
Abstract
Purpose
Many markers of inflammation are increasingly found to have prognostic significance in some cancers. This study investigated the prognostic value of albumin/globulin (AGR), lymphocyte/monocyte ratio (LMR), and other inflammatory markers, including neutrophil/lymphocyte ratio (NLR) and platelet/lymphocyte ratio (PLR), in patients with papillary thyroid carcinoma (PTC).
Methods
We retrospectively analyzed the data of 764 patients newly diagnosed with PTC (608 women, 156 men) aged 10-83 years. Univariate and multivariate analyses were used to analyze recurrence rates and assess potential prognostic factors. Furthermore, we used random survival forests to construct a random survival forest score (RSFscore). The correlations between various inflammatory factors and traditional prognostic factors were analyzed. We also compared the areas under the curve (AUCs) of the RSFscore and 4 inflammation-based markers.
Results
AGR, NLR, PLR, and LMR were strongly associated with invasive clinicopathological features (tumor size, lesions, lymph node metastasis, and lymph node metastasis rate) and postoperative recurrence. In the multivariate analysis, AGR and LMR were independent prognostic markers for recurrent PTC. Higher NLR and PLR values indicated a higher risk of recurrence, while higher LMR and AGR values suggested a lower recurrence risk. The predictive power of the combined indicators was stronger than that of single indicators alone.
Conclusion
Compared to the analysis of a single indicator, the combination of inflammatory markers was more helpful in determining the risk of PTC recurrence, which has an important impact on predicting patients’ cancer-free survival and quality of life.
Keywords
Introduction
Thyroid cancer (TC) is a common form of cancer, with an estimated 43 800 new cases in 2022 and 2230 deaths. 1 More-over, the incidence of TC is increasing.2,3 Although deaths from TC are rare, cancer recurrence is an important factor affecting quality of life.4-6
Traditionally, the tumor-node-metastasis (TNM) staging system has been the most commonly used method to evaluate the prognosis of papillary thyroid carcinoma (PTC). 7 However, an increasing number of individual differences have been observed in cancer patients due to the individual heterogeneity or immune escape associated with the inflammatory response8,9; thus, evaluation methods such as the TNM system have limited reference values for recurrence in low-mortality cancers.
Recent studies have shown that chronic inflammation increases the risk of many malignancies, including PTC. During inflammation, inflammatory cells and their secreted inflammatory factors released are closely related to the microenvironment of TC, in which different cells play different roles. 10 Neutrophils, as inflammatory cells, promote tumor cells growth and invasion by producing cytokines and vascular endothelial growth factor (VEGF).11,12 Platelets can help tumor cells evade anti-tumor immunity and simultaneously secrete VEGF and platelet-derived growth factor (PDGF). Different proportions and degrees of lymphocyte infiltration reflect tumor progression to a certain extent, as well as the status of the patient’s immune system. 13 Thus, some markers of inflammation, including the neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), and lymphocyte/monocyte ratio (LMR), play prognostic roles in PTC.14-16
Inflammatory markers are widely found in TC, some of which are involved in cancer development and metastasis. In their evaluation of 151 patients with TC, Lee et al 17 reported significant reductions in NLR after treatment in patients with a low risk of recurrence, patients with stage I disease, and patients who responded well to treatment. These findings suggest the need to further explore the role of inflammatory factors.
However, the predictive power of these inflammatory cytokines (AGR, NLR, PLR, and LMR) for long-term prognosis and recurrence in patients with PTC has not been elucidated. Therefore, the current study investigated and explored the comprehensive prognostic value of different inflammatory markers, including AGR, NLR, PLR, and LMR, in an independent cohort of patients with PTC.
