
Abstract
This study was conducted to compare the effects of three ankle-foot orthosis (AFO) designs on walking after stroke and determine whether an ankle plantar flexion contracture impacts response to the AFOs. A total of 30 individuals, ranging from 6–215 months post-stroke, were tested in four conditions: shoes only (SH), dorsi-assist/dorsi-stop AFO (DA-DS), plantar stop/free dorsiflexion AFO (PS), and rigid AFO (Rigid). Kinematics, kinetics, and electromyographic (EMG) activity were recorded from the hemiparetic lower extremity while participants walked at a self-selected pace. Gait parameters were compared between conditions and between participants with and without a moderate ankle plantar flexion contracture. All AFOs increased ankle dorsiflexion in swing and early stance. Anterior tibialis EMG was reduced only in the PS AFO. Both PS and Rigid AFOs restricted ankle plantar flexion and increased knee flexion in loading. Peak ankle dorsiflexion in stance and soleus EMG intensity were greatest in the PS AFO. The Rigid AFO tended to restrict dorsiflexion in stance and knee flexion in swing only in participants without a plantar flexion contracture. Individuals without a contracture benefit from an AFO that permits dorsiflexion mobility in stance and those with quadriceps weakness may more easily tolerate an AFO with plantar flexion mobility in loading.
Introduction
Approximately 70–80% of stroke survivors will recover the ability to independently walk short distances without assistance of another person. 1,2 Only 50%, however, achieve limited community ambulation status or better. 1,2 Following a stroke, weakness, abnormal muscle activity, and joint deformity can impair the weight-bearing capability of the limb, as well as the ease of clearing the floor in swing. 3,4 Ankle-foot orthoses (AFOs) are frequently prescribed for patients with hemiplegia to enhance walking function by providing stability during stance or foot clearance during swing. 5,6
AFO designs vary from highly stable to extremely flexible. In the most stable AFO designs, the ankle is held in a rigid position with limited movement in all planes. The more
flexible designs, by use of articulating joints or lighter weight plastics, are designed to provide adequate dorsiflexion during swing to lift the foot but still allow some ankle movement during stance. Mechanical stops can be added to articulating orthoses to limit the maximal excursion of dorsiflexion or plantar flexion.
Many previous studies have documented the affect of a rigid AFO on gait of persons with hemiplegia. 7–11 The stability provided by a rigid AFO has been shown to increase stride length 7–9 and velocity 8–10 when set at neutral or 5° of dorsiflexion compared to walking without an orthosis. The restriction of plantar flexion mobility during loading in a rigid AFO, however, causes the tibia to rotate forward more quickly, at the same rate the foot rotates towards the floor, and results in increases in the knee flexion moment 10,11 and EMG intensity of the vastus lateralis muscle during loading. 12
Fewer studies have evaluated the more flexible and articulating designs. Lehmann et al. 13 compared non-articulating, polypropylene AFOs of varying degrees of stiffness, as determined by trim lines and heights of the braces, and found all AFOs increased dorsiflexion in swing, but only the stiffest design provided added stability during stance. Articulated AFOs with a plantar flexion stop produced modest increases in walking speed (0.05–0.07 m/sec). 14,15 The plantar-stop AFO improved dorsiflexion in swing and early stance but also produced an external knee flexion moment in loading that was greater compared to both walking in shoes only and that seen in able-bodied control participants. 15 The increased acceleration into knee flexion can reduce knee hyperextension but can also produce instability in individuals with quadriceps weakness.
The effect of an articulating orthosis with a dorsiflexion stop and a dorsiflexion assist on walking has not been documented. In addition to assisting dorsiflexion in swing, this AFO is designed to allow plantar flexion during early stance to avoid exacerbating knee flexion in loading. Additionally, this AFO design permits dorsiflexion in stance initially, and then limits it with a mechanical stop to prevent excessive dorsiflexion in late stance that often results from calf weakness. 3
The relative effects of rigid and articulating AFOs on the walking ability have been compared in children with diplegic cerebral palsy. 16–18 Both rigid and articulating (plantar-stop) AFOs improved stride length but not velocity and resulted in increased dorsiflexion in swing and early stance. 16–18 In terminal stance, however, the articulated AFO (with a plantar flexion stop and free dorsiflexion) allowed greater (and more normal) peak dorsiflexion than either the rigid AFO or walking without an orthosis. 16–18 Only one study found a significant impact of orthosis type on knee moments in loading. 16–18 Buckon et al. found that the external knee flexion moment was increased in the articulating (plantar-stop AFO) but not the rigid AFO compared to walking without an orthosis. 16 The comparative impacts of rigid and articulating AFOs on walking have not been investigated in the adult hemiplegic population.
