
Abstract
Background:
The International Classification of functioning, disability and health refers capacity to what an individual can do in a standardised environment and describes performance as what an individual really does and whether the individual encounters any difficulty in the real-life environment. Measures of capacity and performance can help to determine if there is any gap between them that may restrict participation. The aim of this study was to explore the relationship between capacity scores obtained in a standardised clinical setting and proportional ease of performance obtained from a real-life environment.
Methods:
The Assessment of Capacity for Myoelectric Control and the Prosthetic Upper Extremity Functional Index were used to assess capacity and performance in 62 prosthetic users (age 3–17). Spearman coefficient and generalised linear model were used to examine the association between these measures.
Results:
A strong correlation (Spearman = 0.75) was found between the capacity scores and the ease of performance. In both unadjusted and adjusted models, capacity was significantly associated with proportional ease of performance. The adjusted model showed that, by 1 unit increase in the Assessment of Capacity for Myoelectric Control score, the ratio of proportional ease of performance increases by 45%.
Conclusion:
This implies that Assessment of Capacity for Myoelectric Control can be a predictor for ease of performance in real-life environment.
Clinical relevance
The ACMC scores may serve as an indicator to predict the difficulties that the children may encounter in their home environment. This prediction can help the clinician to make decisions, such that if the child requires more control training or is ready to move on to learn more complex tasks.
Background
Children with upper limb reduction deficiency are often fitted with prostheses to compensate for limb absence. The goal of prosthetic fitting is to provide the children with the means to perform daily activities and become more independent. 1 To do so, the children need to achieve an adequate capacity for control and learn to perform activities using the prosthesis. The training is usually provided by the occupational therapist at the prosthetic clinic. The International Classification of functioning, disability and health (ICF) refers capacity to what an individual can do in a standardised environment and describes performance as what an individual really does and whether he or she encounters any difficulty in the home environment. 2 Standardised capacity measures that evaluate the ability in operating the prosthesis are important tools for clinicians.3–5 The assessment results show whether the users are able to control the prosthetic grip skilfully and effectively. Hence, clinicians evaluate the children’s abilities in operating their prostheses (capacity) in a standardised clinical environment using standardised capacity measures. This gives information about the capacity for control but no information about the ability to perform daily activities, the ultimate goal for the prosthetic fitting.
When the children have gone back to their home environment, little is known whether they use their prostheses in any activity and if they encounter any difficulty in using prosthesis in daily activities in their home environment. As most prosthesis users do not live near the prosthetic clinics and assessments in home environment are not always feasible, self-report questionnaires are commonly used to examine performance in their home environment.6,7 The scores provide information whether the prosthesis is being used in any activity and if the child encounters any difficulty in using the prosthesis in the activities.
Measures of capacity and performance provide important information for both prosthesis users and prosthetic providers. 8 What a child can do is not only influenced by what the child can do but also by the child’s physical and social environment. 9 Having access to both capacity and performance scores enable us to determine if there is any gap between capacity in a standardised environment and performance in real-life environment. If ease of performance scores are low this may indicate either that the capacity is low or that the child needs further training in using the prosthesis to perform the tasks. If capacity scores are higher than performance scores, then some aspects of the real-life environment is a barrier to performance. 2 Typically, clinicians expect a high capacity to be related to a high ease of activity performance. However, the relationship between capacity and performance has not been systematically explored in paediatric prosthesis users. The aim of this study was therefore to explore the relationship between capacity scores obtained in a standardised clinical setting and ease of performance scores obtained from a real-life environment. Our hypothesis is that the higher the score in the ability to operate a prosthetic hand, the higher the percentage of daily activities are performed without difficulty.
Methods
This study had a prospective, cross-sectional design.
Participants and procedure
Inclusion criteria were age between 3 and 17 years and being accustomed to use myoelectric prosthesis. A sample of 62 children with transversal upper limb reduction deficiency was recruited from the Limb Deficiency and Arm Prosthetic Centre (LDAPC), Region Örebro County in Sweden between 2012 and 2014. As a clinical routine at the LDAPC, all children with transverse upper limb reduction deficiency are fitted with passive prosthesis at 6 months of age and first fitted with myoelectric prosthesis at around age 3. One-third of the sample was right-sided prosthetic users and 50% of the sample was full-time prosthetic wearers. Demographic characteristics of the participants are shown in Table 1. The Regional Ethics Committee Review Board of Uppsala (reg nr 2009/231, amendment 2012-11-21) approved the data collection. All subjects provided written informed consent prior to inclusion.
Participant characteristics.
