
Abstract
Human placenta-derived adherent (PDA001) cells are mesenchymal-like stem cells isolated from postpartum human placenta. In this study, we tested whether intravenously infused PDA001 improves neurological functional recovery after stroke in rats. In addition, potential mechanisms underlying the PDA001-induced neuroprotective effect were investigated. Young adult male rats (2–3 months) were subjected to 2 h of middle cerebral artery occlusion (MCAo) and treated with PDA001 (4 × 1 0 6) or vehicle controls [dextran vehicle or phosphate buffer saline (PBS)] via intravenous (IV) administration initiated at 4 h after MCAo. A battery of functional tests and measurements of lesion volume and apoptotic cells were performed. Immunostaining and ELISA assays for vascular endothelial growth factor (VEGF) and hepatocyte growth factor (HGF) and brain-derived neurotrophic factor (BDNF) were performed in the ischemic brain to test the potential mechanisms underlying the neuroprotective effects of PDA001 cell treatment of stroke. PDA001 cell treatment at 4 h poststroke significantly improved functional outcome and significantly decreased lesion volume, TUNEL, and cleaved caspase 3-positive cell number in the ischemic brain, compared to MCAo-vehicle and MCAo-PBS control. Treatment of stroke with PDA001 cells also significantly increased HGF and VEGF expression in the ischemic border zone (IBZ) compared to controls. Using ELISA assays, treatment of stroke with PDA001 cells significantly increased VEGF, HGF, and BDNF levels in the ischemic brain compared to controls. Conclusion: When administered intravenously at 4 h after MCAo, PDA001 cells promoted neuroprotective effects. These effects induced by PDA001 cell treatment may be related to the increase of VEGF, HGF, and BDNF expression, and a decrease of apoptosis. PDA001 cells may provide a viable cell source to treat stroke.
Introduction
Stroke is the third leading cause of morbidity and long-term disability. There is a compelling need to develop therapeutic approaches specifically designed to reduce neurological deficits after stroke. Treatment of stroke with cell-based therapy, such as bone marrow stromal cells (BMSCs) (4,25) and human umbilical cord blood cells (HUCBCs) (5,30,44) are neuroprotective and neurorestorative (38). The restorative and regenerative potential of BMSCs has also been identified in myocardial, limb, and brain ischemia (21,25). BMSCs when administered intravenously selectively migrate to the ischemic area in the brain and enhance functional recovery after stroke (5). Bone marrow (BM)-derived marrow stromal cells (MSCs) are attractive sources for autotransplantation with no risk of rejection.
MSCs are spindle-shaped plastic-adherent cells that can be isolated from BM, adipose tissue, and other organs, including the placenta. However, MSCs are a rare population (approximately 0.001–0.01%) of adult human BM. Moreover, numbers and ability of BMSCs significantly decrease with age (37,38). MSCs are also relatively few in adult peripheral blood and in term cord blood (50). Placenta-derived adherent stromal cells have multilineage differentiation potential similar to MSCs in terms of morphology, cell surface antigen expression, and gene expression patterns, are able to differentiate into many types of cells, and are easy to isolate, and large amounts of MSCs can be obtained in culture (2,11,17). Placental-derived adhesive stromal cells (PLX-PDA) can be expanded in vitro without the loss of phenotype and without showing signs of karyotypic changes. The intramuscular administration of PLX-PDA significantly improved vascular remodeling, reduced oxidative stress, and increase limb function vs. control (32). Allogeneic placental-derived adhesive stromal cells provide an off-the-shelf supply of therapeutic cells that would need no histocompatible tissue matching and are considerably more convenient to use than BM or adipose-derived MSC (32). In addition, major histocompatibility complex (MHC) class I chain-related (MIC) proteins A and B, human ligands of the activating natural killer (NK) cell receptor NKG2D, are expressed by placental cells, which play an important role in the placenta as an unique immunosuppressive organ (15). Intravenous transplantation of human placental-derived MSCs attenuates the endogenous lymphocyte reaction and improves functional outcome when treatment starts at 1 or 2 days after stroke (20,48). However, little is known about the neuroprotective effects and the mechanisms of human placental-derived MSC transplantation in the central nervous system after stroke.
