
Abstract
The purpose of this paper was to review the literature through a structured literature review and provide a grade of recommendation for patient safety, gait energy efficiency, and cost effectiveness of the C-Leg microprocessor-controlled prosthetic knee for transfemoral amputees. Medline (Ovid) and CINAHL (EBSCO) data bases were searched to identify potentially pertinent studies within the 1995–2009 time range. Studies were screened and sorted. Pertinent studies were rated for methodologic quality and for risk of bias. Following assessment of methodologic quality and bias risk, the level of evidence and a grade of recommendation was determined for each of three categories: Safety, energy efficiency, and cost effectiveness. A total of 18 articles were determined to be pertinent: seven for safety, eight for energy efficiency, and three for cost effectiveness. Methodologic quality was low with a moderate risk of bias in the safety and energy effectiveness categories. Studies in cost effectiveness received high scores for methodologic quality. Though methodologic quality varied across the selected topics, there was sufficient evidence to suggest increased efficacy of the C-Leg in the areas of safety, energy efficiency and cost when compared with other prosthetic knees for transfemoral amputees.
Keywords
Introduction
Presently there are an estimated 1.6 million persons living with limb loss in the United States. 1 Of these, 86% or approximately 1.3 million, have amputation of the lower extremity. 1 Twenty-six percent of lower extremity amputees, or slightly more than 357,000 individuals have a transfemoral level amputation. 1 Ninety-five percent of transfemoral amputations (TFA) are attributable to vascular disease. The remaining five percent of TFAs are attributable to trauma, malignancy, and congenital limb deficiencies. 1 There is a higher incidence and prevalence of dysvascular related amputation with advancing age and black individuals have the highest incidence of any particular group. 1,2
TFAs who achieve successful ambulation are more likely to do so with upper extremity aids and may develop an adapted gait pattern, even while walking on level ground. 3 It is important for amputees to feel stable and safe while walking with their prosthesis. It is also desirable to achieve the maximal functional level possible. Transfemoral amputees use a prosthetic knee for ambulation. Prosthetic knees are generally available with or without microprocessor control. Microprocessor-controlled prosthetic knees (MPK) are commonly equipped with sensors to continuously detect the position, range and forces acting upon the knee throughout the stance and/or swing phases of gait and other activities. Such sensors provide input to the microprocessor so that the knee can appropriately accommodate the particular activity or phase and velocity of gait. This allows virtually instantaneous adaptation to different walking speeds, terrain, and environmental conditions.
The Otto Bock C-Leg (Otto Bock; Duderstadt, Germany) is an MPK that controls stance and swing phase and adjusts to the requirements of the prosthesis wearer at a rate of fifty times per second. The addition of a microprocessor to rapidly regulate stance and swing phase could improve ambulatory functions such as safety and energy efficiency. Such technological advancements usually come at considerable cost to the healthcare system. It is necessary to evaluate such key features of a component and their cost effectiveness. Several studies have evaluated the safety, energy efficiency and cost efficacy of the C-Leg compared to other prosthetic knees. In some studies it has been reported to actually increase the level of function as well as independence. 4,5 The purpose of this literature review was to determine a grade of recommendation regarding safety, energy efficiency during gait and cost effectiveness of the C-leg for TFAs.
Methods
Search strategy
The Medline and CINAHL data bases were searched via the Ovid and EBSCO Host interfaces (respectively) on March 4, 2010. Primary search terms Microprocessor-Controlled Prosthetic Knees or C-Leg were searched independently and in combination with one of the following secondary search terms: Safety, Falls, Stumbles, Balance, Energy Efficiency, or Cost. Searches were pre-limited using the following criteria: English language, abstract available and peer reviewed (CINAHL only). In Medline, the ‘map term to subject heading’ feature was de-selected to eliminate a MeSH heading search. In CINAHL, a default Boolean search was used. A publication date of 1995–2009 was chosen in both databases as the C-Leg was introduced in 1997. 6 A manual search of journals identified by the Rehabilitation Engineering Research Center in Prosthetics and Orthotics' 2006 State of the Science Report 7 and known to the authors as highly relevant in prosthetics research, was also conducted in the event very recent publications or keywords missed important publications in Medline and CINAHL.
Screening
Resulting references were exported to EndNote (Thompson, CA) bibliographic citation software. Two reviewers independently screened resulting references according to inclusion/exclusion criteria and classified them as either: (i) Pertinent, (ii) not pertinent, or (iii) uncertain pertinence. Full-text articles were reviewed for all citations classified as pertinent or uncertain pertinence. Disagreements regarding citations of uncertain pertinence were resolved by the two reviewers independently reviewing full-text articles then discussing and agreeing on ultimate inclusion/exclusion.
Inclusion criteria
Must be a comparative study;
Study used objective/quantifiable outcome measures;
C-Leg MPK utilized in one arm of the trial;
Must address one or more of the three key areas of interest: safety, energy efficiency in gait, cost effectiveness.
Exclusion criteria
Endoprosthetic knee joints (Total knee arthroplasty/replacement);
Editorial, classification or taxonomy papers;
Paper does not address at least one of the three key areas of interest: Safety, energy efficiency in gait, cost effectiveness;
Duplicate publication.
Sorting by topic
Following screening, full-text articles were sorted by the two reviewers for specific pertinence in one or more of the three subtopics (safety, energy efficiency, and cost effectiveness).
