
Abstract
Background:
Despite the evidence for improved safety and function of microprocessor stance and swing-controlled prosthetic knees, non-microprocessor-controlled prosthetic knees are still standard of care for persons with transfemoral amputations in most countries. Limited feature microprocessor-control enhancement of such knees could stand to significantly improve patient outcomes.
Objectives:
To evaluate gait speed, balance, and fall reduction benefits of the new 3E80 default stance hydraulic knee compared to standard non-microprocessor-controlled prosthetic knees.
Study design:
Comparative within-subject clinical study.
Methods:
A total of 13 young, high-functioning community ambulators with a transfemoral amputation underwent assessment of performance-based (e.g. 2-min walk test, timed ramp/stair tests) and self-reported (e.g. falls, Activities-Specific Balance Confidence scale, Prosthesis Evaluation Questionnaire question #1, Satisfaction with the Prosthesis) outcome measures for their non-microprocessor-controlled prosthetic knees and again after 8 weeks of accommodation to the 3E80 microprocessor–enhanced knee.
Results:
Self-reported falls significantly declined 77% (p = .04), Activities-Specific Balance Confidence scores improved 12 points (p = .005), 2-min walk test walking distance increased 20 m on level (p = .01) and uneven (p = .045) terrain, and patient satisfaction significantly improved (p < .01) when using the 3E80 knee. Slope and stair ambulation performance did not differ between knee conditions.
Conclusion:
The 3E80 knee reduced self-reported fall incidents and improved balance confidence. Walking performance on both level and uneven terrains also improved compared to non-microprocessor-controlled prosthetic knees. Subjects’ satisfaction was significantly higher than with their previous non-microprocessor-controlled prosthetic knees. The 3E80 may be considered a prosthetic option for improving gait performance, balance confidence, and safety in highly active amputees.
Clinical relevance
This study compared performance-based and self-reported outcome measures when using non-microprocessor and a new microprocessor-enhanced, default stance rotary hydraulic knee. The results inform rehabilitation professionals about the functional benefits of a limited-feature, microprocessor-enhanced hydraulic prosthetic knee over standard non-microprocessor-controlled prosthetic knees.
Keywords
Background
Proximal levels of limb amputations usually result in greater functional impairments than more distal levels. Following transfemoral amputation, patients are less likely to be fitted a prosthesis 1 and regain full community mobility than those with limb loss at the, for example, transtibial level. 2 Their physical capabilities are often compromised by impaired balance 3 with frequent stumbles and falls4,5 and increased risk of injuries. In addition, they usually experience slower customary walking speeds within a limited range 6 and increased metabolic 7 and mental energy expenditure. 8 They also suffer impaired mobility on uneven terrain, 9 slopes and hills, 3 and stairs. 10
The selection of a prosthetic knee joint requires comprehensive consideration, to provide safety and function. 11 Typical reciprocal gait on non-level surfaces such as uneven terrain, slopes, and stairs requires controlled knee flexion during prosthetic single limb stance. Friction brake and four-bar knee mechanisms do not provide this function, often times eliciting adaptations such as non-physiologic step-to patterns over these terrains. Polycentric mechanisms may enable limited knee flexion during prosthetic limb loading. Hydraulic stance control mechanisms may allow for unlimited knee flexion during prosthetic limb loading supporting reciprocal step-through gait patterns over non-level terrains. The more stance control a non-microprocessor-controlled prosthetic knees (NMPK) provides, the more difficult it can be for the user to reliably effect and control the switch between stance to swing. Among available NMPK mechanisms, this creates an inverse relationship between inherent stability and functionality: the more stable the prosthetic knee in weighted stance, the less enabling it can be for reciprocal gait on uneven terrain, slopes, and stairs. 12
Microprocessor (MP) control has overcome this design limitation, offering superior safety and function at the same time.13–15 However, prosthetic knees with full MP stance and/or swing control have not even been adopted as standard of prosthetic care in all developed countries to date. The new 3E80 (Otto Bock HealthCare GmbH, Duderstadt, Germany) is a default stance hydraulic knee enhanced by an MP that controls the transition between stance and swing phases and provides a stumble recovery function. The primary objective of this study was to investigate whether or not the MP-enhancement results in reduced fall incident rates and risk of falling. In addition, functional performance on different terrains and satisfaction with the prosthesis were assessed. The MP-enhanced knee was compared to NMPKs usually prescribed and fitted to subjects with a transfemoral amputation who present the ability for unlimited community ambulation in Latin America.
