recommended protocol to allow the simultaneous purification of CD34+ and CD133+ SCs. Briefly, the LP was diluted with 400 ml CliniMACS buffer [phosphate-buffered saline (PBS) + 2 mM ethylene diamine tetraacetic acid (EDTA), clinical grade] supplemented with 0.5% v/v human serum albumin (HSA) (20% solution, CSL Behring AG, Bern, Switzerland) and was centrifuged at 200 × g for 15 min at room temperature (RT) to remove contaminating platelets, and the LP was resuspended in 43.5 ml of CliniMACS buffer. Then, 3.7 ml from each CD34 and CD133 CliniMACS reagent was added to the 43.5 ml patient's LP. We determined these volumes of LP, CD34, and CD133 reagents to maintain the same ratio of microbeads/LP volume/cell numbers that are recommended by the manufacturer. We then incubated the mixture for 30 min at RT with gentle shaking to allow binding of CD34 and CD133 microbeads to CD34+ and CD133+ SCs, respectively. One CliniMACSPLUS® run, one tubing set, and a set of accessories were used for each patient's run. To magnetically purify CD34+ and CD133+ SCs, we used the CD133 program on the CliniMACSPLUS® magnetic purification system.
Cellular Analyses
For each patient, we analyzed cellular components in the original LP immediately before CliniMACSPLUS® purification (ORI), and both the positive fraction (POS) that contains target cells and the negative fraction (NEG) that contains other cell types, after CliniMACSPLUS® purification. Cells were counted both manually by counting at least 200 cells per sample using a hemocytometer (Weber Scientific International, Cambridge, UK) and automatically using a hematology automated counter (Mindray BC-3000Plus, Shenzhen, China). CD34+ and CD133+ SC populations and cell viabilities were then analyzed by flow cytometry using propidium iodide (PI; BD Pharmingen™, Franklin Lakes, NJ, USA) and fluorochrome-conjugated antibodies (Miltenyi Biotec, GmbH). Additionally, the percentage of CD3+ T lymphocytes was determined using anti-CD3-fluorescein isothiocyanate (FITC) monoclonal antibodies (Miltenyi Biotec, GmbH) and flow cytometry.
Conditioning of Stem Cells for Transplantation
Following CliniMACS purification, SCs were centrifuged at 300 × g for 15 min at RT and resuspended in 5 ml of normal saline solution containing 0.5% patient's autologous serum. Finally, the cells were aliquoted into 3-ml injecting syringes (Medispo, Queens Village, NY, USA) (1 ml, 1 ml, and 3 ml) prior to transplantation into the patient.
Stem Cell Transplantation
The level of SCI was defined using MRI and confirmed by intraoperative C-Arm fluoroscopy (Siemens AG). Then, the prepared SCs were injected using 24-gauge spinal needles (Medline, Mundelein, IL, USA) into three sites: the subarachnoid spaces proximal (1 ml) and distal (1 ml) (10–15 mm above and below the injury site), and into the cyst within the injury site in the spinal cord (3 ml).
Results
Mobilization
The total WBC counts were followed from day −5 up to day 0, and the percentages of CD34+ and CD133+ SCs during the course of mobilization (from day −2 to day 0). Figure 2 shows the increase in WBCs, CD34+, and CD133+ SC counts during the 5 days preceding leukapheresis and SC transplantation. These results show that the patients responded well to G-CSF and were mobilized, although to varying degrees. There was a large variation in mobilization results among patients, as obviously seen in Figure 2, which shows WBC counts with high standard deviations. The average WBC counts on day −5 before the start of mobilization was 7.0 × 103 WBCs/μl (±2.4 × 103 SD). Mobilization was not evident until 2 days after the start of G-CSF administration, where the average WBC counts on days −3, −2, −1, and 0 were 1.2 × 104 WBCs/μl (±2.4 × 103 SD), 1.9 × 104 WBCs/μl (±4.3 × 103 SD), 3.7 × 104 WBCs/μl (±1.1 × 104 SD), and 4.1 × 104 WBCs/μl (±9.4 × 103 SD), respectively (Fig. 2).

