
Abstract
Background:
Internal hip abduction moment is a major indicator for hip loading. A new hip bracing concept was designed to unload the cartilaginous area in hip osteoarthritis via an abduction and external rotation force intended to alter the weight bearing area and reduce compression through the joint.
Objective:
To assess the effect of a novel brace on hip rotation in the transverse and coronal planes and on the hip abduction moment.
Study design:
Repeated measures.
Methods:
Gait analysis was performed on 14 subjects with unilateral symptomatic hip osteoarthritis. Pain, joint motion, moments and vertical ground reaction force were compared between the braced and the unbraced (control), randomly assigned, conditions.
Results:
Nine participants felt an immediate reduction in pain while walking with the hip brace. Peak hip abduction moment significantly decreased on the osteoarthritis side (p = 0.017). Peak hip adduction (p = 0.004) and internal rotation (p = 0.0007) angles significantly decreased at stance with the brace.
Conclusion:
Wearing the brace would appear to reduce the compressive joint reaction force at the femuroacetabular interface as indicated by a reduction in internal hip abduction moment along with immediate pain reduction in nine participants. Further long-term studies are warranted.
Clinical relevance
The brace rotates the hip in the transverse and coronal planes, possibly resulting in a decrease in load through the diseased area of cartilage. In some patients, an immediate decrease in pain was experienced. The brace offers an alternative solution for hip osteoarthritis patients not ready for a hip replacement.
Background
Osteoarthritis (OA) is a major degenerative joint disease affecting most commonly the hands, knees and hips. 1 The prevalence of hip OA in developed countries is high among the ageing population, but it has also been more recently documented in younger, more active population aged below 65 years.2–4 Hip OA is characterized by articular cartilage degeneration, symptoms include pain and stiffness and results in abnormal gait patterns.5–9 Whether OA is the cause or result of altered function remains unclear, but the role of biomechanics in hip OA progression has been established. 10
The internal hip abduction moment is the main biomechanical indicator for hip loading during the single limb support phase of gait in the frontal plane. 11 Indeed, because of the short lever arm to the joint centre, the force developed by the hip abductors is a major contributor to the compressive joint reaction force at the femuroacetabular interface. 12 The abductors have the additional responsibility of controlling frontal plane stability of the pelvis during walking and thereby influence the function of the other lower extremity joints.
Currently, non-surgical options for the management of hip OA are limited and mainly rely on medication or activity modification and lifestyle changes (i.e. loss of weight, healthy nutrition and exercises in water). According to the Osteoarthritis Research Society International (OARSI), hip arthroplasties should be considered as a last resort to limit the risk of outliving the hip prosthesis. 13 Instead, improved access to walking aids or other assistive technologies during motion should be possible, and further research on effectiveness of non-surgical and non-pharmacological solutions for the management of hip OA is encouraged. 14
Hip bracing aims to impose mechanical modifications during gait in order to alleviate pain and improve function by unloading the worn cartilaginous area of the hip joint.
Currently, only one pre-operative experimental hip brace called the WISH-type S-form (Wakayama Medical College) has been shown to reduce pain and improve functional mobility,15–17 although the mechanical reasons behind the improvement remain uncertain.
The purpose of this study was to investigate the effect of the brace on lower limb biomechanics during gait of patients with hip OA. More specifically, we hypothesized that the use of the brace would lead to a reduction in the internal abduction moment and an increase in hip external rotation and abduction.
Methods
Participants
A total of 14 participants took part in this study. Among them, 10 were recruited via advertisement placed in the major newspapers asking for volunteers who exhibited frequent hip pain in their daily life. Four others were contacted from the waiting list for hip surgery from the local hospital. Inclusion criteria were symptoms of OA including loss of joint space and osteophytes shown on recent x-rays and ability to perform 15-min walk at a self-selected pace without a walking aid. Unilateral and bilateral radiographic hip OAs were accepted as long as pain was reported in only one leg by volunteers. Exclusion criteria were bilateral painful hips, hip (knee or ankle) replacement or any history of serious injury at the lower limb (that may have resulted in persistent compensatory movement patterns). In case of bilateral radiographic hip OA, the painful hip was referred as the OA hip, and the non-painful hip was considered as the unaffected hip. The National Bioethics Committee of Iceland gave approval for this study, and all participants signed an informed consent.