Methods
Study participants
Participants were enrolled when they had met the following inclusion criteria: age ⩾ 18 years, unilateral transfemoral amputation or knee disarticulation, Medicare Functional Classification Level (MFCL) 3 or 4, use of the current prosthesis for at least 6 months, and written informed consent. Exclusion criteria were defined as additional major limb amputations, use of walking aids, poor socket fit, recurring residual limb skin breakdown, and any medical condition that may have resulted in a limitation or fluctuation of the physical capacity during the study. Since the study center does not provide prosthetic patient care, it had to depend on referrals of potential study participants. Subjects were screened for inclusion and exclusion criteria by certified prosthetists in six local prosthetic clinics who were not otherwise involved in the study process. Referred subjects were evaluated in the study center and enrolled if they had agreed to participate and signed a written informed consent. In total, 15 individuals were referred by the prosthetic clinics. All of them met the inclusion criteria and did not meet any exclusion criteria, so they were enrolled as consecutive patients.
Study design
This study was approved by the Committees on Ethics in Research of the Federal Department of Health of Brazil and of the Municipal Hospital Dr Mário Gatti in Campinas, Brazil.
After baseline assessment with the existing prosthetic knee (NMPK), subjects were fitted the 3E80 intervention knee and allowed for an accommodation period of 8 weeks, after which the study was concluded with a follow-up assessment. Details on the test prostheses are provided in section “Knee conditions.” As subjects had used their current prosthesis for a minimum of 6 months, full accommodation to the NMPK condition was assumed. No additional training or physical therapy other than a basic instruction and 2-hour ambulation training with the intervention knee was provided.
Knee conditions
Most of the NMPKs (86%) were 3R80 default swing knee joints with a monocentric rotary hydraulic with manually adjustable resistances for stance flexion, swing flexion, and swing extension. Stance phase dampening is activated by loading the knee above a manually adjustable threshold. This allows for knee flexion during weight bearing, which is required for reciprocal slope and stair descent. Swing control is activated by unloading the knee or producing a forefoot load with the knee fully extended. One patient used a 3R21 four-bar knee with friction swing control, and one patient used a 3R92 friction brake knee with pneumatic swing control. The intervention knee 3E80 is very similar to the 3R80 rotary hydraulic with the same manual adjustment options. Compared to MPKs that continuously adjust stance and swing resistances for every step, the basic resistance settings for the 3E80 are manually adjusted and do not change between steps. In addition, the 3E80 is enhanced with an MP that controls switching between stance and swing and designed as a default stance knee. The MP utilizes input from a patented sensor that permits the calculation of torques at various points of the prosthesis below the knee. Thus, the MP can distinguish between heel and forefoot loads acting through the prosthetic foot. The 3E80 switches into swing control when (1) the knee is fully extended and (2) a forefoot load is determined to exceed a dynamically calibrated threshold. In early swing, the MP keeps knee flexion resistance low as long as the knee is flexing to allow for sufficient heel rise and thus toe clearance during mid-swing. As soon as the knee and shank start the extension movement after heel rise, the MP re-activates the high knee flexion resistance set for stance to ensure knee stability for stumble recovery in case of any perturbation. Should the forefoot moment decrease at terminal stance without initiation of swing, such as in the case of walking backwards, the MP re-activates the high stance phase resistance setting to ensure knee stability during potential events of stumble.
Subjects’ existing sockets, prosthetic feet, and structural components were used throughout the study. The intervention knee was fitted in all patients by the same certified study prosthetist. Changes to the alignment of the prosthesis and adjustments to the prosthetic knee were made in accordance with the recommendations of the manufacturer.
Participants were allowed to keep the intervention knee if they had demonstrated substantial improvements in at least one safety and one functional outcome. To limit the potential bias of the study results, subjects were only made aware of that opportunity after they had completed the protocol.
Outcome measures
A set of performance-based and self-reported outcome measures was used to assess fall incidence rates and risk of falling, functional walking performance on different terrains, and satisfaction with prosthesis use in both knee conditions. Subjects started with a self-report instrument and were then administered a performance-based test and so forth in alternating order.