Mobilization of WBCs in patients treated with G-CSF. Patients received daily subcutaneous injections of 10 mg/kg G-CSF from day −5 up to day −1. Shown are average WBC counts on days −5 to day 0, with standard deviations.
Additionally, flow cytometry analyses showed that the mobilization of SCs resulted in a marked increase in the concentrations of CD34+ and CD133+ SCs in the PB of patients as shown in Figure 3. Our flow cytometry analyses showed that the average percentages of CD34+ and CD133+ SCs out of all WBCs increased up to 0.71% (±0.51% SD) on day 0. Further analyses showed that the majority (78%) of these mobilized cells were double positive for CD34 and CD133 expression (CD34+/CD133+) (Fig. 3, bar A), whereas single CD133+ and CD34+ SCs were 4% and 18%, respectively (Fig. 3, bars B and C, respectively). Consistent with the high variations in WBC counts after mobilization, there were high variations among the patients in the percentages and absolute numbers of CD34+ and CD133+ SCs on the sixth day after mobilization (day 0). These variations in mobilization results are normally seen among healthy donors and patients.

Flow cytometry analyses of SC mobilization on days −1 and 0. The figure shows percentages of CD34+ and CD133+ SCs out of all WBCs as they increase during a patient's mobilization with G-CSF. Bars indicate averages of CD34+ and CD133+ SCs out of all WBCs in the sample, with standard deviations.
Collection of Leukapheresis Products (LPs)
An average of 202 ml (±10 ml SD) of LP was collected (Fig 4A), which contained an average of 140 million (±69 million SD) WBCs/ml (Fig 4B). Average total WBCs in the LP was 28.5 × 109 (±6.2 × 109 SD) (Fig 4C). Average viability in WBCs was 96% (±3.1% SD) (Fig 4D). Collection of LP was performed 6 days after the start of mobilization (day 0). The collection of LP resulted in a 4.3-fold increase in the concentration of CD34+ and CD133+ SCs in the LP compared with patients' PB. The average percentage of the total CD34+ and CD133+ SCs in the LP was 2.13% (±2.17% SD) (Fig 5A). The LP collection was excellent in quality, with consistently high percentages of MNCs and low numbers of granulocytes, red blood cells (RBCs), and platelets (data not shown). The bulk of RBCs, platelets, and granulocytes were efficiently removed through leukapheresis. The average numbers of RBCs, platelets, and granulocytes in the LP were <0.1 × 106/μl (±0.08 × 106/μl SD) and <1.5 × 104/μl (±0.5 × 104/μl SD), and 26% (±12% SD), respectively. Additionally, CD3+ T lymphocytes showed varying percentages in the LP. The average percentage of CD3+ T lymphocytes in LP was 36.2% (±16% SD), as shown in Figure 6.
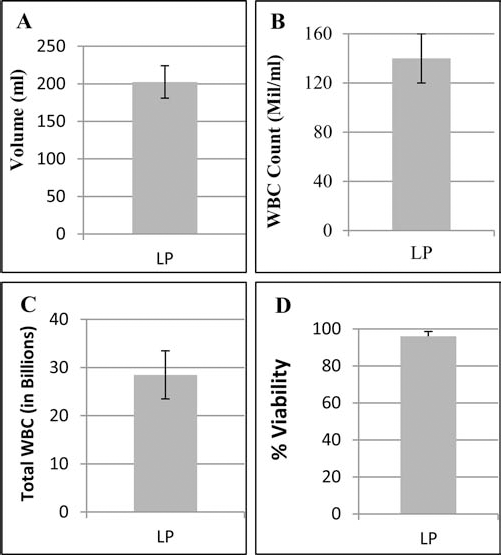
LP analyses and collection of MNCs. Leukapheresis was performed 6 days after the start of G-CSF administration (day 0) using the Cobe Spectra apheresis system. The figure shows averages and standard deviations of LP volumes (A), WBC counts/ml (B), total number of cells collected (C), and percentage of viable cells (D) for each patient.