Methods
Patients
This study retrospectively reviewed the records of patients with PTC treated at the Second Affiliated Hospital of Nanchang University between August 2017 and January 2021. In total, 1704 patients with PTC were selected. The inclusion criteria were histologically confirmed PTC and complete data on preoperative levels of biochemical markers, including neutrophils, lymphocytes, platelets, monocytes, white blood cells, and globules. The exclusion criteria were: (1) obvious inflammatory activity or other diseases that may cause changes in inflammatory markers, such as familial adenomatous polyposis (FAP) and inflammatory bowel disease (n = 231); (2) other thyroid diseases such as hyperthyroidism, hypothyroidism, and Hashimoto’s thyroiditis (n = 185); (3) other histological thyroid cancers such as medullary thyroid carcinoma and anaplastic thyroid cancer (n = 147); (4) previous or simultaneous malignant tumors (n = 127); and (5) patients lost to follow-up (n = 250). All patients provided signed written informed consent after receiving an explanation of the study purpose. This study was also approved by the ethics committee (Ethics number:2 017 045). Ultimately, 764 patients were included in this study and were followed up by phone interviews (Figure 1). Recurrent patients were defined as those with new masses found on any imaging examination and confirmed by pathological biopsy or surgery. Disease-free survival (DFS) was defined as the interval from the date of surgery to the date of the diagnosis of recurrence or the end date of the follow-up (February 21, 2021). Papillary thyroid carcinoma patients exclusion flowchart.
Data Collection
Baseline data were obtained from outpatient records. All laboratory data (blood chemistry analysis) were acquired from patients within 7 days of surgery. Tumor data (tumor size, lesions, lymph node metastasis [LNM], and LNM rate) were obtained from patient pathology and color Doppler ultrasound reports. Unifocal and multifocal lesions were defined as only 1 lesion and 2 or more lesions in the pathological report, respectively. The LNM rate was calculated by dividing the number of lymph nodes detected by the number of metastatic nodes. The LMR was calculated by dividing the absolute lymphocyte count (normal values: (1.5-4) × 109/L) by the monocyte count (normal values: (0-.5) × 109/L), the PLR was calculated by dividing the absolute platelet count (normal values: (125-350) × 109/L) by the lymphocyte count, the NLR was calculated by dividing the absolute neutrophil count (normal values: (2-7) × 109/L) by the lymphocyte count, and the AGR was calculated using the equation AGR = albumin/(total serum protein-albumin) (normal values: (1.2-2.4)). Blood samples were collected from each patient 8-10 h before surgery and analyzed using a Sysmex XT-1800i automated hematology system. The laboratory data included neutrophil, lymphocyte, monocyte, and platelet counts. According to the National Comprehensive Cancer Network guidelines, the standard treatment in our study was total thyroidectomy.
Statistical Analysis
All statistical analyses were performed using R software (3.6.1). Mann–Whitney U and chi-square tests were used to analyze the differences between continuous and categorical variables, respectively. Receiver operating characteristic (ROC) curves were used to determine the optimal cutoff value of the variables, and the areas under the curves (AUCs) were used to reflect their predictive power. Univariate and multivariate Cox analyses were used to further analyze the predictive values of the variables. Random survival forest was used to build an integrated model based on decision trees. Kaplan–Meier (K-M) curves were generated to visualize the prognosis of the variables, and log-rank tests were used to determine the corresponding P-values. P-values < .05 were considered statically significant.
Results
Clinicopathological Features and Treatment Outcomes
The 764 patients with PTC in this study were randomly divided into training and testing sets in a 1:1 ratio using the sample function in R (Figure 2). The patients’ baseline characteristics are presented in Table 1. The mean age at diagnosis was 46.35 ± 13.15 years. The patients included 156 men (20.42%) and 608 women (79.58%). Previous studies have also shown that women have a higher risk of developing PTC than men.
18
In the current study, 257 (33.64%) patients had LNM, while 507 (66.36%) did not. A total of 569 (74.48%) and 195 (25.52%) patients had unifocal and multifocal lesions, respectively. Hypertension was present in 417 (54.58%) patients, while 347 (45.42%) patients did not have hypertension. The mean and standard deviation of tumor size (1.13 ± .84 cm), glucose (6.17 ± 1.64 mmol/L), LNM rate (.15 ± .27%), neutrophils (3.91 ± 1.33*109/L), lymphocytes (1.75 ± .54*109/L), monocytes (.29 ± .12*109/L), and platelets (234.89 ± 59.71*109/L) were listed separately. We also calculated the mean and standard deviation for the LMR (7.69 ± 12.63), NLR (2.44 ± 1.25), PLR (144.44 ± 52.38), and AGR (1.41 ± .21). We performed the same analyses on the training and testing sets. Furthermore, our evaluation of the effect of randomization using the Kolmogorov-Smirnov test showed no statistically significant differences among the groups (P > .05). The data analysis process of the article. Baseline characteristics of PTC patients. Abbreviations: AGR, albumin/globulin ratio; LMR, lymphocyte/monocyte ratio; LNM, Lymph node metastasis; NLR, neutrophil/lymphocyte ratio; PLR, platelet/lymphocyte ratio; PTC, papillary thyroid carcinoma.