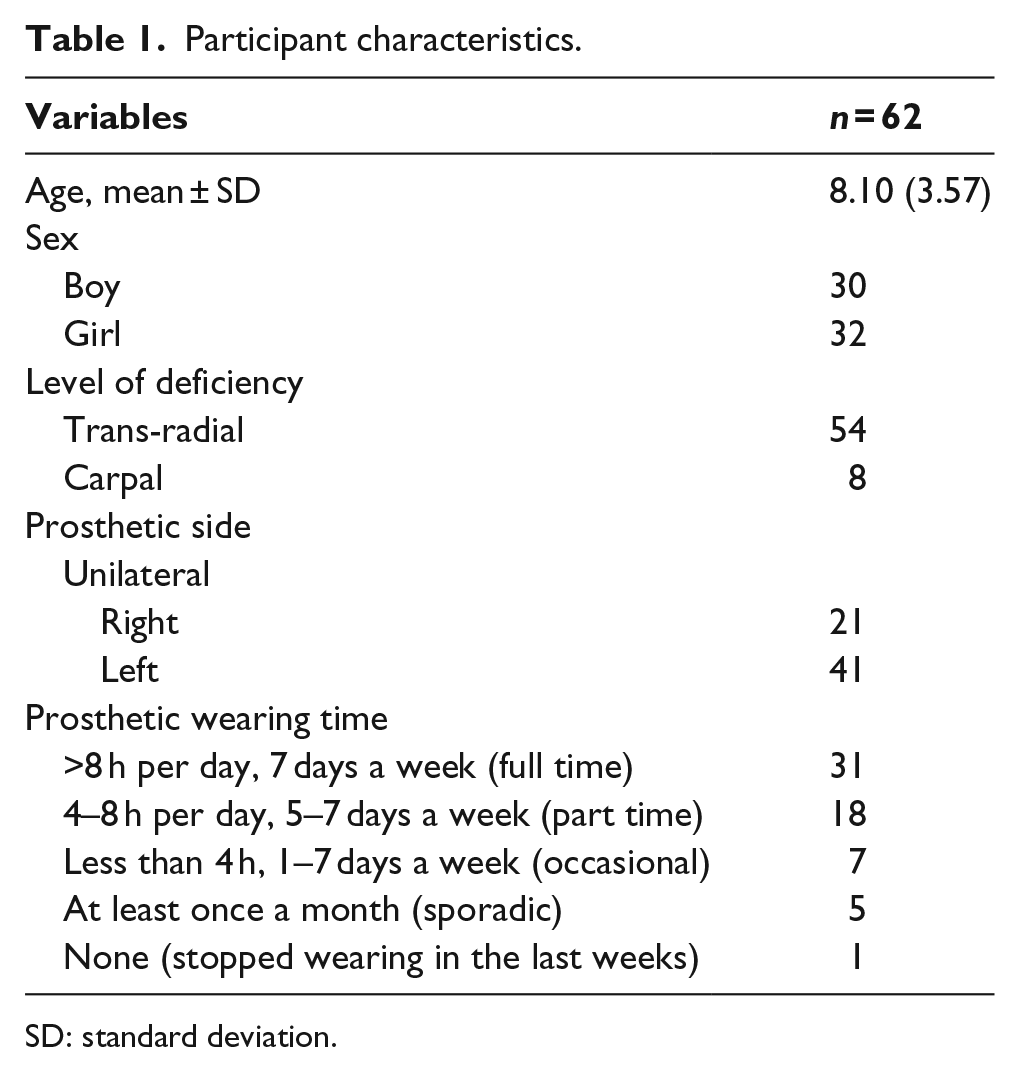
SD: standard deviation.
Instrumentation
Assessment of Capacity for Myoelectric Control
The ability to operate a prosthetic hand was assessed by the Assessment of Capacity of Myoelectric Control (ACMC).4,10–13 The ACMC is an observational based measure that assesses how well a myoelectric prosthesis user operates a myoelectric prosthetic hand. An ACMC training course is given to all ACMC raters. During an ACMC assessment, a certified ACMC rater observes how the prosthesis user operates the myoelectric hand in a bimanual activity and scores the 22 ACMC items on a 4-point rating scale (3 – extremely capable; 2 – generally capable; 1 – somewhat capable; 0 – not capable). The item ratings are entered into the ACMC website 14 where an ACMC ability score ranging from 0 to 100 is calibrated using Rasch analysis. For this study, the non-converted Rasch scores (logits) ranging from −4.09 to +8.07 logits were used. Higher logit scores indicate higher capacity.
