
Abstract
Background:
The 2008 Sichuan Earthquake resulted in many amputees, yet due to the rare incidence, few studies have explored the rehabilitation outcomes and quality of life of bilateral lower limb amputees after major natural disasters.
Objectives:
To evaluate rehabilitation outcomes of 17 young and adult bilateral lower limb amputees under the StandTall rehabilitation programme and to identify factors associated with successful functional recovery of bilateral amputees after large-scale disasters.
Study Design:
Cross-sectional study.
Methods:
Mobility (amputee mobility predictor), prosthesis use (Houghton Scale) and health-related quality of life (Trinity Amputation and Prosthesis Experience Scale, Short Form 12) were evaluated through questionnaires and performance-based assessments. Means of scores were compared using T-tests.
Results:
Subjects with bilateral through-knee or transtibial amputations had less activity restriction (p < 0.01) and higher mobility (p = 0.03). Subjects using prostheses more than 50% waking time had better general adjustment (p = 0.02) and less functional restriction (p = 0.01). Exercise and education were associated with higher mobility (p = 0.06) and mental quality of life, respectively (p = 0.09).
Conclusions:
Amputation level and knee joint salvage, prosthesis use, exercise and education were associated with better rehabilitation outcomes including ambulation, adjustment and quality of life in bilateral lower limb amputees from the 2008 Sichuan Earthquake.
Clinical relevance
The study examined a unique group of traumatic bilateral lower limb amputees who were young and healthy before having traumatic amputations from a single episode of natural disaster. The factors associated with better functional recovery after the earthquake were investigated and may support future development of post-disaster rehabilitation strategies for bilateral lower limb amputees.
Keywords
Background
The 2008 Sichuan Earthquake, measured at 7.9 on Richter Scale, struck the Sichuan Province on 12 May 2008, affecting more than 45 million people. It was the deadliest and strongest earthquake in China since the 1976 Tangshan Earthquake, causing over 88,000 deaths and 350,000 injuries; students accounted for 7% death in Sichuan Province.1–3 Many of the injuries were severe, including fractures, amputations and spinal cord injuries; long-term rehabilitation to optimise functional restoration and prevent medical complications was crucial.
In view of the sudden increased demand for medical care and rehabilitation of earthquake victims, StandTall was initiated by a group of orthopaedic specialists in Hong Kong immediately after the earthquake. The non-governmental organisation was supported by funding from the Hong Kong government and voluntary donations. The rehabilitation team was multi-disciplinary including doctors, physiotherapists, prosthetists, occupational therapists, nurses and psychologists. The rehabilitation team participated in all stages, including post-operative care, pre-prosthetic training and planning, prosthetic prescription and training (supported by Ottobock Ltd.), community integration, vocational rehabilitation and follow-up. The team members worked closely in planning and implementing comprehensive rehabilitation programmes to meet the physical, psychological and functional needs of the patients, with specific care to children with a growing skeleton and bilateral amputees who have more complex needs. StandTall has also regularly organised home visits, clinics and training in schools of hard-hit areas, emphasising the importance of outreach. All victims with traumatic injury from the Sichuan Earthquake are eligible for the StandTall rehabilitation programme for free. From weekly hospital visits in the acute phase to regular 3-to-6 month follow-up sessions after patients’ conditions have stabilised, StandTall has organised over 60 multi-disciplinary clinics (each time for 1–3 days) since 2008, serving over 550 earthquake victims.
Musculoskeletal diseases and trauma were always a major medical challenge in large-scale natural disasters, for example, the Northridge Earthquake, Kashmir Earthquake, South Asia Tsunami and Myanmar cyclone, accounting for 15%–45% of diseases seen in post-disaster clinical settings. 1 Trauma and injuries were the major causes of death in the Sichuan Earthquake. Prevalence of crush syndrome due to prolonged entrapment was around 1%. Amputation was a common medical intervention after major earthquakes, such as the earthquakes in Marmara, Turkey, Kashmir, Haiti and Sichuan Earthquake. 2 In a cross-sectional study of 28,008 Sichuan Earthquake victims conducted 1 month after the earthquake, 255 (0.9%) received amputations, of which 18 (0.06%) received bilateral lower limb amputations. 4 Amputation posed physical and psychological challenges, including drastic changes in physical ability, lifestyle and self-perception.2,5,6 In existing literature on bilateral amputees, most studies consist of subjects who were civilians receiving amputation for vascular diseases or veterans who received amputation during war, and review articles often include amputation of mixed causes, making the evaluation and comparison of rehabilitation outcomes difficult. There is no study on young, traumatic bilateral amputees from a single episode.
This study aimed to report the rehabilitation outcomes (mobility, prosthesis use and quality of life (QoL)) of bilateral lower limb amputees from the Sichuan Earthquake, to explore potential factors associated with good rehabilitation outcomes and to situate the findings in our understanding of the unique circumstances that arise in rapid-onset disaster.
