
Abstract
Little is known about breast cancer in Vietnamese women. Previous studies have reported the frequencies of prognostic factors of breast cancer in this population. The aim of this study was to examine the prognostic factors associated with the survival rates of patients with breast cancer treated at the National Cancer Hospital, Hanoi, Vietnam. We recruited 248 women with operable breast cancer treated with surgery and adjuvant therapy. Tumor tissue samples were stained by many immunohistochemical approaches and analyzed for estrogen receptor, progesterone receptor, and HER2 gene amplification status. A Cox model was used to determine the relationship between survival and the prognostic factors. The disease-free survival rate, overall survival rate, and cancer-specific survival rate were 75.8%, 80.6%, and 86.4%, respectively, at 5 years and 62.3%, 68.1%, and 78.9%, respectively, at 10 years. The lung was the most common metastatic site. Women with factors associated with a poor prognosis (eg, advanced clinical stage, high tumor grade, progesterone receptor [PR] negativity, HER2 amplification) had significantly lower survival rates. Patients with PR-negative breast cancer had significantly worse survival rates compared to those who were PR positive, according to multivariate analysis (hazard ratio = 1.77, 95% confidence interval: 1.01-3.11, P = .045); however, there was only a statistically significant difference in postmenopausal patients. The PR was a prognostic factor in postmenopausal women with breast cancer, but not in premenopausal women.
Introduction
Breast cancer is the most common cancer in women and is a major cause of cancer-related deaths in many countries. 1 There are, however, differences in its incidence, prognostic markers, and survival across ethnic groups. In the United States, the incidence of breast cancer among Vietnamese women is 55.5 of 100 000, which is lower than the rate for other ethnic groups, such as Chinese, Filipino, Japanese, and non-Hispanic white women. 2 In Hanoi (Vietnam), the incidence of breast cancer (per 100 000) is low at 17.5, which is considerably lower than that reported for Vietnamese women (36.6) living in the United States and for Caucasian Americans (98.7). 3
In Vietnam, findings from cancer registries in 3 regions of the country showed that breast cancer is the most common form of cancer in Vietnamese women, 4 but there are no nationwide data available on its incidence and prevalence. Breast cancer deaths account for 5.69% of all cancer deaths in Vietnamese women. 5 Recent reports from the United States showed that the mortality rates of breast cancer of US-born Vietnamese patients were the lowest among Asian populations and were much lower than that of non-Hispanic white women. 2,6 Similarly, it was also found that African American women had lower survival rates than European American women, even after adjusting for prognostic factors. 7 Breast cancer mortality has been declining in Europe over time with marked decreases observed in Northern countries that are attributable to early detection and treatment. 8
Very little data have been reported on breast cancer survival among women living in Vietnam. Two studies showed that premenopausal Vietnamese women benefited from oophorectomy plus tamoxifen. 9,10 In our previous studies, we have found that Vietnamese women tend to have breast cancer with a high frequency of poor prognostic factors among biological factors and present with more advanced stages of tumors compared to Swedish women. 11,12
The aim of this study was to examine the prognostic factors and the relative survival of patients with breast cancer treated at the National Cancer Hospital, Hanoi, Vietnam.
