
Abstract
BACKGROUND AND AIM:
There is a limited data at the moment regarding the clinical value of inflammatory indices and malnutrition markers in children with acute leukemias. We have examined the usefulness of prognostic nutritional index (PNI), Glasgow prognostic score (GPS), Prognostic Index (PI), monocyte to lymphocyte (MLR), neutrophil to lymphocyte (NLR), and platelet to lymphocyte (PLR) ratios to stratify patients as regards the response to induction therapy correlating them to different prognostic factors.
PATIENTS AND METHODS:
Children with acute leukemia and without microbial-induced inflammation at the time of diagnosis were prospectively recruited. Preliminary total and differential CBC, c-reactive protein (CRP), serum albumin (ALB) were used to calculate different inflammatory indicators including NLR, MLR, PLR, PNI, GPS, and PI.
RESULTS:
Higher PNI was significantly more associated to children who achieved remission as compared to those without remission (
CONCLUSION:
Pretreatment PNI, GPS, CRP, serum albumin, NLR, MLR, and PLR are remission promising prognostic markers in pediatric acute leukemias, which deserve to be further investigated in large-scale studies.
Keywords
Introduction
In the pediatric population, acute leukemia is the most common cancer representing 25% of all malignancies, with acute lymphoblastic leukemia comprising 20% and acute myeloid leukemia 5% of all cases; the estimated US and worldwide incidence is 3.7–4.9 cases per 100,000 children aged 0–14 years [1]. In the past few decades, there has been a dramatic improvement in 5-year survival rates that now reach 90% for ALL, and 65–70% for AML [2].
An inflammatory environment for malignant tumors is assumed to modulate the growth of malignant cells, thus contributing to angiogenesis, mutation, cellular migration, and metastasis acting through the release of different cytokines and other inflammatory mediators [3].
Inflammation can result from trauma, ischemia-reperfusion injury, chemically-induced injury, and other causes unrelated to infectious organisms. Sterile inflammation can occur in acute pictures and is similar to microbial-induced inflammation in that it is marked by the recruitment of neutrophils and macrophages, in addition to the production of pro-inflammatory cytokines and chemokines, such as tumor necrosis factor-
Different cohort studies had examined C-reactive protein (CRP) and the risk of malignancy, including a meta-analyses of the risk of incidence of colorectal [5], lung [6], ovarian [7], and breast cancers [8]. Although the results didn’t find significant associations, other case-control studies have reported low positive predictive values for inflammatory markers, including CRP, in a variety of malignancies, such as bladder and renal cancers, Hodgkin’s and non-Hodgkin’s lymphoma, and multiple myeloma [9, 10, 11, 12].
Systemic inflammation is increasingly being recognized as an important outcome determinant in cancer patients [13, 14, 15, 16], as cancer progression and prognosis are affected by the inflammatory response of the patient in the surrounding tumor microenvironment. Neutrophils, lymphocytes, and platelets are recognized to have an important role in carcinogenesis and hence in tumor progression [17].
In a prospective cohort study, the cancer incidence increased with rising of inflammatory markers in a dose-response relationship [18]. Out of 506 people with ESR
Recently, several peripheral blood-derived, inflam- mation-based scores and indices such as neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), Glasgow and modified Glasgow prognostic Scores (GPS), and prognostic nutritional index (PNI) have been assumed to be prognostic markers in cancer [19].
Many studies showed that preoperative inflammatory markers, including prognostic index (PI), were found in univariate analysis to be associated with overall and disease-free survival and were considered to be independent predictors of survival in gastric cancer [20, 21].
In a population-based study, the concentrations of different cytokines and inflammatory markers from 178 children aged 1–9 years with B-ALL were measured and compared to 178 matched controls [22]. The results supported the hypothesis that children with B-ALL were born with dysregulated immune functions.
A growing body of evidence indicates that cancer-related malnutrition, as expressed in GPS and PNI, has adverse effects on treatment and survival outcomes for many solid malignancies [23, 24, 25].
There is a limited data at the moment regarding the clinical value of inflammatory indices and malnutrition markers in children with acute leukemias. We have examined the usefulness of prognostic nutritional index (PNI), Glasgow prognostic score (GPS), Prognostic index (PI), monocyte to lymphocyte (MLR), neutrophil to lymphocyte (NLR), and platelet to lymphocyte (PLR) ratios to stratify patients as regards the response to induction therapy correlating them to different prognostic factors.
Patients and methods
This was a prospective study conducted at The South Egypt Cancer Institute and Assiut University Hospital, which was approved by the Assiut University Ethical Committee. The study involved a cohort 73 children diagnosed with acute leukemias. Patients with microbial-induced inflammation as detected by cultures were excluded.
The diagnosis of acute leukemia depends on peripheral hemogram assessment, morphologic bone marrow (BM) examination, cytochemical studies, and flow cytometry to identify the cell lineages and subsets.
CD56, a marker of natural killer (NK) cell differentiation, defines a rare subgroup representing about 3% of ALL which often displays other early T-cell antigens such as CD2 CD5, CD7 and sometimes cCD3 [26] as measured by flow cytometry.