There is also a need to relate performance in an AFO to the individual's clinical presentation. Woolley 4 emphasized the importance of a clinical assessment to the selection of an appropriate orthotic device, yet few studies relate performance in an AFO to the clinical parameters of the participants. Plantar flexion contracture is a common impairment after stroke. 19 A plantar flexion contracture can prevent progression of the limb over the foot during stance, potentially interfering with the ability to properly use the mobility afforded by an articulating brace. The purpose of this study was two-fold: (i) To compare the effects of three different plastic AFO designs and shoes only on the gait parameters of individuals after stroke, and (ii) to identify whether plantar flexion contracture impacts an individual's response to bracing.
The three different AFO designs tested include: (1) An articulated orthosis that restricts plantar flexion while allowing free movement into dorsiflexion (plantar-stop [PS]), (2) an
articulated orthosis that has unrestricted motion into plantar flexion, with assistance into dorsiflexion and a stop to limit excessive dorsiflexion (dorsi-assist/dorsi-stop [DA-DS]), and (3) a rigid design that limits both plantar and dorsiflexion (Rigid). We proposed four hypotheses based on the design features of each orthosis and the current literature: (1) All AFO designs would improve walking speed, increase ankle dorsiflexion in swing, and reduce intensity of anterior tibialis EMG compared with walking without an orthosis; (2) the Rigid and PS orthoses (both with restricted plantar flexion) would increase both knee flexion motion and moments in loading response requiring increased activation of vastus intermedius; (3) intensity of soleus EMG would be reduced only in the Rigid AFO compared to walking in shoes only; and (4) dorsiflexion in stance would be decreased in the Rigid AFO and increased in the PS AFO compared to walking without an orthosis only for participants without a plantar flexion contracture.
Methods
Participants
Individuals with stroke were recruited from out-patient clinics at Rancho los Amigos National Rehabilitation Center and from local stroke survivor support group meetings. Eligibility for participation required that participants were at least six months post cerebrovascular accident (CVA), and either currently used an AFO for ambulation or had an AFO recommended by a physician or physical therapist. In addition, participants were required to have maximal passive ankle dorsiflexion mobility with knee extension that was either equal to or greater than 0° or between 10 and 15° of plantar flexion measured manually with a goniometer. We selected this range of mobility for the moderate contracture group to ensure separation from those without contracture and to avoid more severe contractures that would not be amenable to control by an orthosis. Individuals requiring physical assistance to walk were excluded, as were persons whose self-selected walking speed was greater than 1.0 m/sec−1 (73% normal walking speed). A written statement of informed consent, approved by the Institutional Review Board of the Los Amigos Research and Education Institute, was obtained from each participant.
A total of 30 participants were tested, nine with passive ankle dorsiflexion (DF) to at least neutral with full knee extension (mean 1.2° dorsiflexion with knee extension and 7.2° with knee flexion) and 21 with passive dorsiflexion limited to 10–15° of plantar flexion (mean 10.7° plantar flexion with knee extension and 1.5° dorsiflexion with knee flexion) (Table I). Mean age for the 30 participants was 58.3 years (range = 36–75 years) and average time since CVA was 25.3 months (range = 6–215 months). The group included seven women (left CVA = 4; right CVA = 3) and 23 men (left CVA = 8; right CVA = 15).
Orthotic fabrication
Enrollment in the project began with the fabrication of two orthoses: Rigid and articulating. Participants wore their own shoes and wore this same pair of shoes for all testing. To provide a model of the shank and foot and accommodate the varying shoe heel heights, a certified orthotist created a cast of the participant's lower leg with the ankle positioned in approximately neutral dorsiflexion (resulting in 5° of anterior inclination of the tibia in their shoe). From this cast, the orthotist fabricated both the Rigid and articulating orthoses. The articulating AFO was made with articulating ankle joints (Oklahoma joints), a posterior chamber, and a posterior strap. For the DA-DS orthosis, rubber straps were attached to
grommets to assist with dorsiflexion and the posterior strap was set to restrict dorsiflexion so that anterior inclination of the tibia in the shoe was limited to 5° (Figure 1). For the PS orthosis, the posterior strap was removed to allow free dorsiflexion and a small plastic wedge was screwed down from the posterior chamber of the orthosis to provide the plantar flexion stop at 0°.
Clinical characteristics of participants stratified by contracture group mean (SD) and range.

significant main effect of group.