Patients and Methods
Study Population and Treatment
Two hundred forty-eight patients with primary breast cancer in clinical stage I to IIIb, operated on between June 2002 and October 2003, were recruited randomly from the National Cancer Hospital, Hanoi, Vietnam. Patients were treated with modified radical mastectomy or conservative surgery and axillary node sampling with a median of 10 lymph nodes excised (range: 6-35 nodes). Classification of histological type was defined according to the World Health Organization criteria. Tumor grade was assessed by the Elston-Ellis criteria. 13 Informed consent was obtained from all patients before treatment. Patients who underwent modified radical mastectomy were treated with adjuvant radiotherapy for tumors ≥3 cm at a dose of 50 Gy to the chest wall and 50 Gy to the axillary area if node positive. Patients who underwent a partial mastectomy were given 50 Gy to the entire breast and a boost of 60 to 65 Gy to the tumor bed. Patients with lymph node metastasis received adjuvant chemotherapy with anthracycline or taxane regimens delivered over 4 to 6 cycles. Of the 123 premenopausal patients with hormone receptor-positive tumors, 104 (84.5%) patients received endocrine therapy, including 74 patients with ovarian ablation by radiotherapy at a dose of 15 Gy; 11 of these patients became menopausal after chemotherapy, and 19 perimenopausal women were treated with tamoxifen alone. Postmenopausal women with hormone receptor-positive tumors were treated with tamoxifen at a dose of 20 mg daily for at least 2 but often for 5 years. In the first few years, all patients were followed up with physical examination, chest X-rays, abdominal ultrasounds, and blood tests for CA15.3 levels. Patients with symptoms suggesting metastasis were examined by computed tomography/magnetic resonance imaging scans or bone scans. The majority of patients were continuously followed up by examination at the National Cancer Hospital, but some patients living outside of Hanoi could only be reached by telephone. If a patient could not be contacted for an interview, her relatives were interviewed to clarify the reason for this loss of contact. The last day of follow-up was January 15, 2019, with a 99-month median follow-up (range: 4-192 months). Patients who were alive after the last day of follow-up were censored.
Tissue Assessment
All tumors were analyzed for hormone receptor content by immunohistochemistry in the Department of Pathology at the National Cancer Hospital, Hanoi, Vietnam. Receptor positivity was defined as >1% of stained nuclei, and patients with positive tumor(s) received endocrine treatment in the National Cancer Hospital. These tumors were also analyzed at Karolinska Hospital (Sweden) for hormone receptor content, HER2 expression, and rate of cell proliferation using an automated immunostaining platform and silver enhanced in situ hybridization procedures. The results of these analyses have been presented previously, 11,12 and these indicators were correlated with disease outcome in this study.
Statistical Analysis
The data were stored using SPSS software, version 19.0 for Windows (SPSS, Chicago, Illinois). Analyses were performed using SPSS and STATA version 10.1 (StataCorp, College Station, Texas). Differences in clinicopathological characteristics, including tumor grade, tumor size, lymph node status, and breast cancer subtype, were compared between premenopausal and postmenopausal patients and were examined using χ2 tests and odds ratios plus 95% confident intervals (95% CIs). Disease-free survival (DFS) was defined as the interval from the date of operation to the date of first detection of metastasis or contralateral breast cancer. Breast cancer-specific survival (CSS) was calculated from the date of the operation to the date of death for patients whose death was directly due to cancer. Overall survival (OS) was defined as the date of operation to the date of death from any cause or the last day of follow-up. Survival rates were estimated for patients according to potential prognostic factors using the Kaplan-Meier method and compared using log-rank tests. Univariate and multivariate Cox regression models were used to determine the relationship between breast cancer deaths and the prognostic and treatment factors. After the modeling process, the proportionality assumption was evaluated using Schoenfeld residual plots, and no violation was found. All tests were 2-sided and a P ≤ .05 was used as the significance level.
Results
Characteristics of the Patients Treated in 2002 to 2003
The median age of the study participants was 46 years (range: 26-72 years). From Table 1, it can be seen that 159 (64.1%) patients were premenopausal, 85 (34.3%) were postmenopausal, and 4 (1.6%) had unknown menopausal status at diagnosis. Among all of the patients, 10.5%, 70.6%, and 18.9% were in clinical stages I, II, and IIIa/b, respectively, and 227 (91.5%) patients had invasive ductal carcinoma, while 21 (8.5%) patients had other subtypes. The tumors were classified according to the Elston-Ellis system as grades I, II, and III in 9.2%, 71.3%, and 10.8% of patients, respectively. At the time of surgery, 109 (44%) patients had metastatic axillary node(s), and 76 (70%) of these patients were given chemotherapy. Hormone receptor-positive tumors (estrogen receptor [ER]+ and/or progesterone receptor+ [PR+]) were found in 164 (66.1%) patients, and 112 (68%) of these women were given tamoxifen. No patient was treated with Herceptin during the study’s time frame.
Comparison of Clinicopathological Parameters According to Menopausal Status.

