
Abstract
Background: One of the main indicators of the suspension system efficiency in lower limb prostheses is vertical displacement or pistoning within the socket. Decreasing pistoning and introducing an effective system for evaluating pistoning could contribute to the amputees’ rehabilitation process.
Objectives: The main objective of this study was to review existing research studies that examine the occurrence of pistoning in lower limb prosthesis with different techniques in static (standing) and dynamic (walking and jumping) positions.
Study Design: Literature review.
Methods: Keywords related to slippage, suspension, pistoning and vertical movement in lower limb prosthetics were used to search the literature available in PubMed, ScienceDirect, Web of Science and Google Scholar databases. Sixteen articles were selected for further analysis according to the selection criteria.
Results: The following methods have been used to measure the occurrence of pistoning in prosthetic limbs: radiological methods, photographic technique, motion analysis system, sensor and spiral computerized tomography (CT). Pistoning was measured both in standing and walking.
Conclusions: The results of this review reveal that further research is needed to develop and evaluate easy, accurate and safe methods of measuring pistoning. Future studies should provide a gold standard for the acceptable range of pistoning in a prosthetic socket.
This literature review contributes to a further understanding of lower limb prosthetic biomechanics by highlighting the strengths and weaknesses of the techniques that are currently available for evaluating the occurrence of pistoning in a prosthetic socket. It provides a useful overview of the current methods of measuring residual limb movements relative to the socket and liner, and will be of use for both practitioners and researchers in prosthetics and orthotics fields.
Background
Suspension systems are utilized as a means of attaching upper and lower prosthetic limbs to the body.1–3 There are several different systems available for lower limb prostheses, which include cuff, supracondylar/suprapatellar socket (SC/SP), rubber sleeve, elastomeric liners, suction socket and elevated vacuum. In addition, recent developments in osseointegration allow the direct attachment of prosthetic components to the residual limb,4–10 which will not be considered in this review study. Prosthetists are required to determine the suitability of a suspension system by considering the level of amputation, the residual limb condition and the amputee’s average activity levels.
The suspension system and socket fit utilized in prosthetic devices play significant roles in the prosthetic function, the patient’s mobility and the amputee’s overall satisfaction with a device.11–14 According to research findings and amputees’ statements, prosthetic fit and suspension are closely interrelated in terms of both the levels of comfort experienced by the patient, and the functional efficiency of the prosthesis.15–17 For instance, many studies have revealed that silicone liners are the preferred suspension systems for many lower limb amputees because they provide good suspension, improved function and a robust fit within the socket. Patients’ comfort and satisfaction were also higher with this system than they were with conventional suspension systems, such as the belt used with the patellar tendon bearing (PTB) socket.5,17–18
The forces (e.g. ground reaction force and torque) exerted on the lower limb during standing and walking can displace the prosthetic limb on the stump. This displacement often occurs during the swing phase of gait and is reversed when the limb is bearing weight during stance. 3 The occurrence of pistoning or vertical movement inside the socket is often considered to be one of the most effective indications of whether a suspension system has been successful or unsuccessful to retain the lower limb prosthesis.3,19 Poor suspension has negative effects on the residual limb skin, amputee’s gait and comfort levels.20–27
Researchers have been working on the development of new suspension systems that can increase the options available to clinicians.4,28–29 The ability to measure pistoning helps when evaluating the quality of a suspension system in a lower limb prosthesis.30–33 Many different methods have been utilized for measuring pistoning movement of the stump or the position of the bone. These include radiography,21,34–35 photographic method,29,36–37 motion analysis technique, 38 and spiral computerized tomography (CT). 32 Photoelectric sensor has been also deployed. 33
Despite its importance and impact on the performance and patient’s satisfaction with a prosthetic device, pistoning in lower limb prosthesis has not been widely studied. At present, the available literature on the socket fitting and suspension is mainly focused on pressure distribution,39–45 shear force46–49 and friction.34,50–52
The objective of this study was to summarize the literature that addresses the occurrence of pistoning in lower limb prosthesis. The objective data were evaluated with regard to the methods that have been used for assessing pistoning during static (standing) and dynamic (walking and jumping) conditions with different prosthetic suspension systems.
Methods
Search
The following keywords were used in the PubMed, ScienceDirect, Web of Science and Google Scholar database search to find suitable research papers: prosthetic pistoning, stump vertical movement, residual limb slippage, and prosthetic suspension.
Selection criteria
Peer-reviewed papers were selected. Only experimental studies were of interest for this paper and, as such, subjective studies that were completed via the use of questionnaires and finite element study designs were excluded. The study design, method of subject selection, research tools, protocol and outcome parameters were reviewed.