Quality assessment
Once pertinent articles were screened and sorted, methodologic quality and risk of bias were independently assessed by the two raters in order to assist with determining the level of evidence to support the three topics of interest. The PEDro Scale was utilized to determine methodologic quality for the safety and energy efficiency topics. The PEDro Scale reportedly has fair to good reliability for application in rehabilitative clinical trials. 8 The scale results in a 0–10 score, with higher scores reflecting higher methodologic quality, based on 11 criteria. The first criterion is not scored. To receive a point in each of the remaining ten criteria, the criteria must be clearly stated in the study resulting in a ‘yes’ answer for presence of that item, and the awarding of one (1) point. If an item is not clearly stated, it receives a ‘no’ answer and receives no point for that criterion. A PEDro score of 6/10 or higher is considered to have high methodologic quality whereas scores lower than 6/10 are considered to have low methodologic quality. 8
Following the rating of methodologic quality, the SIGN 50 9 assessment forms (three forms) were utilized to: (i) Assess internal validity, (ii) assess degree of bias, and (iii) to extract useful data from the pertinent studies for the safety and energy efficiency topics (see Tables 1 and 2). Answers from the checklists are not weighted. The risk of bias is classified as either:
Low. All or most of the criteria from the assessment of internal validity are satisfied. Study conclusions would not likely be altered if methods were changed.
Moderate. Some of the criteria from the assessment of internal validity are satisfied. Study conclusions would not likely be altered if methods were changed.
High. Few or none of the criteria from the assessment of internal validity are satisfied. Study conclusions are likely or very likely to be altered if methods were changed.
To examine methodologic quality for the cost effectiveness topic, the PEDro scale and SIGN 50 assessment forms could not be used. Therefore, we used an internally consistent and validated grading system specifically for the assessment of methodologic quality of health economic evaluations. This grading system, while similar to many checklists, guidelines, and recommendations for economic evaluation and technology appraisal, has several advantages. The grading system is formally validated and can be used to rate economic evaluations on items related to both internal and external validity. A weighted numerical score can be derived to facilitate comparisons and allow users of economic evaluations to discriminate between lower and higher quality evaluations. 