Human placenta-derived adherent cells (PDA001) are a novel, culture-expanded stem cell population derived from normal, full-term human placental tissue and obtained via Celgene Cellular Therapeutics (CCT; Warren, NJ) proprietary processes. In the present study, we test whether intravenously infused PDA001 cells enter brain, survive in the ischemic brain microenvironment, and improve neurological functional recovery after stroke in rats and whether the beneficial effects of treatment persist after stroke. The potential underlying mechanisms of PDA001-induced neuroprotection are also investigated.
Materials and Methods
PDA001 cells (human adherent mesenchymal-like cells isolated from human placental tissue) were obtained from CCT. PDA001 cells are culture-expanded, undifferentiated cells with nominal phenotype CD34-, CD10+, CD200+, and CD105+ (24). The cells are exclusively of human placental (nonmaternal) origin and are karyotypically normal. PDA001 is capable of immunomodulation and suppresses T-cell proliferation and also exhibits immunomodulatory effects on other cell types involved in an immune response such as T-cell subsets, macrophages, and dendritic cells. Preclinical evaluation has demonstrated that PDA001 cells are safe and possess potent immune-suppressive properties (24). Therefore, PDA001 cells were employed in this study.
All experiments were conducted in strict accordance with the Henry Ford Health System's Institutional Animal Care and Use Committee.
Middle Cerebral Artery Occlusion (MCAo) Model and PDA001 Administration
Male Wistar rats (270–300 g; 2–3 months, from Jackson Laboratory, Wilmington, MA) were subjected to 2 h of middle cerebral artery occlusion (MCAo) induced by advancing a surgical nylon filament into the internal carotid artery (ICA) to block the origin of the MCA (1). Briefly, rats were anesthetized with 2% isoflurane in a jar for preanesthetic and spontaneously respired with 1.5% isoflurane in a 2:1 N2O/O2 mixture using a facemask connected and regulated with a modified FLUOTEC 3 Vaporizer (Fraser Harlake, Orchard Park, NY). Rectal temperature was maintained at 37°C throughout the surgical procedure using a feedback regulated water heating system (a recirculating pad and K module monitored via an intrarectal type T thermocouple). A 4–0 nylon suture, with its tip rounded by heating near a flame, was inserted into the external carotid artery (ECA) through a small puncture. The microsurgical clips were removed. The length of nylon suture, determined according to the animal's weight, was gently advanced from the ECA into the lumen of the ICA until the suture blocked the origin of the MCA. The nylon filament was retained inside the ICA for 2 h, and the neck incision was closed. The animals were moved to their cage to awaken. After 2 h of MCAo, animals were reanesthetized with isoflurane, and restoration of blood flow was performed by withdrawal of the filament until the tip cleared the lumen of the ECA. The incision was then closed.
Cryopreserved PDA001 cells were thawed in a 37°C water bath, and cell viability was calculated, with an average viability of approximately 96%. The cells were then diluted with dextran solution (10x, 1.4 mM in 0.9% NaCl; Hospira Inc., Lake Forest, IL) to 4 × 106 cells in a 1.5-ml concentration. At 4 h post-MCAo, randomly selected animals were injected via a tail vein with [1] dextran (1.5 ml) for vehicle control, [2] 1.5 ml PBS, and [3] 4 × 106 PDA001 (in 1.5 ml dextran) (n = 24/group). Previous studies have found that 3 × 106 to 5 × 106 doses of BMSC treatment improve functional outcome after stroke (4,9); therefore, a dose of 4 × 106 PDA001 cells was employed in this study.
Functional Tests
For each experimental animal, a battery of functional tests was measured at 1, 3, 7, and 14 days after MCAo by an investigator trained in functional measurements and blinded to the experimental groups. The battery of functional tests consisted of a modified Neurological Severity Score (mNSS), an adhesive-removal test, and a foot-fault test (4). The mNSS test was also performed immediately prior to treatment.
Histological and Immunohistochemical Assessment
Animals were allowed to survive for 14 days after MCAo, at which time they were reanesthetized with ketamine (44 mg/kg) and xylazine (13 mg/kg). The animals were then subjected to cardiac puncture with saline perfusion and a 4% paraformaldehyde perfusion using a Simon Varistaltic Pump (72-310-300 Manostat; Division of Barnant Company, Barrington, IL). The rat brains were fixed by transcardial perfusion with saline, followed by perfusion and immersion in 4% paraformaldehyde for 48–72 h, after which they were embedded in paraffin for immunostaining. Using a rat brain matrix (Activational Systems. Inc., Warren, MI), each forebrain was cut into 2-mm-thick coronal blocks, for a total of seven blocks per animal. A standard paraffin block was obtained from the center of the lesion (bregma −1 mm to +1 mm). A series of 6-μm-thick sections was cut from the block and stained with hematoxylin and eosin (H&E) in order to calculate the volume of cerebral infarction for each group. For lesion volume evaluation, the seven coronal brain sections were traced using a Global Lab Image analysis system (Data Translation, Marlboro, MA). The indirect lesion area, in which the intact area of the ipsilateral hemisphere was subtracted from the area of the contralateral hemisphere, was calculated (40). Lesion volume was presented as a volume percentage of the lesion compared with the contralateral hemisphere.
