
Abstract
Background and Aim:
Much previous research on orthotic walkers has focussed on their ability to offload structures in the foot and ankle; however, little is known about their effects on lower limb mechanics. This study aimed to determine effects of two orthotic walkers on the biomechanics of the knee and hip joints compared to standardised footwear.
Technique:
A total of 10 healthy participants walked under three conditions: Walker A (Össur, Iceland), Walker B (DJO Global, USA) and standardised footwear (Hotter, UK). Kinematic and kinetic data were collected using a Qualisys motion analysis system (Qualisys Medical AB, Sweden) and force plates (AMTI, Boston, MA, USA). Significant differences were seen in hip kinematics and knee moments between walkers and standardised footwear and in knee kinematics between Walker A and standardised footwear.
Discussion:
Both walkers show significant kinematic and kinetic differences compared with standardised footwear; however, Walker A appeared to produce greater deviation, including potentially damaging greater hyperextension moments at the knee.
Clinical relevance
Further research is needed into the effects of orthotic walkers on knee and hip joint mechanics, which should help to inform future designs of walker, with greater focus on obtaining a more normal gait pattern.
Background and aim
Orthotic walkers are frequently used in clinical practice in the management of various pathologies, though the predominant use of these orthoses is in the management of diabetes-related foot health. 1 Orthotic walkers and total contact casts (TCCs) work by redistributing the plantar pressure more evenly over the midfoot, and TCC techniques are increasingly being replaced by the removable orthotic walker. 2 Orthotic walkers allow early weight bearing while providing protection; they are adjustable and removable for examination, facilitating exercise and early intervention in the event of a problem and reducing the need for orthopaedic technicians. 2 Reduced hospital stay, less rehabilitation sessions and early intervention together with ease of application and adjustment mean orthotic walkers are becoming the cost-effective solution 3 to conservative management of a range of acute and chronic conditions.
Walkers have been shown to be more effective than traditional fibreglass casts in reducing lower leg muscle activity 4 as well as promoting a faster return to baseline activity. 3 Early mobilisation with the use of orthotic walkers affords a better clinical outcome in terms of ankle function, bone strength and faster bone healing,2,5 with individuals showing improved quality of life through a shorter hospital stay and faster return to activities of daily living and sport.2,5,6 In contrast, the use of the TCC to immobilise the lower limb is decreasing, due to the requirements of an experienced technician and its associated joint-, muscle- and skin-related undesirable outcomes. 7 Several studies have explored use of orthotic walkers and their effect on plantar pressure distributions; 8 however, limited attention has been given to the study of kinematics and kinetics when wearing such orthoses.2,9 While these studies imply that orthotic walkers elicit less adverse effects 2 than TCCs, the true impact of these walkers during longer term use requires further investigation. 10 The aim of this study is to explore the short-term effect of two designs of orthotic walkers on hip and knee kinematics.
Technique
Participants
A total of 10 healthy participants (6 males, 4 females; 37.1 ± 12.1 years) were recruited from university staff and student populations. All participants reported to be free from any pain or pathology of the lower limbs or spine at the point of testing. All data collection conformed to the Declaration of Helsinki, and volunteers gave written informed consent prior to participation. The study was approved by the Built, Sport and Health Ethics Committee (University of Central Lancashire, UK).
Procedure
Passive retro-reflective markers were placed on the lower limbs and pelvis using the calibrated anatomical system technique (CAST) to allow for segmental kinematics to be tracked in 6 degrees of freedom. Markers were positioned on the anterior superior iliac spine, posterior superior iliac spine, greater trochanter, medial and lateral femoral epicondyle, medial and lateral malleoli, the head of the 1st metatarsal, the head of the 5th metatarsal, the dorsum of the foot and the calcaneus or equivalent placement over these landmarks on the walker. Additionally, clusters of four non-collinear markers were attached to the body segments of the shank and thigh and on the anterior plate of the walker. Kinetic data were collected at 200 Hz using four AMTI force plates (Boston, MA, USA). Kinematic data were collected using a 10-camera infrared Oqus motion analysis system (Qualisys Medical AB, Sweden) at 100 Hz. All participants were asked to walk along a 10 m walkway under three conditions: (a) standardised footwear (with no orthosis) (Hotter, UK); (b) Walker A (Rebound™ Air Walker; Össur, Iceland) and (c) Walker B (Aircast® FP Walker; DJO Global, USA) (Figure 1). Five repetitions for each condition were performed in a randomised order. All walkers were applied in accordance with the manufacturer’s instructions on the left foot.