10 Sixteen evaluation criteria in this system were ultimately selected based on surveys of 120 international health economists including: Study objectives, design, perspective, data collection, time horizon, discounting, transparency, sensitivity analysis, and incremental analysis. Using weights on each of the 16 criteria a numerical score ranging from 0 (low quality) to 100 (high quality) is obtained. The numerical scores and major evaluation criteria for each economic study are listed in Table 3.
Following assessment of methodologic quality and risk of bias, the level and grade of evidence was determined by using the model designed by the Center for Evidence-Based Medicine. 11
Analysis
Due to heterogeneity in sample size, methods, accommodation periods, outcome measures and design, meta-analyses were not possible. Effect sizes (Cohen's D) 12 were calculated for all papers with available data using formulas based on independent t-tests. It is acknowledged that there is controversy in the use of this method versus a calculation that controls for the dependency of data. Effect sizes are typically larger when dependency of data is considered; limitations though are that more information is needed (for example the correlation coefficient between the data under examination). 12 As the articles reviewed had limited information, we chose to use the calculation based on independent groups, acknowledging that this is a conservative approach.
Results
Following pre-limiting, 45 articles were identified from the database search and three additional articles 5,13,4 from the manual search (Figure 1) for a total of 48 articles. Fourteen duplicate articles were eliminated in EndNote prior to independent screening leaving 34 citations for classification. Sixteen articles were ultimately classified as not pertinent, leaving 18 articles in the review. Of the 18 articles, seven were determined to be pertinent for the safety topic, 4,5,13,15–18 eight were determined to be pertinent for the energy efficiency topic 19–26 and three were determined to be pertinent for the cost effectiveness topic 14,27,28 (see Tables 1–3). The two raters independently achieved identical scoring for methodologic quality and risk of bias so no further statistical analysis was conducted on this.
Safety.
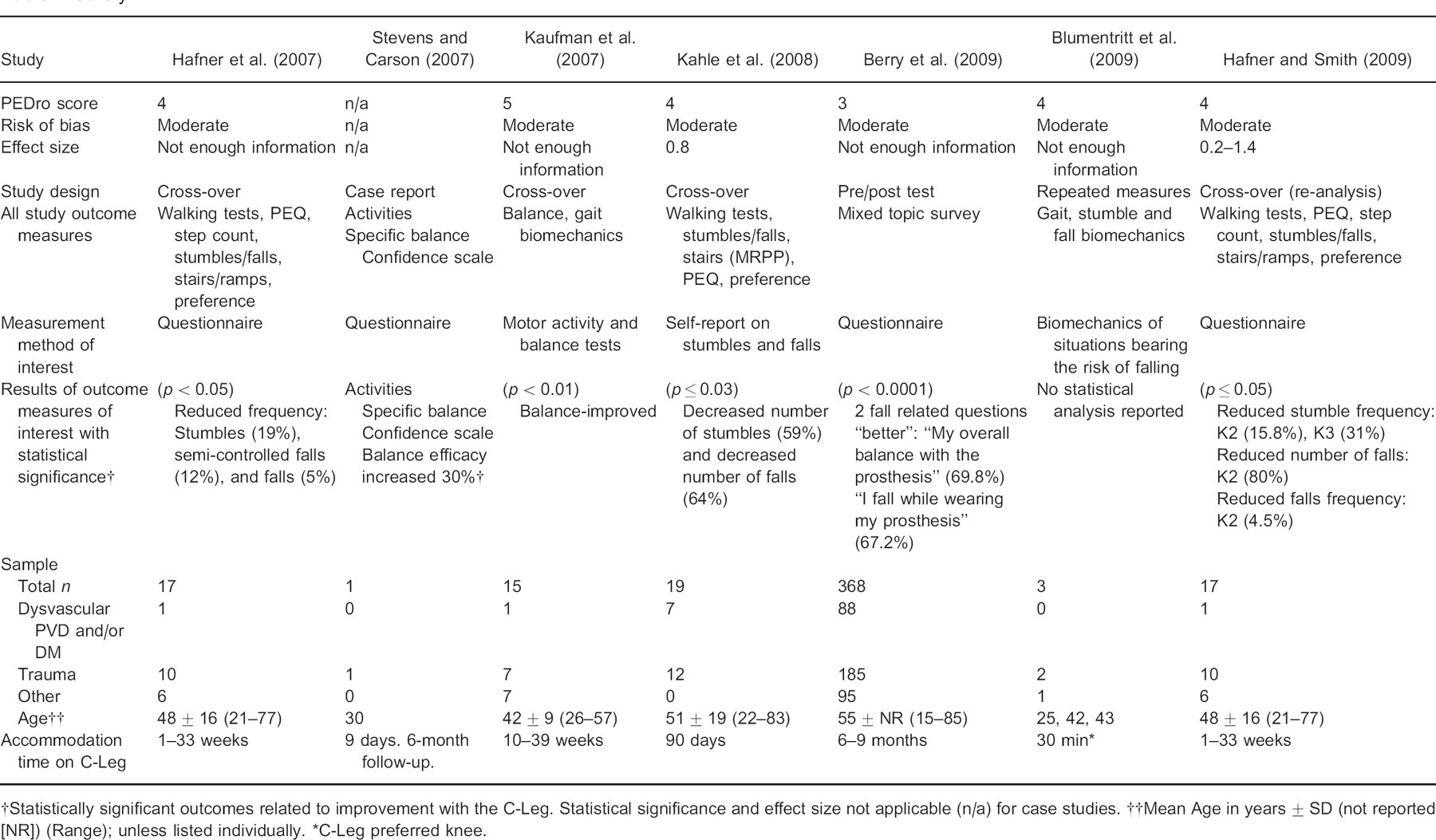
Statistically significant outcomes related to improvement with the C-Leg. Statistical significance and effect size not applicable (n/a) for case studies.
Mean Age in years ± SD (not reported [NR]) (Range); unless listed individually.
C-Leg preferred knee.
Energy efficiency.
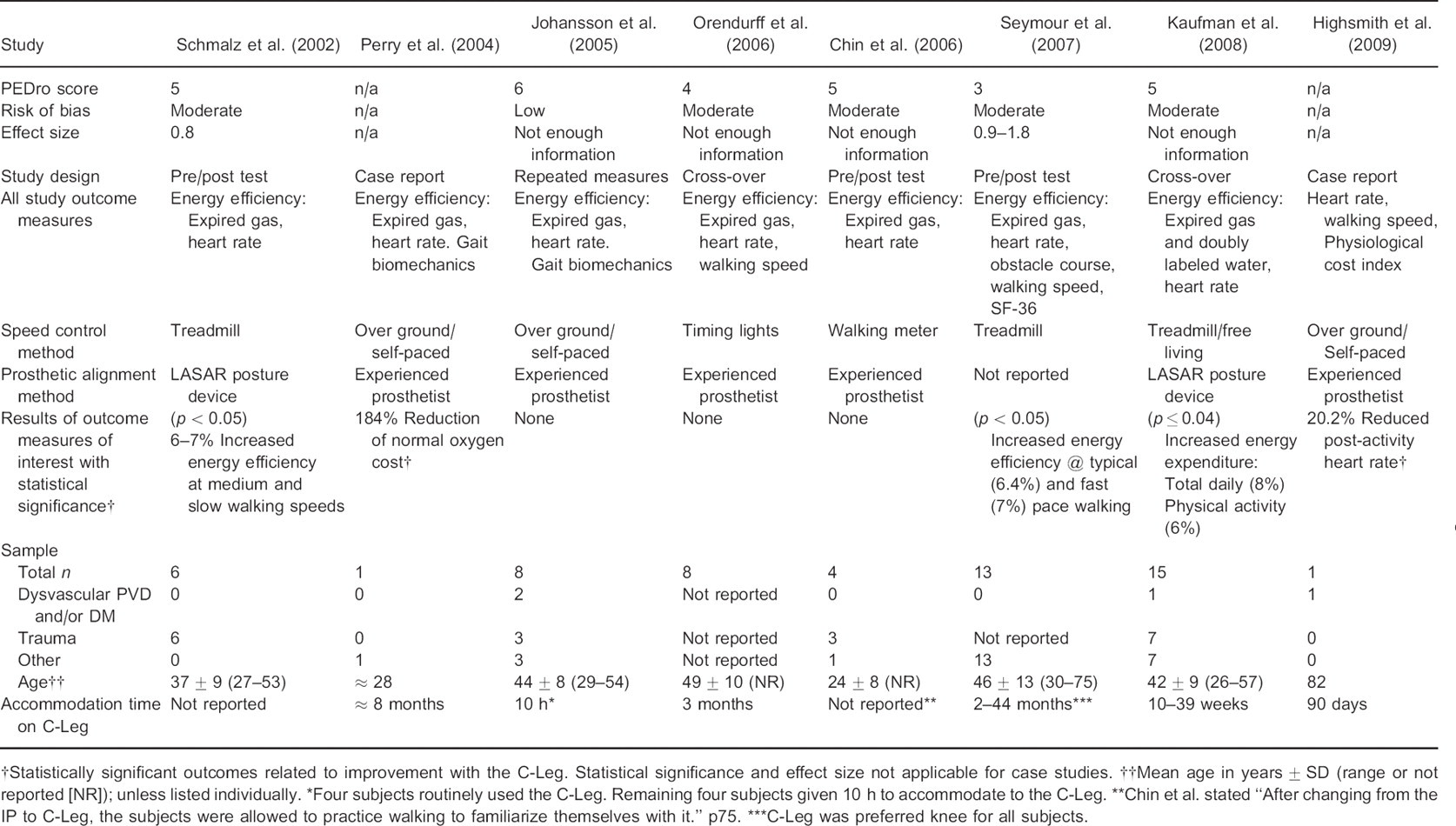
Statistically significant outcomes related to improvement with the C-Leg. Statistical significance and effect size not applicable for case studies.
