
Abstract
BACKGROUND:
Glioblastoma (GBM) is the most common and most fatal primary brain cancer in adults. Due to the complex nature of GBM, its pathogenesis still remain unclear. Accumulating evidence suggest that chemokine receptor CXCR7 contribute to the development of various types of tumors.
OBJECTIVE:
We aim to examine the prognostic significance of CXCR7 in GBM.
METHODS:
CXCR7 were first detected by Immunohistochemistry. The association between CXCR7 and overall survival (OS) were examined. Moreover, multivariate analyses were conducted to evaluate the prognostic factors in GBM.
RESULTS:
Of all 146 GBM patients recruited, 77 were in the high-expression subgroup, the rest 69 were in low-expression subgroup. There are no differences between these two subgroups in terms of age, gender, family history of cancer, extent of surgery, chemotherapy, radiotherapy, KPS, MGMT methylation status and tumor size. However, high CXCR7 expression was robustly correlated with poor OS in GBM. Multivariate analysis confirmed age, KPS scores, chemotherapy, IDH1 mutation, MGMT methylation and CXCR7 were independent factors in survival prognosis.
CONCLUSIONS:
CXCR7 may involve in the clinical GBM progression, and CXCR7 could be a valuable prognostic marker in the treatment of GBM.
Introduction
Glioblastoma (GBM), also known as Grade IV astrocytoma, is the most fatal primary brain cancer in adults with five-year survival rate of only 5% [1]. In most cases, GBM manifest very rapidly without any recognizable precursor lesions. Standard treatment includes complete surgical resection, followed by radiotherapy and adjuvant chemotherapy with temozolomide; however in most cases GBM relapses rapidly. Available GBM management at relapse are usually ineffective. As a result, the median survival of GBM patients with standard-of care treatment is only 15 months currently [2]. Although considerable progress has been made in the last several decades, the exact pathological mechanisms are still unclear and GBM remains an incurable cancer. Therefore, it is of great clinical value to identify the independent and significant prognostic biomarkers, not only improving poor prognosis but also providing promising therapeutic targets.
Chemokines are a group of homologous proteins that interact with G protein-coupled receptors [3]. Chemokines could bind to their receptors on target cells and trigger a series of signal transduction involving the release of intracellular calcium, the generation of inositol triphosphate and activation of protein kinase C [4]. The chemokine CXCL12, also known as SDF-1, regulates many important physiological functions like neuronal development, pro-angiogenic factor and stem cell motility [5]. CXCL12 and its receptor CXCR4 are highly expressed in various types of cancers [6], and play important roles in angiogenesis, proliferation and invasion [7, 8, 9]. In glioblastoma, CXCL12 and CXCR4 are also over-expressed and associated to the regions of angiogenesis and necrosis [10]. CXCR7, another receptor for CXCL12, is expression in many types of cancers such as breast, prostate and lung cancer [11, 12]. It is believed that the CXCR7/CXCR4 heterodimeric complex could enhance CXCL12 signaling and contribute to adhesion to endothelial cells and the inhibition of apoptosis [12]. Although CXCR4-dependent signaling pathway in tumorigenesis and metastasis is actively investigated; the expression of CXCR7 in brain tumor, especially in malignant GBM, has been poorly studied. Previous evidences have demonstrated that CXCR7 was expressed in glioma surgical specimens and various cell lines [13, 14]. In cell lines, CXCR7 was highly expressed and mediated anti-apoptotic effects [13], and targeting CXCR7 could inhibit glioma cell proliferation and mobility [15]. In mice and rats, it was also demonstrated that inhibition of CXCR7 extended survival of brain tumor [16]. Unfortunately, in human glioma specimens, there was no difference for CXCR7 mRNA expression between glioblastomas and non-tumor controls or low-grade gliomas [14]. Here, by examining the expression of CXCR7, our aim was to determine whether CXCR7 was an independent prognostic biomarker of overall survival (OS) in patients with GBM
Materials and methods
Patients and tissue samples
In this study, 146 pathologically proven glioblastoma specimens were obtained from Daqing Oilfield General Hospital between 2002 and 2014. Patients with follow-up information and pathological characteristics available were included; subjects without clinical tissues or incomplete clinical data, preoperative death, and previous treatment with any anti-cancer therapy were not included in current study. All tissues were obtained immediately after surgery. Overall survival (OS), which was calculated as the period from diagnosis until the date of death, was used for prognostic analyses in current study. The authors state that they have followed the principles outlined in the Declaration of Helsinki. In addition, the institutional ethical review board approved our clinical research, and written informed consents were obtained from all participants.
Immunohistochemistry (IHC)
Immunohistochemical analyses were performed as previously described [17]. Paraffin-embedded samples were sectioned with 4 um thickness, subsequently submerged in EDTA (pH 8.0) and autoclave at 120
Molecular methods
MGMT promoter methylation status was examined as previous reported [18]. In brief, DNA from paraffin sections was modified by sodium bisulfite, which converts unmethylated, but not methylated, cytosine to uracil. Modified DNA was submitted to methylation specific polymerase chain reaction (MSP).