Immunostaining and TUNEL Staining
A standard paraffin block was obtained from the center of the lesion (bregma −1 mm to +1 mm), and a series of 6-μm-thick sections was cut from the block. Brain sections were used for each immunohistochemical staining. Immunostaining for antibodies against mouse anti-mitochondria (human-specific antigens, a specific human marker, 1:100; Spring Bioscience, Pleasanton, CA) (45), vascular endothelial growth factor (VEGF; goat polyclonal IgG; dilution 1:200; Cruz Biotech, Inc, Santa Cruz, CA), hepatocyte growth factor (HGF; monoclonal; 1:100; Assay Designs Inc, Ann Arbor, MI), and cleaved caspase 3 (rabbit polyclonal IgG; dilution 1:200; Cell Signaling Technology, Danvers, MA) was performed. Control experiments consisted of staining brain coronal tissue sections as outlined above, but with nonimmune serum substituted for the primary antibody. The immunostaining analysis was performed by an investigator blinded to the experimental groups.
TUNEL (terminal deoxynucleotidyl transferase-mediated dUTP nick-end labeling) staining was employed to determine apoptotic cells in brain section using a commercial kit (ApopTag kit, Chemicon, Temecula, CA; S7100) (25).
Measurement of PDA001 Cell Migration Into the Ischemic Brain.
In order to test whether PDA001 cells migrate into the ischemic brain, mouse anti-mitochondria (specific human mitochondria marker) immunostaining was employed. The total mitochondria-positive cell numbers were counted in the ipsilateral hemispheres of the ischemic brain.
TUNEL, Cleaved Caspase 3, VEGF, and HGF-Positive Cell Expression in the Ischemic Border Zone.
TUNEL, cleaved caspase 3, VEGF, and HGF-immunostained sections were digitized using a 40x objective (Olympus BX40; Olympus Center Valley, PA) via the MCID computer imaging analysis system (Imaging Research, St. Catharines, Ontario, Canada). The total positive cell number was counted in the ischemic border zone (IBZ). The positive cell number for TUNEL, cleaved caspase 3, VEGF, and HGF were measured, and data are presented as total number in mm2 area. The immunostaining measurement was performed by an investigator who was blinded to the experimental groups.
ELISA Assay
Additional sets of rats were sacrificed at 3, 7, and 14 days after MCAo (n = 6/group), and brain extracts were obtained from the IBZ (28). Tissue blocks were dissected on ice and wet weight rapidly measured. The brain extracts were divided into triplicate samples 200 μg each, and ELISA assays were performed using ELISA kits for VEGF (R&D Systems, Inc., Minneapolis, MN, and Calbiochem, Billerica, MA), brain-derived neurotrophic factor (BDNF, InsightGenomics, Falls Church, VA), and HGF (R&D System) (6).
Statistical Analysis
Initially, the two control groups were compared using two sample t tests. If there was no difference between PBS control and dextran vehicle control, the groups would be combined for the analysis. The global analysis using generalize estimating equation (GEE) was used to analyze the group difference on functional recovery (as the primary endpoint) measured from multiple behavior tests (26). If the overall group difference was observed at the 0.05 level, the pair-wise group comparisons would be conducted. If group differences were observed at the 0.05 using the global analysis, the group difference was tested for each functional measure, followed by pair-wise treatment comparisons. Otherwise, the pair-wise group comparison or the group comparison on each functional outcome was considered as exploratory. The global analysis on multiple outcomes is more efficient than a single outcome, when the group effects are consistent on all the outcomes (26).
Two-sample t test was used to test the differences in each histology measurement between PDA001-treated and combined control (co-control)-treated groups, respectively.
Spearman correlation coefficients were calculated among the histological evaluation measurements and their correlation with the functional recovery stratified by the treatment groups.