Methods
Design
This was a cross-sectional study. Data were collected through a performance-based ambulation assessment and questionnaires at clinic, school and home visits in Sichuan between December 2014 and May 2015. Official agreement was signed with the Sichuan Provincial People’s Hospital in collaboration in research and education, and this was a joint research with ethical approval from the Sichuan Provincial People’s Hospital. Ethical approval was also obtained from the ethics review board of the joint New Territories East Cluster (NTEC)/Chinese University of Hong Kong (CUHK) joint-institutional ethics committee. This study was in compliance with the Declaration of Helsinki and ICH-Good Clinical Practice (GCP) guideline. Informed consent was obtained from all subjects, and for subjects under the age of 18 years (adult), the informed consent was obtained from either parents or legal guardians.
Participants
Bilateral lower limb amputees were recruited from StandTall. Inclusion criteria were (1) received bilateral lower limb amputations due to injury from the 2008 Sichuan Earthquake and (2) admitted to and under the care of StandTall prior to the start of study. Subjects with chronic medical conditions before the earthquake were excluded.
All the subjects were young and healthy before the earthquake and traumatic bilateral amputation. They had strong will and stamina to achieve. Some even trained themselves to be top athletes. In addition, all of them had been under the StandTall rehabilitation programme, thus appropriate for reviewing long-term rehabilitation outcomes after a major natural disaster.
Outcome measures
Amputee mobility predictor (AMP) is an amputee-specific tool for predicting ambulatory potential. 7 The AMPPro version was used to assess subjects’ functional mobility on prostheses. Sitting and standing balance, transfer and gait skills and use of assistive device were scored and reported out of a total score of 47. The score was also converted to the Medicare Functional Classification Levels (MFCL).
The Houghton Scale evaluates prosthesis use of lower limb amputees. Time duration on prostheses, context of prosthesis use, use of ambulatory aids and confidence in walking over various outdoor terrains were reported out of a total score of 12. Houghton et al. 8 define that score ⩾6 indicates independent mobility on prostheses in household, while score ⩾9 implies successful and satisfactory rehabilitation. The Houghton Scale differentiates between part-time and full-time walkers, therefore suitable for assessing functional rehabilitation in young, healthy post-earthquake amputees. 9
QoL was assessed using the Trinity Amputee and Prosthesis Experience Scale (TAPES) and Short Form 12 (SF12). TAPES is specific for lower limb amputees fitted with prosthesis, evaluating their psychosocial adjustment, activity restrictions, prosthesis satisfaction as well as residual limb pain, phantom limb pain and general health status.10,11 The SF12 is a non-specific questionnaire widely used in different patient populations on health-related QoL. It covers eight dimensions – physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health. Results were calculated into two meta-scores – the Physical Component Summary and the Mental Component Summary. Each was expressed as a value between 0 and 100, a higher score reflecting better QoL. 12
Data analysis
Means of outcome measures by demographics, prosthesis use and exercising hours were compared using T-tests. Data analysis was performed by IBM SPSS version 22.0 (Armonk, NY: IBM Corp). A two-tailed p ⩽ 0.05 was considered statistically significant, although p ⩽ 0.1 was also considered in this study due to the small sample size limited by the rare incidence of bilateral lower limb amputees.
Results
Out of 32 bilateral lower limb amputees under StandTall, 17 attended the multi-disciplinary clinics or outreach visits during the study period and were recruited into this study. They satisfied all inclusion criteria and had good past health before the earthquake. One subject had T12 vertebrae thoracic spinal cord injury and left upper limb amputation in addition to bilateral transfemoral amputations, one bilateral transfemoral amputee had right brachial plexus injury and one bilateral transfemoral amputee had thoracolumbar vertebral compression fracture; other subjects reported no significant concomitant health conditions or injuries from the earthquake.
Demographics of subjects were shown in Table 1. The average age at the time of study was 25.6 (SD 7.6), and four (23.5%) were younger than 18 years at the time of amputation. Eight (47.1%) were males and nine were females (52.9%). The average prosthesis wearing time was 8.9 h/day (SD 2.8). The immobilisation period (from earthquake to first walking with prosthesis) was 7.9 months (SD 4.7 months).
Demographics of subjects.