A fragment of 129-bp length spanning the catalytic domain of IDH1 including codon 132 was amplified using sense primer IDH1f CGGTCTTCAGAGAAGCCATT and antisense primer IDH1r GCAAAATCACATTATTGCCAAC. Sequences were determined by ABI 3100 Genetic Analyzer (Applied Biosystems, USA).
Statistical analysis
Fisher’s exact test or student’s t test were used to assess the relationship between CXCR7 expression and clinic-pathological characteristics. The Kaplan-Meier survival curves was conducted to estimate overall survival. Survival differences according to CXCR7 expression were analyzed by the log-rank test. The influence of variables on survival was assessed using univariate and/or multivariate Cox regression analyses. All statistical analyses were performed with MedCalc (MedCalc, version 13.0, Belgium), and significance was defined as
Results
Patient characteristics
In current study, a total of 146 GBM patients fulfilled the inclusion criteria and were recruited. The main clinical characteristics of these participants were summarized in Table 1. Seventy-one of these patients were female, and the rest 75 subjects were male. The median age at diagnosis was 51.8 years (range, 15–75); the median follow-up was 8.5 months (range, 1–43). The mean Karnofsky performance score (KPS) was 82.7. Because of the risk of neurological deficits, 40 participants were only conducted partial resection in this study.
Clinical characteristics of patients according to the expression of CXCR7
Clinical characteristics of patients according to the expression of CXCR7
Data are shown as n (%) or mean
Using immunohistochemical techniques, CXCR7 expression was observed in the cytoplasm and the cell membrane of neoplastic cells (Fig. 1). Of all 146 GBM tissues examined, 69 were classified as low-expression, the rest 77 samples were high-expression. As shown in Table 1, there is no statistical differences between these two subgroups in term of age, gender, family history of cancer, extent of surgery, chemotherapy, radiotherapy, KPS, MGMT methylation status and diameter of tumor. Interestingly, compared with CXCR7 positive group, more IDH-1 Mutated patients were included in CXCR7 negative group (
Figure 2 showed the Kaplan-Meier survival curves of all recruited GBM subjects. The overall survivals of patients with high levels of CXCR7 were worse than those with low levels of CXCR7 (Fig. 2). Moreover, the multivariate Cox proportional hazard analysis were carried out to assess the potential prognostic factors (Table 2). These included age, gender, extent of surgery, KPS, diameter of tumor, chemotherapy, radiotherapy, MGMT methylation status, IDH-1 mutation status and CXCR7 expression; among which only age, KPS, chemotherapy MGMT methylation status, IDH-1 mutation status and CXCR7 were independent factors.
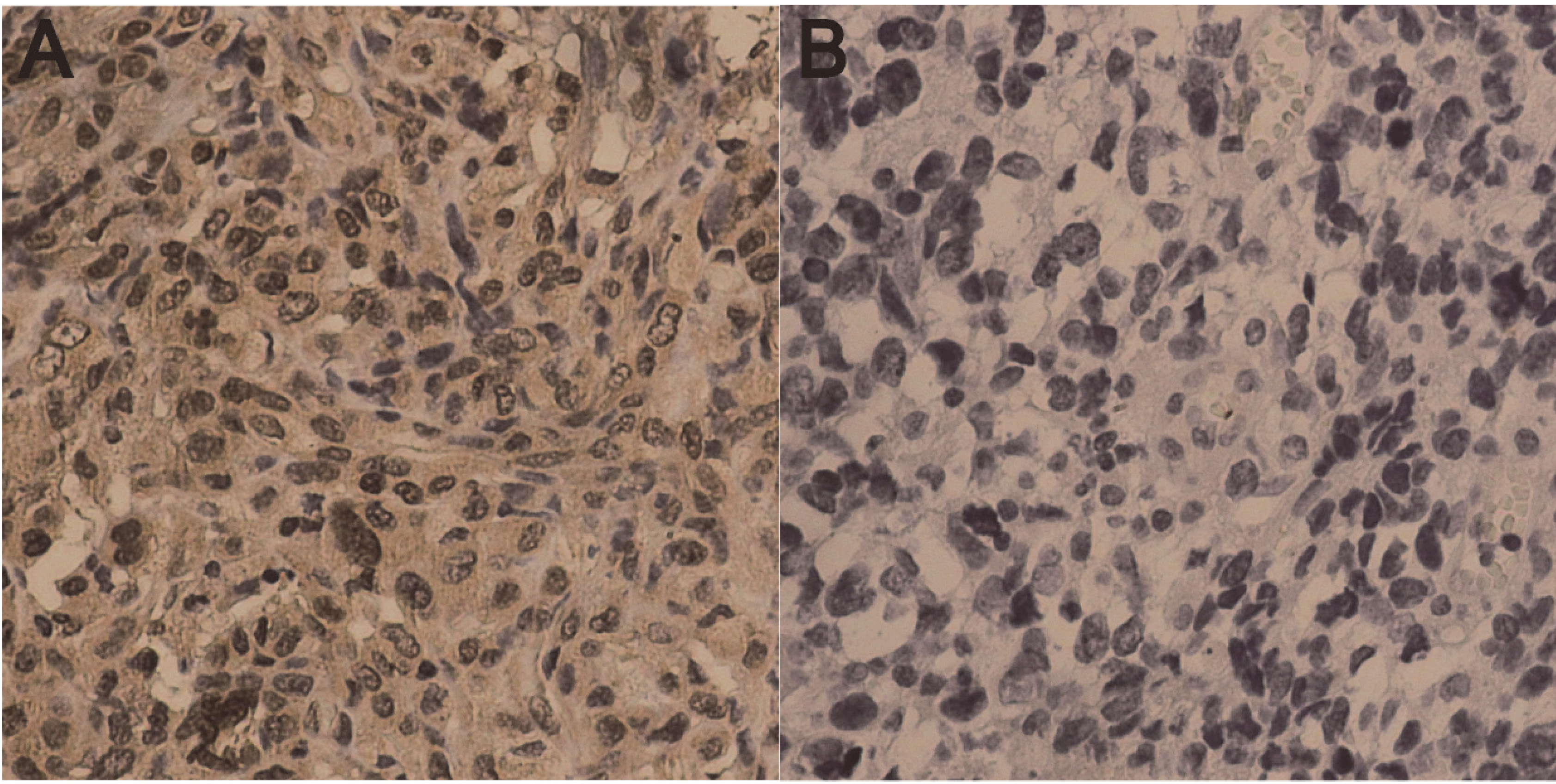
Representative samples with CXCR7 staining in human glioblastoma tissues (

Kaplan-Meier overall survival curves for CXCR7 expression in 146 glioblastoma samples.
Understanding the pathological mechanisms underlying GBM is important for developing target-specific medicines. CXCL12/CXCR4 axis has been implicated in the etiology of numerous types of cancers [7]. However, little attention has been devoted to the role of CXCR7, the second receptor for CXCL12, in the clinical significance of GBM patients. Here our data demonstrated that high level of CXCR7 protein was an independent biomarker of worse prognosis in GBM patients. It also might suggest CXCR7 is a potential therapeutic target in GBM treatment.