Hip brace
The hip brace utilized in this study was Hip Unloader (Össur, Reykjavik, Iceland). It consists of a tight-fitting garment equipped with a thin, elastic strap wrapped above the knee in a medial to lateral and distal to proximal direction and anchored at the sacrum (Figure 1). The strap is applied in a toe-out position in order to move the femur into abduction and external rotation and resist adduction. A pelvis belt is set on the rear half of the pelvis to provide more support around this area and exert pressure on the hip extensors. Additionally, a pad is applied to provide pressure on the greater trochanter.

Hip Unloader (Össur, Reykjavik, Iceland).
Gait analysis
All subjects randomly performed the test twice with the brace on first (braced condition) or with adjusted cycling shorts first (control) in a repeated measures design. Three-dimensional (3D) joint kinematics and moments were calculated from data collected with a set of reflective markers placed over the pelvis, thighs, shanks and feet on specific bony landmarks. Four sets of four tracking markers attached to a rigid shell were added on the thighs and shanks to compute the 3D motion of these segments. 18 The markers’ 3D spatial position was recorded using eight high-speed infrared cameras (Qualisys, Göteborg, Sweden) with a sample frequency of 120 Hz, synchronized with two force platforms (AMTI, Watertown, MA, USA). All kinematic and kinetic factors were calculated using the movement analysis programme Visual 3D (C-Motion, Inc., Germantown, MD, USA).
A static calibration trial was first performed while standing upright to record the neutral location of all markers. A biomechanical body model defining local coordinate systems and joint centres given the geometrical relationships between all markers was built in Visual 3D. To minimize marker position error, electrocardiography (EKG) electrodes were applied on bony landmarks on the pelvis and thighs that would be covered with the brace and cycling shorts (unbraced condition). A small metal stud on the electrodes could be palpated through the garments ensuring the repeatable location of reflective markers between conditions. For landmarks that would not be covered by the brace (femoral epicondyles, malleoli, etc.), a mark was directly applied on the skin using a pen, indicating the location of reflective markers.
Subjects walked at a self-selected speed in a straight line over two force platforms. Kinematic and kinetic peaks were identified during the stance phase of the affected limb and derived from five successful trials for each subject and each condition. Average peak differences between the braced and the unbraced (control) condition were calculated for all. Hip adduction angles and abduction moments were identified during the single support period of the test limb before midstance. All ground reaction forces and body moments were normalized to each participant’s body weight (respectively N/kg and Nm/kg) and moments were expressed as internal moments.
Pain evaluation
Pain levels during each condition were assessed using a visual analogue scale (VAS). Participants were asked to circle the figure from 0 to 10 which best reflected the magnitude of pain after testing with and without the brace.
Statistical analysis
A within-subjects design was chosen to assess the immediate effects of the brace on each participant’s performance compared to the control testing with cycling shorts.
Results were checked for normality with the Shapiro–Wilk test with 5% risk. A two-tailed paired t test in MATLAB 8.2 (MathWorks, Inc., Natick, MA, USA) was used to compare parameters between the braced and the unbraced conditions with a familywise error rate of 0.05. Comparison was made based on the mean differences of these parameters between the braced and the unbraced (control) condition. A negative difference from unbraced to braced condition (with minus without brace) indicates a reduction in the factor of interest. A post hoc false discovery rate was applied to adjust the significance level (αFW) to account for multiple comparisons. Confidence intervals were calculated after adjustment for significance according to Student’s t distribution.
Pain evaluation during walking was used to classify people into two groups: the more pain (MP) group whose pain level increased with the brace and the less pain (LP) group whose pain was reduced (or remained unchanged). Changes in kinematics and kinetics were compared between both groups to better understand mechanical causes for brace effectiveness on pain alleviation. Significance testing was not applied to the MP group due to the small sample size.
