
Abstract
The purpose of this study was to examine the effects of laterally wedged foot orthotic devices, used to treat knee osteoarthritis, on frontal plane mechanics at the rearfoot and hip during walking. Thirty individuals with diagnosed medial knee osteoarthritis were recruited for this study. Three dimensional kinematics and kinetics were recorded as the subjects walked in the laboratory at an intentional walking speed. Peak eversion, eversion excursion and peak eversion moment were increased while the peak knee adduction moment was reduced in the laterally wedged orthotic condition compared to the no wedge condition. In contrast, no changes were observed in the variables of interest at the hip. There was no significant relationship between the change in the peak frontal plane moment at the rearfoot and change in the peak frontal plane moment at the knee or hip as a result of the lateral wedge. Laterally wedged foot orthotic devices, used to treat knee osteoarthritis, do not influence hip mechanics. However, they do result in increased rearfoot eversion and inversion moment. Therefore, a full medical screen of the foot should occur before laterally wedged foot orthotic devices are prescribed as a treatment for knee osteoarthritis.
Keywords
Introduction
Recently, the Center for Disease Control estimated that $128 billion is spent annually on treating arthritis and other rheumatic conditions.1 This recent report highlights the significant economical impact of arthritis along with the concurrent physical disability. Concurrently, recent research has focused on economical treatment options for arthritis. Knee osteoarthritis (OA) is one of the most common forms of this disease, and the medial compartment is most often affected. This can be treated conservatively with various unloading braces for the knee.2,3 However, the compliance with these devices can be problematic due to the fact that they are perceived as being cumbersome to implement on a daily basis.4 Another effective and economical treatment option for medial knee OA is the laterally wedged foot orthotic device.5,6
The laterally wedged foot orthosis indirectly affects the knee by altering foot alignment.7 The device has been reported to reduce pain and pain medication use.8-16 It has also been reported that the device is effective in reducing the compressive forces in the medial compartment of the knee in patients with medial knee OA.17-19 These compressive forces have previously been suggested to relate to the progression of medial knee OA.20,21 While it appears that the wedged foot orthotic device is effective in reducing knee symptoms, little is known about its effect on adjacent joints. It is possible that effects at these other joints may have potentially negative consequences.
To date, only one study has examined the effect of laterally wedged orthoses on joints other than the knee. Kakihana et al.18 observed an increase in the peak frontal plane rearfoot moment with a concomitant reduction in the peak frontal plane knee moment. These results were noted both in subjects with knee OA and in healthy age-matched subjects. Contrary to expectation, no changes were reported in frontal plane rearfoot or knee motion in either group as a result of the lateral wedging. However, these authors only examined a 6° wedge. Recent research has suggested that increased wedging (10°) may be necessary to alleviate symptoms in individuals with Kellgren-Lawrence grades of ≥3.17 This increased amount of wedging may place a greater stress on joints adjacent to the knee, thus, the effect of greater amounts of wedging also needs to be explored. In addition, it is likely that a laterally wedged foot orthosis will have its greatest effect at the foot, with a decreasing effect at more proximal joints. However, the effect of these devices on hip mechanics has yet to be examined.
Therefore, the purpose of this study was to examine the effect of an individually prescribed lateral wedged foot orthosis (5–15°) on rearfoot and hip mechanics during walking in patients with knee OA. It was expected that peak rearfoot eversion, eversion excursion, and the peak eversion moment would be increased while the hip would be unaffected when walking in the laterally wedged foot orthoses. However, it was also thought that the changes in the rearfoot would potentially have effects up the entire lower extremity kinetic chain albeit attenuated at each joint. Therefore, it was hypothesized that the change in the peak rearfoot moment in the wedged foot orthotic condition would be significantly related with the change in the peak knee and hip abduction moments in the wedged foot orthotic condition.
Methods
Participants
Thirty individuals with diagnosed medial knee OA, ≥2 Kellgren-Lawrence grade,22 were recruited for the study. Sample size estimates were performed using α = 0.05 and β = 0.20 with the expectations of a 10% difference in the wedged condition for the peak inversion moment.23 It was estimated that at least 25 subjects would be necessary to observe significant differences for the peak knee adduction moment. Specifically, individuals were required to have an average knee pain of > 3/10 on a VAS (visual analog scale) during weight bearing activities during the past two weeks to be included in the study. Potential subjects were excluded if they had any orthopedic or neurologic condition that affected their gait. In addition, they could not be currently undergoing any type of therapy for treatment of their medial knee OA. All subjects signed an informed consent that was approved by the university's Institutional Review Board.