Patient Grouping and Recurrence Analysis
The optimal cut-off values of the ROC curves were used to determine the effect of the 4 inflammatory markers in determining recurrence in the training set. The evaluation effect of the 4 markers with recurrence as the endpoint is shown in Figures 3(A)-3(D). We also calculated the optimal cut-off values for the 4 inflammation markers. The receiver operating characteristics curve of LMR (A), AGR (B), NLR (C) and PLR (D) for disease-free survival status among 382 atients with PTC in training set.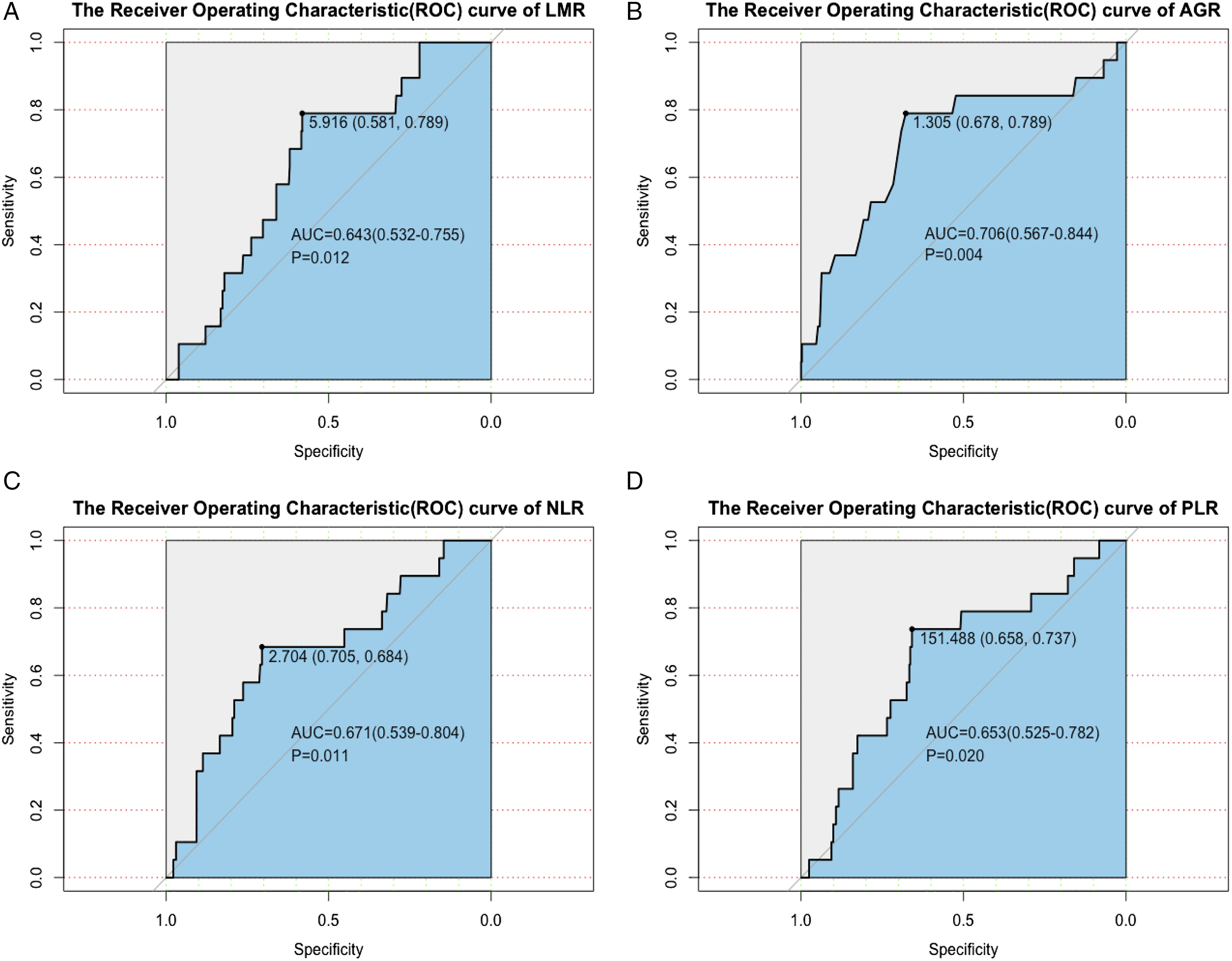
Previous studies have examined the predictive power of the LMR in patients with PTC. Yokota et alshowed that a low LMR was significantly associated with recurrence (P = .002). 19 Our results (P = .001) are consistent with those reported previously, further suggesting the strong predictive ability of the LMR. Other studies have also reported the strong ability of the NLR and PLR to predict PTC recurrence, 20 in line with our findings in 764 patients with PTC. While the prognostic effect of the AGR on renal and oral cavity cancers has been reported,21,22 its prognostic effect on PTC has not. Therefore, the current study is the first to report the effect of the AGR on PTC prognosis. The association between AGR and PTC recurrence warrants attention and may be a new direction for the study of PTC.
K-M analysis of DFS in the training set showed worse DFS rates in patients with lower AGR (P < .001) and LMR (P < .001) (Figures 4(A)-4(B)). The DFS rate in patients with higher PLR (P < .001) and NLR(P < .001) was lower than that in other patients (Figures 4(C)-4(D)). Pretreatment inflammation-based markers and prognosis of PTC patients in training set. (A) LMR<5.916 was associated with poor DFS rate (P < .001). (B) AGR<1.305 was associated with poor DFS rate (P < .001). (C) NLR≥2.704 was associated with poor DFS rate (P < .001). (D) PLR≥151.489 was associated with poor DFS rate (P < .001).