Results
Search results
A total of 285 research papers were identified via the above-mentioned search engines. An additional 10 papers were also found by checking the references of the search results. The title and abstract of each individual study were assessed. Some of these 295 papers were computational models, were conducted on the upper limb prosthetics, dental prosthetics and implants, or were common between the databases; these were subsequently excluded. After refinement based on the above-mentioned selection criteria, 21 related papers remained, from which three articles were subjective studies. These were disregarded and 18 experimental papers were selected for the purposes of this review according to the inclusion criteria.
The study population, prosthetic specifications and data presentation of each paper are summarized in Tables 1, 2, and 3.
Characteristics of subjects in the studied literature.
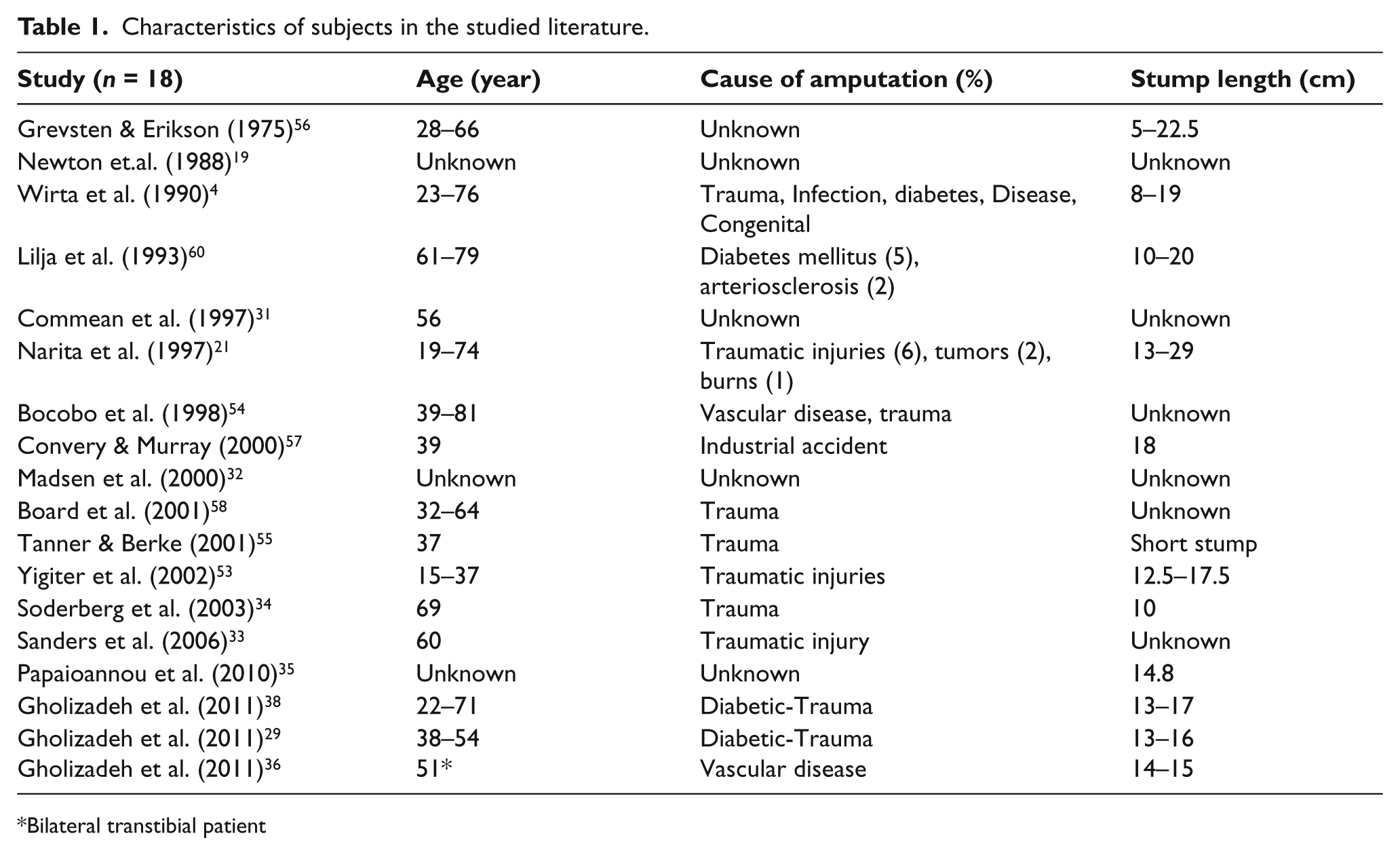
Bilateral transtibial patient
Study population.