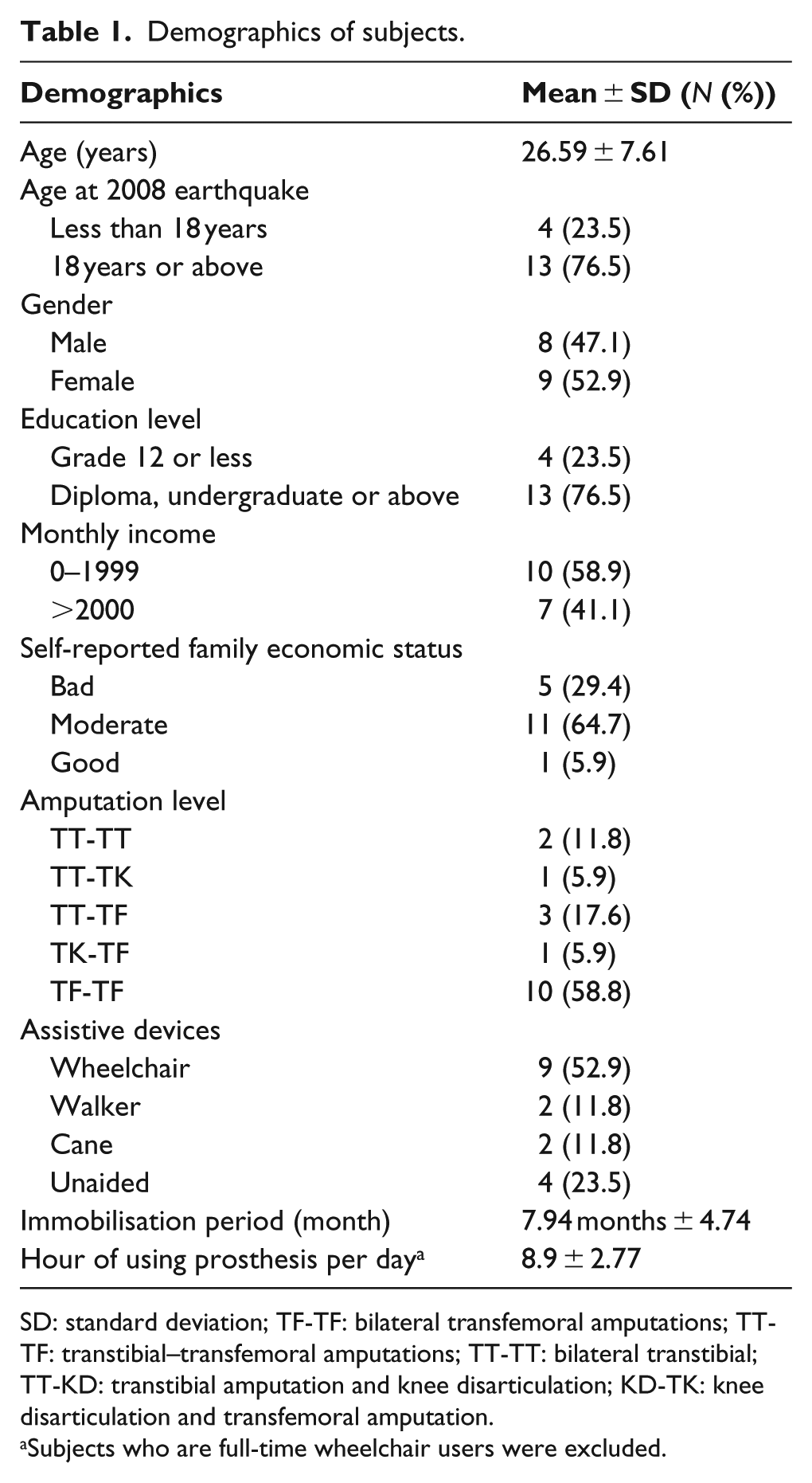
SD: standard deviation; TF-TF: bilateral transfemoral amputations; TT-TF: transtibial–transfemoral amputations; TT-TT: bilateral transtibial; TT-KD: transtibial amputation and knee disarticulation; KD-TK: knee disarticulation and transfemoral amputation.
Subjects who are full-time wheelchair users were excluded.
Amputation level
In all, 10 (58.8%) had bilateral transfemoral amputations (TF-TF), 3 (17.6%) had bilateral transtibial–transfemoral amputations (TT-TF), 2 (11.8%) had bilateral transtibial (TT-TT) amputations, 1 (5.9%) had transtibial amputation and knee disarticulation (TT-KD) and 1 (5.9%) had knee disarticulation and transfemoral amputations (KD-TK).
For assistive device, nine subjects (52.9%) used wheelchairs, two (11.8%) used crutches, two (11.8%) used walking sticks and four (23.5%) were unaided walkers. A majority of transfemoral amputees used wheelchairs; however, the use of assistive devices was not solely determined by amputation level; for example, a bilateral transfemoral amputee walked unaided while a bilateral transtibial–through knee amputee mainly relied on a wheelchair. The main rehabilitation outcomes were shown in Table 2.
Main rehabilitation outcome.
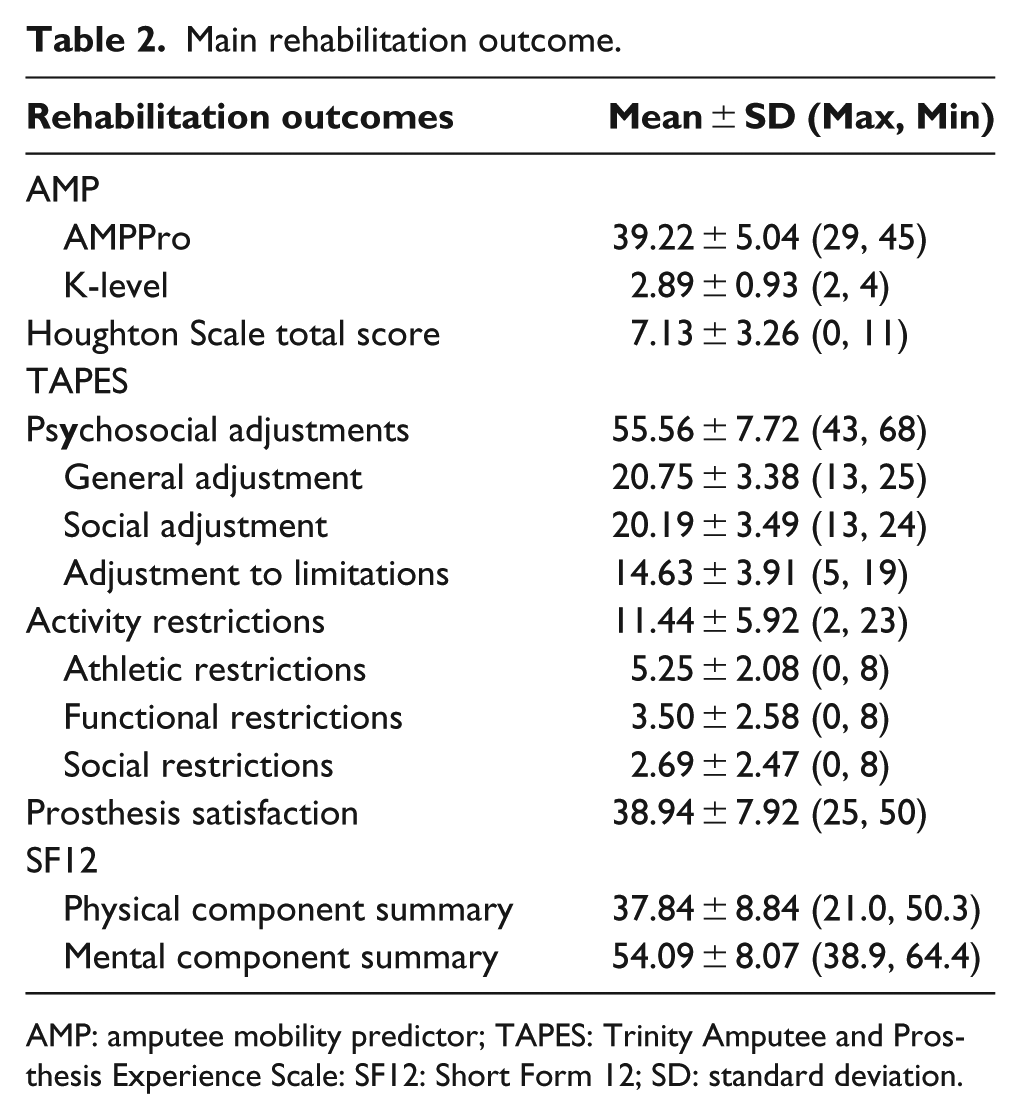
AMP: amputee mobility predictor; TAPES: Trinity Amputee and Prosthesis Experience Scale: SF12: Short Form 12; SD: standard deviation.
Mobility
AMPPro was completed by nine (52.9%) subjects who attended with prosthesis. Out of the nine, three (33.3%) achieved rehabilitation success as defined by AMP score ⩾43 (K4 level), two (22.2%) scored 37–42 (K3 level), and four (44.4%) scored 27–36 (K2 level). 7 One subject was excluded due to T12 spinal cord injury and upper limb amputation, and seven subjects could not complete AMPPro since they did not bring their prostheses or their prostheses were unfit for use.