Mean age in year ± SD (range or not reported [NR]); unless listed individually.
Four subjects routinely used the C-Leg. Remaining four subjects given 10 h to accommodate to the C-Leg.
Chin et al. stated “After changing from the IP to C-Leg. the subjects were allowed to practice walking to familiarize themselves with it.” p75.
C-Leg was preferred knee for all subjects.
Cost effectiveness.
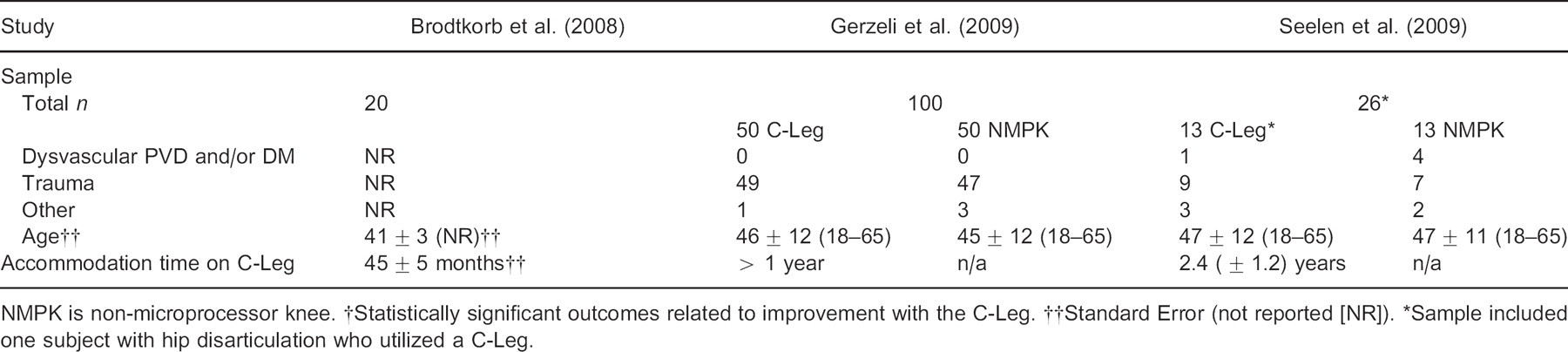
NMPK is non-microprocessor knee.
Statistically significant outcomes related to improvement with the C-Leg.
Standard Error (not reported [NR]).
Sample included one subject with hip disarticulation who utilized a C-Leg.
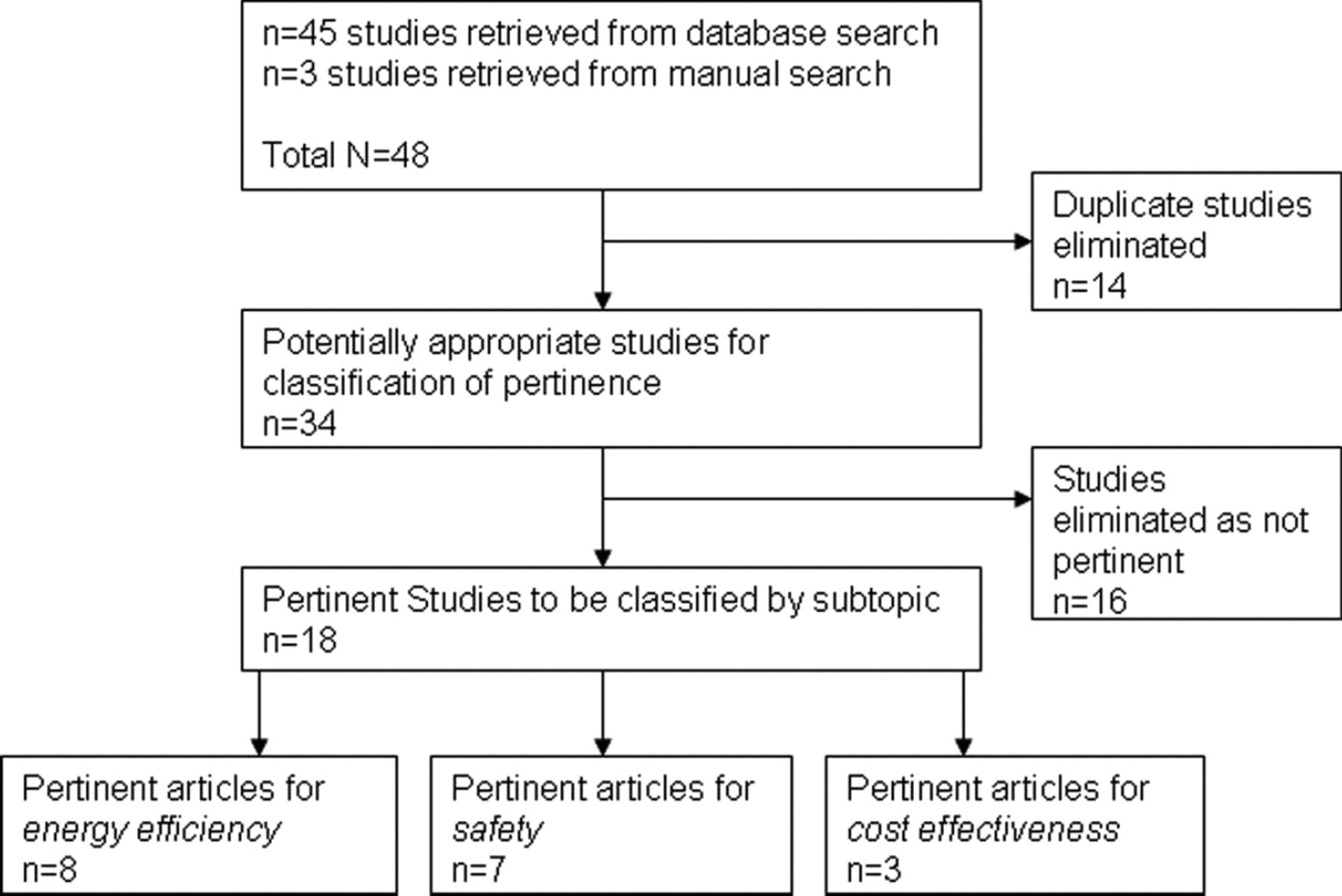
Flowchart showing selection of studies and results.
All seven papers in the safety topic received a PEDro score of ≤5/10 (low methodologic quality) and had a moderate risk of bias according to the SIGN 50. There was one case report that could not be scored for methodologic quality and risk of bias. All studies in the safety topic showed an improvement in some safety or surrogate safety measure with use of the C-Leg although statistical analyses were not available for two papers. 13,15 Effect sizes for the safety papers ranged from 0.2–1.4. Cohen 12 described effect sizes as small (0.2), medium (0.5) and large (0.8). Based on that definition, the studies that had enough information to calculate effect sizes showed large effect across the two treatments for all of the significant outcomes with the exception of uncontrolled falls (Cohen's D = 0.2). Refer to Table 1 for individual study scores of methodologic quality, risk of bias and effect sizes on the safety topic.
Of the eight papers in the energy efficiency topic only one 24 scored 6/10 on the PEDro scale (high methodologic quality) and had a low risk of bias (SIGN 50) whereas five received a PEDro score of ≤5/10 (low methodologic quality) and had a moderate risk of bias. Two 22,26 of these trials reported a statistical improvement in energy efficiency whereas four 19,21,23,24 reported some form of improvement in efficiency or speed that failed to reach significance. The final two papers in this section were case reports, both showing improvements in energy efficiency or a related measure but only minimally contribute to the level of evidence of this section. 