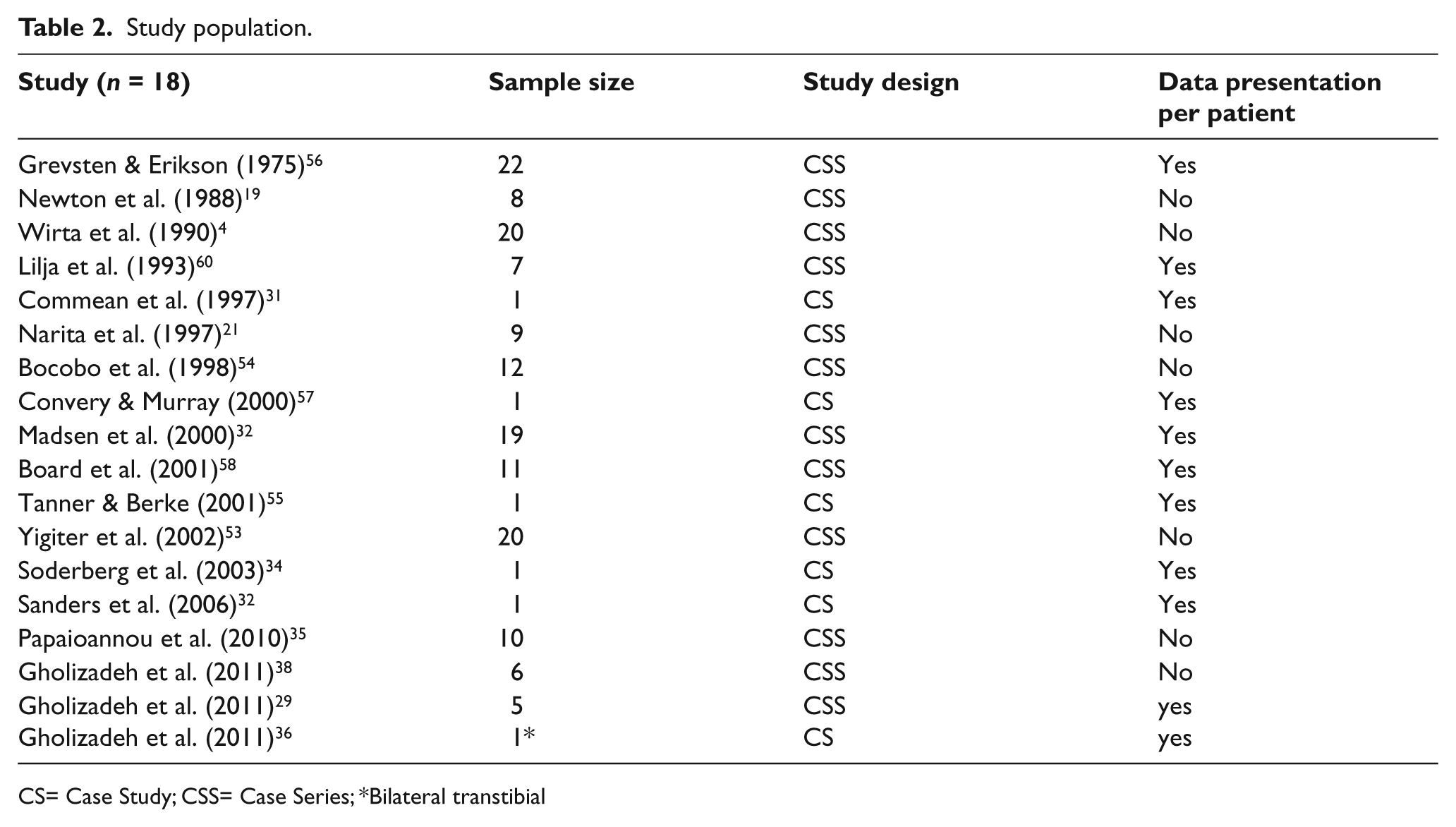
CS= Case Study; CSS= Case Series; * Bilateral transtibial
Distribution of articles based on the methodology and prosthetic components.