Results
A total of eight women and six men took part in this study. Mean age (± standard deviation (SD)) was 59 ± 12 years, and mean body mass index (BMI) was 26.28 kg/m2. Four participants had bilateral OA with pain in only one leg. After the walking test with brace, nine people reported a reduction in pain and five people reported an increase in pain (Table 1).
Pain evaluation during ambulation (from unbraced to braced condition).

CI: confidence interval; LP: group who reported ‘Less Pain’ with the brace on; MP: group who reported ‘More Pain’ or unchanged pain level with the brace on.
The spatial and temporal parameters were similar with and without brace (Table 2). In particular, the difference in walking speed between conditions was negligible. However, 10 subjects had shorter steps on the unaffected limb side resulting in an average reduced non-affected step length for the entire group (n = 14).
Spatial and temporal parameters (difference from unbraced to braced condition).
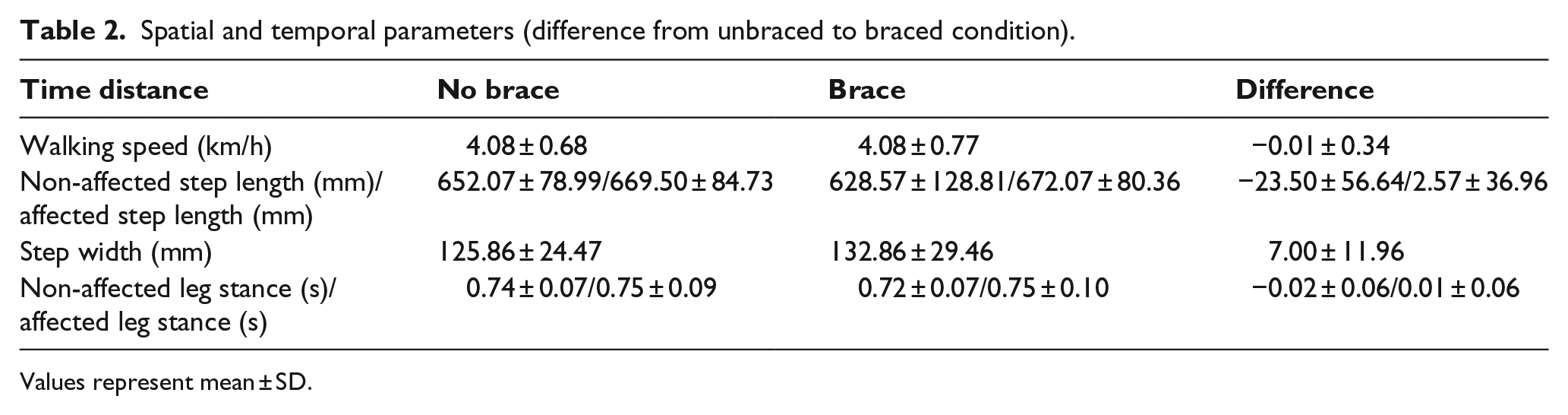
Values represent mean ± SD.
The brace significantly reduced the peak adduction and internal rotation angles of the affected hip during the stance phase (p < 0.01). There was no significant increase in hip extension with the brace (Table 3).
Kinematic and kinetic changes in all participants (n = 14) from unbraced (control) to braced condition.