SC purification for LP samples. Figure shows differences between percentages of CD34+ and CD133+ SCs in the initial LPs (A) and in purified populations after the magnetic purification (B). Bars represent averages of CD34+, CD133+, CD34+/CD133+, and total positive cells for both cell populations, with standard deviations.

Flow cytometry analyses of CD3+ T lymphocytes before and after purification with CliniMACSPLUS® system. Figure shows percentages of CD3+ T lymphocytes before SC purification in LPs and in purified cellular products. The percentages were calculated as CD3+ cells over the total CD45+ cells in the sample.
Stem Cell Purification
The use of CliniMACSPLUS® magnetic purification system yielded substantially higher purities of CD34+ and CD133+ SCs with an average of 94.9% (±3.7% SD) compared with an average of 2.1% (±2.2% SD) in LPs prior to purification as shown in Figure 5. The purified cells consisted of three populations of SCs with varying frequencies. We were able to purify CD34+/CD133-, CD34-/CD133+, and CD34+/CD133+ SCs. The majority of purified cells were in the double positive fraction (Fig 5B).
Our results also showed that the direct purification of SCs led to substantial depletion in the percentages of CD3+ T lymphocytes in the purified populations of SCs as shown in Figure 6. The average percentage of CD3+ T lymphocytes was down to 0.21% (±0.35% SD) in the purified populations compared with 36% (±16% SD) in LP (Fig. 6).
Additionally, to verify the sterility of the purified SCs used in transplantation, a fraction of the purified cells was cultured for at least 15 days. None of the cultured cell populations showed growth of any bacteria, fungi, or any other detectable microorganism.
Evaluation of Patients After Transplantation
All patients had a stable clinical picture of (ASIA-A) complete SCI at the time of transplantation. MRI of the damaged area revealed a focus of cystic–atrophic degeneration in the selected patients. Follow-up of patients revealed that the autologous transplantation of purified SCs was well tolerated in all patients. Seventeen patients (90%) did not develop any allergic or inflammatory reactions in the early postoperative or during the follow-up period. Low-grade fever (38–38.5°C) for 2–3 days immediately after the operation was reported in two patients (10%). The follow-up period of patients ranged from 42–60 months (average 51 ± 8.7 SD).
The follow-up of patients who received purified SCs is shown in Table 2. We report that out of the 19 patients who underwent SCT, 7 patients (37%) showed segmental sensory improvement three to four levels below the injury within 4–12 months after transplantation (from ASIA-A to ASIA-B). Two patients (10%) demonstrated additional voluntary muscle contraction with sensory improvement within 12–24 months after transplantation (from ASIA-A to ASIA-C); the same two patients later presented with improved strength of abdominal muscles and hip abductors enough to walk with braces. Independent of ASIA score improvement, 10 patients had new sensation of fullness of the bladder and control over urination. Interestingly, in five male patients (one ASIA-A to ASIA-C and four ASIA-A to ASIA-B), there was a functional improvement over previous erection status enough to have sexual intercourse. None of the patients we treated with SCT presented in this study completely recovered from the injury (ASIA-E) during the follow-up period.
Post-SC Transplantation Patient Follow-Up
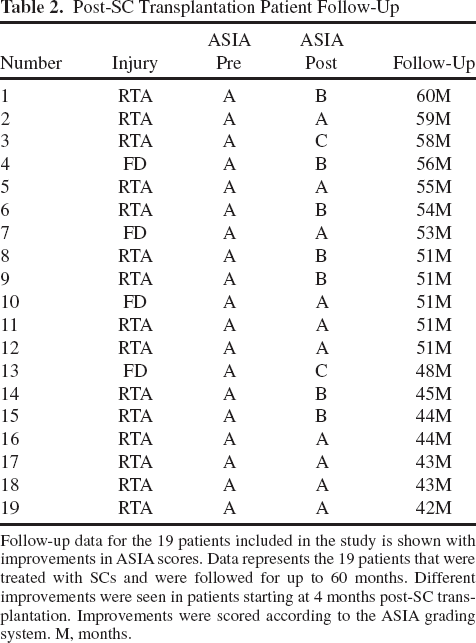
Follow-up data for the 19 patients included in the study is shown with improvements in ASIA scores. Data represents the 19 patients that were treated with SCs and were followed for up to 60 months. Different improvements were seen in patients starting at 4 months post-SC transplantation. Improvements were scored according to the ASIA grading system. M, months.