Procedures
At the first visit, the subjects were fitted with the laterally wedged foot orthotic devices. The amount of wedging prescribed was based upon pain reduction during a lateral step down (8 inch step) test. The subject first performed the lateral step down and stated the amount of pain experienced during the activity using a 0–10 VAS. The subject then repeated the step down with various amounts of lateral wedging in a randomized order. Three and five degree increments were used resulting in total wedging between 5 and 15°. Following each step down test, the subject reported a pain level and a different amount of wedging was placed under the subject's foot. The subject was blinded to the amount of wedging that was applied under their foot. This process continued until the minimal amount of wedging that produced the greatest amount of pain reduction was determined. This amount of lateral wedging was applied to the underside of a semi-custom foot orthotic device with a durometer of 70 and a micropuff cover (KLM Laboratories, Valencia, CA, USA). The front edge of the wedge was beveled with a grinder to improve comfort. The orthosis was then fit into a New Balance 812 walking shoe (New Balance Athletic Shoes, Boston, MA, USA) before being donned by the subject. All subjects were then provided an accommodation schedule for the shoes and orthotic devices. The wear time for the devices increased progressively such that the devices could be worn for a full day by the end of a week.
Once the subject had fully accommodated to the devices, they returned to the laboratory for a gait analysis. Retroflective markers were placed on the upper material of the shoe at the base of the 1st and 5th metatarsal, on the medial and lateral malleoli, on the medial and lateral epicondyle of the femur, and on the left and right greater trochanter to model the lower extremity segments for inertial characteristics and to develop the anatomical coordinate systems. Two rigid shells of four tracking markers were attached to the thigh and shank to track the respective segmental positions. To track the position of the pelvis, retroreflective markers were placed on the anterior superior iliac spine, iliac crest and on the skin between the space of the L5 and S1 vertebrae. Rearfoot motion was tracked with three retroreflective markers that were placed directly on the skin over the calcaneus and projected through windows cut in the heel counter of the laboratory shoes (Nike Air Pegasus, Nike Inc., Beaverton, OR, USA). This method was chosen as previous research has reported that markers placed on the heel counter of a shoe overestimates true rearfoot motion.24 Following a standing calibration trial, the anatomical markers were removed so that the medially placed markers did not alter the individual's gait mechanics during the dynamic trials. However, the attachment posts were kept on the subject in order to ensure reproducibility of the anatomical markers between the laterally wedged and non-wedged conditions.