We also applied the same method to the testing set (Figures 5(A)-5(D), Figures 6(A)-6(D)) and the total set (Figures 5(E)-5(H), Figures 6(E)-6(H)). The results showed that the LMR, AGR, NLR, and PLR predicted cancer recurrence. Through multiple tests, we confirmed that inflammatory markers had strong predictive power for PTC recurrence. The receiver operating characteristics curve of LMR (A), AGR (B), NLR (C) and PLR (D) for disease-free survival status in testing set and that of LMR (E), AGR (F), NLR (G) and PLR (H) for diseasefree survival status in total set. Correlation between the level of 4 indicators and PTC recurrence in testing set (A-D) and total set (E-H).

Correlations Between Markers and Clinicopathological Characteristics
Correlation between inflammation-based markers and clinicopathological characteristics of PTC patients in training set.

Abbreviations: AGR, albumin/globulin ratio; LMR, lymphocyte/monocyte ratio; LNM, Lymph node metastasis; NLR, neutrophil/lymphocyte ratio; PLR, platelet/lymphocyte ratio; PTC, papillary thyroid carcinoma.
mean (standard deviation).
P < .05 considered as statistically significant.
Prognostic Significance of Inflammation-Based Markers in Patients with papillary thyroid carcinoma
PTC recurrence was defined as the recurrence of biochemical abnormalities and structural lesions after PTC surgery. The definition included local (residual thyroid), regional (central or lateral lymph nodes), and distant (lung or bone metastases) recurrence. All patients were followed-up via phone interviews.
Univariate Cox proportional hazards regression analysis for disease-free survival in PTC patients.

Abbreviations: 95%, CI 95% confidencel interval; AGR, albumin/globulin ratio; HR, hazard ratio; LMR, lymphocyte/monocyte ratio; LNM, Lymph node metastasis; NLR, neutrophil/lymphocyte ratio; PLR, platelet/lymphocyte ratio; PTC, papillary thyroid carcinoma.
P < .05 considered as statistically significant.

Multivariate Cox proportional hazards regression analysis for disease-free survival in PTC patients.