Outcome measures for fall rates and risk of falling
Falls
Patients were asked how often they had fallen in the past 4 weeks prior to the visit on their current or intervention prosthetic knees, respectively.
Timed Up and Go test
The Timed Up and Go (TUG) test is a validated test to assess the risk of falling and overall physical function in the elderly 16 and individuals with amputations.17,18 The minimal detectable change (MDC90) in amputees has been reported to be 3.6 s, 19 and completion times ⩾19 s indicate an increased risk of falling. 18
Four Square Step Test
The Four Square Step Test (FSST) is a validated test for the risk of falling in older adults 20 and subjects with amputations. 18 Completion times ⩾24 s indicate an increased risk of multiple falls. 18
Activity-Specific Balance Confidence scale
The Activity-Specific Balance Confidence (ABC) scale is a self-report instrument that assesses perceived balance confidence in 16 activities of daily living (ADL). It has been validated for use in the elderly 21 and persons with amputations. 22 Scores ⩽67 are considered to indicate an increased risk of falling. 22
Falls Efficacy Scale–International
The Falls Efficacy Scale–International (FES-I) is a validated self-report instrument to assess the fear of falling in 10 ADLs. It has been validated for use in the elderly 23 and persons with amputations. 5
Functional walking performance tests
The 2-Min Walk Test on level and uneven ground
Timed walk tests are validated measures of physical performance and overall mobility in the elderly and patients with various medical conditions 24 including lower limb amputations.25,26 The MDC has been reported to be between 17 27 and 34.5 m. 19 However, the latter value was determined in a mixed sample of subjects with transtibial and transfemoral amputations with no specification of their functional levels. Generally, in rehabilitation, increases in walking speed of 0.1 m/s or more, which would equal an increase in walking distance of 12 m or more in the 2-min walk test (2MWT), are considered clinically meaningful.28–30
Rating of Perceived Exertion (Borg scale)
The Borg Rating of Perceived Exertion (RPE) measures the perceived intensity of physical activities on a visual analogue scale. It provides a good estimate of the actual heart rate during physical activity and is correlated with lactate levels, %VO2max, and breathing rates in athletes. 31 It was assessed immediately after the subjects had finished the 2MWT.
Timed Ramp Test
The Timed Ramp Test (TRT) was developed to assess participants’ ability to ascend and descend a 359-cm-long and 60-cm-wide ramp with 19% grade (10° incline) and handrails on both sides. Times were recorded for how long it took each subject to walk as fast as possible from the bottom to the top of the ramp (ascent) and from the top to the bottom (descent).
Timed Stair Test
The Timed Stair Test (TST) was developed to assess participants’ ability to ascend and descend a 122-cm-tall and 76-cm-wide staircase with five steps and handrails on both sides. Times were recorded for how long it took each subject to walk as fast as possible from the bottom to the top of the stair (ascent) and from the top to the bottom (descent).
Orthotic and Prosthetic Users’ Survey
The Orthotic and Prosthetic Users’ Survey (OPUS) is a validated self-report outcome measure to assess perceived difficulty of 20 ADLs. 32
Patient satisfaction
Question #1 of the Prosthesis Evaluation Questionnaire
The Prosthesis Evaluation Questionnaire (PEQ) is a validated self-report instrument to assess quality of life and perceived prosthetic function. 33 In this study, only question #1 “Over the past 4 weeks, how happy have you been with your prosthesis?” was rated on a 100-mm visual analogue scale. Question #1 of the PEQ has been used independently in several prosthetic studies. 34
Satisfaction with the Prothesis questionnaire
Patient satisfaction with the entire fitting process was evaluated using the validated Satisfaction with the Prothesis (SAT-PRO) questionnaire that has also been used in several prosthetic studies.35,36
Knee preference
After completing the research protocol, patients were asked which prosthetic knee joint they would prefer to keep. At the time of the interview, they did not yet know that they would be allowed to keep the intervention knee if they had demonstrated favorable objective outcomes with it.
Statistical analysis
The sample size calculation was based on the published means and variabilities for the reduction in falls demonstrated using MP-controlled knees (MPK).13–15,34,37 Assuming a mean reduction in falls by 60% using the 3E80, the minimum sample size to demonstrate statistical significance was calculated at 15 participants.