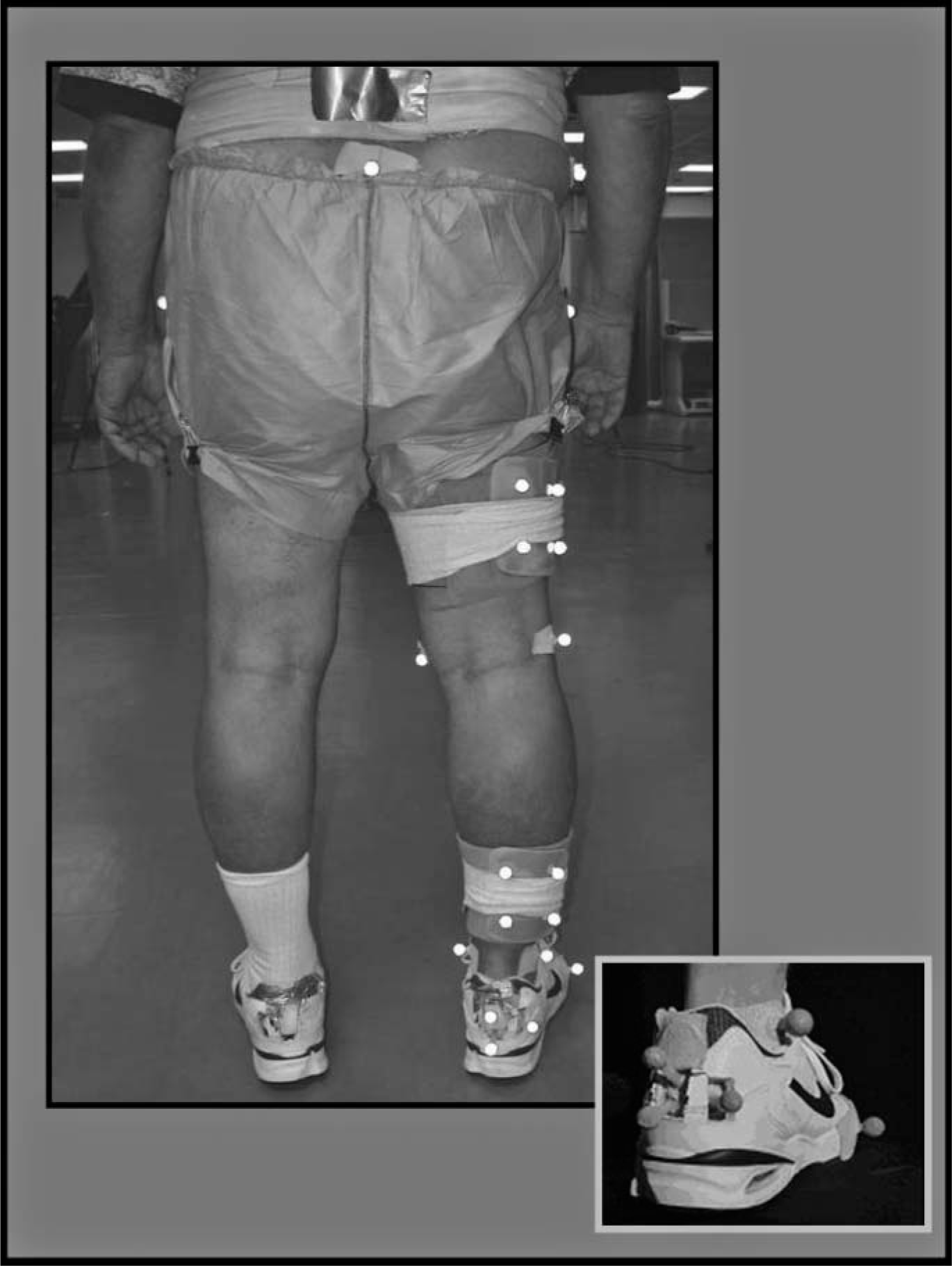
Marker set-up used for the gait analysis (Inset figure portrays markers placed on rearfoot and forefoot).
The gait of each subject was analyzed in the laterally wedged condition as well as in a semi-custom orthosis that had no wedging applied. The order of the conditions was randomized in order to remove any order effects. Subjects walked across a walkway at a constant velocity within 5% of their previously determined intentional walking speed. An intentional walking speed was defined as a pace that they would use to get mail from their mailbox or some other daily functional task.
During the walking trial, the marker trajectories were recorded using a six camera motion analysis system that recorded the marker position at 120 Hz (Vicon Ltd., Oxford, UK). Ground reaction force data were recorded using a force platform recording at 1080 Hz (Bertec Corp., Columbus, Ohio, USA). Visual 3D software (C-motion, Bethesda, MD, USA) was then used to calculate three dimensional lower extremity joint kinematics and kinetics during the walking trial. Five acceptable trials (within 5% of self-selected walking speed) were averaged and normalized from heel strike to toe off to examine the variables of interest.
Data analysis
The variables of interest for the study related to the frontal plane mechanics at the rearfoot and hip. The frontal plane moment at the knee was also examined to assess the effectiveness of the laterally wedged orthotic devices in altering the peak knee adduction moment. The peak knee adduction moment has previously been correlated with compressive forces in the knee and knee osteoarthritis progression.20,21,25 At the rearfoot, peak eversion, eversion excursion (from footstrike to peak eversion) and the peak eversion moment in the two orthotic conditions were assessed. At the hip, the variables included peak hip adduction, hip adduction excursion (from footstrike to peak adduction), and the peak hip adduction moment. Finally, the change in the peak inversion moment between conditions was correlated with the change in the peak frontal plane moment at the knee and hip between conditions.
All statistical analyses were performed using SPSS version 14 (SPSS, Chicago, IL, USA). Dependent samples t-tests were used to determine differences between the laterally wedged orthotic (LW) and no wedge (NW) orthotic condition. Bivariate correlation was used to examine the relationship between the change in the rearfoot frontal plane moment and the change in the peak knee and hip adduction moment as a result of the wedge. All significant differences were detected using a critical p-value of 0.05.