Abbreviations: HR, hazard ratio; 95% CI 95% confidencel interval, AGR, albumin/globulin ratio, NLR, neutrophil/lymphocyte ratio, PLR, platelet/lymphocyte ratio, LMR, lymphocyte/monocyte ratio, PTC, papillary thyroid carcinoma, LNM, Lymph node metastasis.
P < .05 considered as statistically significant.
Wen et al 23 studied the predictive value of inflammatory markers in elderly patients with PTC, but only showed the predictive value of LMR for patient prognosis and did not include AGR. The results of our analysis showed that AGR and LMR both independently and jointly predicted patient prognosis, which was a novel finding.
We further demonstrated the role of multivariate Cox 2 in prognostic analysis. As with the 4 inflammation-based markers, we calculated the AUC and 95%CI of the Riskscore (.860, .766-.955). Based on cancer recurrence, we also calculated the optimal cutoff values (2.039, .702-.895). Analysis of the Riskscore and PTC recurrence showed a significant association between the prediction and recurrence (P < .001) (Figure 7(A)). To investigate the association between the Riskscore and DFS rate, we grouped the patients according to the optimal cut-off. The results showed were statistically significant (P < .001), suggesting that the Riskscore could be used as a reference index for the prognostic analysis of PTC (Figure 7(B)). The predictive power of Riskscore on patient DFS status and DFS rate. (A) The receiver operating characteristics curve of Riskscore. (B) Riskscore ≥ 2.039 was associated with poor DFS rate (P < .001). (C) Comparison of the area under the ROC curves among Riskscore and the inflammation-based markers for prognosis of PTC patients.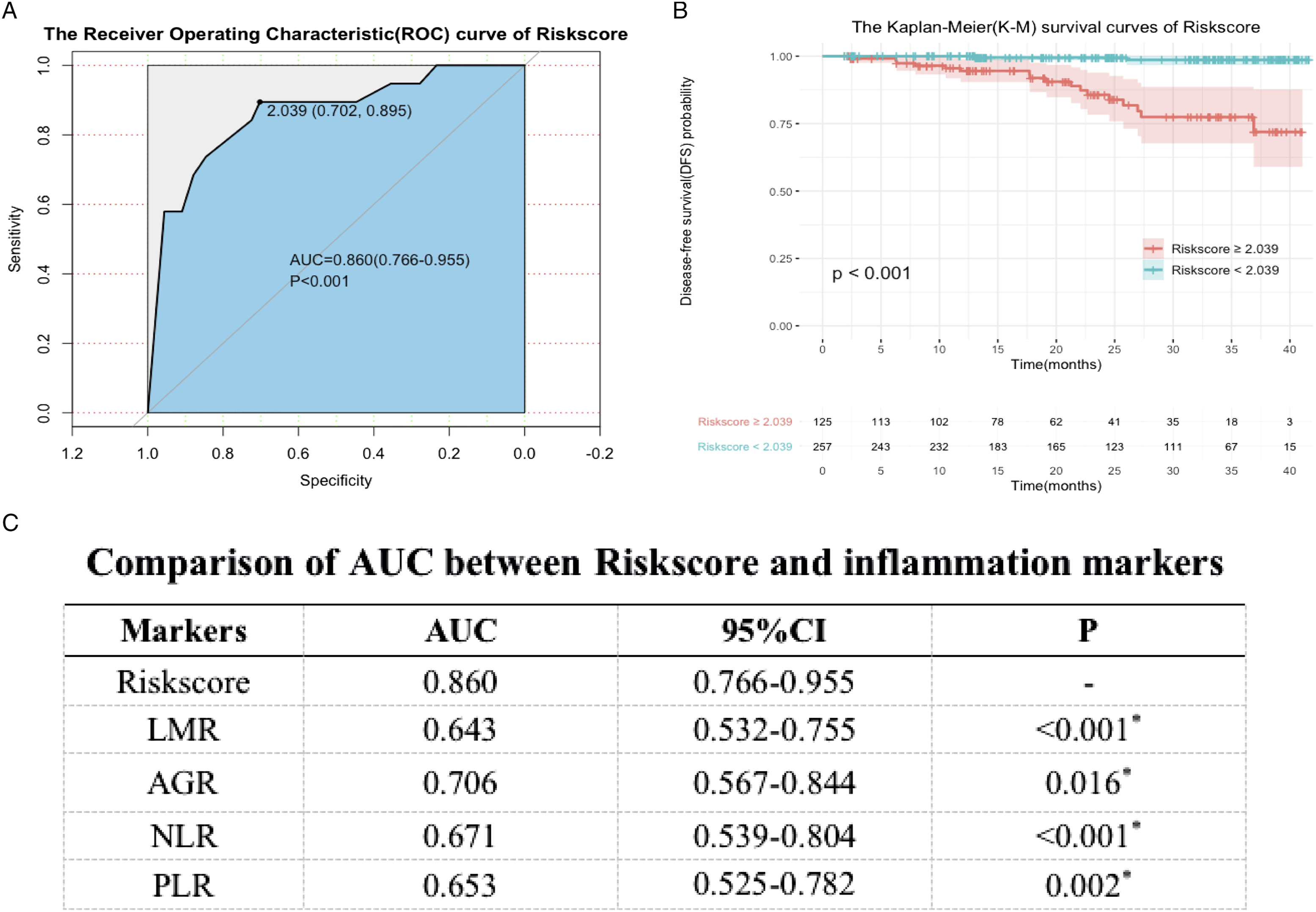
To assess differences in the predictive power of the Riskscore and inflammatory markers, we compared their AUCs (Figure 7(C)). The Riskscore had the highest AUC, indicating the best predictive power. Moreover, there was a statistical difference in the predictive ability between the Riskscore and LMR (P < .001), AGR (P = .016), NLR (P < .001), and PLR (P = .002), which further indicated that it had the best predictive ability.
As machine learning is a good method for the analysis of data associations, we also applied random survival forest (RSF) in the training set to build an RSFscore to predict PTC recurrence (Figure 8). We observed significant differences in predictive ability between the RSFscore and LMR (P < .001), AGR (P = .005), NLR (P < .001), and PLR (P < .001). The predictive power of RSFscore on patient DFS status and DFS rate. (A) The receiver operating characteristics curve of RSFscore. (B) RSFscore ≥.560 was associated with poor DFS rate (P < .001). (C) Comparison of the area under the ROC curves among RSFscore and the inflammation-based markers for prognosis of PTC patients.