Prosthesis use
Rehabilitation success, which is defined as Houghton Scale ⩾9 by Houghton et al., 8 was achieved by seven (43.8%) subjects; independent household mobility on prosthesis (scores 6–8) was obtained by two (12.5%). One subject was excluded due to T12 spinal cord injury and upper limb amputation.
Health-related QoL
Subjects who were prosthetically rehabilitated (Houghton Scale ⩾ 9) had better QoL, including better general adjustment (p = 0.021), less activity restriction (p = 0.008), less athletic restriction (p = 0.012) and less functional restriction (p = 0.001). They also scored higher in the physical component summary of SF12 (p = 0.083).
Comparison of subjects with different amputation levels
Significant differences in rehabilitation outcomes were observed between subjects with salvage of knee joint(s) (TT-TT, TT-TK and TT-TF) and those without (TK-TF and TF-TF; Table 3). Subjects with one or both knee joint(s) preserved achieved higher mobility (p = 0.03) (Figure 1) and better prosthesis rehabilitation (p = 0.004). All subjects with knee joint(s) salvage wore their prostheses more than 50% waking time, while 40% subjects with no knee joint salvage used prostheses for more than 50% waking time. Subjects with knee joint(s) salvage also had better general adjustment (p = 0.052), less activity restriction (p = 0.003), athletic restriction (p = 0.012) and functional restriction (p < 0.001; Figure 2).
Amputation level as a significant determinant of rehabilitation outcomes.