At diagnosis, preliminary total and differential CBC, c-reactive protein (CRP), serum albumin (ALB) were used to calculate different inflammatory indicators including: neutrophil to lymphocyte ratio, calculated by dividing absolute neutrophilic count by absolute lymphocytic count; monocyte to lymphocyte ratio, calculated by dividing absolute monocytic count by absolute lymphocytic count; platelet to lymphocyte ratio, calculated by dividing absolute platelet count by absolute lymphocytic count; Glasgow prognostic score (GPS); defined by CRP (g/L) and serum ALB (g/L) as 0, 1, and 2. GPS score 0 is given for those with CRP
The treatment for newly diagnosed ALL has 3 major phases, reflecting a reliance on multidrug regimens to avoid the development of resistance, with variable intensities according to each patient’s risk. Remission induction is the first phase of chemotherapy, lasting 4 to 6 weeks, that includes agents such as vincristine, corticosteroids, asparginase, and anthracycline. It is followed by consolidation, which consists of 8 weeks of multidrug chemotherapy given to eradicate the microscopic residual disease that persists after induction of remission, with higher risk patients receiving longer and more intensified regimens. The final and long-lasting phase is maintenance chemotherapy in which less intensified usage of cornerstone drugs such as methotrexate, and 6-mercaptopurine, proceeds for 2–3 years. In parallel, prophylaxis and treatment of CNS disease is achieved through intrathecal chemotherapy, administration of systemic chemotherapy able to penetrate the blood-brain barrier, and cranial irradiation.
Treatment of AML depends on induction with anthracycline and cytarabine for all patients in course 1 and for non-high risk (HR) patients in course 2, and mitoxantrone combined with cytarabine in high risk patients in course 2, different regimens are used in induction of remission including FLAG-Ida, ADE, this is followed by consolidation chemotherapy given in courses 3, 4 consisting of two courses of high dose Ara-C plus intrathecal chemotherapy for standard risk AML, while FLAG-Ida is given in course 3 followed by high dose Ara-C and L-Asparginase for high risk patients if stem cell transplantation is not available. HR patients are sent for stem cell transplantation at specialized centers if feasible.
ALL remission has been defined by morphology (
According to the revised recommendations of the International Working Group (IWG), the criteria used to define complete remission are:
Statistics