Our results showed that clinical improvement was correlated with younger age and a shorter duration of injury, where almost all of the patients who improved were between ages 26 and 33 (average 29.5 years), and the duration of injury was less than 2 years (average 19.2 months) (Table 3).
ASIA Score Improvements in SCI Patients Post-SC Transplantation

Correlation between patient's age, ASIA score before SC transplantation, duration of injury, and ASIA score after SC transplantation is shown for all patients that improved their ASIA score.
Discussion
In this report, we present for the first time a novel method for the treatment of complete SCIs using a magnetically purified combination of CD34+ and CD133+ SCs. We focus in this report on the development of the new method and show its safety on the patients following SC transplantation on the long run within the 5-year follow-up period. Using this protocol, we were able to simultaneously purify three different populations of viable and functional SCs (CD34+, CD133+, and CD34+/CD133+ SCs) that have varying curative potentials, for transplantation into patients with complete SCIs. We showed that the cells we used in this therapy were both highly pure and viable. The transplanted cells contained very low numbers of WBCs that we believe may cause chronic damage if deliberately infused into patients' CNS.
Recent studies have demonstrated that using unpurified SCs that may contain WBCs in spinal cord repair may lead to severe neuronal damage, CNS or oligodendrocyte impairment or autoimmunity, neurodegeneration, demyelination, and axonal dysfunction that are associated with severe neuronal diseases, including stroke, multiple sclerosis, and Parkinson's disease (4,15,27).
If the BBB is compromised, and immune cells come in contact with CNS-specific antigens, the immune system may attack the CNS, which can be chronic in nature; the possible outcomes of this attack can range from mild autoimmunity to significantly elevated CNS inflammation, severe CNS autoimmunity, and neurodegeneration (2,4). Therefore, repairing tissues in the CNS, such as the spinal cord, by using autologous SCs that are taken from sources, such as the bone marrow (BM) or PB, that contain high numbers of WBCs raises the concern of deliberately enhancing the immune attack on the CNS, causing CNS autoimmunity, and the ultimate rejection of these infused cells by microglial cells of the CNS (17).
Currently, there are no approved methods available for treating the CNS through the regeneration of defective CNS components (22). The ultimate goals of treatment of CNS diseases remain to stop the attack on the CNS tissues and to seek the implementation of specific strategies for regeneration of the lost or damaged CNS tissues.
In the current study, we utilized clinically approved methods for the purification of SCs. [The CliniMACS® System components (reagents, tubing sets, instruments, and PBS/EDTA buffer) are manufactured and controlled under an ISO 13485 certified quality system and are marketed world-wide as CE-marked medical devices. In the US, the CliniMACS® CD34 Reagent System is used as an FDA-approved method for selecting hematopoietic stem cells from donor apheresis for use in the treatment of patients with acute myeloid leukemia (AML), while for other applications in the US, the CliniMACS System components including the CliniMACS reagents are available for use under an approved Investigational New Drug (IND) application or Investigational Device Exemption (IDE).] The CliniMACS® system is currently utilized for SC purification purposes in routine BM transplant procedures around the world. In this study, we used clinical-grade, nontoxic, biodegradable, superparamagnetic particles for purifying CD34+ and CD133+ SCs that may have the potential for the repair of the injured spinal cords. Magnetically purified CD34+ and CD133+ SCs with high purities were used in autologous SC transplantation for 19 patients suffering from SCIs.