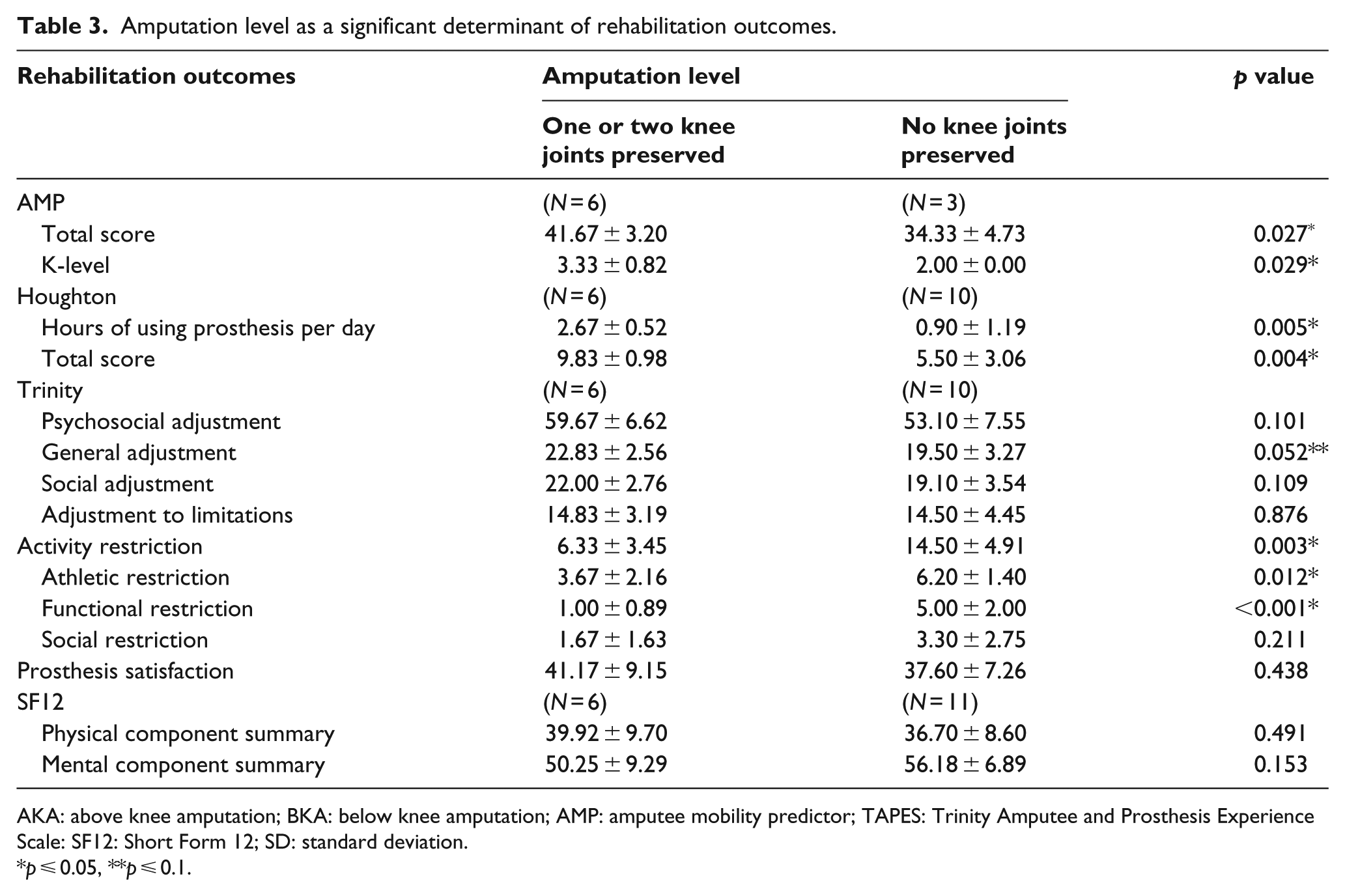
AKA: above knee amputation; BKA: below knee amputation; AMP: amputee mobility predictor; TAPES: Trinity Amputee and Prosthesis Experience Scale: SF12: Short Form 12; SD: standard deviation.
p ⩽ 0.05, **p ⩽ 0.1.
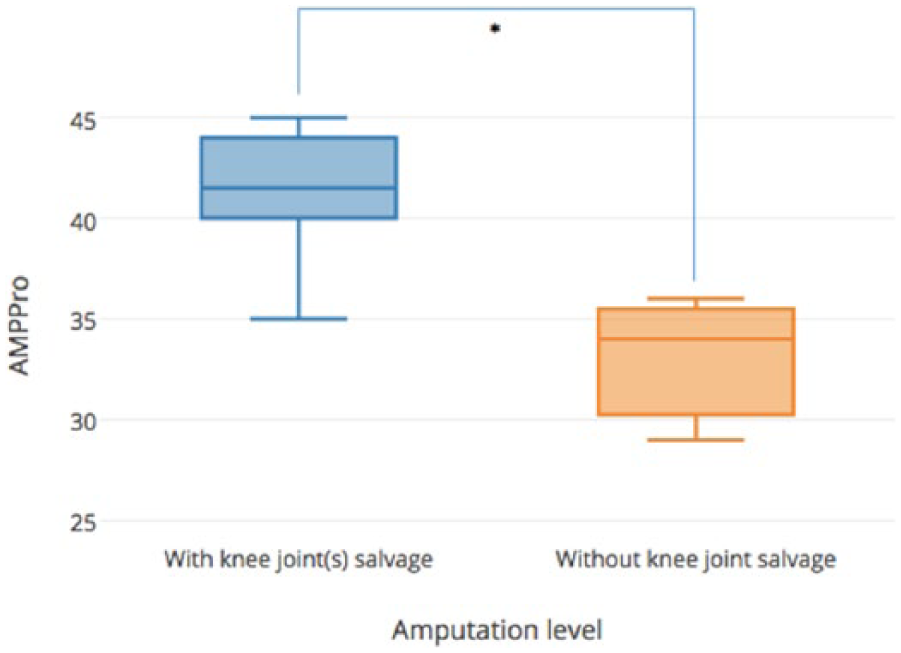
Amputation levels and mobility (AMPPro).