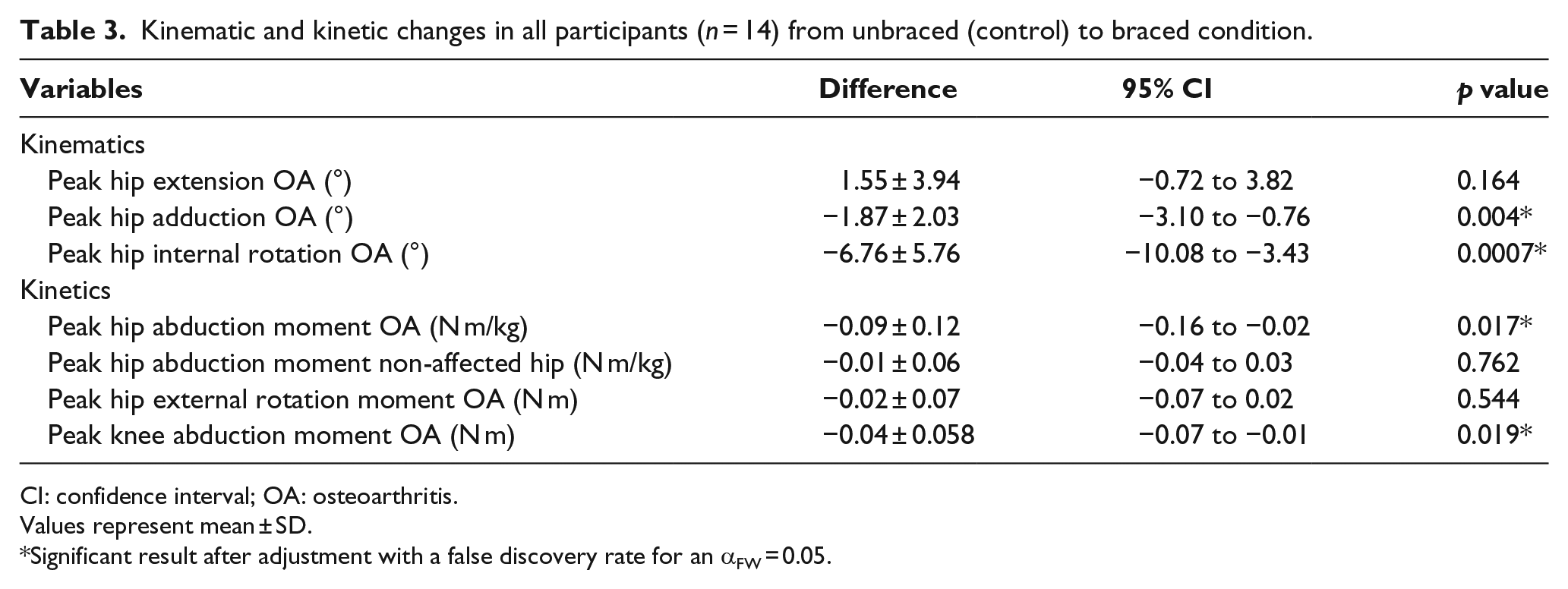
CI: confidence interval; OA: osteoarthritis.
Values represent mean ± SD.
Significant result after adjustment with a false discovery rate for an αFW = 0.05.
The peak hip abduction moment on the affected OA side was reduced by 9.34% (p < 0.01) with the brace compared to the unbraced condition. The peak hip abduction moment remained unchanged in the unaffected hip (Table 3). In the MP group, the reduction in hip abduction moment was double that of the LP group (Table 4).
Kinetic changes in MP (n = 5) versus LP (n = 9) groups from unbraced (control) to braced condition.
