
Abstract
Ankle Foot Orthoses (AFOs) to promote walking ability are a common treatment in patients with neurological or muscular diseases. However, guidelines on the prescription of AFOs are currently based on a low level of evidence regarding their efficacy. Recent studies aiming to demonstrate the efficacy of wearing an AFO in respect to walking ability are not always conclusive. In this paper it is argued to recognize two levels of evidence related to the ICF levels. Activity level evidence expresses the gain in walking ability for the patient, while mechanical evidence expresses the correct functioning of the AFO. Used in combination for the purpose of evaluating the efficacy of orthotic treatment, a conjunct improvement at both levels reinforces the treatment algorithm that is used. Conversely, conflicting outcomes will challenge current treatment algorithms and the supposed working mechanism of the AFO. A treatment algorithm must use relevant information as an input, derived from measurements with a high precision. Its result will be a specific AFO that matches the patient's needs, specified by the mechanical characterization of the AFO footwear combination. It is concluded that research on the efficacy of AFOs should use parameters from two levels of evidence, to prove the efficacy of a treatment algorithm, i.e., how to prescribe a well-matched AFO.
Keywords
Introduction
Orthotic treatment is a common intervention to support reduced or diminished functioning of the human musculoskeletal system. To promote walking ability Ankle Foot Orthoses (AFO) are frequently prescribed to various groups of patients who experience loss of control or impairments of muscle functions around the ankle. 1–4 This includes children with Cerebral Palsy (CP), patients with hemiplegia after a cerebrovascular accident (CVA) and patients with a range of diseases of the muscles and peripheral nervous system. 1–4
However, the apparent conviction by orthotic professionals that AFOs are effective is not supported by well established evidence. At this moment no conclusive evidence exists, neither to endorse nor to discard orthotic treatment around the ankle, in a context of promoting walking ability of the patient. Several recent studies present conflicting results, or even mixed results within one study. 1,3,5–9 Recent systematic reviews concluded that studies using high quality methods are still needed to support evidence-based decisions regarding the use of AFOs for CP. 10,11 A systematic review on the quality of AFO studies in children with CP concluded that substantial variability in the quality or reporting was present in currently published studies. 12 Another recent review concluded that only limited evidence exists for AFO management in hemiplegia.
The lack of evidence is also reflected by a scarcity of prescription guidelines. For instance, on how abnormal functioning of the musculoskeletal system should be supported or counteracted by an AFO to enhance walking ability in the aforementioned groups of patients. In the recent past, the International Society of Prosthetics and Orthotics (ISPO) has organized consensus meetings on the treatment of CP, CVA and poliomyelitis patients. However, these consensus reports are still inconclusive towards specific prescription guidelines for orthotic treatment of the ankle. 13 17 Moreover, it was summarized that the level of evidence is poor, with scarcity of randomized clinical trials. 14–16 Consequently, the grade of recommendation stated in those consensus reports concerning orthoses are mostly absent; occasionally C, being the lowest level of evidence; rarely B, the middle level of evidence; and never A, the highest level, being conclusive according to the Evidence Based Medicine methodology. 18
In clinical practice this lack of consensus is reflected by differences in treatment paradigms with respect to both the indication as well as to the mechanical construction of AFOs. 19 Therefore our community is compelled to design a long-term vision to establish unambiguous, realistic guidelines for orthotic treatment based on the highest level of evidence. In this article we will argue that a two-level approach for creating evidence should be followed in any AFO research project that evaluates AFO prescription to promote walking ability.
Evidence at Activity level
Following the framework of the International Classification of Functioning, Disability and Health (ICF), 20 outcome measures might be at the level of either function, activity or participation. Taking the patient's perspective, the most relevant outcome parameter is therefore at the level of the need of a patient. Within the focus of this paper we consider that the main reason for a patient to consult a physician, surgeon or orthotist to be his/her limitations of walking ability, as the main determinant of the problem. Thus a relevant context for the potential benefit of orthotic treatment around the ankle is presented, and therefore the relevant (primary) outcome parameter is at the level of activity, i.e., a parameter that quantifies walking ability. Walking performance, i.e., walking in daily life, comes most close to the problems experienced by the patient. 21–23 Unfortunately, up to now, not many studies on the efficacy of orthotic treatment included such measure. An alternative to objective measures is the use of perceived performance, e.g., the SF-36. 24
From the patient relevant point of view, it then seems second best to evaluate at the level of walking capacity, i.e., the actual performance in a laboratory environment. Laboratory measures focus on more specific indicators: Stability (safety); walking speed; and walking economy. Outcome measures of dynamic stability are currently under development. 25–27 Walking speed, either measured over 10 m of walking or as the 6 min walking test, is considered an important comprehensive functional outcome parameter. For stroke, it was proven that walking speed has a strong predictive validity towards community ambulation. 23 Measures of the economy of walking, include the physiological cost index (PCI, based on Heart Rate) and the Energy Cost (EC) of walking (based on breath-by-breath oxygen uptake measurements), the latter being superior. 28,29 EC of walking was shown to be a very reproducible and sensitive measure in postpolio and CP patients. 24,30,31
Use of the above-mentioned outcome parameters will provide the potential evidence that proves efficacy of orthotic interventions at the ICF activity level (See Figure 1a).