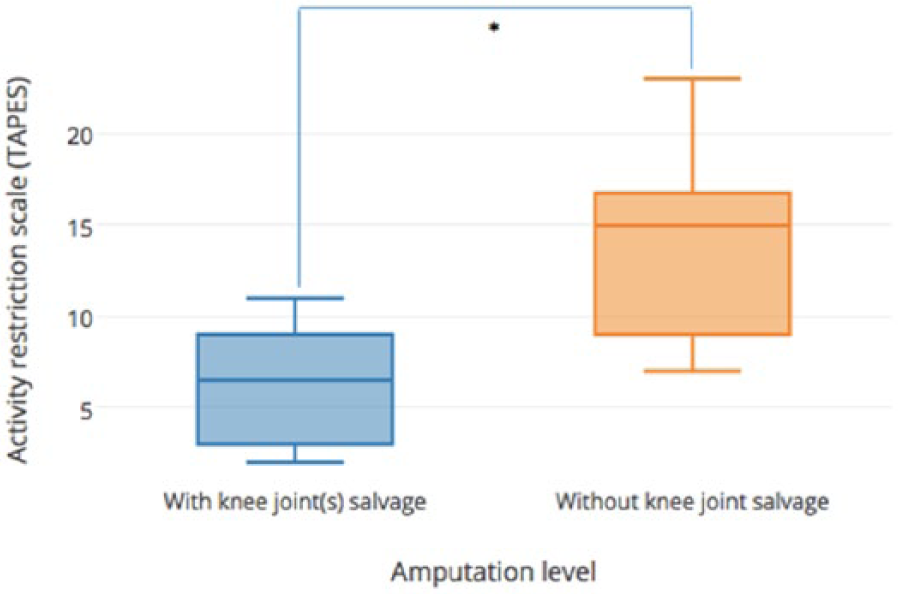
Amputation levels and activity restriction scale (TAPES).
In further sub-divisions, subjects with both knee joints preserved (TT-TT; n = 2) had less athletic restrictions (p = 0.069) than those with one knee joint salvaged (TT-TK and TT-TF; n = 4). Subjects with one knee joint salvage had higher mobility (p = 0.093), better prosthesis use (p = 0.013) and less activity restrictions (p = 0.021) comparing to subjects with no knee joint salvage (TK-TF and TF-TF; n = 11). The results supported benefits in mobility and health-related QoL with each additional knee joint salvage.
Association between prosthesis use and QoL
Prosthesis use was associated with better QoL. Subjects using prosthesis over 50% waking time had better general adjustment (p = 0.027) and less functional restriction (p = 0.010). This suggested that those who did not use prosthesis were likely the people at risk of poorer QoL (Figures 3 and 4).
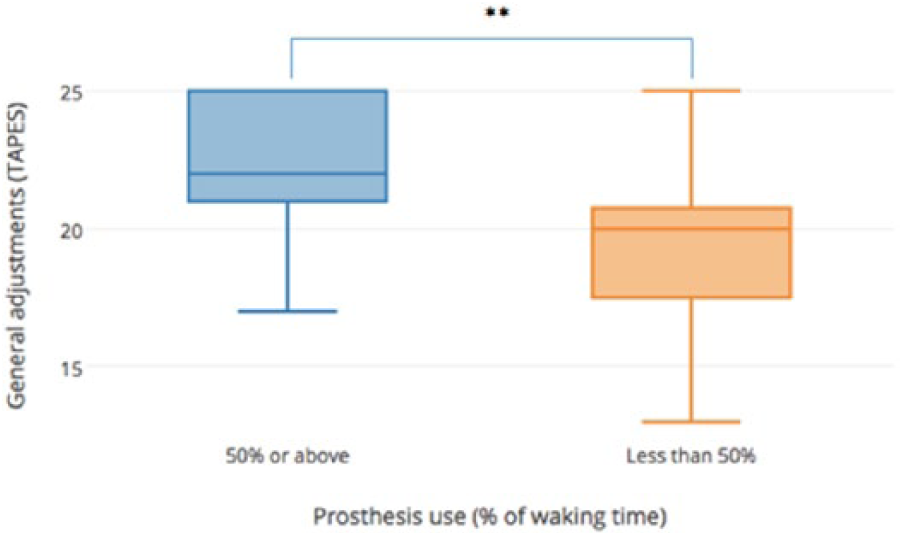
Prosthesis usage time and general adjustments (TAPES).
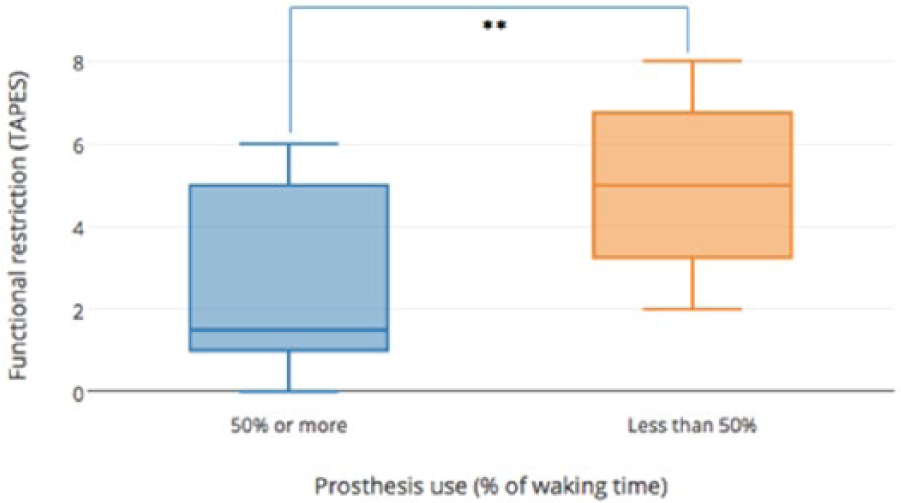
Prosthesis usage time and functional restriction (TAPES).