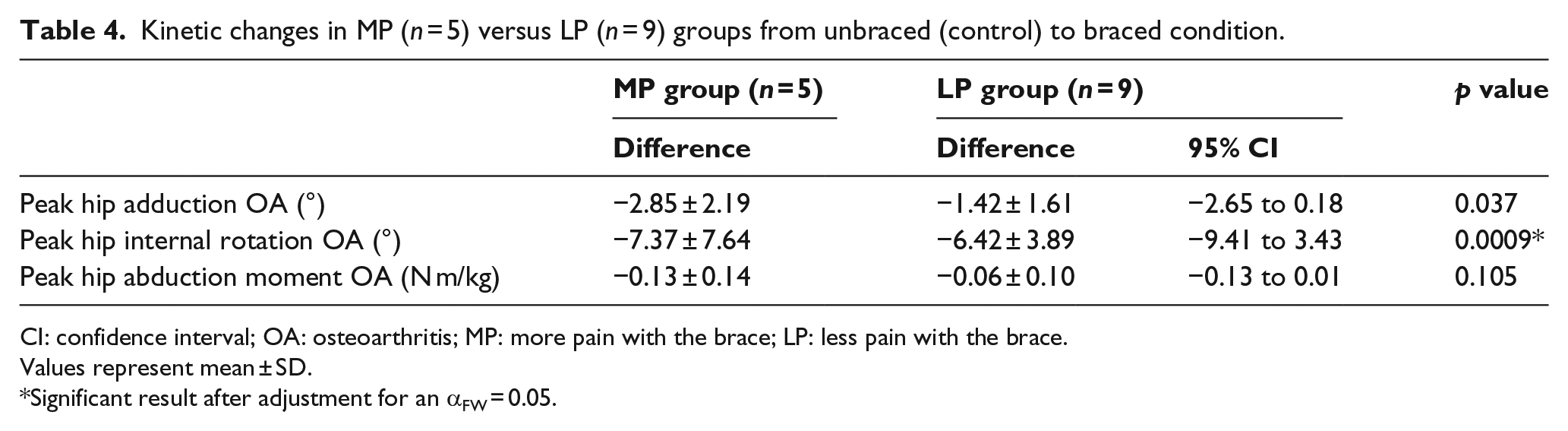
CI: confidence interval; OA: osteoarthritis; MP: more pain with the brace; LP: less pain with the brace.
Values represent mean ± SD.
Significant result after adjustment for an αFW = 0.05.
Figure 2 compares the normalized values of the first peak of the vertical ground reaction force (zGRF) on the non-affected and OA sides in the MP and LP groups. The common strategy adopted in the MP group when walking with the brace was to reduce the loading response on the OA side. Indeed all but one of the MP participants showed a reduced zGRF on the OA side (i.e. subjects 1, 3, 4 and 5). For subject 2, the zGRF increased on the non-affected side instead. In the LP group, five subjects (6, 7, 9, 12 and 14) showed increased zGRF on both limbs at each step with the brace. Yet, the strategy employed by the LP group was less obvious since changes in the zGRF distribution between the braced and unbraced conditions were smaller.
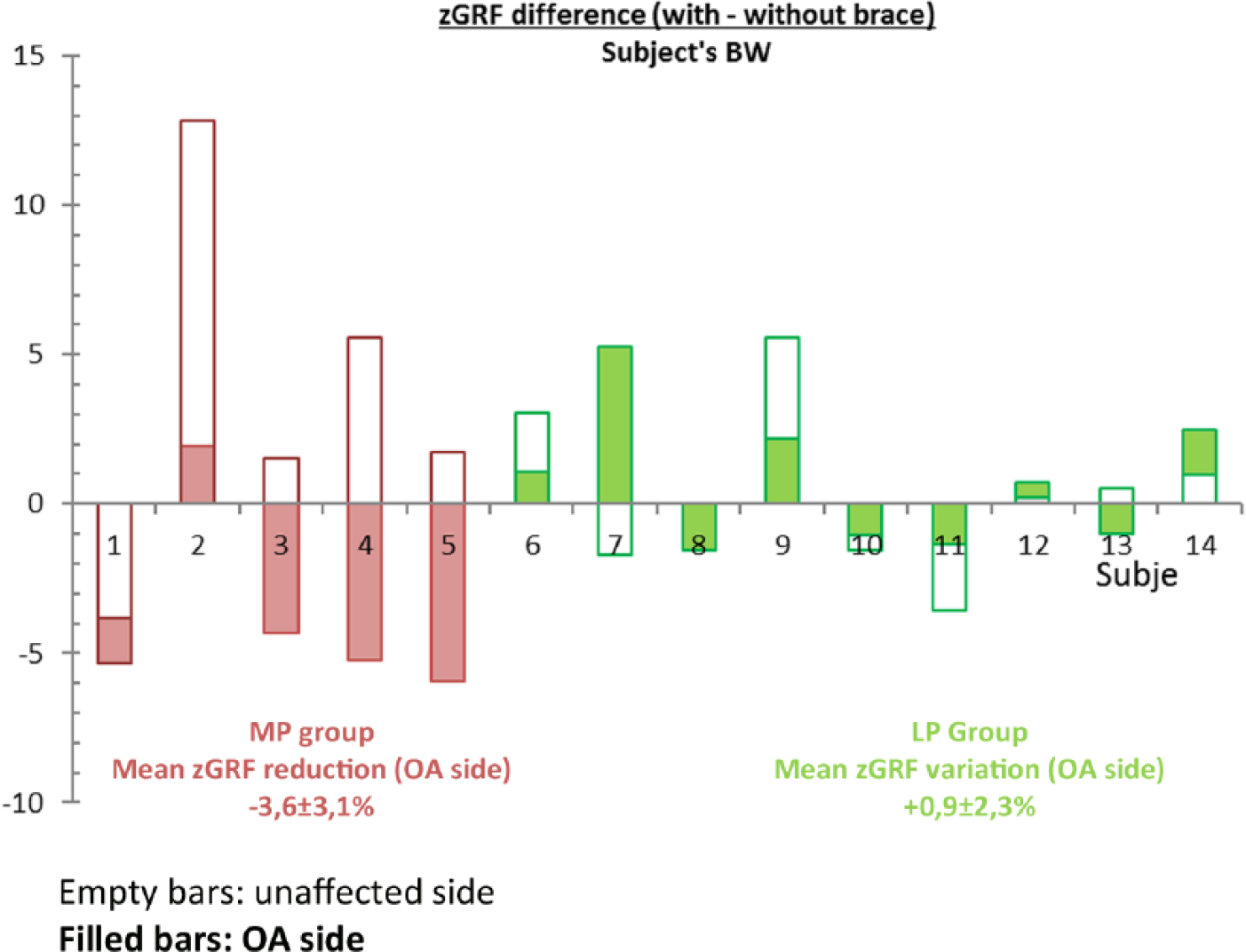
Changes in normalized zGRF on the unaffected and OA sides (from unbraced (control) to braced condition) for each participant while walking with the brace. Pink filled bars represent the zGRF increase or reduction in the OA side of the MP group. Green filled bars represent the zGRF increase or reduction in the OA side of the LP group. Empty pink and green bars, respectively, represent the zGRF changes in the unaffected sides of the MP and LP groups.
Discussion
Walking with the brace significantly decreased the peak hip abduction moment on the OA side. The peak adduction and internal rotation angles were significantly decreased on average over all participants. Because these gait modifications were associated with a reduction in pain in the LP group (n = 9), the reduction in the hip abduction moment might be due to the positive unloading effect of the brace in this group, whereas it might result from a pain-avoidance mechanism in the MP group.
Our hypothesis was supported by the results. First, significant reduction in the peak hip adduction and internal rotation angles during the single support phase of the OA leg indicates that the femur was pulled into external rotation and abduction by the brace. This pulling movement comes from the tension imposed by the stretched elastic strap during the extension phase of the OA hip at stance. A previous study by Wallace and Barr 19 already reported that the peak hip adduction significantly decreased and the peak external rotation significantly increased in people with knee OA when using the tension of a neoprene strap wrapped around the thigh and anchored around the pelvis in a different setting. Our study confirms that greater hip abduction and external rotation can be obtained from a hip brace using the tension of an elastic strap and the support of a pelvis belt.
Second, we observed a significant reduction in hip abduction moment on the OA side, which is considered a major indicator for hip unloading. 11 However, the cause for this reduction appeared to be different in the LP and MP groups as shown by the variations of the zGRF.