All data were tested for normal distribution to determine the appropriate statistical test for each outcome measure. Normally distributed data were analyzed using the t-test for paired samples, non-normally distributed data were analyzed with the Wilcoxon test. All statistical analyses were conducted using MATLAB (The MathWorks, Inc., Natick, MA, USA) with thresholds for statistical significance set a priori to 0.05. For the interpretation of statistically significant results, MDC and minimally clinically important differences (MCID) of the respective measures, if published, were used as references.
Results
Subject demographics
A total of 15 subjects gave informed consent to participate in the study. One subject withdrew prior to the baseline assessment due to time constraints, and another subject dropped out during the study due to a medical condition unrelated to the intervention. Thus, 13 participants (11 males, 2 females) with a mean age of 33.1 ± 8.8 years, who had used their existing prostheses for 5.8 ± 2.6 years, completed the study protocol. Detailed demographic information on all participants is presented in Table 1.
Demographic information on the participants.
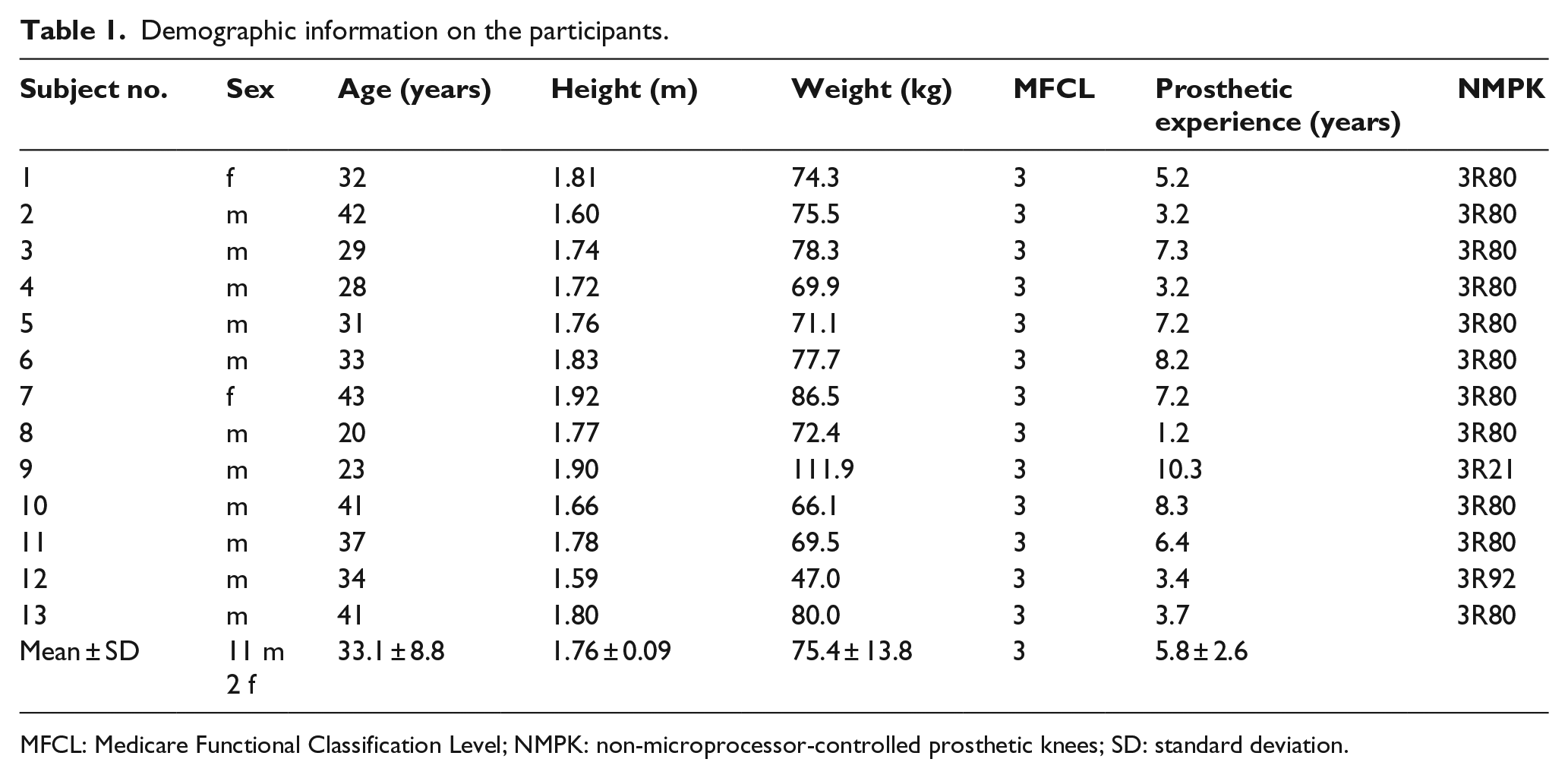
MFCL: Medicare Functional Classification Level; NMPK: non-microprocessor-controlled prosthetic knees; SD: standard deviation.