Association between exercise and mobility
The average exercising hours was 7.5 h per week (SD 9.16), ranging from no exercise to 24 h of exercise per week. Subjects with three or more exercising hours per week had higher mobility (p = 0.056).
Stump pain and phantom pain
In this study, nine (53%) subjects experienced stump pain, with an average frequency of 1.80 (SD 2.39) episodes in the past week. The average intensity was distressing (three out of five; interquartile range (IQR) 2–3) and caused mild interference with normal lifestyle (two out of five; IQR 1–3). Stump pain could be relieved in four (55.6%) subjects, such as by taking pain killers and massage.
Phantom pain was experienced by 12 (75%) subjects with an average of 2.08 (SD 1.80) episodes in the past week. The average intensity was distressing (three out of five; IQR 2.5–4) and had mild effects on normal lifestyle (two out of five; IQR 1–2). Phantom pain could be relieved in three (23.1%) subjects, by methods including resting, exercise, massage, therapy and warm bathing.
Age, the presence of stump pain and phantom pain showed no significant effects on rehabilitation outcomes.
Discussion
Our study reported the rehabilitation outcomes of a group of bilateral traumatic amputees from the 2008 Sichuan Earthquake. Our results suggested that amputation level and knee joint salvage, prosthesis use and exercise were associated with better rehabilitation outcomes including mobility, adjustments and QoL.
In the 2008 Sichuan Earthquake, due to the lack of experience and poor resilience at local level, the disaster rapid response work was mainly carried out by the People’s Liberation Army and the People’s Armed Police. The centralised political system ensured a determined and efficient relief response, and victims were quickly transferred to health facilities in over 20 cities and provinces to compensate for overwhelmed and inadequate medical resources in Sichuan Province.1,13 However, as patients’ conditions stabilised and they returned to Sichuan, a major challenge was the limited expertise, facilities and programmes in rehabilitation in the local province, which were inadequate to meet the sudden increase in rehabilitative needs after the earthquake. A large proportion of the amputees from the Sichuan Earthquake were young people with promising future and good past health before the disaster, they had a long life expectancy and are determined to achieve some trained themselves to be top athletes and some joined the healthcare profession to help others. StandTall recognised that a vigorous rehabilitation (through early mobilisation, advanced prosthesis installation and training, adaptive strategies, environmental modifications, long-term regular follow-up) was crucial for restoring function and independence of the earthquake amputees. During immediate relief, the first priority was lifesaving, and traumatic amputations were performed with little planning; therefore, long-term complications by scar tissues were common. In addition, schools were heavily hit in the earthquake and a fair number of amputees were students with growing skeletons. Due to the rapid bone growth, they needed more frequent prosthetic changes, and more than half of the bilateral amputees of StandTall received revision surgeries.
The rate of rehabilitation success in lower limb amputees varied greatly in past literature depending on the definition of ‘success’, 14 ranging from 5% to 90%.9,15 Bilateral lower limb amputee tended to have lower physical capability than unilateral amputees. 16 In this study, 33.3% subject achieved rehabilitation success in terms of mobility, attaining the highest K-level in AMP. For prosthesis use, 44% scored ⩾9 in Houghton Scale and obtained rehabilitation success, another 12.5% attained ‘independent mobility on prosthesis in household’. 8 Comparing with unilateral lower limb amputees in the StandTall rehabilitation programme, bilateral amputees had lower mobility, prosthesis use and physical QoL and more activity restrictions. 17 However, they obtained similar psychosocial adjustments and even better mental QoL than unilateral lower limb amputees, highlighting that despite more complex needs and physical impairment, we can hope for positive outcomes for bilateral amputees.
Our study found that distal amputation level, knee joint salvage in particular, was associated with better functional restoration in bilateral lower limb amputees, with benefits in mobility, prosthesis use and QoL. The finding was consistent with existing literature.18,19 The higher ambulation energy expenditure accounts for reducing mobility as amputation level moved proximal. According to the biochemical studies, the ambulation energy cost of unilateral transfemoral amputees is 40% higher than unilateral transtibial amputees, 20 and the energy expenditure of bilateral transfemoral amputees walking with prosthesis is 280% of unimpaired controls. 21
Prosthesis use was significantly higher in bilateral lower limb amputees with lower amputation sites. All subjects with knee joint(s) salvage used prosthesis over 50% of waking time with an average of 10 h per day, while only 40% of those with no knee joint salvage used prosthesis over 50% waking time. Prosthetic rehabilitation success (Houghton Score 9 or above) was associated with better general adjustment (p = 0.021), less activity restriction (p = 0.008) and physical QoL (p = 0.083). The positive correlation with prosthesis use and QoL prompted surgeons to pay serious consideration in preserving limb length and knee joint(s) when possible during operation.