Mechanical evidence
Another approach to prove efficacy of orthotic interventions is to evaluate gait outcomes at the ICF level of body functions and structures. In this context, the use of 3D gait analysis has proven to be a powerful tool to explicitly quantify joint kinematics and kinetics during gait. It is used as an evaluation tool, as well as to support clinical decision-making in complex cases like multilevel surgery in CP. Recently, the use of 3D gait analysis has also been used to evaluate orthotic interventions. 3,6–10,24,30–34 Evaluating orthotic interventions at the level of kinematics and kinetics of the ankle, as well as more proximal joints, can be regarded as a technical quality check of the orthotic intervention itself, since the primary effect of an AFO is to influence ankle and foot function. Evaluating orthotic interventions at the level of kinematics and kinetics at more proximal joints provides an (intended) indirect effect of the AFO (e.g., stance phase control of the knee), but are still at the mechanical level. The reference values to evaluate the joint functions against are the kinematics and kinetics of normal walking. Normal walking is very stereotyped in terms of joint functions, and several comprehensive indices have been designed to express the amount of aberrancy. 35–37
Using outcome parameters from 3D gait analysis, either comprehensive indices or specific joint functions, that express a shift towards normality as the effect of wearing an orthosis, can thus be regarded relevant to prove efficacy of orthotic interventions at the ICF level of body functions (Figure 1b).
Redundant levels of evidence?
Figure 1 presents the two possible schemes of how orthotic interventions for ambulation can be evaluated. Both the Activity level as well as the mechanical approaches are used in clinical studies that aim to create evidence for the orthotic interventions. Proponents of the Activity level evidence method would argue that the aim of orthotic prescription is to promote walking ability of the patient, so any outcome needs to be at that level. Proposers of the mechanical evidence, on the other hand, would argue that the working mechanism of an orthotic intervention is to support the joint according to its mechanical design. So it should be adequate to investigate whether or not the mechanical support or constraint provided by the orthosis would result in normalization of joint function during gait. When these functions are indeed normalized, or significantly shifted towards normal values, the orthotic intervention can be concluded to be effective.

Schematic designs of an experimental study of orthotic intervention. (a) Using outcome parameters at walking ability level creating evidence at activity level (A) versus (b) Outcome parameters at joint function level creating mechanical evidence (M).
Both sides have strong arguments, and it probably depends on someone's disciplinary background which approach would be considered the most appealing. Nevertheless, both approaches do have a major assumption in common, namely that the other level can be uniquely concluded from the evaluated one. This means that normalization of walking kinematics and improved walking ability are closely coupled, also in the context of orthotic interventions. If this assumption is true, both approaches are valid to provide evidence for orthotic interventions, specifically AFOs. In order to examine this assumption, we could start by looking at studies that have included both ICF levels to study the efficacy of AFOs. This will demonstrate whether indeed a redundant level of evidence is presented or that the assumption is violated, meaning that the levels of evidence are not redundant.
The study of Bregman et al. 38 investigated the effectiveness of low stiffness AFOs to promote walking capacity in stroke patients, while measuring 3D joint kinematics and kinetics as well as the energy cost of walking. It was concluded that when the AFO effectively corrected a decreased dorsiflexion of the ankle at terminal swing, the EC was effectively reduced as well, where otherwise it did not. So in this case, targeted improvement at function level coincided clearly with the outcome parameter at Activity level. Such correspondence of outcomes across different levels was also found by Balaban et al., 30 who investigated the effect of hinged AFOs in children with hemiplegic Cerebral palsy. They found a decrease in Energy Cost and a simultaneous improvement of ankle kinematics. This is in line with a study in hemiplegic CP children by Buckon et al., who found that an improvement in EC coincided with normalization of ankle kinematics and kinetics. 34 For the diplegic children, they found that the non-hinged orthoses worked best. 7 Brehm et al. investigated how the changes in the kinematics of gait were related to changes in EC, as a result of wearing an AFO in children with CP. 3 They found that kinematics of gait improvements in efficiency were reflected by changes of stance and swing phase knee kinematics. 3
In another study, Brehm et al. showed how the biomechanics of gait in postpolio patients can be used to target the orthotic design of an knee-ankle-foot-orthosis based on normalization of selected gait variables. 39 A decrease of EC was associated with the successful normalization of specific biomechanical parameters of gait, that were a priori identified as a target for orthotic intervention. However, it is interesting to note that not all parameters that were associated with a decrease of EC of walking did change significantly and that not all significant changes of biomechanical parameters were positively associated with a decrease of the EC. 39
Overall, these studies showed a positive relationship between the orthotic intervention that aimed at a specific mechanical effect of joint function(s), and the observed positive effect at Activity level. This suggests that both levels of evidence are redundant.