Fall rates and risk of falling
In the 4 weeks prior to the assessment sessions, participants reported significantly fewer falls with the 3E80 knee than with their previous NMPKs. An extreme outlier with 10 falls per day (280 falls in the past 4 weeks) on his NMPK, but no falls on the 3E80, was excluded from the analysis to prevent this dataset from distorting the average number of falls with an NMPK in the rest of the study sample. Thus, the number of reported falls in the remaining 12 subjects decreased significantly by 77% (p = .04). Similarly, the rating of perceived balance confidence on the ABC scale improved significantly by 12 points (p = .005). The individual results for the falls and ABC scores are presented in Table 3. Eight subjects each (62%) were able to reduce falls or improve their ABC score by 10 or more points. The FSST, TUG, and FES-I did not reveal any significant differences between the knee conditions (Table 2).
Safety, functional, and mobility outcomes.
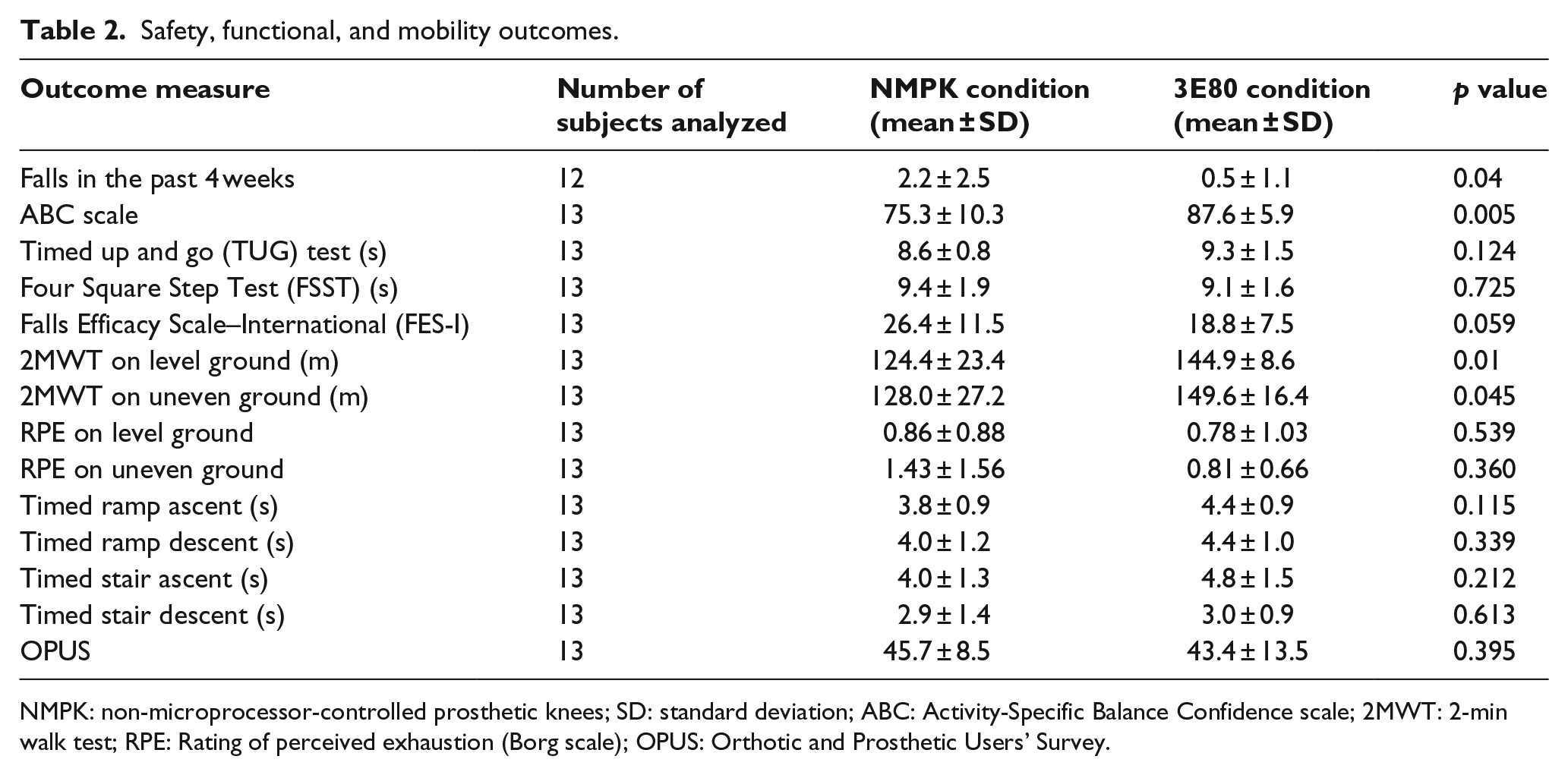
NMPK: non-microprocessor-controlled prosthetic knees; SD: standard deviation; ABC: Activity-Specific Balance Confidence scale; 2MWT: 2-min walk test; RPE: Rating of perceived exhaustion (Borg scale); OPUS: Orthotic and Prosthetic Users’ Survey.
Functional walking performance tests
The 2MWTs on level and uneven terrains demonstrated significant improvements in the distance walked with the 3E80 as compared to the NMPK that exceeded one of the MDCs reported in the literature. 27 The corresponding increase in walking speed of 0.18 m/s was well above the widely accepted MCID of 0.1 m/s.28–30 The individual results for the distance walked in the 2MWT on both terrains are presented in Table 3. On either terrain, eight subjects (62%) improved their average walking speed by more than 0.1 m/s. The Borg RPE for the 2MWTs did not show a difference between the knee conditions and neither did the completion times in the timed ramp and stair tests or the rating of perceived difficulty of ADLs in the OPUS questionnaire (Table 3).