We further evaluated the predictive ability of the 2 models in the testing (Figures 9(A), (B), (E) and (F)) and total (Figures 9(C), (D), (G) and (H)) sets. The results showed that the 2 models constructed in this study were applicable to the 2 datasets (P<.001). The receiver operating characteristics curve of Riskscore (A) and RSFscore (B) in testing set and that of Riskscore (C) and RSFscore (D) in total set. Correlation between PTC recurrence and the level of Riskscore in testing set (E) and total set (G) and that between PTC recurrence and the level of RSFscore in testing set (F) and total set (H).
Based on the selected prognostic factors, a nomogram was constructed to predict the 1, 2, and 3-year DFS rates of patients who underwent surgery (Figures 10(A)-10(C)). We found that the higher the LMR and AGR, the lower the NLR and PLR, without LNM, the smaller the tumor size and the unilateral lesion, and that the lower the Riskscore and RSFscore, the smaller the total score, indicating a better prognosis. Compared with NLR and PLR, LMR and AGR have a more significant impact on patient prognosis. The 1-year DFS rate was the lowest, while the 3-year DFS rate was the highest, consistent with previous studies. Thus, a shorter recurrence time was associated with a poorer prognosis in patients with PTC. Nomogram construction and evaluation for predicting 1, 2 and 3-year DFS in PTC patients. (A) Riskscore or RSFscore is not included in the nomogram construction for the 1, 2 and 3-year DFS probability prediction. (B) Riskscore is included in the nomogram construction for the 1, 2 and 3-year DFS probability prediction. (C) RSFscore is included in the nomogram construction for the 1, 2 and 3-year DFS probability prediction.
No previous combination analysis of inflammatory markers to determine prognosis in patients with PTC has been reported. Our results showed that the model had good predictive ability and was of practical significance in clinical practice. The combined effect of AGR and LMR in the analysis of patient prognosis suggests a deeper association between these measures. Therefore, the mechanism of AGR and LMR in the recurrence of PTC, as well as the interaction between them, requires further study. Moreover, the influence of AGR and LMR on cancer occurrence and development warrants future research.