Results
We first tested the difference between the two control groups, PBS control and dextran vehicle control. There was no significant difference between the two control groups in functional outcome, lesion volume and TUNEL, cleaved caspase 3, and growth factor expression; therefore, the two controls were combined together as one control group, called co-control, for comparison to PDA001 treatment.
PDA001 Treatment Promotes Functional Outcome After Stroke in Rats
Functional response was measured for each experimental animal before cell therapy and after cell therapy at days 1, 3, 7, and 14 until sacrifice. The battery of functional tests consisted of mNSS, adhesive removal test and foot-fault test. There were no significant differences at 4 h after MCAo (before treatment) among the three groups measured by mNSS tests (PBS control: 10.9 ± 0.3; dextran vehicle control: 10.6 ± 0.4; PDA001 treatment group: 10.2 ± 0.6). The global analysis showed a significant group difference on functional recovery at day 7 (p = 0.00830) and day 14 (p = 0.0016) after treatment. Figure 1 shows that PDA001 treatment of stroke starting 4 h after MCAo significantly improved functional outcome at 1, 3, 7, and 14 days.

Functional tests. The difference between the two control groups (PBS control and dextran vehicle control) was analyzed. Since there is no significant difference between the two control groups in three functional tests, the two control groups were combined into one control group called combined-control (co-control) for comparison to PDA001 treatment. PDA001 treatment (4 × 106 cells) starting 4 h after middle cerebral artery occlusion (MCAo) (4hPDA4m) significantly improves functional outcome after stroke compared to co-controls (p < 0.05): (A) foot-fault test, (B) modified Neurological Severity Score (mNSS) test, (C) adhesive-remove test. *p < 0.05 vs. co-control group.
PDA001 Treatment Decreases Lesion Volume
In order to test whether PDA001 cell treatment induces neuroprotection, brain lesion volume was measured 14 days after MCAo. Lesion volume is presented as a percentage of the lesion volume compared with the contralateral hemisphere. Figure 2A shows that PDA001 cell (4 × 106) treatment of stroke initiated 4 h after MCAo significantly decreased lesion volume compared to co-controls (p < 0.05). In nontreatment control group, the lesion included both cortex and striatum. By comparison, in the PDA001 treatment group, 50% of animals had a lesion localized in both the cortex and striatum and 50% of animals had a lesion localized to the striatum only.

Lesion volume, PDA001 cell migration, terminal deoxynucleotidyl transferase-mediated dUTP nick-end labeling (TUNEL) and cleaved caspase 3 measurements at 14 days after MCAo. (A) PDA001 treatment starting 4 h after MCAo significantly decreased lesion volume compared to co-controls *p < 0.05 vs. co-control group. (B) Mitochondria (specific human marker) staining: A few PDA001 positive cells are present in the ischemic brain after intravenous administration of PDA001 cells post stroke (B, arrow: PDA001 positive cell). (C, D) PDA001 treatment significantly decreased TUNEL (C, arrow: TUNEL-positive cells) and cleaved caspase 3 (D, arrow: cleaved caspase 3-positive cells) expression in the ischemic brain compared to co-controls *p < 0.05 vs. co-control group. Co-control group: n = 26; PDA001 treatment group: n = 10. Scale bar: 100 μm (in B–D).
PDA001 Cells Migrate Into the Ischemic Brain
To test whether PDA001 cells migrate into the ischemic brain, mouse anti-mitochondria (specific human marker) immunostaining was employed (45). The total positive cell number was counted in the ipsilateral hemispheres of the ischemic brain. Few PDA001-positive cells were present in the ischemic hemisphere (12.4 ± 4.6/section); thus, approximately 1–2% of injected PDA cells (4 × 106) were present in the ischemic hemisphere at 14 days after MCAo. Figure 2B shows that very few PDA001 cells migrated into the ischemic brain and survived until 14 days poststroke.
PDA001 Treatment Decreases TUNEL and Cleaved Caspase 3 Number in the Ischemic Brain
In order to test whether PDA001 cell treatment starting 4 h after MCAo decreases cell apoptosis, cleaved caspase 3 and TUNEL immunostaining was performed at 14 days after MCAo (22,42,43,46). Cleaved caspase 3 and TUNEL-positive cells were measured in the ischemic border and in the ischemic core in the PDA001 cell treatment group. Figure 2C, D shows that PDA001 cell (4 × 106) treatment of stroke starting 4 h after MCAo significantly decreased TUNEL and cleaved caspase 3 number in the ischemic brain compared to co-controls (p < 0.05).