Prosthetic Upper Extremity Functional Index
The Prosthetic Upper Extremity Functional Index (PUFI) is a client-reported questionnaire that evaluates the extent to which a child uses prosthesis for daily activities and the ease of performing these activities using prosthesis, during the last 2 weeks.6,7 In 2006, we started to use the authorised Swedish version of PUFI in the LDAPC as standard clinical procedure to evaluate daily activity performance among the children. The young child version (age 3–6) has 26 bilateral activities while the older child version (age 7–17) has 38 bilateral activities. The young child version is completed by the child and the parent together while the older child version is completed by the child. On each activity, the child answers a number of questions. One question is about ease of performance – ‘how well do you/your child do the activity with the prosthesis?’ and five options are given, ranging from ‘cannot do’ to ‘no difficulty’. The number of activities that are performed with ‘no difficulty’ are divided by the number of activities that are performed using prosthesis, producing the proportion of activities conducted with no difficulty. This is used to measure the ‘ease of performance’ proportion for this study.
Prosthetic wearing time
Prosthetic wearing time was collected using a client-rated scale that has been used earlier in other studies to classify wearing time.4,15 The scale has five categories (more than 8 h daily, 4–8 h daily, less than 4 h in 1–7 days a week, at least once and a month, not used in the last weeks). For this study, these categories were divided into two groups: full-time users and non-full-time users.
Procedure
Information about the study was given twice to the family and the children, once sent to their homes and once given when they arrived at the LDAPC for their regular clinical visit. Formal written consents were obtained directly from the participants (aged 15–17) or from the parents.
The ACMC assessments and PUFI questionnaires of children who visited the clinic were collected as a regular clinical routine for the LDAPC. During the clinical visit, the occupational therapist (an ACMC-certified rater) asked the child to perform a bimanual activity. Using the ACMC, the occupational therapist observed how the child operated the prosthesis and scored the ability on the ACMC scoring sheet. 16 In all, six occupational therapists (ACMC-certified raters) performed the data collection. Fair to excellent agreements were previously shown in inter-rater reliability in ACMC.10,12 During the same visit, the child (accompanied with one parent if between age 3 and 6) filled in the PUFI questionnaire. Prosthetic wearing time was collected verbally from the child or the parent. Information on age, sex and prosthetic side was retrieved from the patient records.
Data analysis
Descriptive statistics was used to present ACMC logit scores and the PUFI ease of performance percentage according to participant demographics. Spearman coefficient was used to assess the correlation between the ACMC logit scores and the PUFI ease of performance percentage. T-tests were used to examine differences in ACMC logit scores and the PUFI ease of performance percentage regarding prosthetic wearing time, sex and prosthetic side.
Generalised linear model with logit link and the binomial family was used to examine the association between ACMC logit score and PUFI proportional ease of performance. Robust standard errors were obtained. Prosthetic wearing time, sex, age (continuous) and prosthetic side were used as controls. After unadjusted analysis was conducted for each variable, multivariable regression models adjusting for prosthetic wearing time, sex, age (continuous) and prosthetic side were performed. The exponentiated estimates are the relative difference in proportional ease of performance. This is interpreted as the relative change in the proportional ease of performance by the levels of explanatory variables. Furthermore, for the ease of understanding, the percentage points are computed based on the estimated ratio. Data analysis was performed using SPSS 23 and Stata 14/SE.17,18
Results
Capacity – ACMC logit scores
On average, the whole sample was generally capable in operating myoelectric prostheses (Table 2). Full-time prosthetic wearers showed significantly higher mean ACMC score than non-full-time wearers (t-test p < 0.001). As the prosthetic wearing time increased, the ACMC score also increased (Figure 1). The older age group had significantly higher mean ACMC score compared to the younger group (p < 0.001) while there was no significant difference by sex (p = 0.747) and prosthetic side (p = 0.591). Among the full-time wearers, the older group (age 7–17, n = 21) also had significantly higher mean ACMC score (p = 0.04) compared to the younger group (age 3–6, n = 10).
Distribution of prosthetic capacity scores and proportional ease of performance by the levels of wearing time and demographic characteristics, as measured by ACMC and PUFI.