Wheelchair assistance was high among amputees with no knee joint salvage. Out of 11 subjects with TK-TF or TF-TF amputations, 9 (81.8%) required wheelchair assistance and only 3 (27.1%) attended the session with prosthesis. A low mobility score did not necessarily reflect the capabilities and independence of participants, who used a range of adaptions and strategies to achieve their goals. This included independent living activities and high-level participation in sport (two bilateral transfemoral amputees were professional swimmer and table tennis player, respectively). In view of the long sitting duration of wheelchair users, prevention of hip flexion contraction was crucial. The common use of wheelchairs highlights a need for accessibility of infrastructure in post-earthquake reconstruction plans, such as barrier-free schools.
Bilateral amputees of this study had higher sports participation (76.4%; with an average of 7.5 h per week) in comparison with previous studies in Europe and United States on mixed unilateral and bilateral amputees (11%–61%). 22 Two bilateral transfemoral amputees were professional athletes, with over 20 exercising hours per week. Exercising ⩾3 h per week was associated with higher mobility (p = 0.056). The relationship could be bidirectional, amputees with high mobility could participate in sports with less restrictions, while exercise strengthen their physical fitness. Exercise should be promoted in post-disaster rehabilitation programmes of young and healthy amputees, which could enhance physical fitness and also increased patients’ involvement.
Phantom pain and stump pain are common complaints among amputees.6,23–25 An epidemiological study of 437 lower limb amputees reports prevalence of 86% and 68% for phantom and stump pain, respectively. 23 Prevalence of phantom pain decreased with time after amputation. 25 Our study was conducted 7 years after the earthquake, the time gap could allow better adaptation, thus a lower prevalence of 75% phantom pain and 53% stump pain. Phantom pain and stump pain had no significant effects on QoL and other rehabilitation outcomes.
Apart from attending to the physical functions, the psychosocial needs and mental status of earthquake amputees should also be carefully addressed in a comprehensive rehabilitation programme. Education level was an important factor of QoL for amputees.2,6 A prospective cohort of 72 amputees from the Sichuan Earthquake found that illiterate survivors with lower limb amputations has poorer QoL and life satisfaction. 2 This was consistent with our findings, and bilateral lower limb amputees with higher education level had better mental QoL (p = 0.089). Education can contribute to better coping strategies which facilitated adaptation after amputation, better mobilisation of resources and support and better employment opportunities. Students made up a fair proportion of amputees in the Sichuan Earthquake, and it was important to ensure that education opportunities were not denied due to their physical impairment. China’s first barrier-free school (Dujiangyan Youai School in Sichuan Province) started in 2009 and has admitted over 100 earthquake survivors with physical impairment. It regularly hosts clinics and training organised by StandTall and the Sichuan Provincial People’s Hospital, and it also offers student support services by trained mental health volunteers. This highlighted the value of community support and community-based rehabilitation in a post-disaster setting.
A review of the emergency medical response of the Sichuan Earthquake found that post-traumatic stress disorder, anxiety and depression remained high in hard-hit areas 1 year after the earthquake; the prevalence was 26.3%, 49.8% and 49.6%, respectively. 26 While this study briefly touched on the mental QoL of bilateral amputees, the effect of earthquake on their mental health, body image perception, self-esteem and life satisfaction was to be explored by further research, especially in adolescent amputees.
Limitations
The major limitation of the study was the small sample size, which was limited by the rare incidence of bilateral lower limb amputation. In a survey of 28,008 patients hospitalised in Sichuan 1 month after the earthquake, only 18 (0.0006%) received bilateral amputation. 4 StandTall has served a total of 32 bilateral lower limb amputees since 2008, and 17 attended the multi-disciplinary clinics or outreach visits during the study period and were recruited into this study. There was some loss of follow-up due to long commuting distance, relocation and loss of contact. The small sample made statistical analysis more difficult to reach significance; therefore, while conventionally p value was only considered significant when smaller than 0.05, a less stringent criteria of p value between 0.05 and 0.1 was also considered in the study.
The study was cross-sectional and conducted 7 years after the earthquake, amputees’ performance at different rehabilitation stages was not investigated, and causal relationships could not be established. Although the study was cross-sectional in design, data collection was carried out in two phases due to logistic limitations (e.g. limited time per visit for data collection and long travelling time for home visits of subjects living in remote areas). Selection bias was present, and patients who attended regular follow-up clinics and those who agreed to home visits were recruited into the study, suggesting better compliance and commitment to the rehabilitation programme in recruited subjects, and this could lead to more favourable rehabilitation outcomes.
Conclusion
Our study reported the rehabilitation outcomes in a group of traumatic bilateral amputees from the 2008 Sichuan Earthquake, and we found that potential factors associated with good rehabilitation includes distal amputation level and knee joint salvage, prosthesis use and exercise. With a rehabilitation like StandTall, even with complex needs on a background of large-scale rapid-onset emergency, we can hope for positive outcomes. These results may support the development of future rehabilitation strategies for bilateral lower limb amputees after natural disasters.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was financially supported by Otto Bock HealthCare Deutschland GmbH and Össur.