Three AFO designs: Rigid, dorsiflexion assist/dorsiflexion stop (DA-DS), and Plantar flexion stop (PS).
The order of distribution of the three AFO designs was determined by random assignment. Approximately one week after the casting, an initial fitting and training session was provided by the orthotist and a physical therapist. Each AFO was worn by the participant in the community for at least two weeks prior to quantitative gait testing. At the conclusion of a quantitative gait assessment session, the next orthosis was fitted and the participant received a gait training session with the physical therapist to assist in adjusting to the new orthosis.
Strength and spasticity assessment
Maximal isometric torques were recorded in a sitting position with a LIDO Active dynamometer (Loredan Biomedical Inc., Davis, CA, USA) during two 5-second trials for the ankle plantar flexors, ankle dorsiflexors, knee extensors, and hip flexors of each participant's paretic leg. A tensiometer recorded the maximal isometric force produced by the hip extensors. The lever arm utilized during the effort was measured manually and used to calculate hip extension torque values. Peak torque values were averaged from the two trials for each muscle group and expressed both in absolute values (Nm) and as a percentage of gender-matched normal using a laboratory database of maximal isometric torques in non-disabled individuals 40–65 years of age. Spasticity of the calf was assessed with the Modified Ashworth Scale. 20
Gait testing
Quantitative gait analysis was performed with the participant walking at a self-selected speed over a 10-m walkway. The central 6-meters were designated by photoelectric cells for data acquisition. Gait testing included simultaneous acquisition of spatio-temporal parameters, lower extremity motion and kinetics, and fine-wire electromyography (EMG). Two trials of ambulation at a self-selected speed were collected for each orthotic condition. Walking in shoes without an AFO was conducted during each of the three AFO assessments.
Spatio-temporal parameters. Individually sized footswitches (B & L Engineering, Tustin, CA, USA) were taped to the bottom of each shoe. Each footswitch contained a compression closing switch located under the heel, 1st metatarsal head, 5th metatarsal head, and great toe.
Motion analysis. A six-camera Vicon Motion Analysis system (Vicon Motion Systems, Oxford, UK) was utilized to acquire three-dimensional motion for the trunk, pelvis, and paretic lower extremity. Retro-reflective spheres (17 mm diameter) were taped onto the skin overlying bony landmarks including the midline sacrum at the level of the posterior iliac spines, anterior superior iliac spine (bilaterally), greater trochanter, anterior thigh, medial and lateral femoral condyles, and anterior tibia. Markers were also placed on the shoe (at the level of the 1st and 5th metatarsal heads, over the dorsal aspect of the foot, and on the posterior heel) and on the orthosis (over the medial and lateral malleoli).
Joint kinetics. Ground reaction forces were recorded by a force plate (Kistler Instrument Corp, Amherst, NY, USA) embedded in the center of the walkway. Participants were positioned within the walkway to permit force plate contact by only the test (paretic) foot. Walking was repeated until two successful trials with the participant's paretic foot landing
completely within the force plate were recorded. Any trial that resulted in only part of the foot landing within the force plate was discarded. Anthropometric measures were obtained for each participant including height, weight, limb segment length, and limb segment circumference.
Fine-wire EMG. A pair of nylon-coated, stainless steel wires were inserted into the muscle bellies of tibialis anterior (AT), soleus, and vastus intermedius (VI) using a 1.5-inch, 25-gauge hypodermic needle as a cannula. 21 Electrode placement was confirmed by palpation of tension within the muscle belly and tendon in response to a brief electrical stimulus passed through the wires. EMG signals were transmitted by FM-FM telemetry (Biosentry Telemetry Inc, Torrance, CA, USA) (Model 2600), band-pass filtered through an analog filter (150–1000 Hz) and sampled and digitized at a 2500 Hz rate with a uniform gain of 1000. EMG signals were recorded during a 5-sec manually-resisted maximal voluntary effort for each muscle prior to the walking trials. Maximal voluntary effort was recorded with the participant supine during resisted isometric contractions of either isolated movements or massed flexion or extension patterns except for soleus which was tested in standing during the isometric portion of a single limb heel rise.