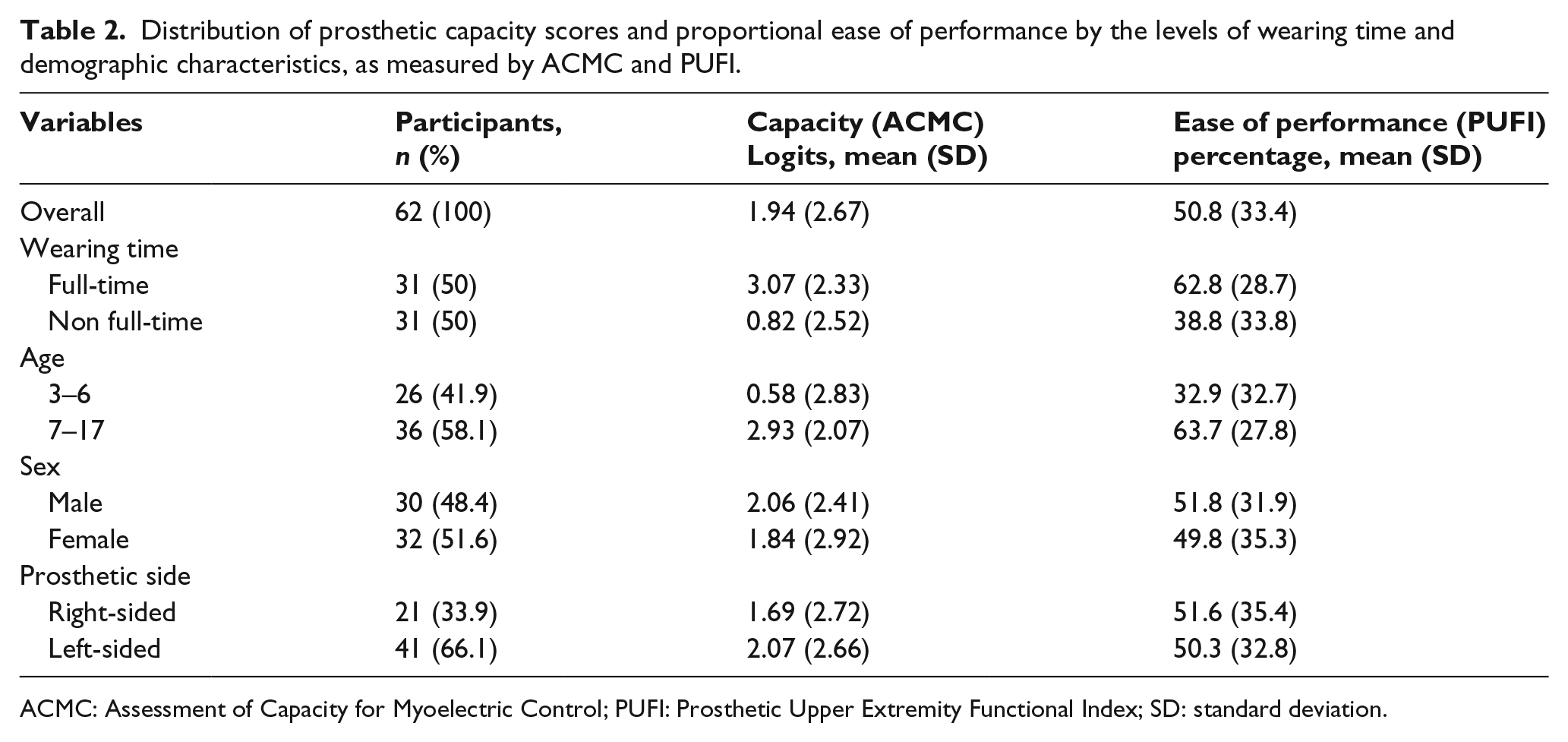
ACMC: Assessment of Capacity for Myoelectric Control; PUFI: Prosthetic Upper Extremity Functional Index; SD: standard deviation.