A nested model
If the two levels of evidence would be redundant, it would be sufficient to evaluate treatment of AFOs to promote walking ability at just one level. However, results that are found on the global level might hide specific information. Further analysis might show us which critical mechanical factors determine Activity level evidence.
In a retrospective study of Brehm et al. 3 in which 80 children with CP were identified from a clinical database with ICF assessments at both levels, walking ability was assessed using normalized walking speed and Net Non-dimensional (NN) EC, 40 and joint function was assessed using 3D movement analyses of walking. The overall effect on normalized walking speed (+9%) and NN EC (-6%) demonstrated Activity level evidence for the whole group. Furthermore, several subgroups could be recognized: A large group showed improvement at both outcome parameters; another group showed worsening at just one parameter and improvement on the other; while the last showed worsening on both parameters. Apparently, the AFO works very well (i.e., minimizes EC and increases walking speed) for some subjects, but fails to be effective, or was even counter-effective in others, using this Activity level output parameter. Meanwhile the effects on this parameter were not reflected in the Gillette Gait Index (GGI), 35 a parameter of gait normality based on overall gait kinematics. Specific analyses revealed that a reduction of knee angle in stance was moderately associated with more efficient gait. So it was not possible to find a conclusive patient/orthosis match. The authors consider that inadequate prescription of AFOs (which is inevitable in retrospective research) contaminates a stronger relation between knee angle and EC. Therefore future research is suggested that uses specific hypotheses related to the goals and design of the AFO prescription. Similar observations were stated by Buckon et al, 7,34 who did not carry out any subgroup analysis, but recognized that AFO configuration differences have a significant effect on the economy of walking in some children with CP.
Another retrospective study was performed by Rogozinski et al. 32 looking at a floor-reaction AFO in children with CP who were walking in crouch gait. A measure of the cost of walking was not available, but walking speed was improved. A focus was put on the reduction of the knee angle in stance, which is a mechanical outcome parameter, but also a known main determinant of energy cost of walking. 41 An analysis of multiple regression, to appreciate what factors are related to this outcome parameter, revealed that knee and hip flexion contractures greater than 15° were found to limit the efficacy of the orthosis in controlling knee extension in midstance. The study concluded to consider these values as contraindications for the prescription of a floor-reaction AFO in children with CP who walk in crouch.
In the above-mentioned studies, the aim was to prove the efficacy of orthotic interventions and also to investigate the relationship between Activity level evidence and mechanical evidence. These two do not appear redundant in general, but for specific applications a relationship could be established. In such cases, both quantitative physical examination as well as biomechanical evaluation of gait, are important tools do decide which changes at the level of joint function should be targeted by the orthotic intervention. For children with CP, Davids et al. argued that, analogous with multilevel surgery decision-making, optimal orthotic management requires the physician to clearly identify the gait deviation and functional deficits to be addressed with the orthosis. 42 Integrating the approach of Activity level evidence and mechanical evidence will result in a nested decision scheme (see Figure 2), and consequently a nested evaluation scheme. The function level or mechanical evaluation has now taken the role of explaining the result at Activity level, i.e., it creates Explaining Evidence on the patient/orthosis match. The parameters that are considered necessary to feed the treatment algorithm, i.e., the results from physical examination and biomechanical gait analysis, are the same elements that are internally evaluated, to check for the correctness of the patient/orthosis match.