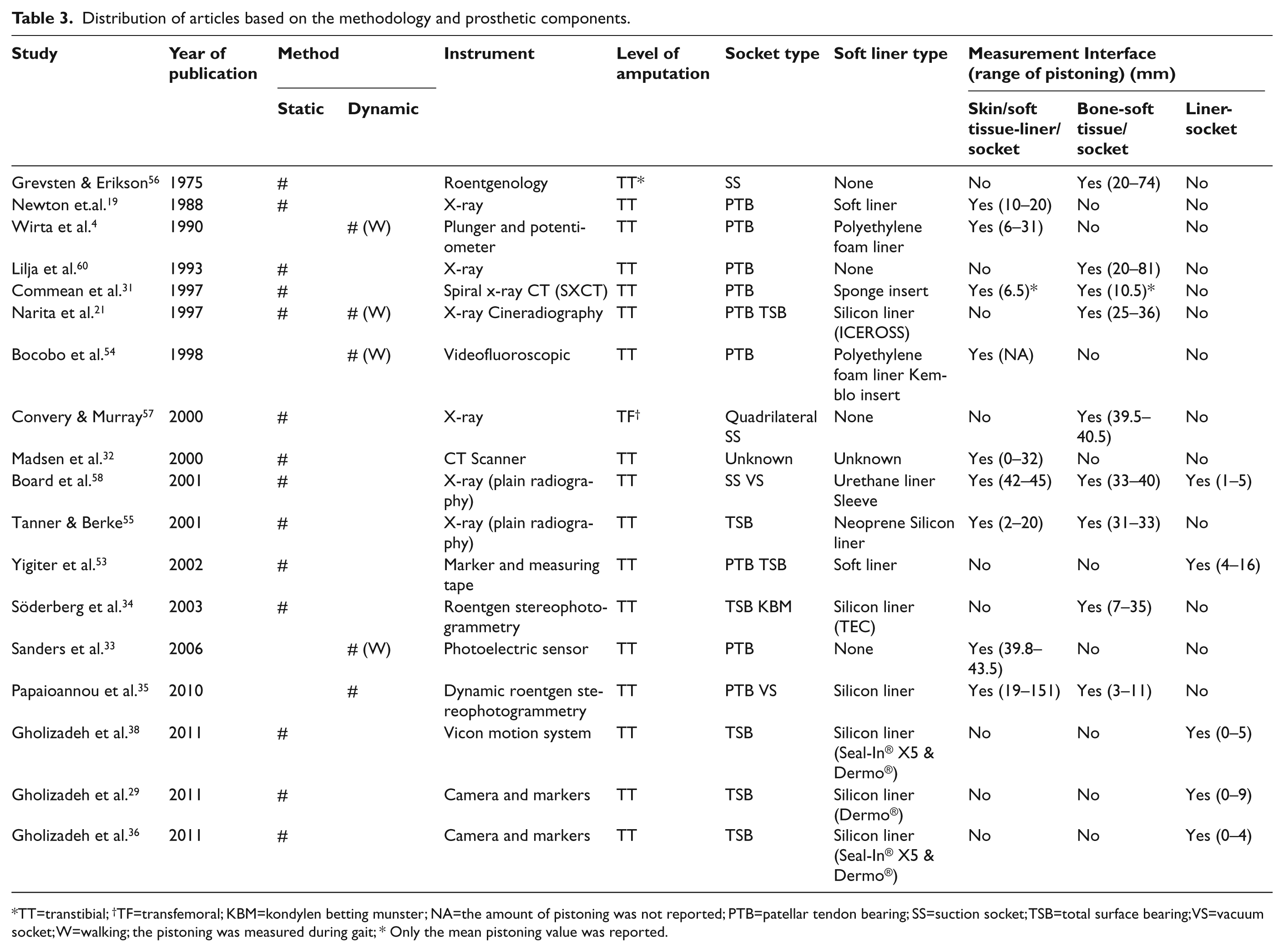
TT=transtibial; †TF=transfemoral; KBM=kondylen betting munster; NA=the amount of pistoning was not reported; PTB=patellar tendon bearing; SS=suction socket; TSB=total surface bearing; VS=vacuum socket; W=walking; the pistoning was measured during gait; * Only the mean pistoning value was reported.
The number of subjects that participated in the studies, except from those involved in case studies, ranged from five 29 to 22. 53 The age of participants varied widely from 15 53 to 81. 54 Six papers were case studies.31,33–36,55 Time since amputation was between one month 56 and 46 years 34 ; however, not all studies provided details of the time since amputation. While both unilateral and bilateral amputees were included, the subjects were mostly unilateral transtibial amputees. Only one study was conducted on a transfemoral subject. 57 The cause of amputation was mostly trauma, but also included diabetes, infection, arteriosclerosis, tumor, burn, Berger’s disease and congenital limb defects (Table 1).