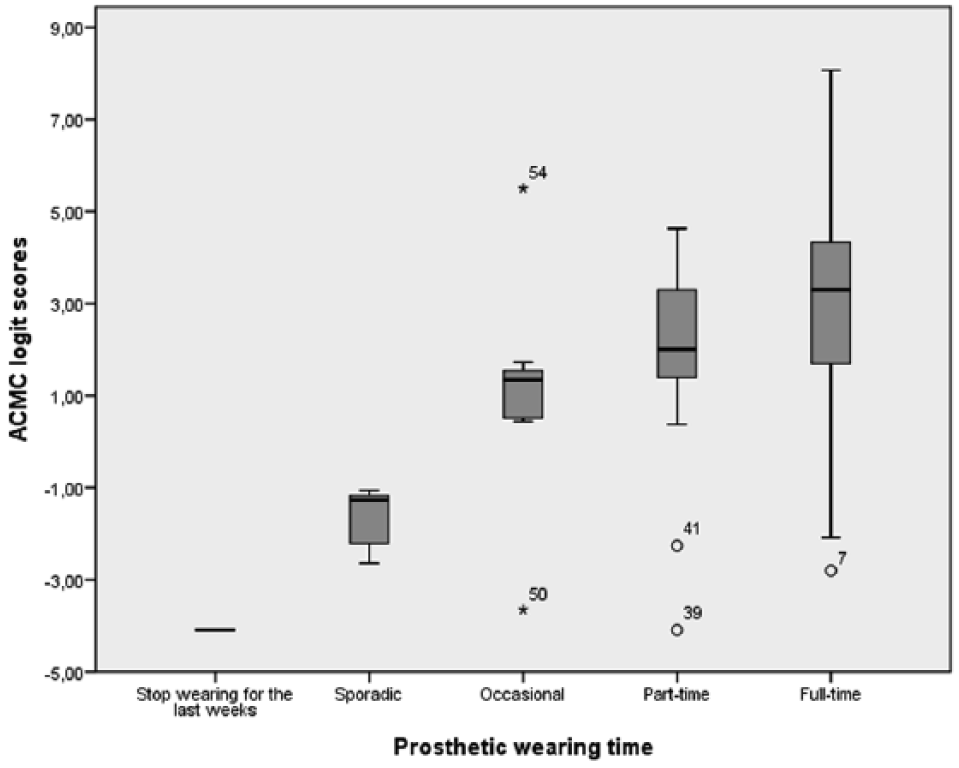
ACMC logit scores of capacity in relation to prosthetic wearing time.
Performance – PUFI proportional ease of performance
Children aged between 3 and 6 performed on average 22 out of 26 PUFI activities (85%) and children between age 7 and 17 performed on average 30 out of 38 (82.5%). The whole sample showed an average proportional ease of performance with a significant higher mean percentage in full-time prosthetic wearers than in non-full-time prosthetic wearers (p < 0.001). As the prosthetic wearing time increased, the proportional ease of performance also increased (Figure 2). Significant difference was also found in the proportional ease of performance between age group 3–6 and age group 7–17 (p < 0.001). No significant difference was found regarding sex (p = 0.810) and prosthetic side (p = 0.890). Among the full-time wearers, the older group (age 7–17, n = 21) also had significantly higher proportional ease of performance (p = 0.02) compared to the younger group (age 3–6, n = 10).
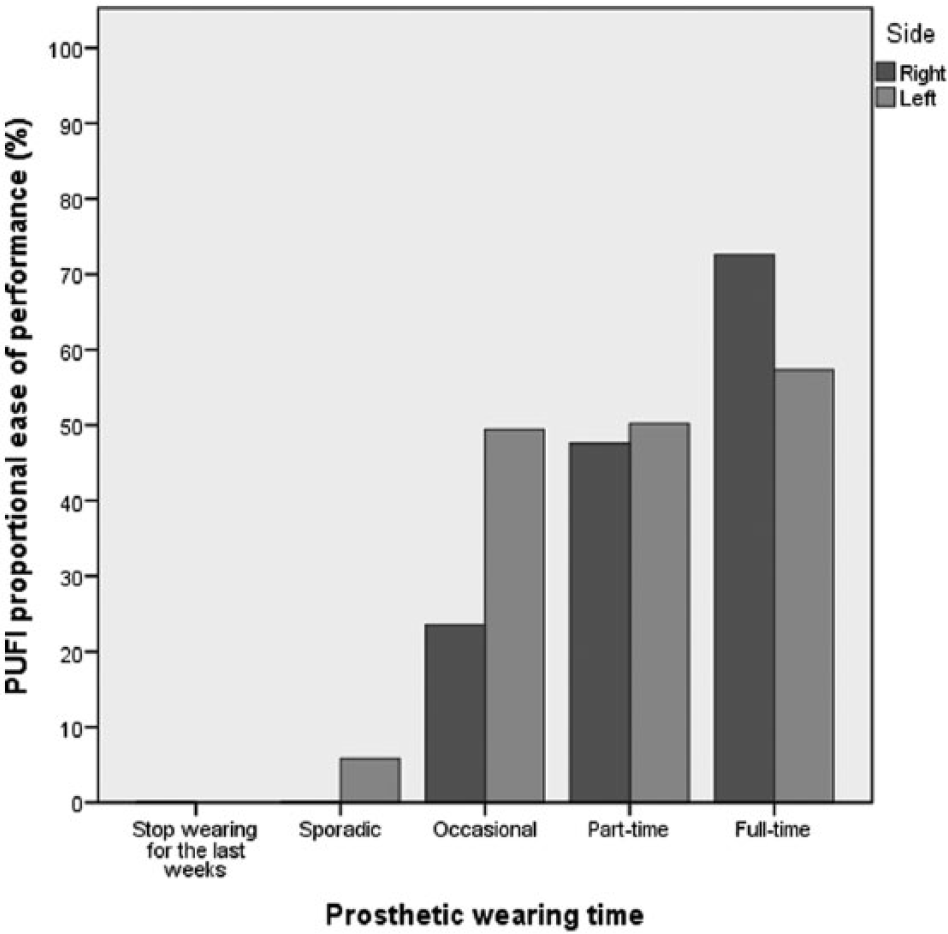
PUFI proportional ease of performance in relation to prosthetic wearing time.