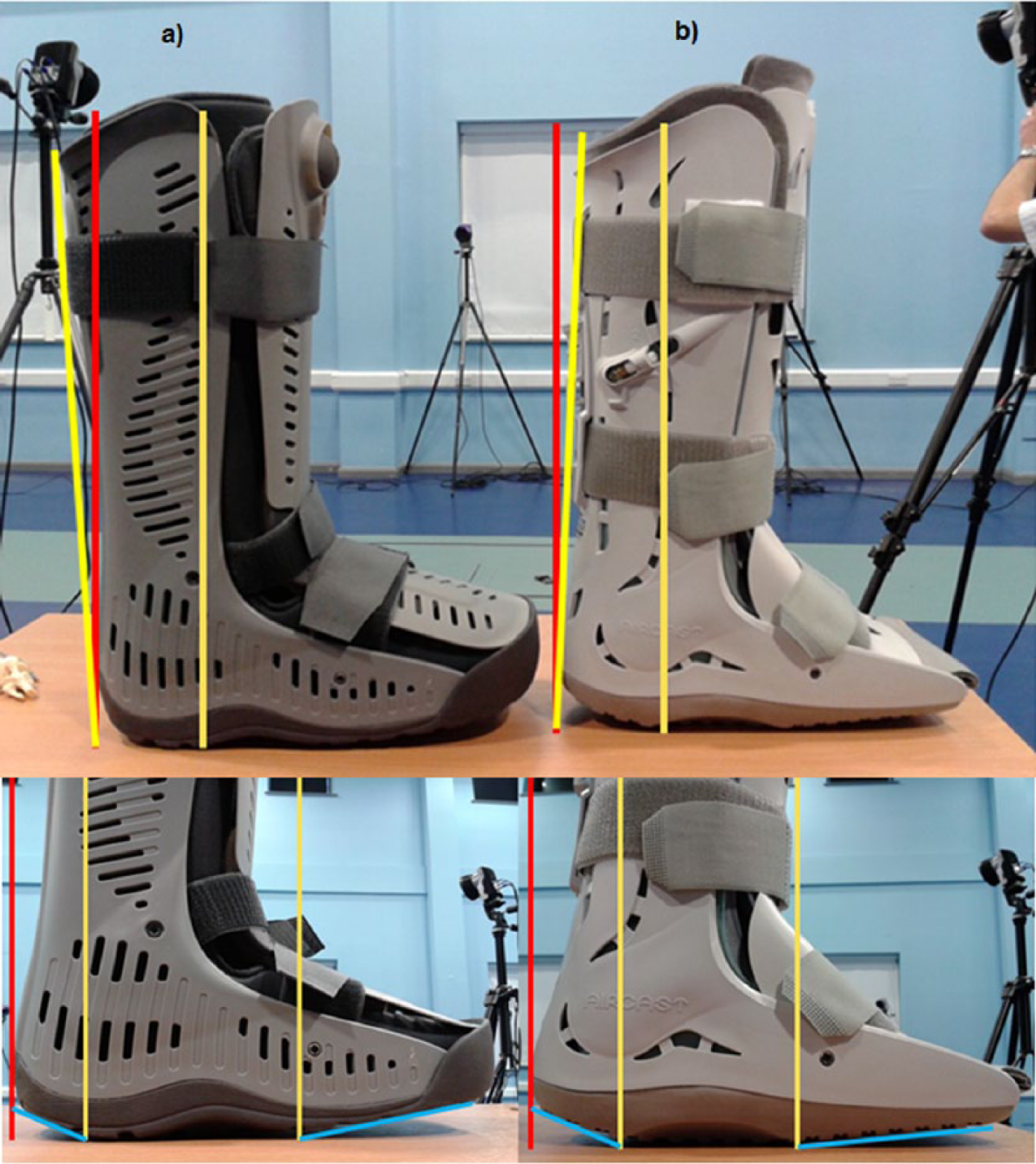
Showing the tibial inclination and rocker profile of (left) Walker A (tibial inclination angle: 4.3°, heel rocker profile: 25°, forefoot rocker pofile: 12°) (Rebound™ Air Walker; Össur, IS) and (right) Walker B (tibial inclination angle: 2°, heel rocker profile: 22°, forefoot rocker profile: 6°) (Aircast® FP Walker; DJO Global).