Abbreviations: OR, odds ratio; Pre, premenopause; Post, postmenopause.
aDuctal and ductal carcinoma component.
bCompared for hormone-positive patients.
Survival and Clinicopathologic Factors
During the median observation time of 99 months, 48 patients died of breast cancer and 28 patients died of unknown causes. No autopsies were performed. Of the 171 (68.9%) living patients, 13 patients had evidence of recurrence/metastasis. One patient dropped out after confirmed metastasis. In addition, during the follow-up, one patient developed leukemia and another had Vaquez disease, but both were still alive at the end of the follow-up period. The DFS, OS, and CSS rates were 75.8%, 80.6%, and 86.4% at 5 years, respectively, and 62.3%, 68.1%, and 78.9% at 10 years, respectively. The lung was the most common site of metastasis in this population, followed by liver and bone (Table 2).
Metastatic Sites During Observation.

Table 3 shows the OS rates correlated with various clinicopathological and prognostic factors. The OS rates at 5 years and 10 years were significantly higher in premenopausal patients compared to postmenopausal patients: 84.5% versus 72.3% and 72.7% versus 58.9%, respectively (P = .03). Additionally, those with favorable tumor grades I and II, negative axillary nodes, and stages I and II tumors had significantly better survival (P = .029, P < .0001, and P < .0001, respectively). Table 3 also shows that patients with ER-negative or PR-negative tumors had poor OS after 5 years and 10 years compared to patients with receptor-positive tumors. In addition, patients with HER2-amplified tumors also had shorter survival times compared to those without amplified tumors.
Overall Survival Rate According to Prognostic Factors.
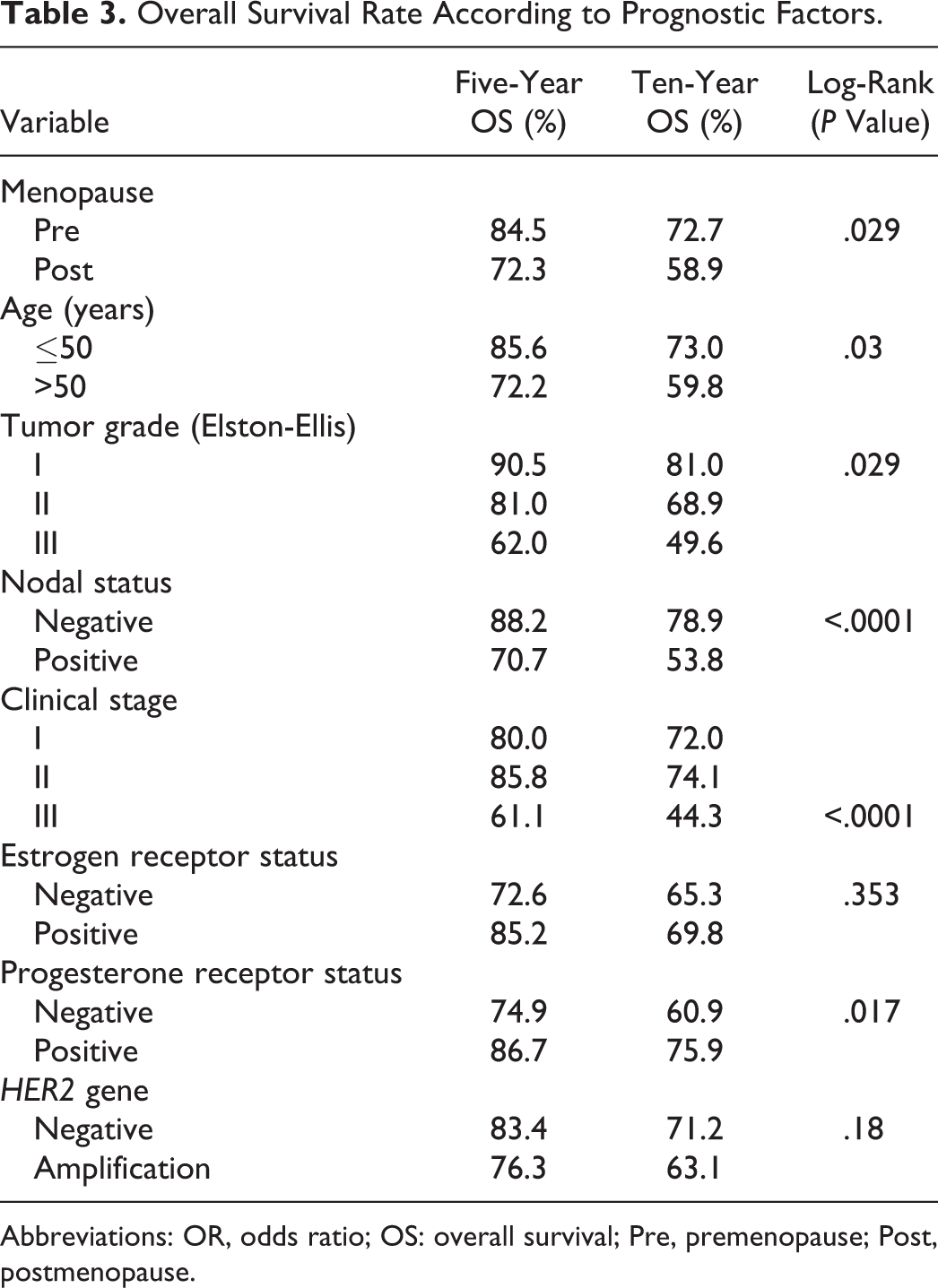