Correlation between ACMC logit scores and PUFI proportional ease of performance
A strong correlation (Spearman = 0.75) was found between the ACMC logit scores and the PUFI proportional ease of performance. From the scatterplot (Figure 3), it is shown clearly that the higher the ACMC logit score, the higher the proportional ease of performance. Children with −0.1 logit score had less than 30% of proportional ease of performance.
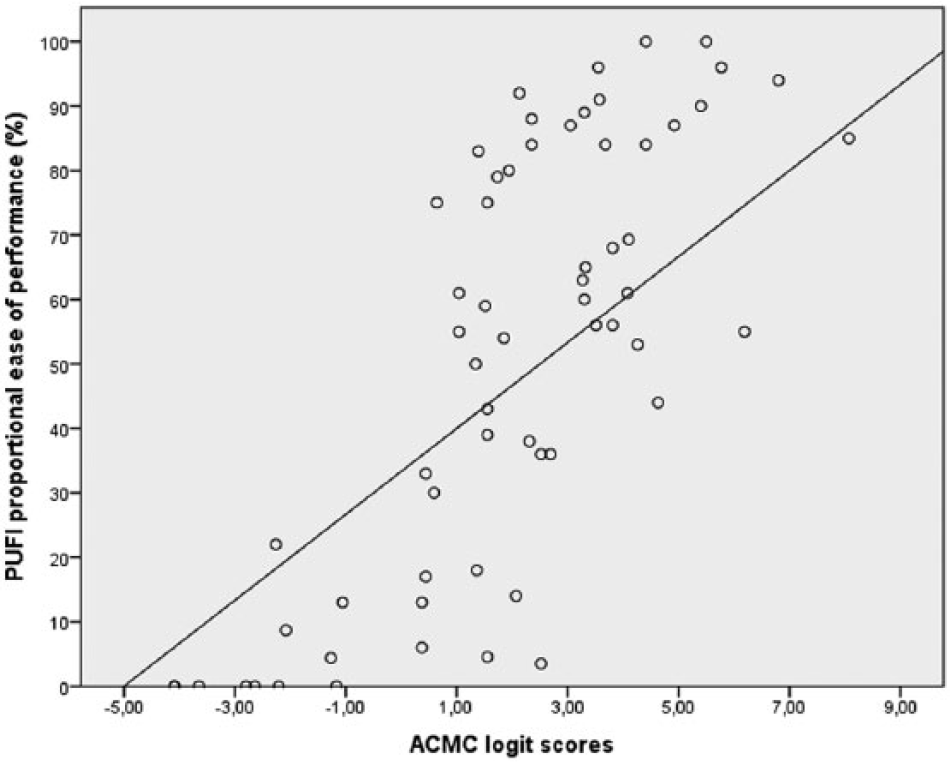
Scatterplot of the ACMC logit scores of capacity and the PUFI proportional ease of performance.