PDA001 Treatment Increases Growth Factor Expression in the Ischemic Brain
Growth factor treatment of stroke induces neuroprotective effects (10,36). In order to test whether PDA001 cell treatment regulates growth factor expression, VEGF and HGF immunostaining were employed. Figure 3 shows that treatment with PDA001 cells (4 × 106) starting 4 h after MCAo significantly increased HGF and VEGF expression in the IBZ compared to co-controls (p < 0.05). Using ELISA assays, Figure 4 shows that treatment with PDA001 significantly increased VEGF levels (at 7 and 14 days after MCAo; p < 0.05), increased BDNF levels (at 3 and 14 days after MCAo; p < 0.05), and increased HGF levels (at 7 days after MCAo; p < 0.05) compared to co-controls.
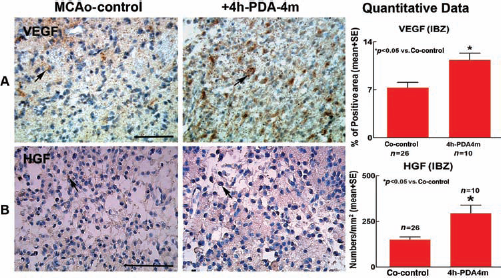
Vascular endothelial growth factor (VEGF) and hepatocyte growth factor (HGF) expression in the ischemic brain at 14 days after MCAo. PDA001 treatment starting 4 h after MCAo significantly increases VEGF (A, arrow: VEGF-positive cells) and HGF (B, arrow: HGF-positive cells) expression in the ischemic brain compared to co-controls *p < 0.05 vs. co-control. Co-control group: n = 26; PDA001 treatment group: n = 10. Scale bar: 100 μm (in A, B).

Growth factor measurements at 3, 7, and 14 days after MCAo using ELISA assay. PDA001 treatment starting 4 h after MCAo (+PDA-4M) significantly increases brain-derived neurotrophic factor (BDNF) levels at 3 and 14 days after MCAo (p < 0.05) compared to co-controls (MCAo-control) (A), increases VEGF levels at 7 and 14 days after MCAo compared to co-controls (B), and increases HGF levels at 7 days after MCAo compared to co-controls (C). *p < 0.05 vs. co-control group. MCAo-control: n = 11–12/group in each time point; PDA001 treatment group: n = 6/group in each time point.
Discussion
In this study, we found that PDA001 treatment initiated at 4 h after MCAo improves functional outcome and decreases lesion volume, TUNEL, and cleaved caspase 3 cell number in ischemic rat brains. PDA001 treatment also significantly increases VEGF and HGF expression and increases VEGF, HGF, and BDNF levels in the ischemic brain as measured by ELISA assay. The data suggest that PDA001 treatment at 4 h after MCAo promotes a neuroprotective effect after stroke in rats.
Previous studies have found that human placenta cells display low immunogenicity both in vitro and in vivo (2). Intravenous transplantation of human placenta MSCs attenuates the endogenous lymphocyte reaction (20). The immunosuppressive effect is more pronounced in human placental MSCs, possibly due to the expression of intracellular human leukocyte antigen-G (HLA-G) (3). Human placental MSCs suppress both mitogen-induced and allogeneic lymphocyte proliferation in both CD4 and CD8 populations (3). The immunosuppression of human placental MSCs was significantly stronger than that with BMSCs (3). Therefore, immunosuppressants were not employed in this study.
The pathophysiological events after cerebral ischemia leading to neuronal death and functional disabilities are complex and interconnected. Acute neuronal injury is followed by a secondary neuronal death in the neighboring area of the ischemic core (19). Apoptosis is a key factor that contributes to the delayed injury in the penumbra (12). Caspases are essential players in cell death (34). Administration of a broad spectrum of caspase inhibitors to ischemic rodents induced neuroprotection (33). PDA001 treatment significantly decreased TUNEL and cleaved caspase 3 number as well as decreased lesion volume compared to MCAo control. Decreased TUNEL and cleaved caspase 3 may contribute to the PDA001-induced neuroprotection. Previous studies also found that transplantation of human placenta adherent stromal cells derived from maternal or fetal placenta improves functional outcome after stroke (20). The placenta may prove to be a useful source of MSC-like cells (27) for the treatment of stroke and possibly for neural injury and neurodegenerative disease (31). The data demonstrate, for the first time, that PDA cells administered to a model of focal stroke, provides neuroprotection. The mechanism of how PDA001 treatment decreases apoptosis and whether regulation of Bcl2 and Bax reduces apoptosis, warrant further investigation.