Individual subject results for those outcome measures that demonstrated significant differences for the entire study sample.
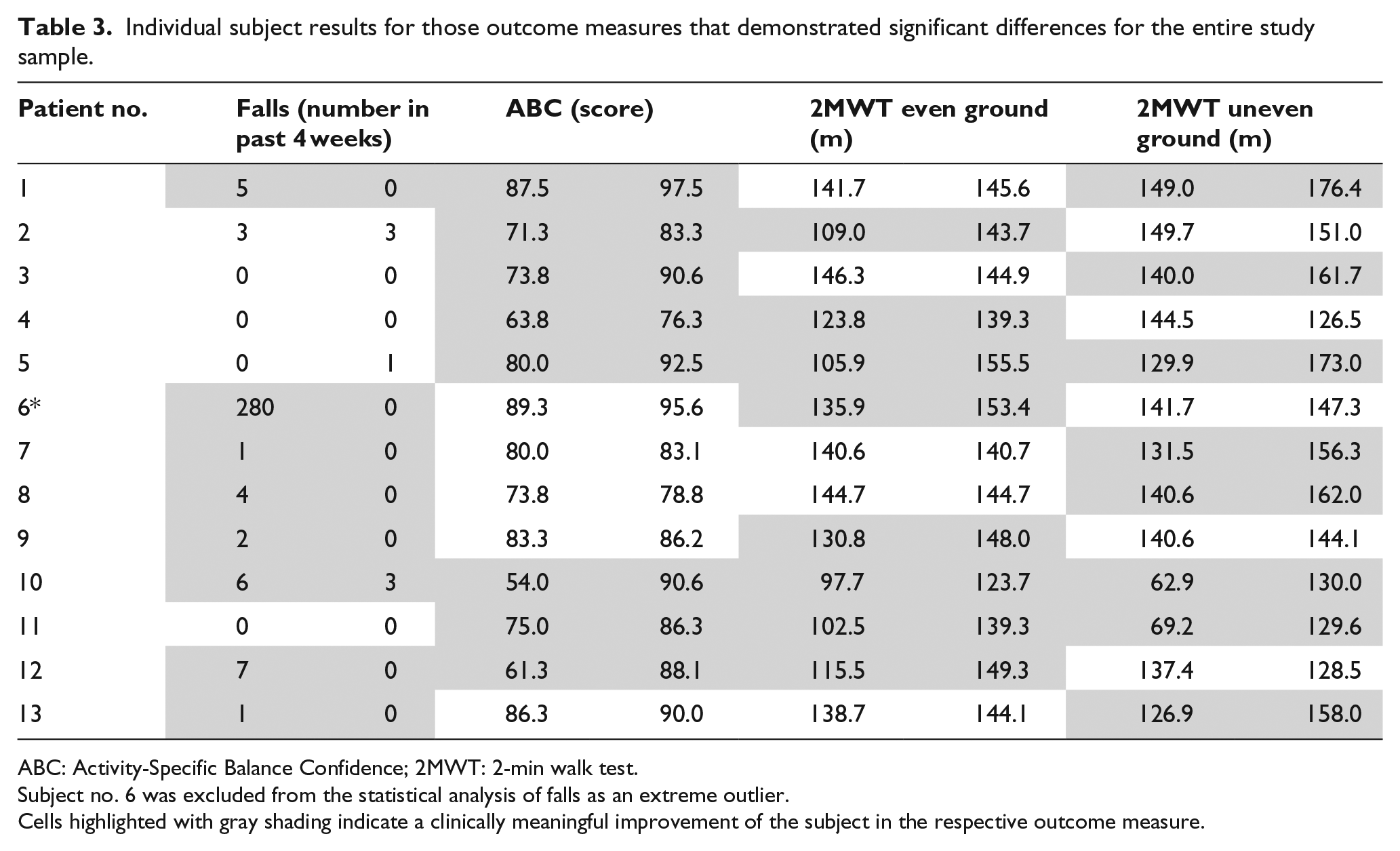
ABC: Activity-Specific Balance Confidence; 2MWT: 2-min walk test.
Subject no. 6 was excluded from the statistical analysis of falls as an extreme outlier.
Cells highlighted with gray shading indicate a clinically meaningful improvement of the subject in the respective outcome measure.
Satisfaction with the prosthesis
Subjects’ satisfaction with the prosthesis as measured with question #1 of the PEQ demonstrated a significant 41% increase from 63.8 ± 22.3 to 89.9 ± 8.9 (p = .0006) when using the intervention knee. The satisfaction with the entire fitting process as assessed with the SAT-PRO questionnaire demonstrated a significant 20% improvement from 30.5 ± 6.7 to 24.6 ± 5.5 with the 3E80 (p = .01). At the end of the study, all 13 patients preferred the MP-enhanced, default stance knee. All of them were allowed to keep it as they all had demonstrated substantial individual improvements in at least one safety outcome and one functional performance test (Table 3).
Discussion
In this first clinical study, with an MP-enhanced, default stance hydraulic knee, subjects experienced a significant 77% reduction in falls as well as a significant 12-point improvement in balance confidence during ADLs as compared to using their previous NMPKs. These improvements have the same magnitude as those reported for the C-Leg and C-Leg Compact compared to NMPKs.13,14,34,37,38 However, some other MPKs have not been able to demonstrate reduction in falls and risk of falling.39,40 In addition, our participants were able to increase their walking speeds in the 2MWT from 1.03 to 1.21 m/s on level terrain and from 1.07 to 1.25 m/s on uneven terrain with the 3E80 knee. Together with the significantly improved ABC score, this clinically meaningful improvement may reflect increased confidence in the