Discussion
The results of this study demonstrated the association of inflammatory markers with recurrence and poor prognosis in patients with PTC. In predicting the prognosis of these patients, the combined values of various inflammatory markers showed significantly higher AUC values than in the past. To our knowledge, this is the first study to use the joint prognostic values of inflammatory markers for PTC recurrence.
Previous studies reported the association of patient sex with TC incidence and recurrence; thus, these studies tended to focus on female patients. 18 However, the results of the present study showed that although inflammatory markers were strongly associated with PTC recurrence, they were not associated with patient sex. Therefore, the effect of inflammatory markers on relapse may be universal. Various inflammation-based markers reportedly play prognostic roles in many cancers. Current studies have mostly focused on the mechanisms of inflammation and tumorigenesis 24 ; few have shown a link between markers of inflammation and cancer recurrence.
Our results showed that a variety of inflammatory markers (NLR, PLR, LMR, and AGR) were associated with common clinicopathological features that are considered malignant, including tumor size, lymph node metastasis, and advanced TNM stage. High NLR and PLR values indicated a higher recurrence rate, while high LMR and AGR values indicated a lower recurrence rate in patients. The combination of these measures showed significant prognostic value for patients with PTC.
The relationship between tumors and inflammation is generally considered an important mechanism of cancer development. The increase or decrease in different cell proportions directly or indirectly affects tumor prognosis.25-27
The results of the present showed significantly higher AUC values for AGR and LMR compared to those for the other indicators and that the combined values of various indicators helped improve the diagnostic efficacy of recurrence. No previous study has combined the predictive abilities of AGR and LMR to assess the prognosis of patients with PTC. Our results showed that these 2 measures had predictive ability both independently and in combination, which reflects the novel findings of our study.
Other factors may also affect the levels of inflammatory markers in the body after surgical treatment. In general, we believe that the level of specific inflammatory markers may greatly influence the risk of relapse. Since the underlying mechanisms by which some inflammatory factors have predictive power have not been clarified, we attempted to explain these mechanisms.
Abnormalities in the AGR may be associated with adverse effects or liver diseases. Albumin has been widely used to assess the prognosis of cancer patients, as malnutrition or liver disease can affect its synthesis.28,29 Regarding the LMR, lymphocytes play an important role in immune-related tumorigenesis. In general, they can induce tumor cell apoptosis and inhibit tumor cell proliferation and migration.19,20 Lymphocytes in the tumor microenvironment produce different degrees of infiltration to achieve anti-tumor effects. 30 Our results can be inferred from several other cancer-related risk factors. The association between LMR and AGR in cancer warrants further discussion.
The current study had several limitations. As a retrospective study, bias was unavoidable. In addition, the true recurrence rate in patients may be affected by the limited follow-up time. Multi-center data with larger sample sizes and longer-term follow-ups are required. In general, the occurrence of inflammation and cancer is a dynamic process, with different changes in the course of treatment, which is a new direction for future research. However, multi-center studies with larger sample sizes are needed to further verify our findings.
Conclusion
Our findings suggested that AGR or LMR are promising predictors, with better differentiating ability than other inflammatory markers. We believe that a combined diagnosis can better predict postoperative recurrence in patients.
Supplemental Material
Supplemental Material - Inflammation Markers Have Important Value in Predicting Relapse in Patients with papillary thyroid carcinoma: A Long-Term Follow-Up Retrospective Study
Supplemental Material for Inflammation Markers Have Important Value in Predicting Relapse in Patients with papillary thyroid carcinoma: A Long-Term Follow-Up Retrospective Study by Yanyi Huang Yushu Liu, Guoheng Mo, Tao Zhou, Qian Hou, Chaoqun Shi, Qunguang Jiang, and Yunxia Lv in Cancer Control
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (nfsc: 81660294).
Ethics Statement
This study was approved by the ethics committee of the Second Affiliated Hospital of Nanchang University.
Informed consent
All patients provided signed written informed consent after receiving an explanation of the study purpose. In addition, research principles outlined by the World Medical Association Declaration of Helsinki.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.