Results
The average age of the 30 subjects (17 females and 13 males) was 63.1 ± 6.8 years and their BMI was 33.8 ± 6.9 kg/m2. Nine of the subjects had a K-L grade of 2, nine of the subjects had a K-L grade of 3 and 11 of the subjects had a K-L grade of 4. The average amount of lateral wedging that was prescribed for the subject was 10.0 ± 3.2°. It was interesting to note that the amount of wedge needed to reduce pain during a step down significantly increased with the K-L grade (Figure 2).
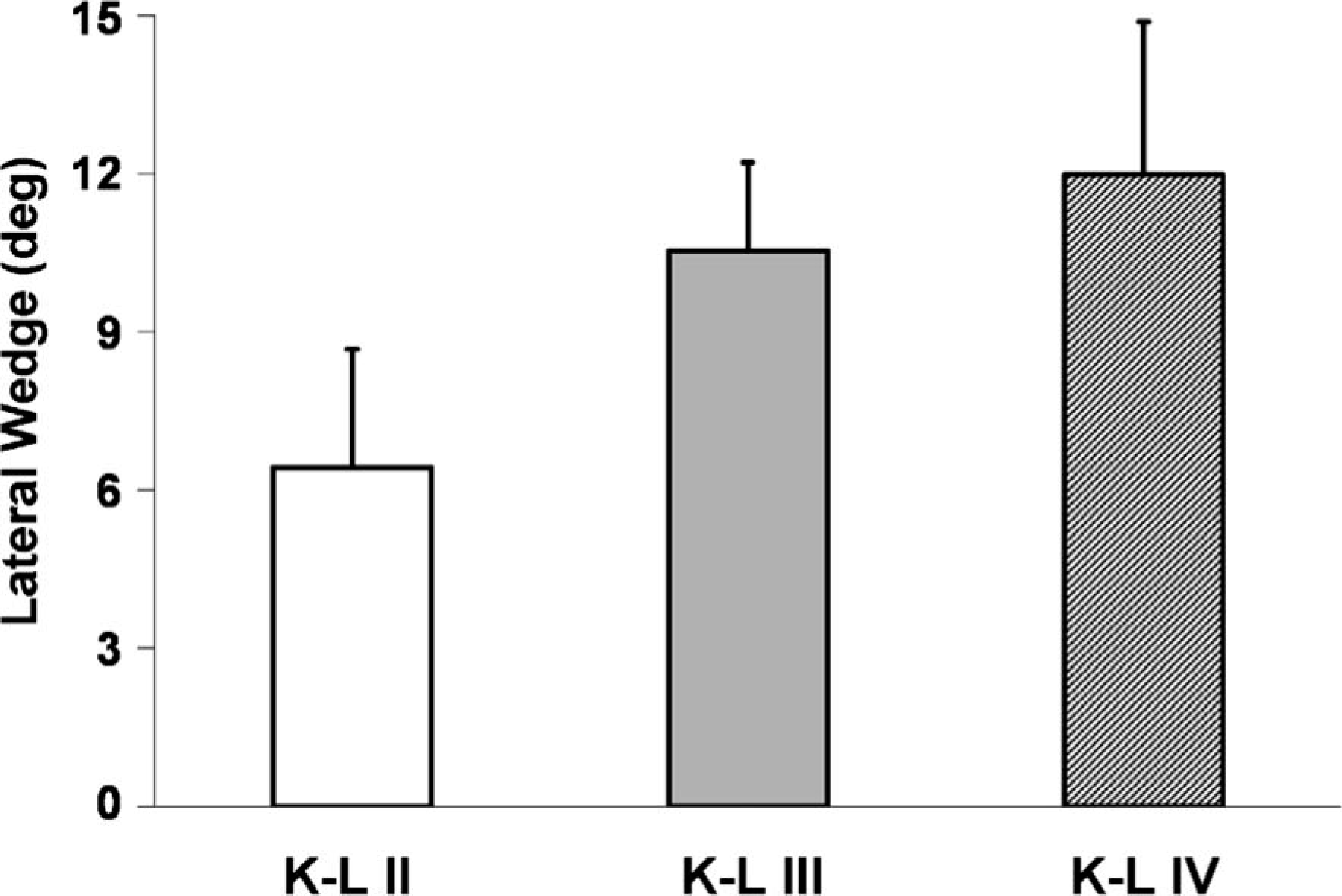
Subject selected amount of lateral wedging in degrees (°) that reduced pain during a lateral step down test for the different Kellgren-Lawrence (K-L) grades.