Descriptive statistics including percentages, mean, median, standard error were used in this study. Inferential statistics utilized to determine data significance included independent sample
Results
Seventy-three children with acute leukemia were recruited including 48 patients with ALL and 25 patients with AML; the median age was 9 years, male predominance was observed, Table 1. Different laboratory parameters were illustrated in Table 2.
Demographic data of 73 children with acute leukemia
Demographic data of 73 children with acute leukemia
Laboratory parameters of 73 studied patients with acute leukemia
HB; hemoglobin, CRP; c-reactive protein, ALB; albumin, BM; bone marrow, ESR; erythrocyte sedimentation rate.
The mean BM blasts was 56.78
Eighteen out of forty-eight ALL patients achieved complete remission to induction therapy, while 9/25 patients with AML achieved complete remission, Table 3.
Significantly, all patients without remission were shown to have PNI
Glasgow prognostic score (GPS) and remission
By the same token, all patients without remission were found to have GPS 1 and 2, while most patients in remission (21/27) were found to have GPS 0 and 1 (
Relation of PI to induction results
Although both CRP and white blood cells were elevated in acute leukemias, PI had no relation to response to induction chemotherapy, Fig. 3.
Relations of NLR, MLR, and PLR and induction results
The mean NLR for patients who achieved complete remission was 3.5
Response to induction therapy
Response to induction therapy
Induction results according to different PNI categories, (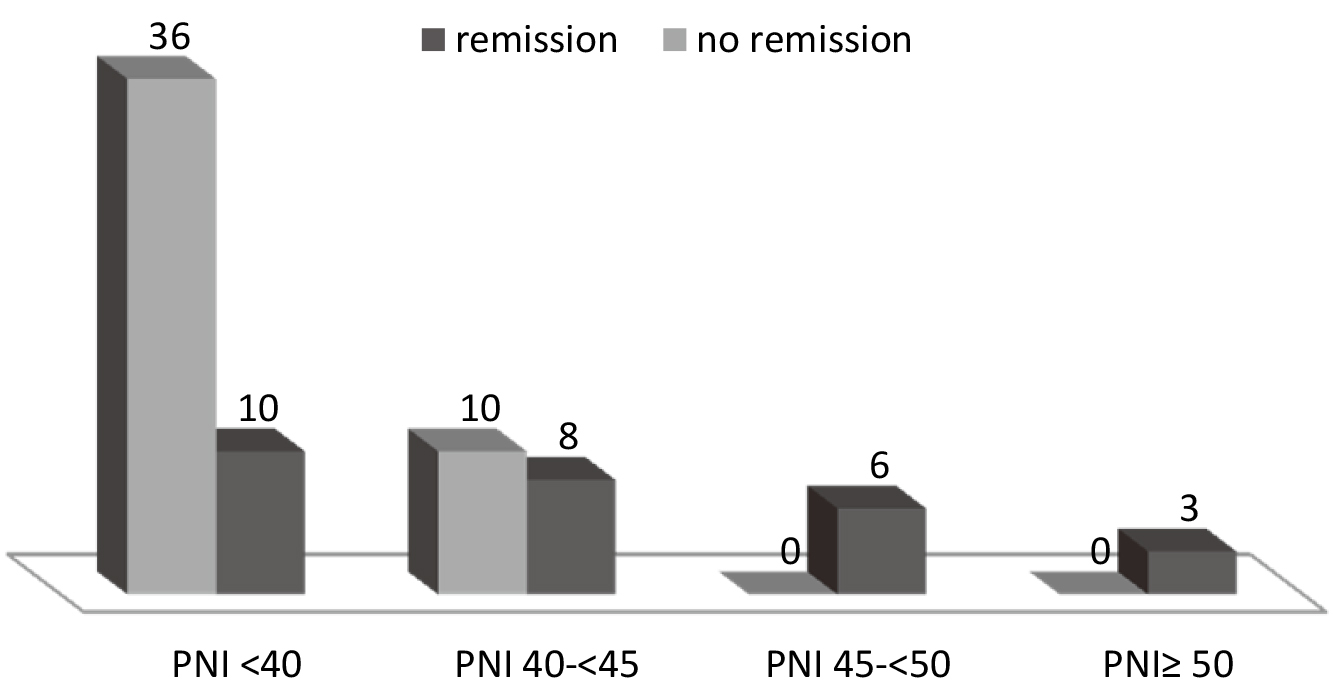
Induction results according to different GPS categories, 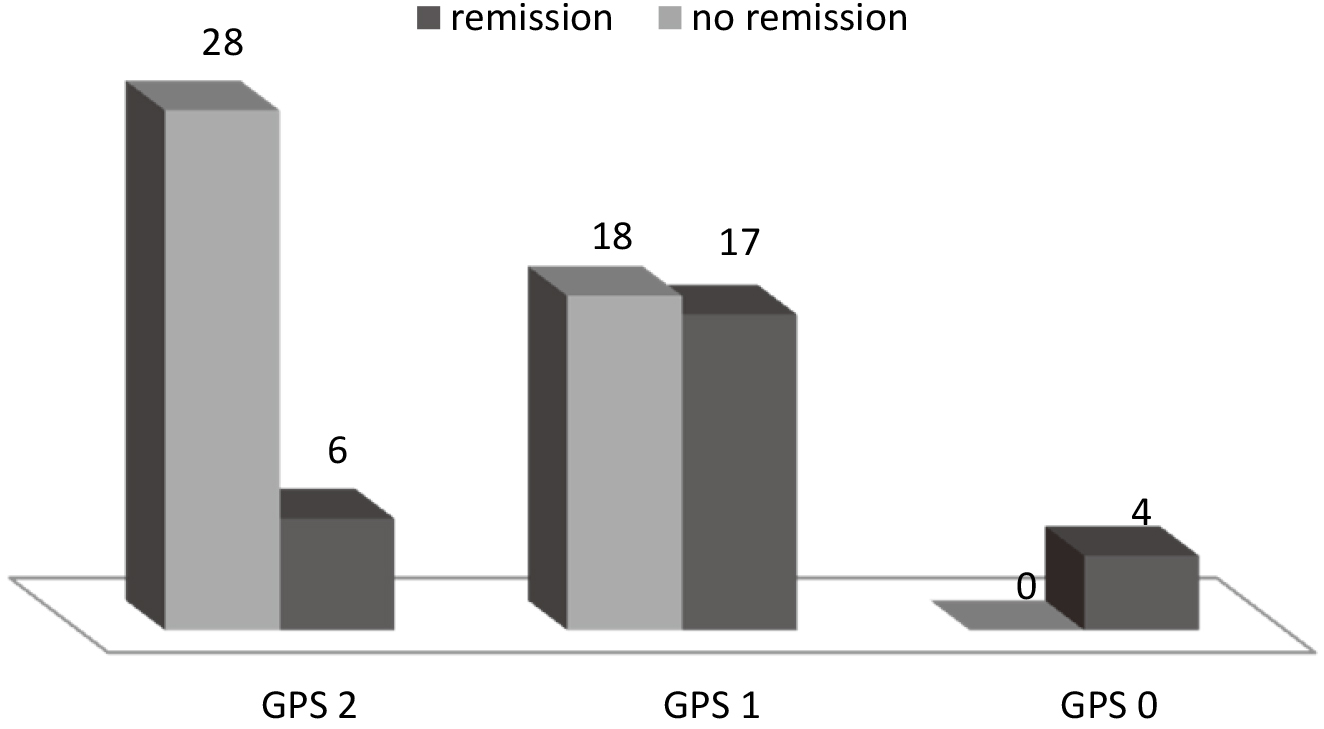
Relation between PI categories and induction results, Cramer’s V value 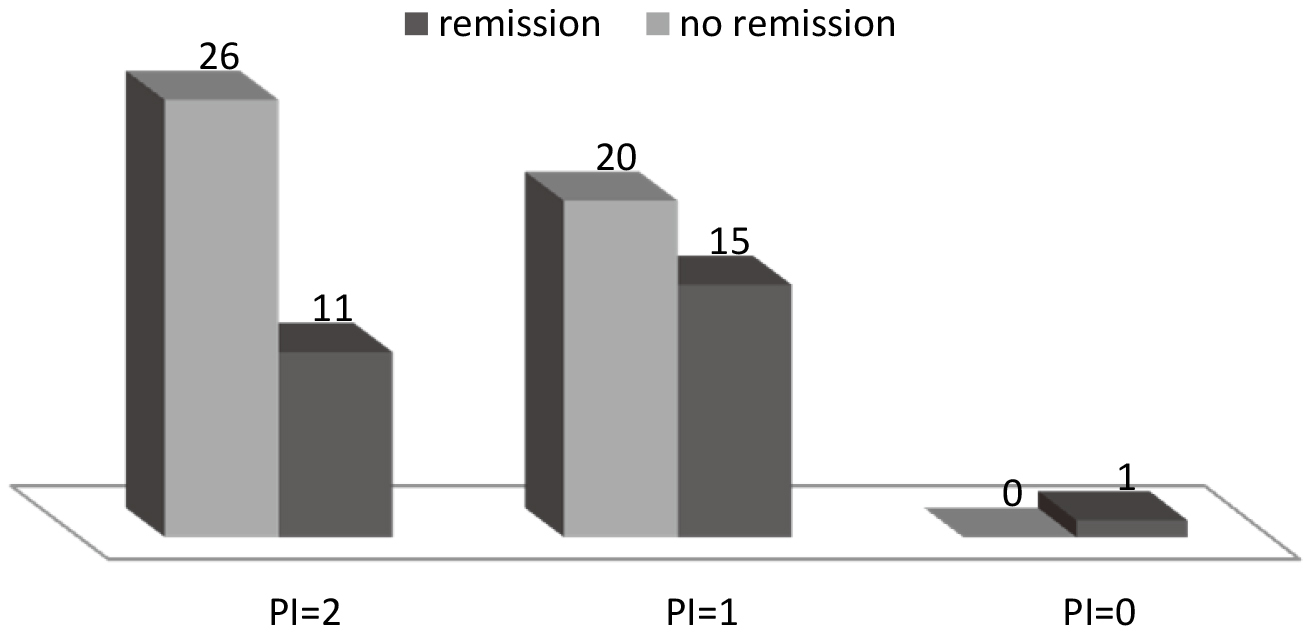
Difference of mean NLR according to induction results.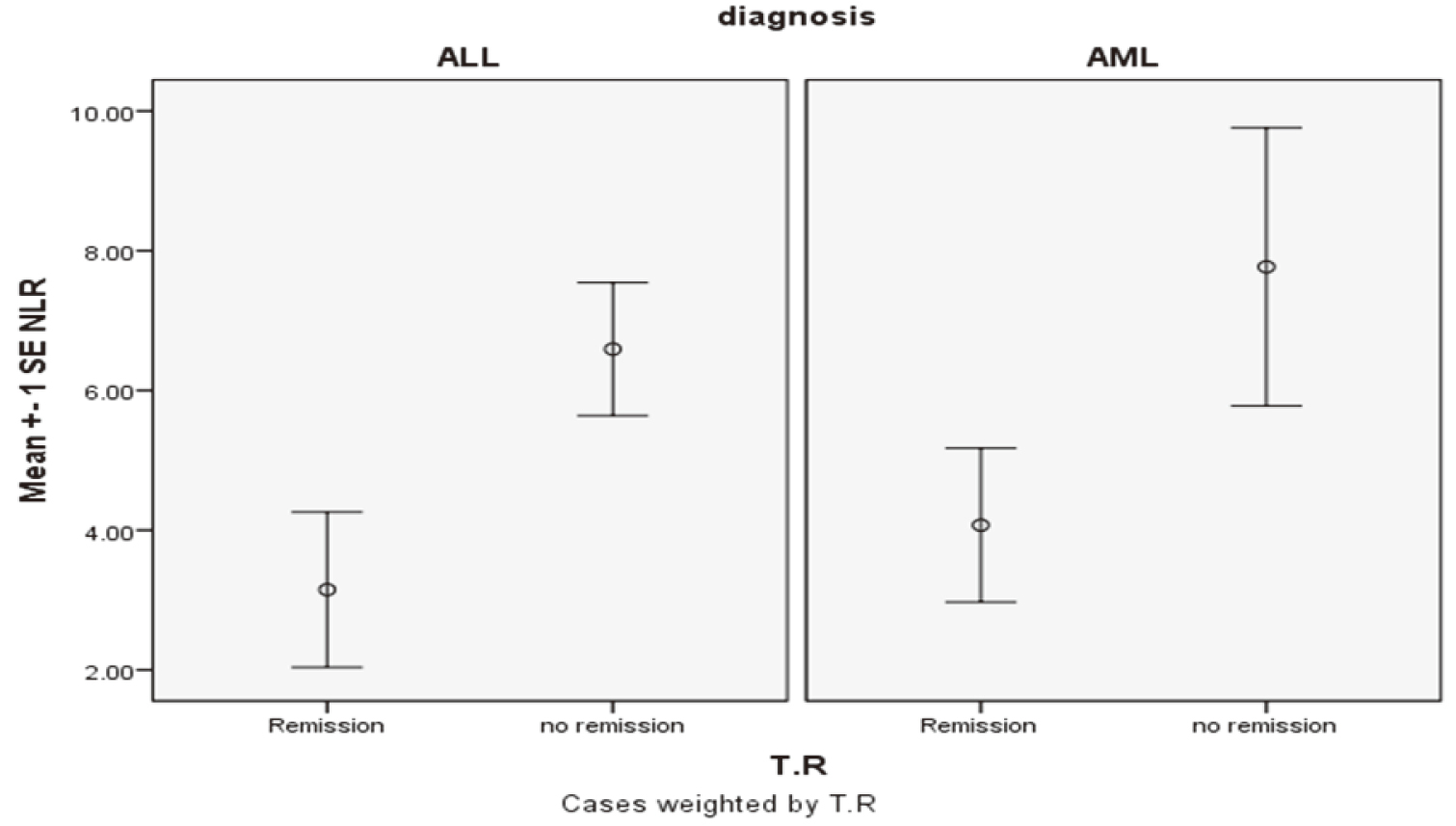
The ROC curve for MLR and PLR showed AUC for MLR 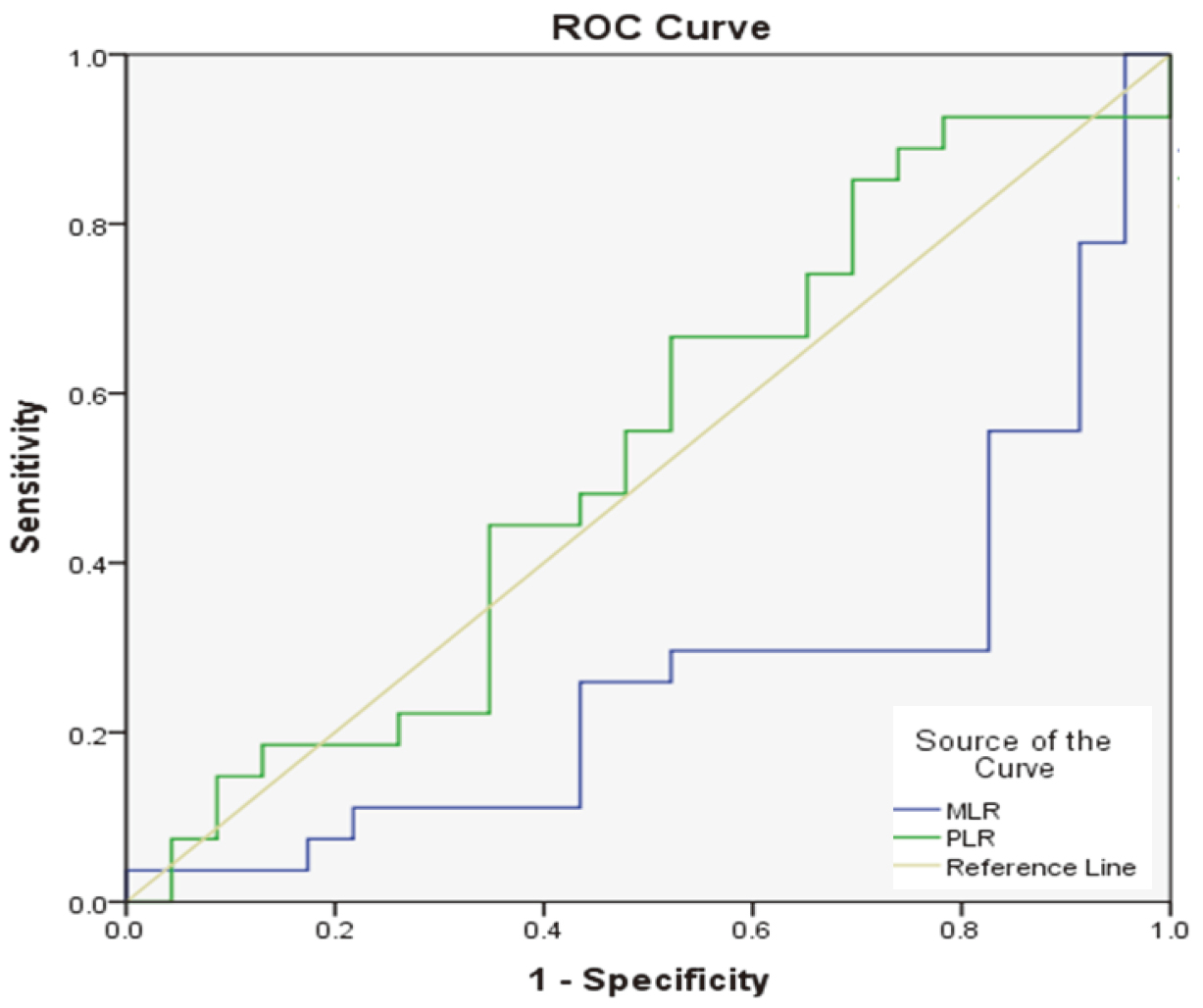
A ROC curve was built to determine the cutoff values for MLR and PLR allowing adequate discrimination between patients who achieved complete remission and those without complete remission, Fig. 5.
Relation between MLR categories and treatment response
Relation between MLR categories and treatment response
Data analyzed by Phi test.
Differences in ALL and AML regarding inflammatory indices
Data expressed as mean
Univariate analysis of inflammatory indices in treatment results of ALL patients
Data analyzed by using independent sample
Patients without remission had a significantly higher MLR than those in remission as illustrated in Table 4.