The zGRF vector represents the sum of all net muscle and gravitational forces acting at each instant of time over the stance period. 20 Its value fluctuates up to ±20% of body weight and is used to describe the load on the body. 21 However, the causes for the fluctuations of the vertical load curve in an OA population might be difficult to identify due to the sensitivity of the zGRF to any action of the body. 21 In a study on the WISH brace, Yamaji et al. 17 qualified the zGRF as an indicator showing ‘how strong’ the steps of patients were. According to this interpretation, the results indicate that the MP subjects may have attempted to reduce the impact on the OA side as they seemed to walk with stronger steps on the unaffected side. Thus, in the MP group, the reduction in the hip abduction moment might result from a pain-avoidance mechanism that decreased the force on the femoral head to protect the joint instead of an effect of the brace. This finding is consistent with a study from Hurwitz et al. 7 showing that pain reduction is correlated with decreased zGRF among other gait adaptations and leads to decreased hip moments as well as decreased demand on hip muscles. The risk of this unloading strategy is that a decreased activity of the abductors might result in muscle weakness in the long term and cause further complications on other joints. 22
The LP group showed smaller changes in the distribution and magnitude of the zGRF in both limbs when walking with the brace; although the strategy employed was less obvious than for the MP group, it might provide a different explanation for the reduction in hip abduction moment in this group. First, it means that the global loading response at each step was not altered when wearing the brace. In particular, five LP subjects seemed to improve recruitment of their braced OA hip during ambulation by increasing the zGRF in both limbs. Thus, LP subjects did not try to avoid recruiting their braced OA leg in contrast to the MP group. Therefore, the reduction in the hip abduction moment by 6.18% ± 10.04% in the LP group might be attributable to the effectiveness of the brace. However, the mechanical cause for reduction in hip abduction moment in the LP group remains unclear.
Both the LP and MP groups developed unloading strategies via lowering of the hip abduction moment but only the LP subjects seemed to benefit from the mechanism induced by the brace. The different causes for reduction in hip abduction moment in the LP and MP groups mainly depended on subjects’ ability to recruit their braced limb as shown by the changes in the distribution of the zGRF. Recruitment of the OA hip probably depends on the confidence that subjects have in their braced leg during testing. The fact that MP subjects walked with less strong steps could reflect a lack of confidence in using a new device which significantly modified their way of walking. Indeed, all of the MP subjects reported a ‘restriction of movement’ when walking. On the contrary, in the LP group, six subjects rather mentioned the good support provided by the brace, in particular the pelvis belt. This feedback confirms that time for adaptation and acceptation of the medical device remains to be an important parameter to consider when evaluating the brace effectiveness. For this reason, developing a compliant design is essential for brace acceptance.
Additional outstanding queries remain unanswered and constitute the main limits of this study. First, with a majority of subjects in the LP group, this study shows that hip bracing can bring immediate relief in patients with hip OA. However, the reason for pain reduction in this group remains unknown and could help to improve the mechanism of the brace. We can only presume that pain reduction results from a decrease in the internal abduction moment, as it is a major contributor to joint compression. In addition, the changes in rotation and abduction may alter the weight bearing area between the femur and the acetabulum. This new area could be less affected by the disease and thus less painful on compression. Nevertheless, this second mechanism enhancing pain reduction is uncertain. Indeed, the MP group showed greater hip abduction and external rotation than the LP group with the brace which implies greater rotation of the femoral head, and yet they reported more pain. Further research focusing on OA location and severity is needed to investigate this further. Finally, inherent limits of the human movement analysis such as soft tissue artefacts may influence the kinematic changes observed between conditions, and long-term studies to assess the effectiveness of the brace and its mechanism are encouraged.
Conclusion
Wearing the hip brace would appear to reduce the compressive joint reaction force at the femuroacetabular interface as indicated by a reduction in internal hip abduction moment along with immediate pain reduction in nine participants. In the LP group, reduction in internal hip abduction moment may be achieved by the action of the brace, whereas it probably resulted from a decreased demand on the OA limb in the MP group as indicated by the decreased zGRF.
Considering that effective hip bracing should not alter but rather support the recruitment of the OA hip, we suggest that confidence in the braced limb is an essential parameter to regain mobility. Therefore, further long-term studies on a bigger population are warranted to test whether acclimatization to the brace after longer use would show greater reduction in joint load and greater recruitment of the braced hip.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Micah Nicholls is employeed by Össur hf, Reykjavik, Iceland.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was fully funded by Össur hf, Reykjavik, Iceland.