Prosthesis specifications
Transtibial prostheses were mainly total surface bearing (TSB) and PTB. The only transfemoral prosthetic socket was a quadrilateral suction socket, with single axis foot and mechanical knee joint. 57
The various suspension systems that were the subject of the research in SC/SP, 4 SC, 4 cuff,4,34 waistband with cuff, 4 elastic sleeve4,34,55 and supracondylar wedge. 4 On the whole, the type of liners utilized was unclear; however, some studies did mention that they had employed Pelite,4,31,54 silicone liner21,34–38 and urethane liners 58 . Söderberg et al. 34 (2003) used four different suspension systems (cuff, SC, pin and lock, and vacuum) with the same soft liner (TEC liner) and same socket, for one 69-year-old transtibial amputee. Gholizadeh et al.36,38 fabricated TSB sockets with Talux feet and two different suspension systems (pin and lock system and suction system).
Data presentation
Except from the case studies, data for each patient were provided individually in four studies. Yigiter et al. 53 and Wirta et al. 4 presented only group data (Table 2).
Outcome parameters
The following outcome parameters were considered in the study: static pistoning, dynamic pistoning and amount of residual limb, bone or skin slippage within the socket.
Pistoning measurement methods
Various imaging methods have been successfully used to evaluate the position of bones inside the prosthetic socket. 59 Mostly radiological methods have been used.19–21,34–35,54 Spiral or helical CT also provides a high resolution, 3-D image of the stump and prosthesis. 32 Recently, a simple photographic method has been reported29,36–37 and finally, Gholizadeh et al. 38 used Vicon motion analysis system to evaluate pistoning in transtibial amputees.
The literature review revealed that the majority of researchers measured the displacement between the bone and the socket, the liner and socket or the soft tissue, by using different techniques in static position19,29,32,34–38,53,55 or during dynamic tasks33,35,54,60–61 to check pistoning inside the socket. Therefore, the methods available were classified according to whether they utilized static or dynamic pistoning. These are presented in Table 3. By static pistoning, authors mean the pistoning due to loading during standing and dynamic pistoning happened in activities such as walking or jumping.
Static pistoning
In 1975, Grevsten and Erikson, 56 and then later in 1980s, Newton et al. 19 were among the first to study PTB prosthesis by roentgenology, during which the pistoning motion was evaluated in four and two weight bearing positions, respectively.
Some researchers tried to mimic the gait by adding loads to the prosthesis when it was in a static position.21,31,38 In one study, pistoning of the tibial end was assessed in four simulated phases of the gait cycle. The researchers achieved that through the utilization of a board that was tilted 15 degrees in order to position the limb in arrangements that mimicked heel strike and toe off. When attempting to imitate the swing phase, they positioned the prosthetic limb at 45 degrees relative to the floor. 60 The same levels were used in a study by roentgen stereophotogrammetry to measure four types of suspension (supracondylar, PTB strap, distal pin suspension and vacuum suspension with expulsion valve), during which a 1-kg load was applied to the prosthetic foot as a means of replicating the centrifugal force. 34
In another study, a 5-kg load was applied to the foot of the prosthesis to simulate the swing phase, and an x-ray was taken with the prosthesis suspended at a knee flexion angle of 30°. On the radiograph, the tibial bone displacement relative to the socket bottom was measured by calculating the value difference between the weight-bearing and non-weight-bearing positions. 21
An x-ray study determined the amount of pistoning between residual femur and socket both while bearing the weight over the transfemoral prosthetic limb and during the non-weight-bearing condition. The sagittal and coronal planes of the residual femur were x-rayed. The axial distance from a reference point at the lateral distal socket wall to the distal end of the femur was measured. 34
The effect of the neoprene sleeve on the vertical tibia and stump displacement was compared with a shuttle lock suspension system in a study by Tanner et al. 55 The pistoning motion was assessed via a total of six radiographs for two suspension systems in three weight bearing positions (full, partial and none). The distance between each of the end of tibia and the distal residual limb soft tissue to proximal lock was measured on the x-ray films. One prosthesis with shuttle lock was fabricated, but in order to evaluate the neoprene sleeve, the pin was removed. 55
Yigiter et al. 53 assessed suspension systems in PTB and TSB sockets by marking the anterosuperior edge of the socket as it appeared while standing and during the swing phase. However, no data was produced that indicated exactly how the measurement was performed.
Loads of 44.5 N and 88.9 N were used to simulate the swing phase during walking and running respectively in a study of pistoning by x-ray. The x-rays were taken while the subject was lying supine and the data produced during loaded and unloaded positions was compared. 58
Some researchers attempted to measure suspension systems by applying weight to the prosthetic limb. Commean et al. 31 used a harness in order to apply the force to the prosthesis by the shoulders. In a further study, Madsen et al. 32 designed a loading device for the spiral CT method that provided a means by which large loads could be applied. The loads were determined according to the subject’s weight (full and half body mass). In both studies, the patients were evaluated in supine position.