Mean CRP value 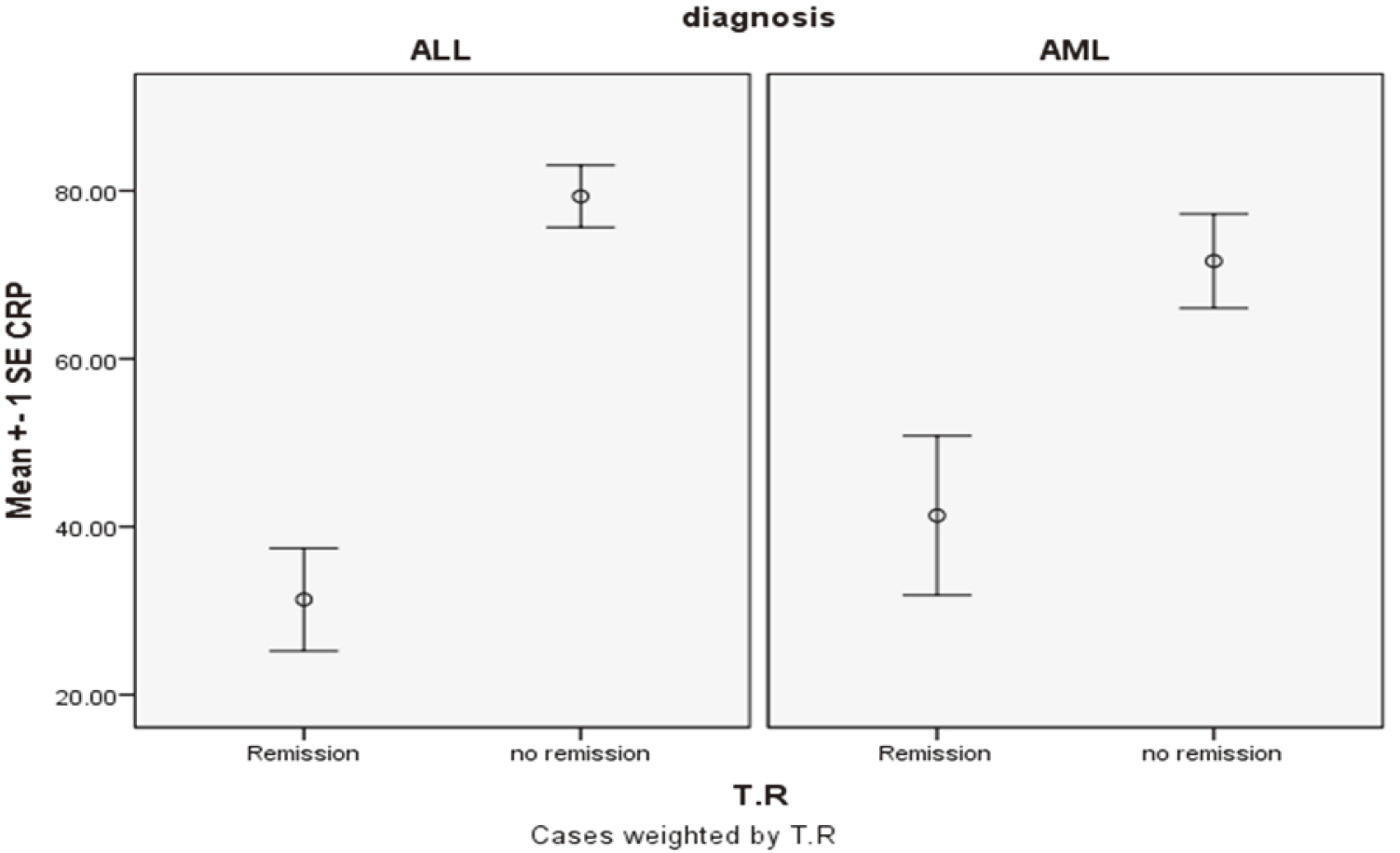
Significant differences were observed in the mean CRP values obtained from patients who attained complete remission (CRP
No significant differences were found in the mean
Univariate analysis of inflammatory indices in the treatment results of AML patients
Univariate analysis of inflammatory indices in the treatment results of AML patients
Data analyzed by using independent sample
Logistic regression of inflammatory indices in ALL patients
Data were analyzed by using logistic regression with the method forward stepwise (likelihood ratio) method.
We found similarity between both ALL and AML as regards the distribution of inflammatory markers and indices in ALL and AML with the majority of cases showing higher scores of PI, GPS, PNI, and MLR
Patients in complete remission had significantly lower NLR (
Differently from ALL, patients with AML achieving remission were found to have significantly lower MLR mean
Correlations between different prognostic features of acute leukemia and inflammatory indices
Data analyzed by Pearson correlation,
Differences in the mean 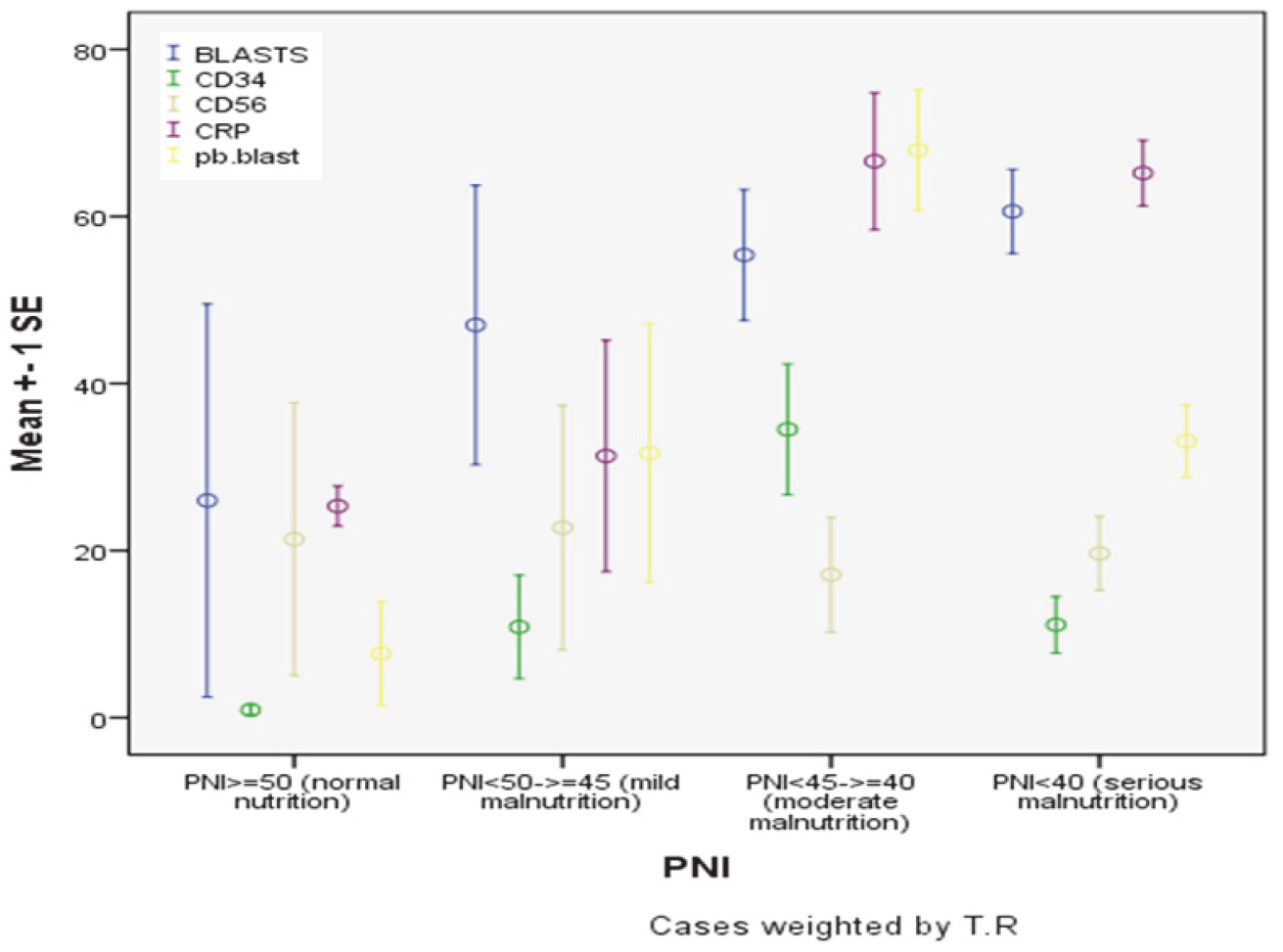
Different prognostic features of acute leukemia according to MLR categories, independent sample 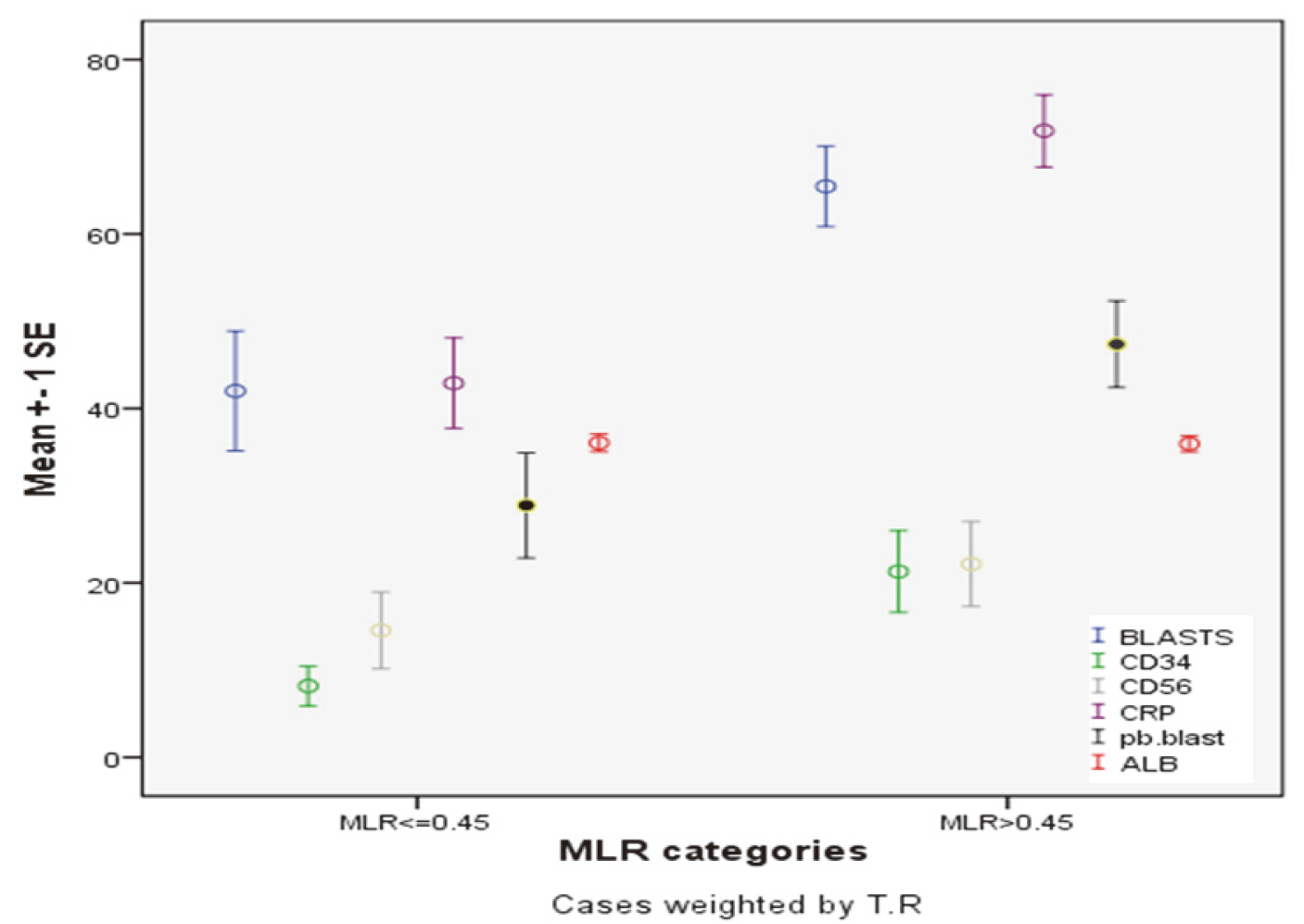
The independent predictors of treatment response for ALL were GPS (Wald
Significant positive correlations were found between CD34 and CRP (
Relations of PNI, GPS, and MLR categories to adverse prognostic factors of 73 children with acute leukemias
Significant differences were found in the mean values of CD34 among different PNI groups, with higher mean CD34 in PNI
Patients with MLR
Discussion
Pediatric acute leukemia has moved from being an incurable fatal disease to a disease with a cure rate exceeding 75% [28], and 5-year survival rates approaching 90% in ALL and 70% in AML.
Management of childhood acute leukemia in Egypt suffers from multiple challenges, including limited health resources, inadequate financial support, treatment abandonment, decreased adherence to standardized protocols, and limited diagnostic measures for adequate risk stratifications.