Multivariate analysis for overall survivals
HR, hazard ratio; CI, confidence interval.
The complex nature of GBM has not been completely elucidated, therefore only very few therapies could provide significant improvement in overall survivals currently. It has long been known that the heterogeneities in GBM patients are prominent, and early diagnosis and treatment do not always improve the clinical outcomes. However, with the increasing knowledge, GBM can be classified into different subgroups based on the molecular signature, and clinician are better understanding this lethal disease. Many predictive and prognostic biomarkers have been discovered that could contribute to the GBM management in clinic [19]. For example, IDH 1 and 2 mutation, MGMT promoter methylation and loss of heterozygosity 1p/19q have been proved to be important in GBM treatment and prognosis [20]. Other known characteristics that could affect OS include age, tumor histological grade, its location and KPS [21]. Even so, evaluation the clinical outcome of GBM was still very difficult. In this study, we mainly focus on the significance between overall survival and CXCR7 in GBM patients. Furthermore, the other OS prognostic characteristics, including age, gender, extent of surgery, KPS, diameter of tumor, chemotherapy MGMT methylation status, IDH-1 mutation status and radiotherapy were subjected to multivariate analysis. The results revealed that age, KPS, chemotherapy, MGMT methylation status, IDH-1 mutation status and CXCR7 were independent prognostic factors.
CXCL12 is a chemokine that is expressed in numerous types of tumor cells and involves in invasion and metastasis [9, 22]. For many years, CXCR4 is believed to be the unique receptor for CXCL12 and CXCL12 the only ligand for CXCR4 [23]. Moreover, CXCR4 has been discovered to be most widely expressed in various types of cancers and contributes to cancer cell proliferation, invasion, as well as in metastasis and survival [7, 8, 9]. Although CXCR7 showed ten-fold higher affinity to CXCL12 compare with CXCR4; little knowledge is available on the biological role of this newly discovered receptor. CXCR7 is absent or expressed at very low levels in most normal tissues, but presents in several different malignant cell types [24, 25]. Typical chemokine responses, such as modulation of adenylyl cyclase activity or intracellular calcium mobilization, are not generated after CXCL12/CXCR7 binding. It is originally believed that the major role of CXCR7 is to modulate the biological function of CXCR4 [26]. This opinion was now challenged by the discoveries that CXCR7 could elicit MAPK, Akt and JAK/STAT3 activation through a
In conclusion, the CXCR7 expression in GBM tissue is an important prognostic tool in predicting overall survival independent of the traditionally used clinicopathological characteristics. CXCR7 expression may be a valuable prognostic biomarker and worthy of further studies in other patient cohorts to validate our results.
Footnotes
Conflict of interest
None.