Photographic method by the use of a camera and markers was recently introduced as a new approach for the pistoning measurement.29,36–37 Photos were taken in five loading conditions. Then the images were analyzed on the computer to measure the pistoning. The reproducibility of measurements was reported to be good.
In a recent study, 38 researchers used a Vicon motion system to evaluate the pistoning in transtibial amputees while in static positions. They attempted to simulate ambulation by adding three different loads (3, 6 and 9 kg) to the prosthetic foot. The authors claimed that the Vicon motion system was capable of quick and easy determination of the occurrence of pistoning between the liner and socket. Furthermore, they presented the motion system as a preferable alternative to exposing amputees to x-ray.
Dynamic pistoning
We found only a few studies that focused on the occurrence of pistoning during gait. Sanders et al. 33 (2006) used a non-radiological tool to measure the position of the distal end of the residual limb surface in relation to the socket when walking on an 18.5 meter walkway. Measurements were provided by means of a photoelectric sensor, which was placed in a holder and mounted on the inside distal socket wall.
In another study, the prosthetic pistoning that occurred when an amputee walked on a treadmill during one gait cycle was measured using cineradiography. The distance between the socket and the distal tibia was measured and the movement of the stump was calculated by subtracting the distance value in the weight-bearing position from the value in the suspension position. 21
Wirta et al., 4 in a study of the effect of below-knee suspension systems, placed a potentiometer as an axial movement detector at the distal end of the socket. The subjects were asked to walk a 7.5-meter distance at three different speeds: normal walking speed, fast and slow. The following seven suspension systems were compared: cuff (PTB/C), supracondylar (SC), figure-of-eight SC strap, waistband with cuff, (SC/SP, rubber sleeve and SC wedge.
In a videofluoroscopic research study, the participants were asked to walk at a comfortable speed on a treadmill. The researchers raised the treadmill so that the knee and stump were fully visible. Leaded elastic markers were attached to some of the prosthetic components both outside and inside the socket. Three exposure rates of 50, 80 and 110 KV were selected and the results were compared. Anteroposterior and mediolateral views were taken. A video camera was used to record the treadmill gait during the mean trial time of 40 s. 54 Two researchers evaluated the recorded videos and their agreement over the detection of a particular component (stump or prosthesis) was taken as the reference.
Finally, Papaioannou et al. 35 presented a new method of 3-D) socket–stump telescopic movement evaluation that was executed while the subject performed sudden fast stops and descended the stairs. They measured the piston motion between the skin and socket through the use of a roentgen stereogrammetric system that measured pistoning via tantalum pigments, which were fixed to the bone, skin and socket. Imaging could only be conducted within a confined region between the orthogonal x-ray systems. The technique did not allow evaluation during walking. The authors claimed that their method produced results of high accuracy when measuring pistoning between the stump, socket and bone. 35
Amount of pistoning
Grevesten and Erikson found an 11.3-mm bone displacement in relation to the socket when a suction-based PTB prosthesis was utilized. 56 In another study with a PTB prosthesis, the average distal tibia vertical movement during a gait cycle was 57 mm. 60
Wirta et al. 4 compared the vertical movement of conical and cylindrical residual limb shapes and reported a mean pistoning movement at the end of the residual limb of 19.1 mm. In both conical and cylindrical stumps, the rubber sleeve produced the least pistoning of the seven evaluated systems. 4
In 1997, a research study by Commean et al. 31 monitored the slippage between the skin and socket as well as tibia movement in order to evaluate the prosthetic fit in a transtibial subject. For simulating the gait, the researchers used two axial loadings of 44.5N and 178N. They identified a 10-mm tibial slippage and a movement of approximately 7 mm for the distal end of skin relative to the socket. 31 It is not clear what suspension system was used.
In an x-ray study that was completed by Narita et al., 21 the tibial displacement between the stance and swing phase was identified as 25.3 ± 9 mm for the TSB prosthesis and 36 ± 5.6 mm for the PTB prosthesis. The translation for the TSB prosthesis was significantly lower (p < 0.05) and the suspension effect of the TSB prosthesis was consequently superior to that of the PTB prosthesis. 21 Similarly, another study on the pistoning effects of PTB and TSB sockets, within which marker was placed on the sock over the stump, 53 revealed less displacement with TSB (40 mm).