20,25 Except for Orendurff et al. 23 and Johansson et al. 24 from the energy efficiency section, all studies in this entire review lacked randomization. All studies in the review lacked blinding. Effect sizes for the energy papers ranged from 0.8–1.8 resulting in large effect sizes with the intervention. The large effect size is only in regard to two of the eight papers 22,26 that reported significance on expired gas treadmill testing between knee conditions and also presented sufficient data to calculate effect size. Refer to Table 2 for individual study scores of methodologic quality, risk of bias and effect sizes on the energy efficiency topic.
The three studies 14,27,28 in the cost-effectiveness topic scored ≥81 out of 100 on Chiou's cost-effectiveness grading system. One study used a cost-consequence economic evaluation and the other two used cost utility. All three studies concluded that the C-Leg was a societally cost-effective prosthetic knee option. Effect sizes for total cost and utilities were calculated for the economic evaluation by Seelen et al., which was the only economic evaluation reporting standard deviations for both total cost and utilities. Effect sizes for utility ranged from 1.3 for both new and experienced prosthetic users to 1.5 for new prosthetic users only. Effect sizes for total cost ranged from — 0.2 for both types of users to 0.2 for new users only. Refer to Table 3 for individual study scores of methodologic quality and effect sizes on the cost efficacy topic.
It is important to note that there were no adverse events, safety concerns, detriments to energy efficiency reported in association with use of the C-Leg.
Discussion
Safety: Falls, stumbles & balance
Falls and fear of falling are significant health problems that are of interest to health professionals because they may indicate a decline in function. 29 Miller et al. 30 found that among community-living persons with lower extremity amputation, 52% had fallen in the past 12 months, 49% had a fear of falling, and 65% had low balance confidence scores. The fear of falling is one of the major factors for decreased activity, mobility, and quality of life. For the individual with TFA, selection of the appropriate prosthesis and knee mechanism can restore much of the ambulatory function that has been lost and have an impact on patient safety as it relates to stumbles, falls, balance and balance confidence.