In the current study, we focused on simple and easily applicable measurements that might correlate with prognosis, including GPS, MLR, NLR, and CRP, which were found to be significantly higher among those children unable to achieve complete remission, as well as PNI whose increase was associated to remission.
PNI was originally proposed to assess the perioperative surgical risk and immunological status in gastrointestinal malignancies, with values
On the other hand, little is known about the role of PNI in hematologic malignancies. Thus, Go et al. reported that PNI
Systemic inflammation promotes angiogenesis, proliferation, and survival of tumor cells as well as tumor progression and metastases. Inflammation-based prognostic scores, including platelet-to-lymphocyte ratio, neutrophil-lymphocyte ratio, and Glasgow Prognostic Score- which combines both C-reactive protein as a marker of inflammation and albumin as a marker of nutrition-, have been attributed prognostic value for patients with cancer [32, 33]. Furthermore, the role of GPS remains to be defined in hematologic malignancies, although a retrospective evaluation of 252 patients with DLBCL demonstrated that high GPS, high NLR, high PLR and low PNI in univariate analysis, were all associated with poor overall survival (
Interleukin-6 is implicated in quite a number of acute and chronic inflammation-related diseases through promotion of positive acute phase reactants (e.g., CRP) and negative reactants (e.g., ALB), which participate in tumor growth and invasion. Previous studies reported that IL-6 was associated with poor survival in DLBCL [34], and therefore, the shutting-off of inflammatory cytokines greatly interfere with tumor progression. Likewise, patients with higher CRP had lower remission rates in both ALL and AML (
Although GPS is a good index of inflammation and malnutrition and has suggested prognostic value in many solid malignancies [35, 36, 37, 38], studies discussing its role in hematologic malignancies are lacking. To our knowledge, the current report is the only one to address its prognostic significance in pediatric acute leukemias.