Abbreviations: OR, odds ratio; OS: overall survival; Pre, premenopause; Post, postmenopause.
A comparison of prognostic factors between pre- and postmenopausal patients can be seen in Table 1. Postmenopausal patients more often had factors indicating a poor prognosis, such as late stage disease, negative hormone receptor staining, and HER2 amplification. In the univariate model, premenopausal patients seemed to have better survival (hazard ratio [HR] = 0.61, 95% CI: 0.38-0.95, P = .03); however, this relationship was diminished in the multivariate model (HR = 0.67, 95% CI: 0.41-1.08, P = .10; Table 4). We found that patients with earlier stage disease (I/II) had better survival rates than those in a later stage (IIIa/b; HR = 2.45, 95% CI: 1.49-4.02, P < .0001). An improved survival rate for premenopausal patients was also seen as shown in Figure 1. Survival rates according to biological factors and menopausal status are displayed in Figure 2 as well. Patients with PR-negative tumors also had lower significantly survival rates than those with PR-positive tumors (HR = 1.77, 95% CI: 1.01-3.11, P = .045; Table 4). However, PR was an independent prognostic factor to survival in postmenopausal women, but not in premenopausal women.
Results of Univariate and Multivariate Analysis of Crude Survival Rate.

Abbreviations: CI, confidence interval; HR, hazards ratio; Pre, premenopause; Post, postmenopause; Ref., reference.
aSignificant.

Overall survival of operable breast cancers by menopausal status.

A, Comparison of overall survival by estrogen receptor (ER) and menopausal status. B, Comparison of overall survival by progesterone receptor (PR) and menopausal status. C, Comparison of overall survival by HER2 and menopausal status.