Several studies have evaluated the effect of the C-Leg in safety or surrogate safety related outcomes. Kahle et al., 4 Hafner et al., 18 Hafner and Smith 5 observed persons with TFA transitioning from a non-MPK to a C-Leg prosthesis and used either a 60-day recall or self-report instrument (PEQ-A) to collect data on stumbles and falls. Kahle et al. reported a statistically significant reduction in the number of stumble (p = 0.006) and fall (p = 0.03) events in a sample of subjects with heterogeneous function and etiology. Subjects in this study reported an average reduction (59%) from seven to three stumbles and 64% reduction from three falls to one following accommodation with the C-Leg. 4 Hafner and Smith 5 reanalyzed prior data 18 by dividing their original group into Medicare Functional Classification Levels (MFCL) 2 and 3. In this reanalysis, MFCL 2 users reported a 15.8% (p = 0.05) reduction in the frequency of stumbles, a 4.5% reduction (p = 0.01) in the frequency of uncontrolled falls, and an 80% reduction (p = 0.01) in the number of uncontrolled falls. MFCL 3 users reported a 31% reduction (p = 0.03) in the frequency of stumbles.
Balance and balance confidence are believed to be related to and/or associated with falling and risk of falling in persons with TFA. 31,32 Kaufman et al. 17 directly evaluated balance using Dynamic Posturography; specifically the Sensory Organization Test (SOT) following subjects' accommodation with the C-Leg. Investigators reported that use of the C-Leg significantly improved balance performance (p < 0.01) as measured by a significantly improved composite score. Stevens and Carson 13 utilized the 16-item Activities-Specific Balance Confidence Scale in a case report where a subject transitioned from a mechanical knee to C-Leg. Following initial fitting of the C-Leg the subject reported a 30% increase in balance confidence. This was unchanged at six month follow-up. Using a 50 question multi topic survey, Berry et al. 16 evaluated balance more subjectively in two items. In these two items, “My overall balance with the prosthesis” and “I fall while wearing my prosthesis” respondents scored 69.8% and 67.2% “better” respectively, with use of the C-Leg. Also worthy of mention is that the two items of interest come from two separate sections from Berry et al.'s survey and each section was in total, statistically improved (p < 0.0001). 16
Collapse of the prosthetic knee joint can occur whenever the amputee is suddenly faced with any situation that creates an unanticipated risk of falling. It is during such instances that the safety properties of the prosthetic knee joint are critical if falling and the ensuing risks of injury are to be avoided. Blumentritt et al. 15 performed biomechanical tests in an instrumented gait laboratory to evaluate the safety of the C-Leg. They postulated that three biomechanical factors would be sufficient to assess the clinical safety of prosthetic knees: knee angle, knee moment, and hip moment. Test conditions included: Level ground walking at self-selected velocity, sudden stopping, sidestepping, stepping on an object and tripping by disrupting swing extension. In all conditions tested, the C-Leg never collapsed compared against the non-MPK prostheses, which either collapsed under some or all conditions, and were reportedly “unsafe”.
Five 4,5,16–18 of these seven studies (Table 1) provide consistent, statistically significant findings of improvements in self-reported reduction in stumble and fall events and improved balance. Additional non-statistically significant improvements support the latter findings and include knee stability in conditions resulting in collapse of other knees and improved balance confidence. 13,15 In total, these seven studies provide a grade “B” recommendation 11 that following accommodation with a C-Leg when transitioning from a non-MPK, subjects will recall experiencing a reduction in the number and frequency of stumble and fall events and have improved balance. It must be mentioned that while studies in this section achieved statistically significant improvements, methodologic quality was low and the risk of bias was moderate.
Energy efficiency
Transfemoral amputees are less efficient ambulators and demonstrate a 27–88% increase in energy cost during walking compared with intact individuals. 33,34 Several studies have compared the energy efficiency of walking with the C-Leg to that of other prosthetic knees, and in two pertinent cases, other MPKs. 19,21–26 Using expired gas analysis (Figure 2) and controlled walking conditions, the literature has conflicting results. Several authors have reported an increase in energy efficiency with use of the C-Leg that does not reach statistical significance. 19,21,23,24 Chin et al.'s study included the Intelligent Prosthesis MPK (Blatchford, Hampshire, UK) and reported a non-significant improvement with the C-Leg. 19 Johansson et al. compared the ambulatory energy efficiency of the Rheo knee (Ossur, Reykjavik, Iceland) to the C-Leg and found that the Rheo was more efficient, but the difference also did not reach statistical significance. 24 Contrary to these findings that do not reach statistical significance are study outcomes that do reach significance. Seymour et al. and Schmalz et al. both reported increased energy efficiency with C-Leg compared to non-MPK's at two differing walking speeds: typical (p = 0.05) and fast (p = 0.04) pace, and medium (p < 0.05) and slow (p < 0.05), respectively. 22,26
In two separate case studies comparing non-MPKs to the C-Leg, two unique patient circumstances were presented. These reports described setting activity intensity in a geriatric patient and quantifying rate of oxygen consumption in a bilateral TFA patient. Highsmith et al. 20 utilized a practical clinical assessment of heart rate to determine the efficacy of a rehabilitation program that included the C-Leg. Following the program the geriatric patient experienced a reduction in heart rate more conducive to daily activity. Perry et al. 25 also reported favorable outcomes regarding reduced oxygen consumption. Their subject with bilateral TFA was able to walk farther, faster, and with a lower oxygen cost compared with Mauch knees (Ossur, Reykjavik, Iceland) and stubby prostheses.