Association between ACMC capacity score and PUFI proportional ease of performance
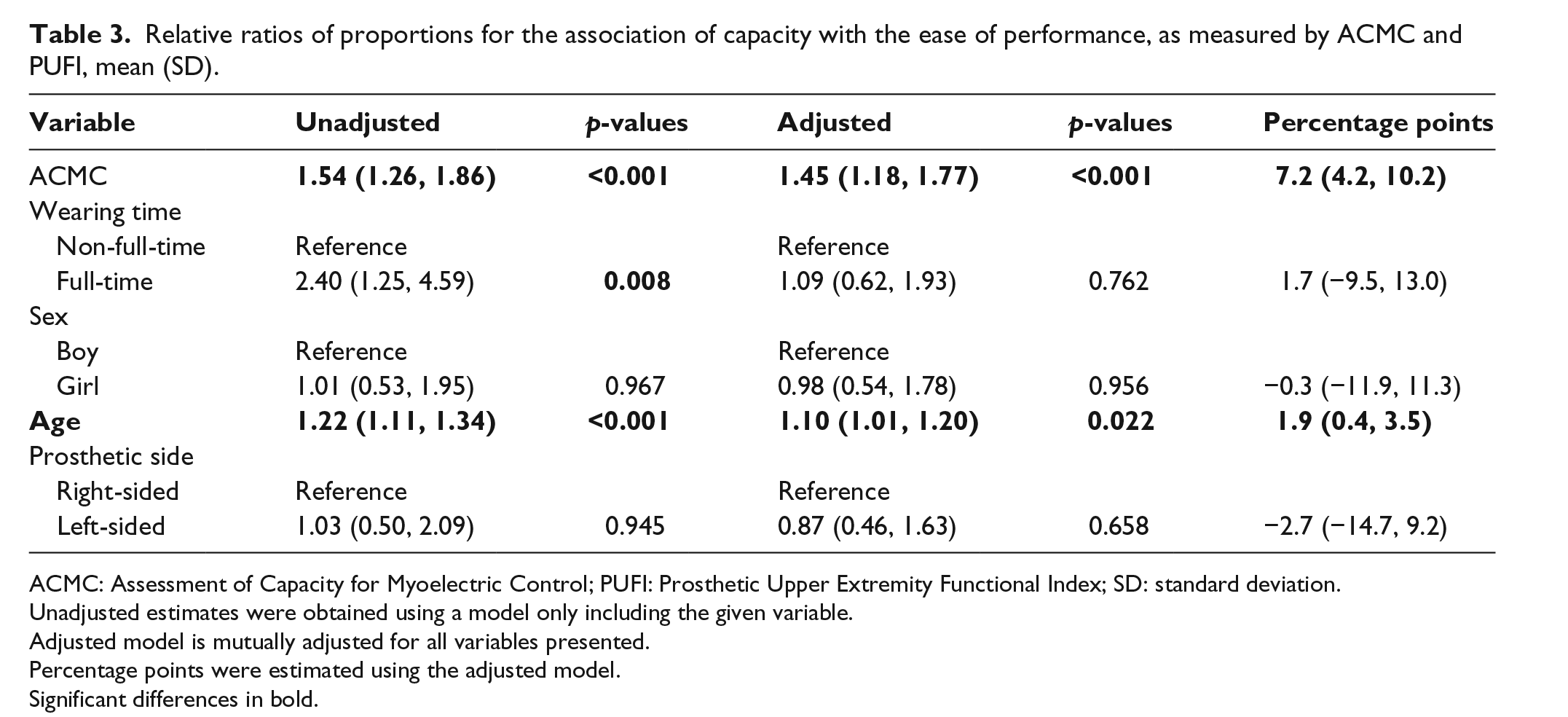
In the unadjusted analysis, capacity, prosthetic wearing time and age were associated with increased proportional ease of performance (Table 3). By 1 unit increase in ACMC, the ratio of proportional ease of performance increased by 54% in the unadjusted model, which is equivalent to 8.5 percentage points (data not shown). Compared with non-full-time wearers, full-time wearers showed significantly higher likelihood of proportional ease of performance, equivalent to 21.5 percentage points.
Relative ratios of proportions for the association of capacity with the ease of performance, as measured by ACMC and PUFI, mean (SD).
ACMC: Assessment of Capacity for Myoelectric Control; PUFI: Prosthetic Upper Extremity Functional Index; SD: standard deviation.
Unadjusted estimates were obtained using a model only including the given variable.
Adjusted model is mutually adjusted for all variables presented.
Percentage points were estimated using the adjusted model.
Significant differences in bold.
In the adjusted model (Table 3), capacity retained significant association with ease of performance, and by 1 unit increase in the ACMC score, the ratio of proportional ease of performance increased by 45% (equivalent to 7.2 percent points). However, prosthetic wearing time was no more associated with ease of performance. Age remained significantly associated with increased proportional ease of performance. This implies that capacity and age are independently associated with the proportional ease of performance, but not wearing time once other variables are accounted for.
Discussion
In this study, we examined whether higher score in the ability to operate a prosthetic hand is associated with higher percentage of daily activities that are performed without difficulty. We found that as the ability for prosthetic control (ACMC) increases, ease of performance also increases. Full-time prosthetic wearers had an average of better prosthetic control and less difficulty in daily prosthetic use. Prosthetic wearing time did not retain independent association with performance, whereas ACMC remained being associated with the ease of performance. The ACMC as an independent variable was the strongest among the predictor variables.