Anatomical frames were defined by landmarks positioned at the medial and lateral borders of the joint; from these right-handed segment, co-ordinate systems were defined. The kinematics were calculated based on the Cardan sequence of XYZ. Raw kinematic and kinetic data were exported to Visual3D (C-Motion Inc., USA). Kinematic and kinetic data were filtered using fourth-order Butterworth filters with cut-off frequencies of 6 and 25 Hz, respectively. Knee and hip angles and moments and centre of pressure were exported and repeated measures analyses of variance (ANOVAs) were performed on maximum, minimum and range values using SPSS v20 (IBM, NY, USA).
Results
The two walkers showed a slight increase in the amount of knee flexion during stance phase. Significant differences were also seen between walking with standardised footwear and Walker A and between the two walkers with Walker A showing a greater transverse plane range of motion during stance phase (Table 1). A trend towards a significant difference was seen between walking in standardised footwear and Walker A, for peak hip extension during stance phase (Table 1). Although the average walking speed for both Walkers was notably smaller than when walking with standardised footwear, the differences were not significant (p = 0.099).
Knee and hip joint angles for SF, WA and WB.
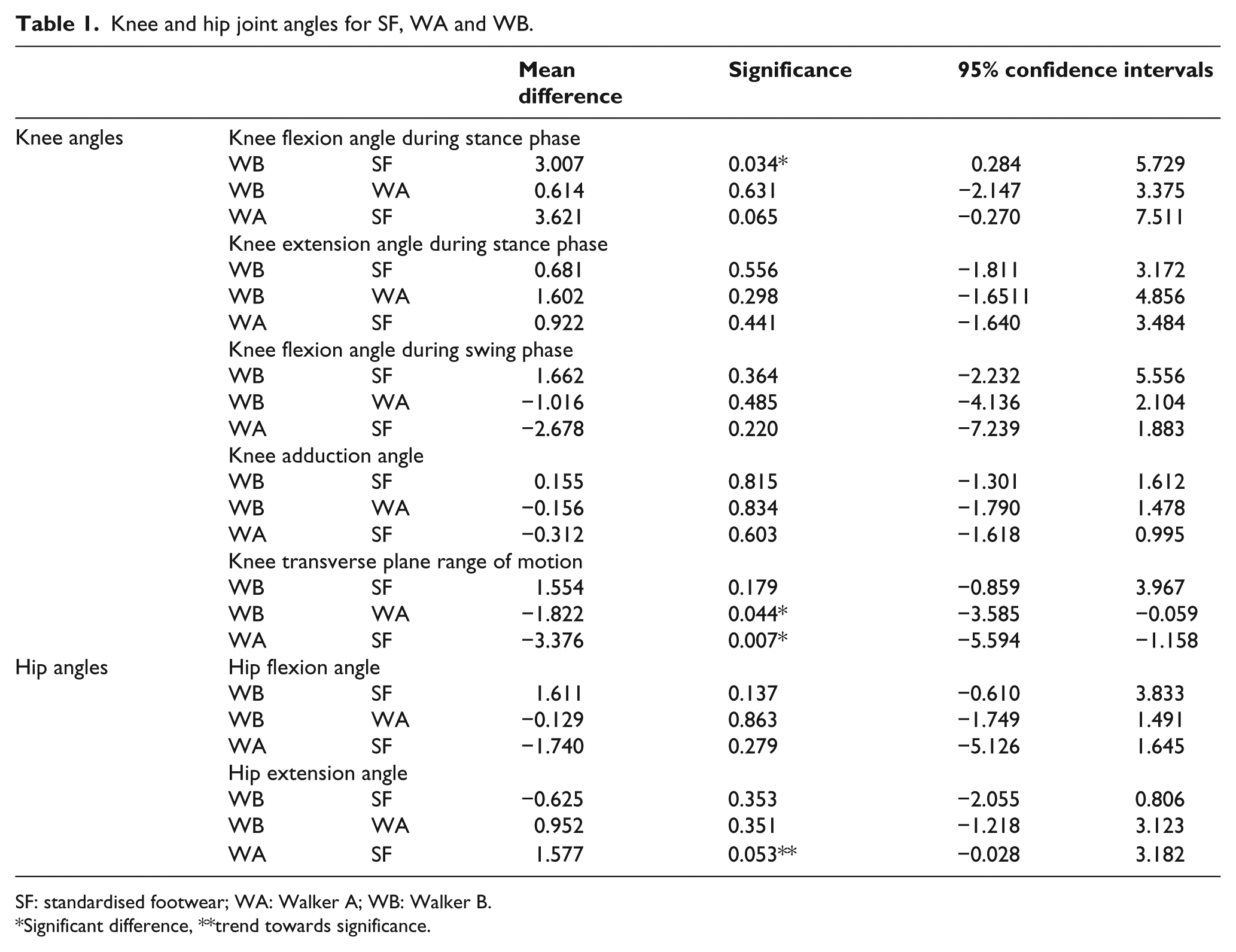
SF: standardised footwear; WA: Walker A; WB: Walker B.