Data management
Footswitch, force plate, and EMG signals were sampled at a rate of 2500 Hz on the acquisition computer (Digital Equipment Corporation, Cambridge, MA, USA). Raw EMG data recorded during walking trials were full wave rectified and integrated over a 0.01 sec processing interval. Integrated EMG data were subsequently expressed as a percentage of the EMG recorded during a participant's maximal voluntary effort (% Max) for each percent of the gait cycle (% GC). For muscles in which the subject lacked sufficient volitional control to produce a significant electrical signal during manual muscle testing, we used a minimum threshold normalization value to prevent inflation of EMG signals during walking. 22
Footswitch data were processed using the EMG-Stride Analyzer Software (B & L Engineering, Tustin, CA, USA). Spatio-temporal parameters (speed, cadence and stride length) were averaged across two gait trials for each test condition. Sub-phases of the gait cycle were defined based on the timing of single and double limb support for each participant. 3 The first period of double limb support just prior to single limb stance is loading response, preswing is the second period of double limb support. Single limb stance is divided into two equal sub-phases, mid and terminal stance. Swing, the period of non-weight-bearing on the reference limb is divided into three equal sub-phases: initial, mid, and terminal swing.
Kinematic data were sampled at 50 Hz on a second, time-synchronized, acquisition computer (Digital Equipment Corporation, Cambridge, MA, USA) and were smoothed with a 6 Hz low pass filter. Kinematic data were processed with Adtech Motion Analysis Software (Adtech Inc, Honolulu, HI, USA) to produce 3-D trajectories for each marker. The position and orientation of each lower extremity segment were obtained and lower extremity joint angles for each percentage of the gait cycle were determined with computer algorithms using Euler embedded coordinates. The foot segment was defined relative to the foot-sole plane, independent of the heel of the shoe in order to reflect anatomical dorsiflexion. An inverse dynamics model was utilized to calculate external net joint moments from force, kinematic, and anthropometric data using linear interpolation to allow expression for each 1% of the GC. The external moments indicate that an opposing internal moment from either muscle or passive structures is required to meet the net joint demands.
Data analysis
All data from the shoes only condition were averaged across the three test sessions. Motion and kinetic data analysis was limited to the sagittal plane for the knee and ankle joints. An ensemble average of all strides (2–6) for each AFO condition was calculated from the kinematic and kinetic data of each participant. Peak values of ankle and knee joint motion and moments were extracted from the ensemble averaged data.
Intensity of EMG activity during walking was determined with the EMG Analyzer Software (B & L Engineering, Tustin, CA, USA). 23 The EMG Analyzer identified the relative intensity of EMG (normalized by manual muscle test value) for each percentage of the gait cycle where the intensity was at least 5% MAX. The average EMG intensity was calculated for each muscle during the sub-phases of gait when each is normally active. 3 Mean EMG activity was calculated for VI from terminal swing through mid stance, soleus from loading response through terminal stance, and AT from pre-swing through loading response.
Baseline clinical characteristics (isometric torques and spasticity scores) were compared between participants in the neutral and moderate contracture groups with an independent t-test using SPSS statistical software (SPSS Inc., Chicago, IL, USA). For all dependent variables during walking, a two-way repeated-measures analysis of variance tested for differences among the four orthosis conditions (three AFOs and shoes-only) and between neutral and moderate contracture groups. A significance level of p < 0.05 was used. If a statistically significant interaction between orthosis condition and contracture group was identified, simple main effects testing was conducted to compare the parameters between orthosis conditions separately for each contracture group. If a statistically significant main effect of orthosis condition was identified, post-hoc comparisons were conducted between each orthosis condition. A Bonferroni correction for multiple comparisons was applied to both post-hoc comparisons and simple main effects tests.
Results
Muscle strength and spasticity
Maximal isometric torques in the paretic leg were reduced compared to non-disabled individuals for all muscle groups tested in both contracture groups (Table I). Muscle weakness was greatest distally in both the ankle plantar flexor and ankle dorsiflexor muscle groups (21.2–30.0% of torques in non-disabled population). Muscle strength was similar in the two contracture groups except for the hip extensors. Participants in the Neutral contracture group had significantly stronger hip extensors than those in the Moderate contracture group (8.8 [4.6] Nm vs. 5.4 [3.2] Nm; and 46.9 [22.5] % non-disabled vs. 30.6 [17.0] % non-disabled respectively, p < 0.05, Table I). Spasticity in the ankle plantar flexors as measured by the modified Ashworth Scale was similar in the two contracture groups with a median value of 1.5.
Stride characteristics
Participants in the neutral group walked at a significantly faster speed than those with a moderate contracture in all AFO conditions (0.597 vs. 0.373 m/sec) (p = 0.014) (Table II). In the neutral group stride length was also significantly longer (0.865 vs. 0.671 m) (p = 0.023), and there was a trend for a faster cadence in the neutral dorsiflexion group (78.7 vs. 63.6 steps/min), but it did not reach statistical significance (p = 0.62). There was a trend for a
faster walking speed in the plantar stop AFO compared to the Rigid AFO, but it did not reach statistical significance (p = 0.55). There were no effects of AFO condition on cadence or stride length for either group.