prosthesis. That is likely the result of the safer MP-controlled gait phase switch mechanism and stumble recovery function. It has been reported that an average walking speed of 1.08–1.25 m/s or a distance of 130–150 m covered in the 2MWT, respectively, indicate good overall walking capabilities and no longer represent a substantial impairment of ambulation and daily activity.41,42 With the NMPK, our study sample was slightly below this important threshold but was able to reach it when using the 3E80. There are distinct technical differences between the MPKs available.43,44 C-Leg (MP stance and swing control) and C-Leg Compact (MP stance control) have demonstrated not only improvements in walking speed and/or quality of gait on even37,38,45 and uneven terrains 37 but also on obstacle courses, slopes, and stairs.13,14,26,34,38,46 Other MPKs have failed to demonstrate benefits in some of these measures39,40 or have not even been subjected to clinical studies yet. In this study, the 3E80 knee did not improve slope and stair mobility nor perceived difficulties of performing ADLs. This is not surprising as negotiating slopes and stairs and performing many ADLs depend on the control of stance phase resistances and behavior of the knee rather than on the gait phase switching mechanism. Stance control and behavior do not differ between 3E80 and 3R80 that was used as control by 86% of subjects. Both knees use the same hydraulic unit and resistance adjustment options. Improvement in participant satisfaction with the intervention knee was significant and similar in magnitude to that reported for other MPKs.13,14,34,37,38 We assume that, based on our findings and subjects’ comments, this increase in satisfaction is mainly due to improved safety and balance confidence. The 3E80 MP-enhanced, default stance hydraulic knee may therefore be an alternative for active individuals with MFCL-3 mobility who desire or need more safety but are satisfied with the functional support of a regular hydraulic knee.