Significant difference, **trend towards significance.
Significant differences in peak knee extension moments were seen between all conditions with Walker A showing the highest knee extension moment followed by Walker B, and in the peak knee flexion moments between the two walkers. Significant reductions in peak knee adduction moments were seen when walking with both walkers compared with standardised footwear (Table 2). Hip extension moments also showed significant differences between Walker A and both Walker B and standardised footwear (Table 2).
Knee and hip joint moments for SF, WA and WB.
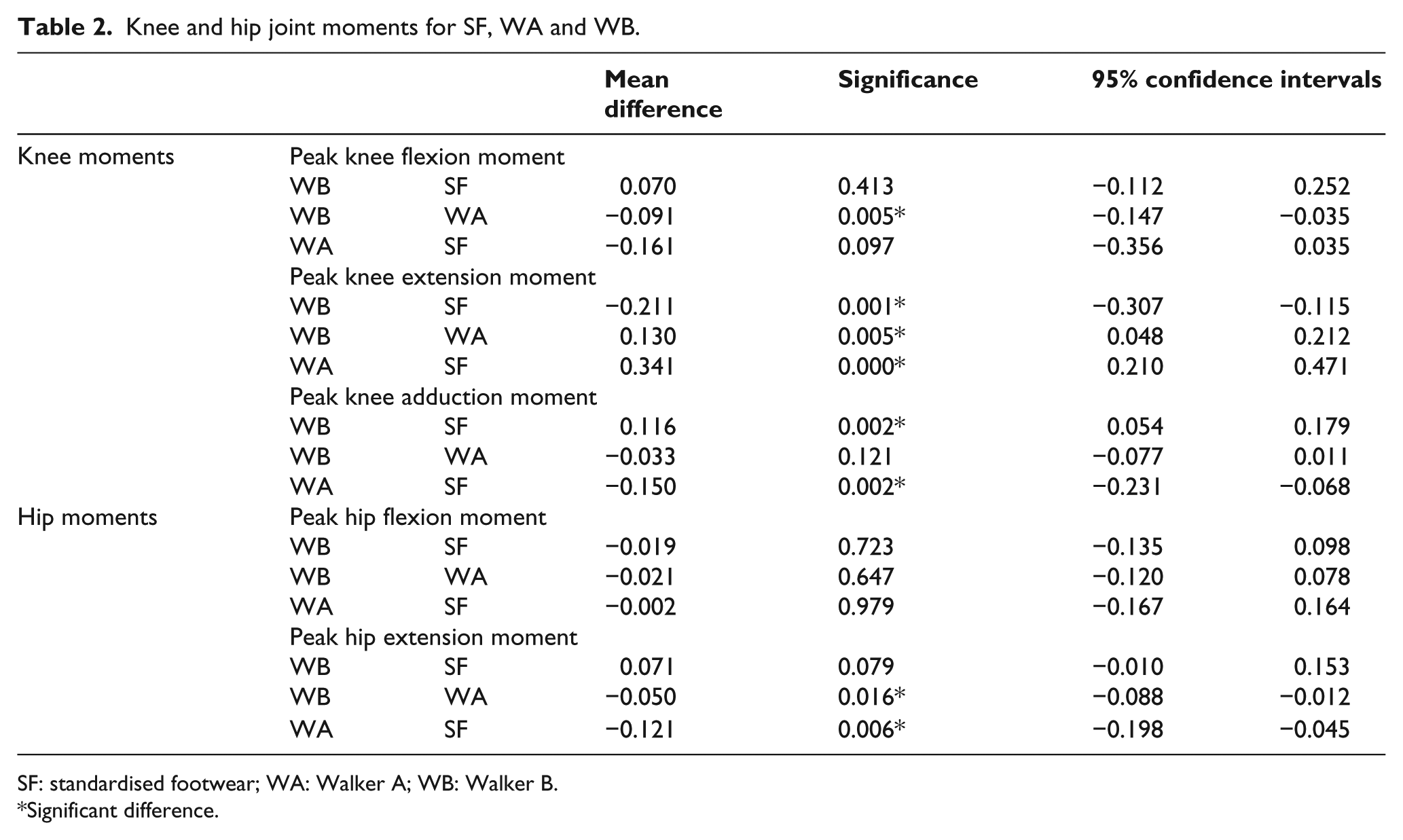
SF: standardised footwear; WA: Walker A; WB: Walker B.