Moreover, systemic inflammation induces the release of inhibitory cytokines, including transforming growth factor-
Patients with multiple myeloma ineligible for autologous BMT and treated with melphalan, bortezomib and prednisone with NLR
Inflammatory cytokines such as IL-3, IL-6, and IL-10 produced in different cancers that cause thrombosis and enhance tumor growth and motility, contributing to metastasis. It has been previously shown that patients with PLR
Because of low cost, easy reproducibility, and wide availability of these inflammatory markers and indices, they were extensively studied in many cancers to evaluate their prognostic impact and their capacity to provide an easy and rapid outcome prediction. However, the best marker and the optimal cutoff value for each type of cancer are still debatable.
The relation between severity of symptomatic burden and several inflammatory markers was analyzed in a prospective study involving 95 patients with AML before and during the induction phase of the treatment. This study concluded that the change in severity of symptoms during therapy was not translated significantly into a change in levels of inflammatory markers suggesting that the absolute levels of inflammatory markers during induction treatment was more important than their relative change over time [43].
Serum albumin was considered an independent prognostic factor in AML, given that patients with levels
The current study is limited by its single arm nature with relatively small number of analyzed patients, and also by of the acute leukemias heterogeneity. Pretreatment measurement of inflammatory indicators is not currently a standard practice in acute leukemia and should not be overestimated until a properly designed prospective trial with the correct sample size proves the potential role of these markers.
Conclusion
Pretreatment CRP, ALB, PNI, GPS, NLR, MLR, and PLR are promising prognostic markers of remission in pediatric acute leukemias that need to be further investigated in large scale studies.
Footnotes
Conflict of interest
None.