Bocobo and colleagues 54 described two case reports that focused on 12 subjects. Of the amputees that were the subjects of the research, only one case was reported to have a PTB socket. It was stated that significant piston action was observed in one subject, possibly by comparison between two phases of gait; however, they did not mention in which phase the pistoning was the most severe. They also did not provide the value of the pistoning. The pistoning movement was measured by subtracting the position of patellar tendon bar marker from the knee joint during two gait phases. 54
A spiral CT study completed by Madsen et al. 32 did not represent any specific value for the pistoning that was observed, and was limited to the provision of a figure legend that provided details of differences in displacement between full body weight and non-loading conditions. The displacements ranged from 0 to 32 mm.
In a study by Board et al., 58 the observed amounts of liner and tibia bone displacement relative to the end of socket marker were 40 mm and 70 mm for the socket with electric vacuum pump (Harmony® system) and the normal valve transtibial socket, respectively. The amount of pistoning with normal suction was reported to be 50 mm. Although the pistoning was measured statically under loads, the majority of subjects stated that they felt less pistoning with the vacuum socket than they did with the normal suction during walking activities. 58
When the shuttle lock system was evaluated versus the no lock condition, the value of tibial end displacement from the proximal edge of the lock was almost equal in both suspension conditions across three different loading positions. However, there was less soft tissue displacement noted with the shuttle lock system. The patient also preferred the shuttle lock as a result of lower pistoning. The researchers concluded that the amputee’s opinion about the pistoning was more related to the soft tissue movement than the tibia. 55
In Söderberg’s et al. 34 study, the pistoning of the tibia within the Kondylen Betting Munster (KBM) socket with SC strap was revealed to be about 35 mm, while the pin and sleeve resulted in approximately 17 mm of displacement.
Sanders et al. 33 studied distal residual-limb position during gait. In their findings they mentioned that after toe off, the residual limb came 30 mm out of the socket. They also identified an overall 40-mm stump displacement in proximal direction at the end of the swing phase. Additionally, they stated that pistoning in the PTB without strap was 0.8 mm larger than it was when the strap was used. Furthermore, after a five minute rest, 3.7 mm more pistoning was found (before rest: 39.8 mm, after rest 43.5 mm for PTB with SC strap).
A roentgen stereogrammetric study on transtibial amputees that was completed by Papaioannou et al., surprisingly revealed 151 mm pistoning movement in the fast stop task and 19 mm pistoning movement for the step down between the markers on the skin and socket.35,62 However, they could not measure the pistoning during walking. Except from one case that used a customized vacuum socket with silicone liner, the type of suspension systems was not specifically indicated. 35
In the only study on transfemoral prosthesis, Convery and Murray 34 measured the vertical movement of the femur. After the subject changed his position from full weight to non-weight-bearing, the femur displacement was measured at 1 mm.
Photographic method showed about 9 mm of pistoning between the Dermo® liner and socket in non-weight bearing compared with full weight bearing position. 36 Another study using same photographic methodology revealed that adding loads to the prosthesis caused less pistoning between Seal-In® X5 liner and the socket (2 mm) compared with Dermo® liner (4 mm). 29
Gholizadeh et al. 38 compared the pistoning between two different transtibial liners (Seal-In® X5 and Dermo® liner) and the socket through the use of a motion analysis system. The analysis of the data showed the maximum amount of pistoning within the socket occurred after 90 N was added to the prosthetic limb. On average, 2 mm (SD 1) pistoning occurred with the Seal-In®X5 (60% less than Dermo® Liner) and 5 mm (SD 1.5) with the Dermo® Liner (p < 0.02), after the 90 N load was added. 38
Discussion
Suspension systems should help to establish a firm prosthetic attachment to the limb. It is claimed that suspension systems that are based on the suction concept reduce the displacement of the skeletal anatomy by 50%, which will in turn result in increased stability between the stump and socket and a reduction in skin sores. 56 Above all, less pistoning may indicate a more natural gait and the amputee is more likely to feel like the prosthesis is a part of their body.19,63,38 Different methods have been used to evaluate pistoning in lower limb prosthesis, both in static and dynamic positions (Table 3). To date, radiological methods have constituted the more popular methods of measuring the pistoning. However, such methods are rarely available to prosthetists due to the cost of the equipment involved and the complex, time consuming data collection required. In addition to that, such methods involve exposing the patient to radiation via the x-ray process which is not desirable. 64 Although some of these studies tried to produce precise x-ray examinations, measurement inaccuracy still exits. 56 The measurements may vary a little owing to distortion following the minor changes in distances between the extremity and the film. In order to get higher resolution images some studies tried different exposures rates.