This is the first finding in the field of upper limb prosthetics that shows that a capacity measure can be a predictor for performance in real-life environment. A recent study on children with congenital hand differences, being non-prosthetic users, also showed that a capacity measure can predict performance measure. 9 Together with this study finding, this suggests that it is possible to predict performance using capacity measures in children with upper limb reduction deficiency. Despite the small sample in this study, these findings have an important implication for clinicians and prosthetic providers. For clinicians, the ACMC scores may serve as an indicator to predict the difficulties that the children may encounter in their home environment. This prediction can help the clinician to make decisions, such that if the child requires more control training or is ready to move on to learn more complex tasks. From an economical perspective, it could be convenient for clinicians to predict difficulty in prosthesis use in home environment by ACMC assessments.
Despite the limitations of current prostheses in terms of mechanical and myoelectric functions, 19 this study finding shows that upper limb prostheses do facilitate the performance of daily activities if the users have adequate capacity. Prosthetic training has been proven to be useful to increase the ability to operate a prosthetic hand.20–22 Researchers suggested that the prosthetic skills of small children between 3 and 6 years are in the process of development and repeated practice is required to integrate their prosthetic skills into daily task performance. 6 Children aged 7–17 years have a significant higher ACMC score and proportional ease of performance than children aged 3–6 years. This suggests that both capacity and daily activities that are performed without difficulty increase with age. The children in our sample received regular prosthetic training and some of them had taken part in a 1-week intensive training. One-week intensive training with 6 h/day has previously been proven to improve ACMC scores in a small sample of paediatric prosthesis users. 23 A prospective study to compare PUFI scores in children receiving either intensive training or regular training would provide us valuable information if intensive training would have an immediate or different impact on prosthesis use in everyday life compared to regular training.
All children, with or without upper limb reduction deficiency, are expected to participate in a wide range of activities and PUFI includes self-care activities and leisure activities that are among those that are most relevant for children. The children in our sample performed most of the PUFI activities independently. This is similar to another PUFI study with European children where 84% of the PUFI activities were performed. 24 This suggests that using prostheses may increase independent performance of activities.
As prosthetic wearing time increased, the range of ACMC scores became wider (Figure 1). Some full-time wearers had high ACMC scores whereas some had low ACMC scores. The ones with low ACMC scores were children between age 3 and 6 (n = 10). This younger group had significantly lower ACMC scores and PUFI scores than the older group. Low ACMC scores and low PUFI scores among these young full-time wearers can be explained by their short experience with myoelectric control. The younger children had switched from passive to myoelectric prosthesis 1–3 years ago and it will take them some years to reach a high ACMC score and great ease of activity performance. Longitudinal studies that follow the development of full-time prosthetic wearers will provide us more valuable information about the relationship between prosthetic control and ease of performance in this group.
Another important factor that may affect the capacity and performance scores is prosthetic wearing time. Wearing the prosthesis daily gives the opportunity to the child to use the prosthetic hand when it is needed, thus practising the performance skill. Full-time prosthetic wearers were found to have a higher ability in operating their hands than those who are part-time and sporadic wearers. 11 Although it is known that adult prosthesis users often wear the prostheses for cosmetic purposes,25,26 younger children tend to use their prosthetic hands actively when they are wearing them. 27 The finding that full-time prosthetic wearers have a significantly higher capacity score and proportional ease of performance than non-full-time prosthetic wearers suggests that children use their hands when they are wearing them. Regular use of prostheses may, thus, be recommended for children.
Study limitations
There were several study limitations. The sample was small and recruited from one centre only. As many of these participants came to the LDAPC for prosthetic training and new prosthetic fitting, they were probably more active and motivated in using their prostheses in their home environment. Furthermore, the study result cannot be generalised to children with acquired amputation, higher level of amputation and other types of prostheses. Another study limitation was non-blinding of the therapists that assessed the children. The therapists knew the children and this may have influenced the therapists’ ACMC assessments. The third study limitation could be an over-estimation of proportional ease of performance; the children may have rated no difficulty in the activities more often than the parent together with the child. Also, as the study was cross-sectional, temporal association was not possible to ascertain. Those who performed activities without difficulty may be more motivated to wear prostheses more often and longer, hence, achieving higher ACMC score.
Conclusion
In conclusion, practising capacity for control may reduce barriers in the environment and facilitate participation in daily activities for children with myoelectric prosthetic hands. Future studies using case–control design or longitudinal design are recommended to confirm whether capacity measures can predict performance.
Footnotes
Acknowledgements
The authors would like to thank all the children, parents and occupational therapists for their time and contribution to this study.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.