The LW condition did significantly reduce the peak knee adduction moment by 10% compared to the NW condition (Figure 4). At the rearfoot, peak eversion and eversion excursion significantly increased (1.8 and 3.4°, respectively) in the LW condition compared to the NW condition (Table I and Figure 3). In addition, the peak eversion moment increased by 93% in the LW (Table I and Figure 4). At the hip, neither peak hip adduction, hip adduction excursion, nor the peak hip adduction moment were significantly altered by the LW condition (Table I, Figures 3 and 4).
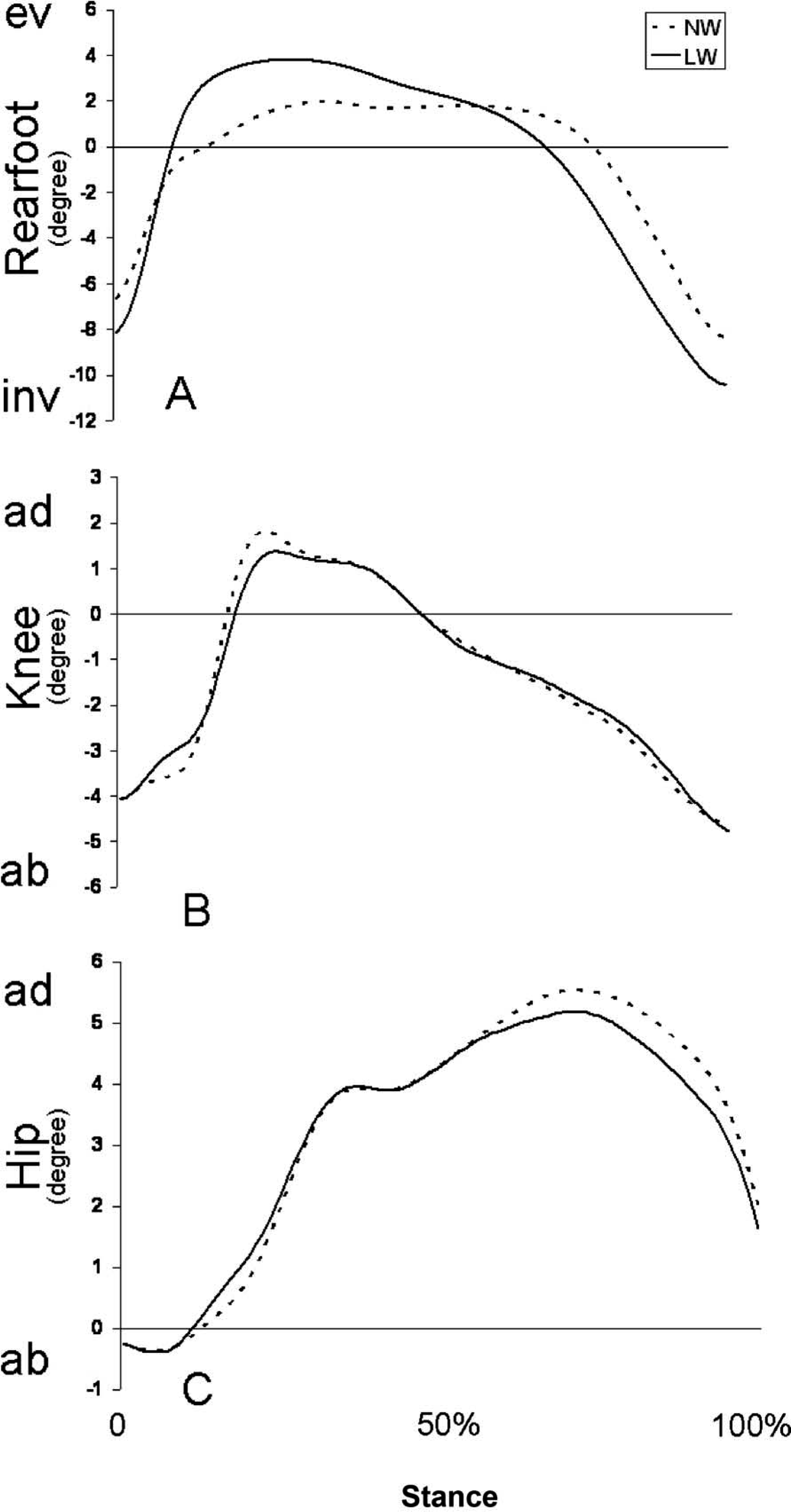
Ensemble graphs for all of the subjects frontal plane angles (°) at the rearfoot. (A) in = inversion, ev = eversion), knee. (B) ad = adduction, ab = abduction) and hip. (C) ad = adduction, ab = abduction) in the laterally wedged foot orthotic device (LW, solid) and non-wedged (NW, dashed) foot orthotic device during the stance phase of walking.