Significant difference.
No significant differences were seen between walking with standardised footwear and the two walkers for centre of pressure velocity during stance phase (Table 3).
Centre of pressure velocity.
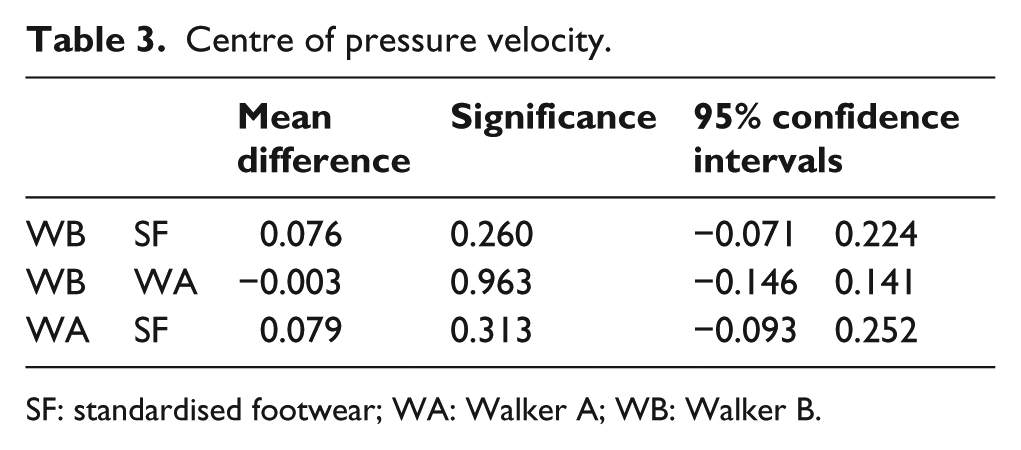
SF: standardised footwear; WA: Walker A; WB: Walker B.
Discussion
A slight increase in the amount of knee flexion was seen during stance phase when wearing both the walk-ers; however, there was a significantly greater flexion moment when walking with the Walker A compared with Walker B. The increased knee flexion moment during loading response may be attributed to the difference in the rocker profile under the heel during the loading response phase (Figure 1).
A trend towards a significant difference was seen between walking with standardised footwear and Walker A for peak hip extension angle, and significant differences in peak knee and hip extension moments were also seen between all conditions with the Walker A showing the highest knee extension moment and the lowest hip extension moment. Despite there being no significant difference in walking speed, an increased knee flexion moment during loading response suggests that either the angle of tibial inclination or the movement of the centre of pressure under the rocker sole could be responsible. This increase in the moments being exerted at the knee could have damaging complications to the internal structures of the knee.
Significant differences were also seen between walking with standardised footwear and the two walkers for peak knee adduction during stance phase; however, no differences were seen between the two walkers. Differences were also seen between walking with standardised footwear and Walker A and between the two walkers in the transverse plane range of motion with Walker A showing a greatest amount of rotation. As these orthotic walkers can be prescribed over an extended period of time, for instance, over a period of 4 weeks in conservative treatment of Achilles tendon rupture,11,12 further investigation is warranted on the long-term effects of these results.
No significant differences were seen between any of the conditions for centre of pressure velocity during stance phase indicating that both walkers were able to produce a smooth forward progression of the ground reaction forces. The differences seen may be related to the rocker sole profile and/or the tibial inclination angle of the walkers as this is the only major technical difference between the walkers (Figure 1).
Key points
Both walkers showed significant differences compared with standardised footwear, in a sample of 10 healthy individuals; however, Walker A appears to produce the greatest deviation. This is particularly noteworthy in knee flexion, knee extension moments and hip extension moments which could be damaging over long-term usage.
The differences between walkers may be attributed to the subtle differences in rocker profile and tibial angles.
It is clear from this study that further research is required with a greater number of individuals, in order to explore the effects of orthotic walkers on the knee and hip joint mechanics. This should in turn help to inform future designs of walker, with a greater focus on obtaining a more normal gait pattern.
Footnotes
Acknowledgements
The authors would like to thank DJO Global for supplying the walkers.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.