Using CT scanners as a means of measuring pistoning does have some advantages. These include the ability to produce high spatial resolution that provides 3-D visualization of the prosthesis and the internal tissues of the stump. However, such measurement methods require the subjects to be positioned supine. Madsen et al. 32 stated that evolution in CT imaging systems may entail that these devices could easily be adapted to perform more sophisticated loading protocols. The harness that Commean et al. 31 used to apply load to subjects had several limitations because it took a long time to set up and the subject needed to be fully cooperative.
The evaluation of pistoning by photoelectric sensor was also reported to have some drawbacks because it was not wireless and a cable was required to connect the sensor to the data acquisition system. This problem could be overcome with radio-frequency telemetry systems. A further problem with this measurement method was that it did not allow the use of a liner with shuttle lock and pin as it was impossible to make a hole at the end of the liner. 33
The researchers were able to measure piston motion between the socket and liner by a photographic method.29,36,37 They claimed easy and fast determination of pistoning; however, the reliability and repeatability of the method needs to be further investigated.
The use of a Vicon motion system 38 has been recently reported for the purposes of static pistoning measurement. The technique was said to be accurate. However, one of the main problems with this measurement system is the fact that it requires a motion laboratory that may not be accessible to every rehabilitation or prosthetic center. Additionally, it cannot be employed to monitor the tibial movement within the soft tissue.
Only five studies indicated that the trials were repeated three to five times21,29,33,36,38; therefore the reliability of the data in most of the reviewed papers is questionable. However, it can be justified to some extent by ethics related to the x-ray exposure. Finally, as far as the current research established, no one has set a limit for the acceptable amount of pistoning. Only Newton et al. 19 stated that vertical displacement of 10 mm or less is considered ideal and comfortable. Nevertheless, they did not provide any evidence to support their statement.
Conclusions
The focus of this paper was on the available methods for measuring pistoning in lower limb amputees. Some 70% of the available studies measured pistoning by simulating the gait through applying static loads. The loads were meant to mimic the centrifugal or inertial forces that acted on the limb during walking (mostly swing). Some say that the pendulum dynamic applies to the swinging lower limb 65 and, as such, this inertial force is influenced by the segment weight (here the prosthesis mass). Nevertheless, similar loads were used for different subjects which is somewhat controversial.
Overall, some important points can be inferred from the evaluation of the available literature. With regard to the complicated equipment and techniques that are available for the purpose of measuring pistoning, existing methods seem to be far from practical in a clinical setting and, as such, many of them are only suitable for manufacturers who wish to evaluate their suspension system products, including the liners. Since a reduction in pistoning significantly contributes to optimal prosthetic fit, further research with larger sample sizes seems necessary in order to invent and evaluate accurate, safe and simple methods of pistoning measurement that can be made more widely available to every prosthetist.
Displacement of the residual limb relative to the socket or ‘pistoning’ causes frictional loads. 66 The present study revealed that the majority of the studies focused on slippage or vertical movement of the residual limb inside the socket. However, as friction has two components of slippage and shear force, both should be taken into account. 66 While low pistoning might be an indicator of proper coupling between the skeleton and prosthesis, it might, in turn, result in skin breakdown. 52
Pistoning is mainly a phenomenon that occurs during the gait and functional activities. Today, with technological advances that have resulted in more choices of kinematic gait analysis, static techniques seem to be of no use and research studies should employ methods of dynamic evaluation. Moreover, there are many different liners available and there is a distinct lack of published research that addresses how these liners influence pistoning.
It is also worth noting that, consistent assessment is of importance. Fabrication and fitting by one single prosthetist would be one possible solution. Future research should also examine the occurrence of pistoning during activities of daily living. The effect of body mass index (BMI) is another area that has not been fully addressed within the existing literature. Walking causes sweating which, in turn, changes the biomechanics of the liner-skin interface and might influence the prosthetic attachment to the stump. Therefore, research studies should be conducted to determine the effect of walking time and distance. Little is known about the bone-stump-socket interface kinematics in transfemoral prostheses. Hence, investigation of socket suspension in transfemoral prostheses is also recommended.
Footnotes
Acknowledgements
We appreciate the help and support of Össur (Reykjavik, Iceland), especially Ms Ása Lúðvíksdóttir and Mr Scott Elliott. The authors would also like to thank Dr Steven A Gard at Northwestern University Prosthetics-Orthotics Center, and Dr Anthony McGarry at the National Centre for Prosthetics and Orthotics, University of Strathclyde for their invaluable advices.
Conflict of interest
The authors report no conflict of interest.
Funding
This work was supported by the Malaysia UM/MOHE/HIR grant (Project Number: D000014-16001).