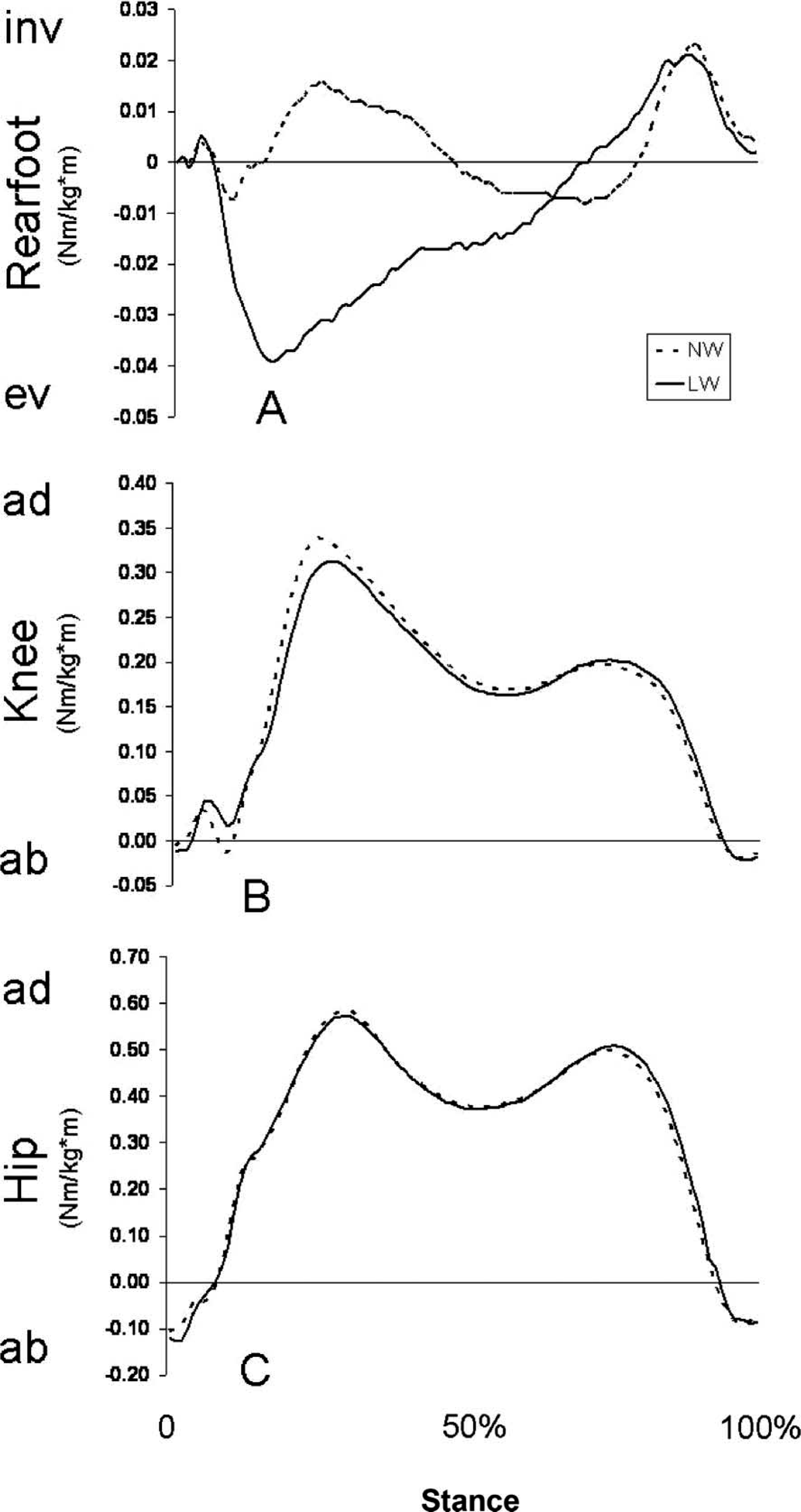
Ensemble graphs for all of the subjects frontal plane moments (Nm/kg∗m) at the rearfoot (A) in = inversion, ev = eversion, knee. (B) ad = adduction, ab = abduction, and hip. (C) ad = adduction, ab = abduction, in the laterally wedged foot orthotic device (LW, solid) and non-wedged foot orthotic device (NW, dashed) during the stance phase of walking.