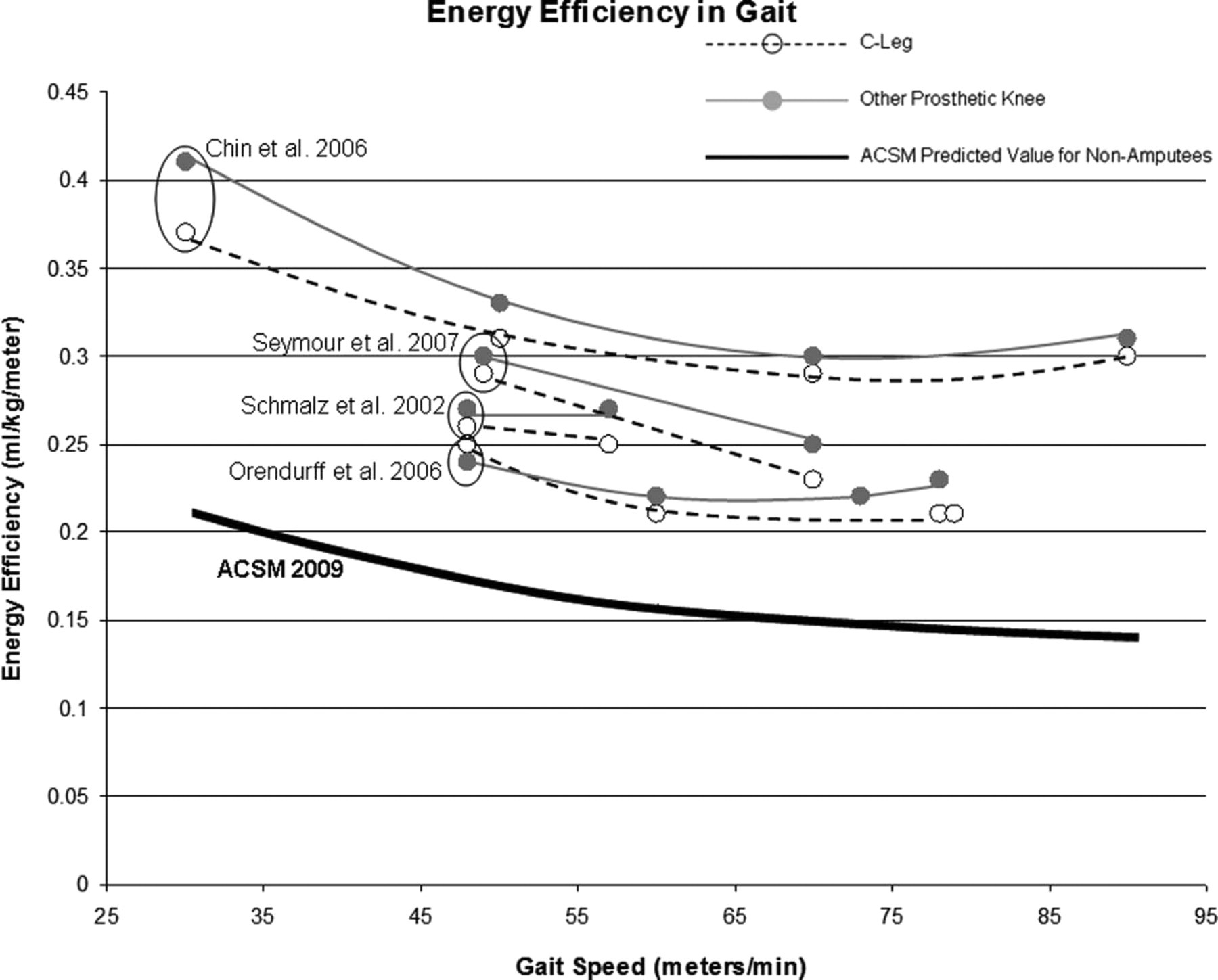
Energy efficiency plotted as a function of gait speed for studies providing the necessary data for graphing. C-Leg is plotted as dashed lines with open circles whereas ‘other’ prosthetic knees are plotted as solid grey lines and circles. For reference, energy efficiency of able-bodied non-amputee ambulation, as defined by the American College of Sports Medicine prediction equation, is plotted as the solid black line.
Seven of the eight studies in this section (Table 2) consistently showed increased energy efficiency while walking with the C-Leg compared to other knees. 20–26 However, only two reached statistical significance. 22,26 Two 23,25 of the four studies that could not demonstrate statistical significance did show an increased self selected walking speed, consistent with Kahle et al. 4 as well as increased total daily energy expenditure associated with increased physical activity. 21 Johansson et al.'s study was the only one in this section with high methodologic quality and a low risk of bias. 24 Using analysis of expired gas, in aggregate, seven of these studies provide statistically inconsistent evidence that the C-Leg improves energy efficiency while walking. 19,21–26 Additionally, one case report supports the finding of improved efficiency using measures of heart rate. 20 Because of the inability to consistently demonstrate a statistically significant increase in energy efficiency, these eight studies provide a grade “D” recommendation 11 in favor of using the C-Leg to increase energy efficiency during gait.
However, energy efficiency during gait does not predict activity of amputees during daily living. In order to determine amputee activity in their free-living environment, Kaufman et al. 21 measured total daily energy expenditure using the doubly labeled water method. This is the most accurate and robust method available to estimate energy expenditure in free-living conditions. 35,36 There was a statistically significant increase of 6% (p = 0.02) in the portion of total daily energy expenditure attributed to physical activity. This increased energy expenditure represented more physical movement rather than increased effort to walk because controlled condition energy efficiency while walking was found to be statistically equivalent in several studies. 21,23,24 Kaufman's conclusion that the C-Leg enables a free living activity increase is in contradiction to studies with step count which do not show increased activity. 18,37 Kaufman explained that the discrepancy is due to the fact that step counts do not reflect different metabolic requirements associated with changes in walking elevation or walking speed changes. This is an area that needs further exploration, and is a potential topic area for future review.