Limitations
This study has several limitations. The average age of subjects was much younger than in most prosthetic studies in Europe or North America. Reasons are somewhat different amputation etiology and incidence patterns and a higher likelihood of older amputees in Latin America not fitting the ambitious inclusion and exclusion criteria. In addition, older individuals in Latin America are not used to the concept of clinical research. This results in a low willingness to participate in such projects. Although a selection bias executed by the prosthetic referral clinics cannot fully be excluded, they were not involved in the study process beyond patient screening. Due to the limited number of subjects referred, the study center did not have the chance to individually select or turn away eligible individuals willing to participate. However, it is much more challenging to study clinical differences between prosthetic interventions in such a young and high-functioning sample, since the high physical capabilities of the subjects are more likely to outweigh technical and functional differences between prosthetic components. Due to attrition, we were not able to finish the study with the minimum sample size calculated. That might raise a concern that the study was underpowered to find differences between the interventions. As the p values of the statistical tests for all outcome measures illustrated in Table 2, only the FES-I score might have reached statistical significance with the full sample of 15 subjects. However, as the FES-I scores for both knee conditions were way below the established threshold of ⩾70 indicating increased fear of falling, a would-be statistical difference might not be interpreted as clinically meaningful. Although 11 of the 13 participants used a non-MP hydraulic stance and swing control knee, the NMPK condition was not fully standardized. In addition, the prosthetic foot condition was not standardized, since subjects kept their existing feet. There is no consensus on the optimal accommodation time to prosthetic interventions. The acclimation period used in our study was consistent with the 2–3 months commonly allowed for in most prosthetic studies. 47 In addition, as the only difference between the 3R80 used by 86% of subjects prior to enrollment and the 3E80 intervention was the gait phase switch mechanism, 8 weeks were deemed sufficient. For the same reason, only a basic 2-hour training session with the intervention knee was provided, which largely eliminated training as a confounding factor of effects. The order of knee conditions was not randomized, and neither participants nor assessors were blinded. Some of the outcome measures were developed for this study and have not yet been validated. These factors may impose a bias in the results.
Conclusion
In this study, use of the 3E80 MP-enhanced, default stance hydraulic knee resulted in significantly fewer self-reported falls, improved balance confidence, faster walking speed on level and uneven terrain, and increased satisfaction with the prosthesis compared to the use of traditional NMPK commonly available.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Committees on Ethics in Research (CEP) of the Federal Department of Health of Brazil and of the Municipal Hospital Dr Mário Gatti in Campinas, Brazil, with CAAE number 32859214.2.0000.5453 and review number 977,585 on 12 February 2015.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Fundação de Apoio à Capacitação em Tecnologia da Informação (FACTI), the employer of Sara Agueda Fuenzalida Squella and Ângelo Brandão Benetti, received a research grant from Ottobock to conduct this study. Andreas Kannenberg is a full-time employee of Ottobock, the manufacturer of the studied 3E80 MPK. The intervention knees were made available by Ottobock, and subjects were fitted with the intervention prosthesis by a certified prosthetist employed by Ottobock do Brasil.