Means, standard deviations and statistical findings for the variables of interest.
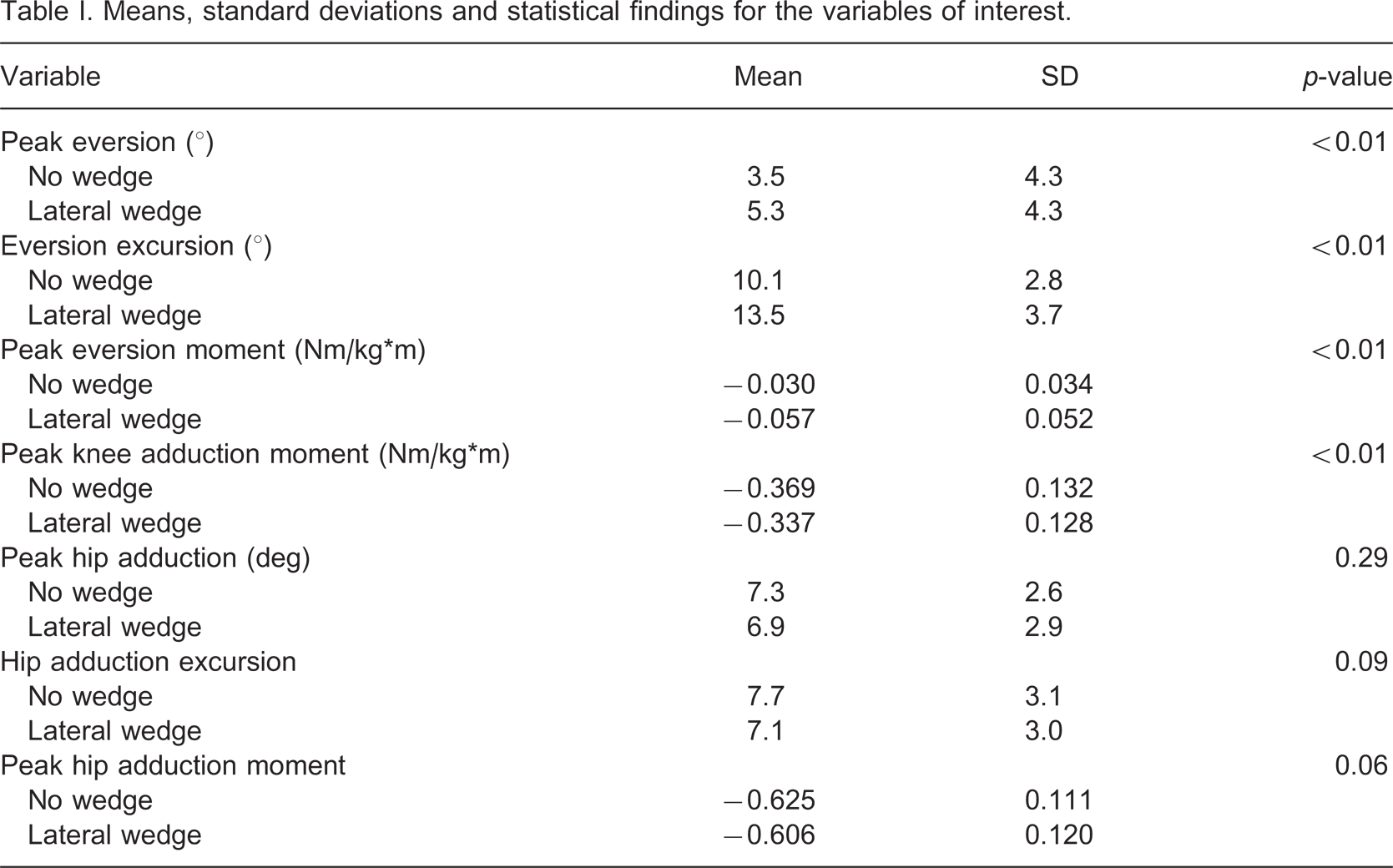
Surprisingly, there was no relationship between the change in the rearfoot frontal plane moment and the change in the frontal plane moment at the knee. The same was true for the relationship between rearfoot and hip. However, it is noteworthy that the relationship between the rearfoot and knee approached significance (p = 0.06, r = −0.345) but this was not the case for the relationship between the rearfoot and hip (p = 0.48, r = −0.136).