Cost effectiveness
The economic evaluations graded in this review were based in Europe (Sweden, Italy, The Netherlands) and each study evaluated cost and effectiveness from their respective healthcare system. All economic studies also evaluated cost and effectiveness from the societal perspective including productivity losses and patient/caretaker costs with the exception of Brodtkorb et al. 28 While each study reported some measure of utility, only Seelen et al. was classified as a cost-consequences study as no cost-utility ratio was reported. Even though Seelen et al. 14 did not report incremental cost-utility ratios of C-Leg vs. the comparator, the implied societal incremental cost-utility ratio for the Seelen et al. 14 study can be calculated based upon the reported cost and SF-6D values. The ratio of incremental cost to incremental utility in Seelen et al. is €52864/QALY (US$ 74697/QALY) and €65398 (US$ 92407) for first-time prosthesis users and repeat and first-time users combined. These results suggest that depending upon the distribution of new prosthetic users and previous prosthetic users in the eligible population the cost will vary and hence the cost-effectiveness of the C-Leg.
All of the studies reporting societal cost-effectiveness data found that C-Leg is the dominant prosthesis strategy providing lower societal cost and a positive QALY gain from C-Leg adoption. Brodtkorb et al. 28 reports a health system perspective incremental ratio of €3218/QALY (US$ 4560), falling well within standard cost-effectiveness thresholds. Given the negative societal incremental cost-utility ratios and the higher cost of the C-Leg, cost saving in these studies must be accomplished via higher productivity loss, patient/family caretaker costs, and household assistance costs associated with non-electronic prostheses. Gerzeli et al. 27 report productivity losses using the human capital approach as being over 40% higher for the mechanical knee group. Seelen et al. 14 also find lower productivity cost for the C-Leg group but also higher housekeeping assistance cost associated with the non-electronic knee joint group. In total, these three studies provide a grade “B” recommendation 11 that provision of a C-Leg is cost effective from a societal perspective and provides a positive QALY gain. Further research on differences in the duration of time to employment and on housekeeping assistance requirements during rehabilitation needs to be conducted to determine if these cost-effectiveness results are robust.
Several limitations regarding these studies and the grading system should be noted. First given the limited number of economic evaluations caution should be exercised in interpretation of the incremental cost-utility ratios. While sensitivity analysis was performed in all of the studies reviewed, the studies reporting cost saving from the societal perspective did not perform sensitivity analysis on those costs most likely to change the decision rule if varied, namely productivity, family/patient, and housekeeping assistance costs. In some cases these cost differences were insignificant and this should be examined by careful sensitivity analysis of these parameters. Relatively sophisticated sensitivity analysis was performed by Brodtkorb et al. 28 but they did not report societal costs and the study was penalized in the grading system by relying upon expert opinion for key parameters in the model. Secondly all of the current economic studies on C-Leg are set in countries within healthcare systems that vary from country to country. The differences in the structural characteristics of each country's healthcare system make the comparability of the results tenuous. Further studies will need to be performed in different country settings on the cost-effectiveness of the C-Leg. Finally there are some limitations to the grading system used to score the economic evaluations. While the system is flexible with regard to the variety of evaluations one finds in economic studies of new medical technologies, the scoring system is less able to distinguish quality among studies that score in the good to excellent range. 10 Each study is ranked dichotomously on each of the 16 criteria but each study reviewed performed at differing levels of quality on key criteria including transparency, sensitivity analysis, data quality, and conclusions. Each study clearly had strengths and weaknesses but all studies included key elements necessary for a sound economic evaluation.
Study limitations
This review of the literature is limited in that it is not fully inclusive of all studied aspects of the C-Leg as compared to other knees. While conducting this review the following areas emerged as future potential literature review topics but were classified as “not pertinent” for our a priori areas of interest: Perceived function (i.e., the Prosthesis Evaluation Questionnaire, patient preference and body image) and biomechanical measures (i.e., gait on flat ground, stairs and ramps). Additionally, amputees of dysvascular etiology were not represented at levels commensurate with estimates from epidemiologic studies, 1,2 which limits generalizability of results to this sub-group. Finally, it was observed that numerous variables were not controlled or standardized across studies. Examples include functional level and its rating, accommodation time, control knees, methodologies and selection of outcome measures. This variability across studies prevents the ability to conduct meta-analyses.
Conclusion
There was sufficient evidence to suggest increased efficacy of the C-Leg in the areas of safety, energy efficiency and cost when compared with other prosthetic knees for transfemoral amputees. Regarding safety, available evidence supports a grade “B” recommendation that following accommodation with a C-Leg, users will experience a reduction in stumble and fall events and have improved balance. Use of the C-Leg for the purpose of improving energy efficiency is supported by a grade “D” recommendation. However, research has shown that amputees spontaneously increase their physical activity in the free-living environment when using the C-Leg compared to a non-microprocessor controlled knee. So, energy efficiency may not be of primary relevance. Finally, evidence supports a grade “B” recommendation that the C-Leg is cost effective and worth funding. Based on standardized review criteria, methodologic quality could be improved and the risk of bias minimized with improved study design, decreased attrition, and use of double blinding for microprocessor-controlled knee prosthetic studies. While these are worthwhile goals, the practicality of some of these methodological changes in prosthetic research is currently unrealistic. 38,39 Specifically, patients recognize differing prosthetic components and the different prosthetic knees need to be aligned differently, which makes it unrealistic to conduct double-blind studies. 38 So, given these constraints, the grades of recommendations demonstrate that the C-Leg is a clinically significant improvement for transfemoral amputees.