The mechanisms underlying transplanted PDA001 cell-induced functional benefit and neuroprotection after stroke are not clear (48). In contrast to the focus in the field of stem cell transplantation, in which the implanted stem cells are expected to integrate into and to replace the damaged tissue, only a very small percentage of PDA001 migrated into the ischemic brain in our study; functional recovery was found 1 day after administration of PDA001. In addition, the number of cells that enter tissue is small, and tissue replacement would comprise far less than a cubic millimeter. Previous studies also found that only few human placenta MSCs migrate into the ischemic brain and express astroglial and neuronal markers (48). Central nervous system availability of grafted cells is not a prerequisite for acute neuroprotection provided (1). Therefore, it is highly unlikely that these cells integrate into the cerebral tissue and make appropriate connections after transplantation and contribute in a substantive way to the observed therapeutic benefit.
Recent evidence indicate that transplanted MSCs promote endogenous repair of neurologically damaged areas via the release of soluble trophic factors and cytokines (13). We and others have shown that exogenous cells produce factors and more importantly stimulate the production of neuroprotective and neurorestorative factors in parenchymal cells (7,16,25,41,49). Intravenously administered BMSCs used to treat stroke or CNS disease produce trophic factors and stimulate parenchymal cells to express trophic factors (7,8,47). Growth factors are the molecular signals by which the body regulates cell survival, proliferation, and differentiation. Human MSCs cultured with ischemic rat brain extract show increased production of BDNF, VEGF, and HGF (8). Human placenta-derived adhesive cells also express and secrete HGF and VEGF (14,29). Many factors may regulate neuroprotection after PDA001 treatment. In the present study, based on prior work (8), we elected to measure VEGF, BDNF, and HGF expression. We found that PDA001 treatment of stroke significantly increases VEGF, BDNF, and HGF levels in the ischemic brain. VEGF is an angiogenic and neuroprotective factor that can increase axonal outgrowth, block neuronal apoptosis, and increase neurogenesis, thus promoting neuroprotection post stroke (18,39). HGF is a candidate for acute stroke treatment: overexpression of the HGF gene attenuates brain ischemic injury through angiogenic and neuroprotective actions in rats (35). Acute HGF treatment induces long-term neuroprotection and stroke recovery via mechanisms involving neural precursor cell proliferation and differentiation (10) and decreases caspase 3-dependent hypoxic injury in cultured neurosphere (10). Intravenous administration of conjugated BDNF promotes neuroprotection in ischemic brain (51). BDNF also plays an important role in promoting neuroprotection after stroke. MSCs transfected with the BDNF or GDNF gene improves neurological function and reduces ischemic damage in a rat model of MCAo (23). Increased VEGF, BDNF, and HGF levels may therefore contribute to PDA001-induced neuroprotection after stroke in rats. We found that BDNF expression was significantly increased at 3 days after stroke. HGF was increased at 3 and 7 days after treatment. VEGF was significantly increased at 7 and 14 days after MCAo. Therefore, the increase of VEGF may play an important role in maintaining functional outcome after PDA001 treatment but may not initiate the neuroprotection effect. The present study is the first to report that intravenous administration of PDA001 during the hyperacute stage in stroke can regulate growth factor expression and induces neuroprotective effects. Which factors initiate the neuroprotective effects, what is the mechanisms underlying the neuroprotective benefit early after onset of treatment, and whether PDA001 cell treatment modulates innate cerebral inflammatory responses and the immunomodulatory properties of PDA001 treatment warrant further investigation.
Conclusion
We found that 4 h after MCAo, intravenously administered PDA001 cells improved functional recovery and decreased lesion volume, TUNEL, and cleaved caspase 3 after stroke. PDA001 treatment also increased growth factor expression, which may mediate or contribute to the PDA001 treatment-induced neuroprotective effect after stroke. Since PDA001 cells are widely available and have been used preclinically, they are potentially an excellent source cells for treatment of stroke and deserve further investigation.
Footnotes
Acknowledgments
The authors wish to thank Qinge Lu and Sutapa Santra for technical assistance. Funding support for this study was provided by Celgene Cellular Therapeutics. Ajai Pal, Andrew Zeitlin, and Robert Hariri are employees of Celgene and hold stock options in Celgene.