Discussion
The aim of the current study was to examine the changes in frontal plane gait mechanics at the rearfoot and hip when a LW foot orthotic was used to treat symptoms associated with medial knee OA. It appears that the LW foot orthotic causes increased movement and joint moments at the rearfoot but has no effect at the hip (Figures 3 and 4) while reducing joint moments at the knee. Surprisingly, the changes observed at the rearfoot were not correlated with changes observed at the knee or hip.
The increased amount of eversion, as well as eversion moment, suggest that greater muscle torques are required to control the increased amount of rearfoot motion in the laterally wedged condition. These findings were similar to those of Kakihana et al.18 who observed an increased frontal plane moment and peak eversion with a 6° lateral wedge. Therefore, it is possible that the LW device may adversely affect individuals with a foot pathology exacerbated by excessive eversion.
As a result of this finding, greater caution should be taken when prescribing the LW device for individuals with foot conditions that are worsened by an increased frontal plane load and increased rearfoot eversion, such as a hallux valgus, flexible pes planus, or plantar fasciitis. Individuals with these conditions may benefit more if they are prescribed a varus unloading knee brace to conservatively treat their knee OA. However, since there is no long term data available on the LW foot orthotic devices, all individuals with asymptomatic foot types who are prescribed the device should be monitored for increased symptoms to their feet due to the increased movement and moments that occur as a result of the devices. Additionally, there is currently no research on the effect of the LW orthotic device on the contralateral limb which may need to attenuate altered forces as a result of the device. Therefore it is important to monitor both feet for any changes in symptoms. Based upon this potential increased risk, we recommend using the device for activities of daily living, but not for activities of higher loading such as running and jumping. In order to minimize adverse effects of the device it is recommended that the laterally wedged foot orthotic is also adequately supportive of the foot. The orthosis that was used in the current study had a contoured surface that supported the arch. This contour potentially assisted in minimizing arch flattening while improving the transfer of motion from the foot to the knee.
In contrast to the rearfoot, frontal plane mechanics of the hip appear to be unaffected by the LW device. This suggests that there may be no adverse effects expected at the hip as a result of the devices. These results are similar to a previous study that reported a minimal effect of foot orthoses on hip mechanics.26 However, it is important to note that the current study included individuals with only knee OA. Individuals with both hip and knee OA may respond differently than our cohort. Therefore, any individual who has a history associated with the development of hip osteoarthritis should be monitored closely if a LW device is prescribed until further information is available.
The lack of a relationship between the change in rearfoot moment and change in hip moment was not surprising as the hip moment was not altered in the wedged condition. However the frontal plane rearfoot moment was significantly increased, and the frontal plane knee moment was significantly decreased by the LW. Thus, an inverse relationship was expected. While not statistically significant, the results suggested that this relationship was present. However, the observed relationship only explained 12% of the variance between the variables and thus it appears that there are additional factors that affect the relationship between the frontal plane rearfoot and knee moments.
In conclusion, the results of this study suggest that a laterally wedged foot orthotic device increases the eversion moment, peak eversion, and eversion excursion at the rearfoot during walking, while there is no effect of the devices on the frontal plane mechanics of the hip. This is the first study to examine acute changes in rearfoot and hip joint mechanics during walking as a result of the LW. However, follow-up studies are needed to determine the effect of the devices on the contralateral limb joint mechanics as well as examining whether there are any deleterious long-term effects of LW on the rearfoot and hip.
Footnotes
Acknowledgements
This publication was made possible by Grant Number P20 RR016458-05 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NCRR or NIH. The authors wish to thank Nike, Inc. for donating the footwear used for the laboratory experiment. The authors also wish to thank New Balance, Inc. for donating the footwear used during the accommodation period of the study.