Characterize AFO mechanics
Any treatment algorithm will include a specific type of AFO. 42–44 So besides the nested decision model on the two levels of treatment outcome and also the intervention itself, the AFO should be unambiguously and objectively characterized. Subtyping of AFOs is common in clinical practice, but unfortunately it is usually in global terminology referring to design, material or apparent stiffness. Since the AFO is a mechanical device, its function about the ankle will be unambiguously characterized by quantifying its behaviour in mechanical terms around the talocrural joint. Using this approach it was shown that the ankle part of the AFO could be characterized by an elastic spring: i.e., its stiffness and a neutral angle. 45,46 It will depend on the treatment algorithm how the AFO requirements based on those two parameters are specified. For example, AFO stiffness must be just enough to counteract the passive stiffness of the triceps surae to keep the foot in dorsiflexion during swing. 47
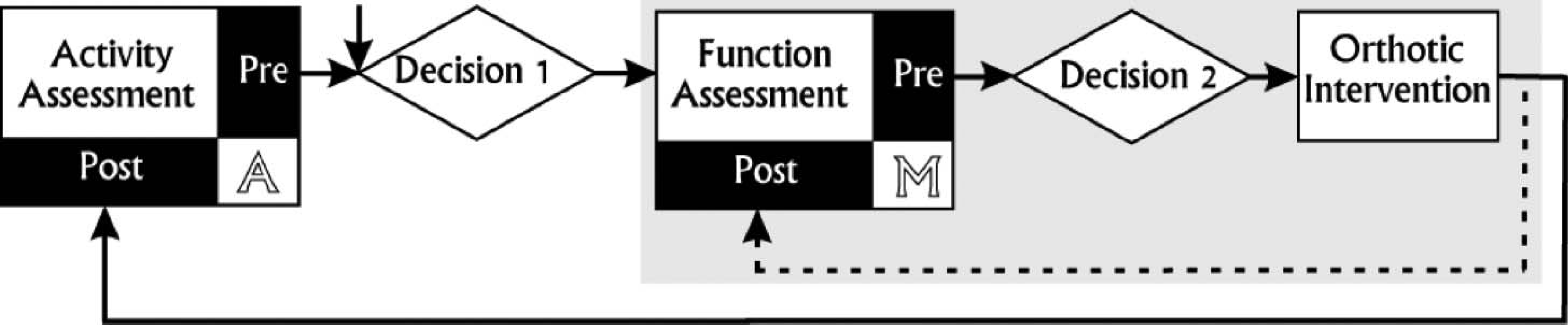
A nested decision scheme is ideally used in clinical practice. Decision 1 results in a tentative orthotic intervention with goal setting at ICF Activity level. Decision 2 is based on gait analysis and physical examination and concludes which specific technical requirements the orthosis should fulfil to effectively influence the ICF function level. These two decisions comprise the treatment algorithm. Evaluation is at two levels again, A: Activity level, that should match treatment goal setting, and M: Mechanical evidence that is necessary additional information to evaluate the correctness of the treatment algorithm (dashed line).
The foot part of the AFO serves usually to create a solid lever arm for the AFO to be effective. Stabilizing the foot as a rigid segment is also achieved by the shoes, which demonstrates that footwear is a part of the orthotic intervention. Besides stiffening the foot, the shoes will also determine how the neutral angle of the AFO will affect the inclination of the tibia. 33,48 Because the AFO fixes the ankle angle, the alignment of the neutral angle of the AFO directly influences knee and hip net joint moments, and should therefore be carefully aligned. The tuning of the AFO footwear combination is achieved by manipulating the heel height of the footwear to arrive at the optimal tibia inclination, guided by measuring net joint hip and knee moments. 49,50
It must be concluded that an unambiguous mechanical AFO characterization, either in a research project or as a prescription clinical practice, must mention its stiffness and the neutral angle in combination with the footwear. More extensive guidelines for AFO description in reporting AFO intervention studies in CP were recently published. 12
Evidence into practice
In the preceding section, some prospective studies on AFO efficacy were discussed that used outcome measures at ICF levels of body functions and structures (mechanical) as well as Activity level, to learn about its relation. The body of knowledge on the efficacy of AFOs will gradually grow using well designed studies, i.e. (a) homogeneous patient groups are measured; (b) relevant outcome measures are used; and (c) the AFOs in the study are unambiguously mechanically characterized. Future studies would also profit from including Activity measures at the level of activity performance, i.e., ambulatory recording of actual ambulation 21–23 and compliance of AFO use. Meanwhile, the bundle of evidence can be used to construct treatment algorithms, to be applied in clinical practice. When current evidence is lacking, expert opinions must be used to construct provisional treatment algorithms. Such a decision scheme, roughly outlined in Figure 2, will need the use of measurement instruments, to provide information to make decisions. 51 This use of measurements in clinical practice requires a much higher precision than most instruments that are used in research studies. Measurements of EC of walking and biomechanical gait analysis have been shown to have a precision that meets clinical relevant values. 52,53 This means that the error for an individual measurement will not obscure a relevant change or deviation from a reference value. Although this requirement seems self-evident, most instruments that are used in research studies are not directly applicable in clinical practice. A first step should be that the community establishes a core set of measurement instruments at the two levels of evidence (e.g., 54 ). These measurements instruments must be considered relevant, but must also possess proven methodological quality. This will contribute to the harmonization and generalization of clinical trials aiming to evaluate the efficacy of AFOs in the future that acknowledges subtyping of AFOs in the treatment algorithm.
Conclusion
Efficacy studies of AFOs to promote walking ability should comprise two levels: Efficacy on Activity level will determine the meaningfulness of the orthotic intervention for the patient; efficacy on the body function and structure (mechanical) level is necessary to establish a treatment algorithm that includes a specific orthotic intervention. This intervention is characterized by the mechanics of the AFO footwear combination. Future efficacy studies should include all these elements to construct a clinically relevant body of knowledge.