In the present model, we aimed at using autologous SCs for repairing injured spinal cords to avoid rejection of the transplanted cells. The use of embryonic SCs was ruled out due to limited sources, ethical considerations, and safety issues. Several sources of autologous SCs were considered for utilization in our model, including neuronal precursors, olfactory bulbs, BM, lipoaspirates, and LP collected from PB following mobilization with G-CSF (3,10,13). We opted for using LP as a source of SCs in our model due to many factors, including the availability to mobilize and collect LP from SCI patients since they have normal hemopoiesis and blood circulation, ease of collection of SCs using noninvasive surgical methods, the ability to collect sufficient numbers of SCs that do not need to be expanded ex vivo and subjected to unknown growth factors, and the ability to collect different types of early progenitor SCs that have been shown to give rise to various types of specialized neuronal cell lineages (25,26).
Several previous studies have demonstrated that CD34+ and CD133+ SCs have the potential to generate various types of neuronal cell lineages (5,25). It was shown that CD 133+ SCs possess a high potential for neuronal differentiation (11). Additionally, CD133+ SCs from human PB were found to promote corticospinal axon regeneration in the spinal cord and cortex from neonatal rats by upregulating vascular endothelial growth factor (26). On the other hand, CD34+ SCs were found to mobilize to the blood in patients with severe SCI (23).
These existing studies provide evidence of the high potentials for CD34+ and CD133+ SCs and directed the authors to utilize purified SCs in treating patients with complete SCI in order to increase the efficacy of the transplant and to reduce the possible side effects from transplanting other phenotypic cells that can be harmful and have little contribution to the regeneration of the injured spinal cord at the same time.
Our results show that after SC purification, the percentages of CD34+ and CD133+ SCs increased from an average of 2.1% in the initial LPs up to 95% pure CD34+ and CD133+ SCs in the purified cell populations. Patients received purified cells that consisted of high potential, early progenitor CD34+ and CD133+ SCs. In all 19 patients who underwent SCT in this report, the purified cells contained <1% CD3+ T lymphocytes, which we believe may have positively influenced patients' outcomes in terms of limiting anti-CNS autoimmunity of the grafted cells.
The follow-up period of our patients was 42–60 months (average 51 ± 8.7 SD). The authors hypothesize that the improvement in neurological function can be attributed mainly to the transplantation of SCs that may act in different but yet unclear mechanisms. This may include the production of neurotropic factors that stimulate neuronal growth and promote regeneration of the nervous system, differentiation of the transplanted SCs into neuronal cell lineages, or yet unknown mechanisms. Understanding mechanisms of SC-based tissue repair is currently under investigation at our facilities and elsewhere.
The time of transplantation in our group of patients ranged from 12 to 48 months from the time of injury (average 30 ± 11.25 SD). The effect of this parameter assessed in this study suggests that earlier transplantations may have better outcomes (Table 3). Further studies are needed to determine the ideal time for cell transplantation to promote neuronal regeneration following SCI and may open the doors for possibilities to implement SC transplantations for acute SCIs.
The neurological improvements noticed in our group of patients within the follow-up period reached a maximum of ASIA-B in 7 out of 19 patients (37%) and ASIA-C in two patients (10%). Although these patients are still dependent, their families noticed marked changes in their psychological status; they became more motivated and active, along with marked improvements in their lifestyles.
The authors believe that this neurological improvement, even being moderate, has great impact on the patients and their families. Although we noticed marked improvements in patients who received SCs in the past months, a more thorough study with a larger number of patients is still required to assess the effectiveness of SC-based therapy in SCIs.
We believe final conclusions on the efficacy of the procedure should be drawn after continuous extensive research in the field. However, we can generally conclude that the procedure is safe with minimal complications and that the associated improvement rates in the sensory, motor, urinary, and sexual functions are promising.
Footnotes
Acknowledgments
We would like to sincerely thank the National Center for Diabetes, Endocrinology and Genetics (NCDEG), Amman, Jordan, for permitting the use of their facility for cell processing and flow cytometry procedures, Ms. Rahaf Al-Zoubi for her help with processing SCs and CliniMACS separations, and members of Al-Khaldi Medical Center and the cellular and molecular laboratories at NCDEG for their tremendous help. The authors declare no conflicts of interest.