Discussion
It is estimated that more than 16 000 women in Vietnam are diagnosed with breast cancer every year. Vietnamese patients generally tend to be younger than Western patients at the time of diagnosis. It also seems that there are differences in tumor prognostic markers between Vietnamese and Swedish patients with breast cancer. 11,12
The 5-year OS in the current study was 80.6% for all patients, which is similar to that reported for France, 14 but lower than the survival rates of non-US-born Vietnamese patients living in the United States, which was reported to be 86%. 6 The 5-year survival rate of Vietnamese patients under 50 years of age who were treated in the National Cancer Hospital is similar to that reported in the eastern region of England (85.6% vs 85.0%) but was slightly lower after 10 years of treatment. 15 This observation might partly be explained by the fact that all patients in these studies were most likely treated in tertiary care hospitals capable of following treatment guidelines and offering up-to-date technology. However, the 5-year DFS in our study population was lower than that of Chinese patients in Hong Kong with similar stages of disease (75.8% vs 81.2%), respectively. 16
To our knowledge, this is the first study using active, long-term follow-up of pre- and postmenopausal women with breast cancers in Vietnam. We usually recommend that patients with breast cancer have regular checkups after treatment at the National Cancer Hospital in Hanoi. This follow-up was, however, difficult for patients living far from Hanoi. This distance resulted in a loss to follow-up of 10 (4%) patients during the study. Some patients also decided to go to their local hospital or to seek traditional medicine treatment. In fact, it appears that some patients did not seek medical attention at all, although they had various symptoms. We therefore believe that our data overestimate the DFS rate and, to some extent, also overestimate CSS, while the OS data are likely to be more robust. Vietnam began reporting national mortality statistics in 1992 based on community-level reports. However, the assessment of the cause of death in many patients is still unclear. 5 In the present study, 48 (63%) of the 76 patients who died had evidence of metastasis found through investigation at hospitals, making it possible to identify cancer as the primary cause of death.
More advanced treatment and early diagnosis have improved breast cancer survival in recent years. 2,7 In our study, variables including menopausal status, clinical stage, tumor grade, and various biomarkers were associated with survival. The lowest survival rates were seen in patients with advanced-stage, high-grade tumors and high rates of cellular proliferation. The stage of disease was the strongest prognosticator regardless of other factors. A report on breast cancer survival among Asian patients living in Malaysia and Singapore indicated a 5-year survival rate that was lower than that found in our study. 17 The survival rate was associated with both tumor characteristics and hospital setting. 15 Although ER and HER2 status in our study did not relate statistically to survival, it seems that patients with ER(−) and/or HER2 amplified tumors generally had poor survival. These findings are consistent with previous reports based on random samples of Asian or Western patients living in their countries of origin. 15,18 –21 However, it should be noted that the survival rate is dependent not only on clinicopathological features but also on the hospital providing the treatment. 15,22
As we reported previously, we found that there were different tumor cell characteristics of breast cancers between Vietnamese and Swedish patients. The differences were particularly remarkable in respect to the age of the patients. 11 Dabakuyo et al stated that the survival rate was lower in patients above 60 years or postmenopausal patients. 14 It has also been reported that the cancer mortality rate has increased with age in Northern Vietnam. 23 We found that postmenopausal patients had a significantly lower OS rate than premenopausal patients. However, postmenopausal patients were also more likely to have tumors with factors indicating a poor prognosis compared to premenopausal patients in this study. When adjusted for disease stage, hormone receptors, and HER2 gene status, we found that postmenopausal patients still tended to have a lower survival rate although the difference was not statistically significant.
Strengths and Limitations
Our findings are based on data from patients with breast cancer treated in a single institution with adequate therapies. All biological factors were assessed by advanced techniques and the tumor samples. Therefore, our findings might not reflect treatment outcomes in other hospitals in Vietnam. Further studies are needed on similar groups of patients across cancer centers throughout Vietnam to access the association between survival rates and prognostic factors.
Conclusions
We measured the survival rate of Vietnamese patients with breast cancer receiving multimodal treatments based on biological receptors. Although many patients had tumors with unfavorable prognostic characteristics, their long-term survival prospects were favorable. However, PR expression was found to be an independent prognostic factor in postmenopausal patients but not in premenopausal patients. These findings also suggest that we can potentially achieve greater effectiveness of adjuvant hormonal therapy in old women with breast cancer.
Footnotes
Authors’ Note
This work was approved by the ethical committee of the Hanoi Medical University, No 38/HMURB, 95/HMURB-extension (Vietnam).
Acknowledgments
We express our sincerest thanks to the nurses and doctors at the National Cancer Hospital, Hanoi, Vietnam, for help in assessing patient records, Sinclair H. Mantell for critically reviewing the English version of this paper, and Gaetano Marrone for guidance on statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from Sida/SAREC, Stockholm, Sweden, for a collaborative study between Hanoi Medical University (Vietnam) and Karolinska Institute (Sweden).