Stride characteristics - velocity (m/sec), cadence (steps/min) and stride length (m) - (Standard Deviation) for the neutral ankle dorsiflexion and moderate plantar flexion contracture groups.
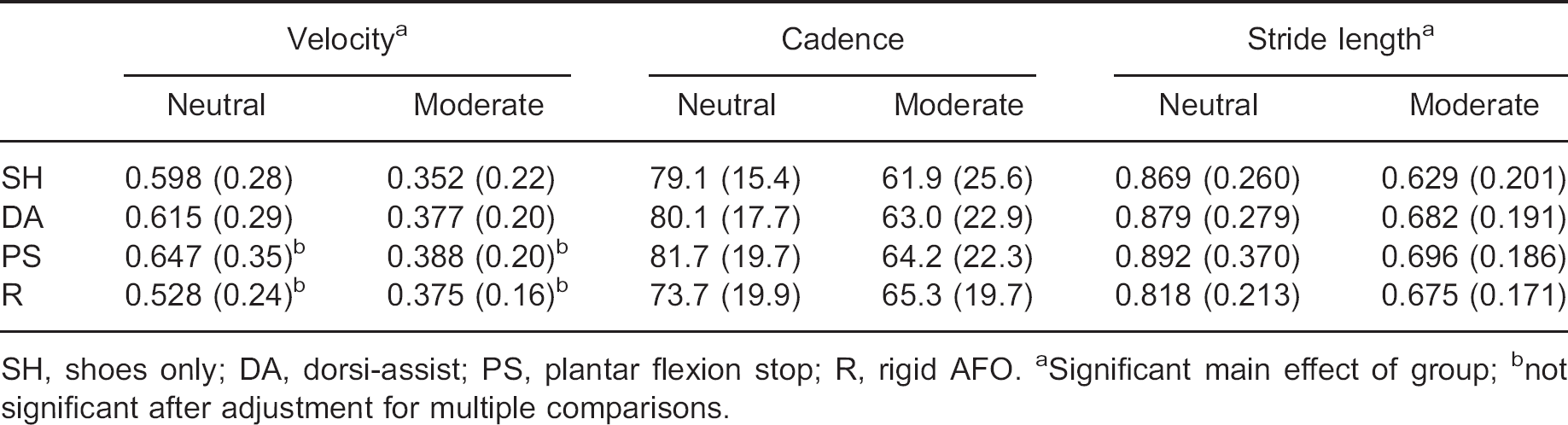
SH, shoes only; DA, dorsi-assist; PS, plantar flexion stop; R, rigid AFO.
Significant main effect of group
not significant after adjustment for multiple comparisons.
Motion
Participants with a moderate plantar flexion contracture had a significantly greater plantar flexion angle at initial contact, less dorsiflexion in stance and mid swing, and a reduced knee flexion angle at initial swing compared to those in the neutral group (Table III, Figure 2 and Figure 3). All three AFOs increased ankle dorsiflexion in mid swing and at initial contact, and reduced plantar flexion during loading response compared to shoes only for both contracture groups (Table III, Figure 2). All three AFOs increased ankle dorsiflexion to a similar extent in mid swing compared to shoes only (an increase of 5–6° for the neutral group and 9–11° for the moderate contracture group). During Loading Response, however, the DA-DS orthosis allowed more plantar flexion than both the PS and Rigid orthoses.
We found a significant interaction between the effects of AFO condition and contracture group for peak ankle dorsiflexion angle in stance (Table III). For the moderate contracture group peak ankle dorsiflexion in stance was greater in the DA-DS and PS AFOs compared with shoes only (6.6 and 7.1 vs. 3.2°). Peak ankle dorsiflexion in stance also was greater in the PS AFO compared with the Rigid AFO (7.1 vs. 4.6°). In the neutral group there was a significant effect of AFO condition on peak ankle dorsiflexion in stance (p = 0.008). Peak ankle dorsiflexion was greater in the PS AFO compared with the Rigid AFO (15.7 vs. 9.3°), but this did not reach statistical significance after adjustment for multiple comparisons. Peak ankle plantar flexion in pre-swing was reduced in all three AFOs compared to shoes only for both groups.
At the knee, all three AFOs led to increased knee flexion at initial contact and loading response compared to shoes only for both groups. In addition, both the PS and Rigid AFO allowed greater knee flexion in loading response than the DA-DS AFO (Table III and Figure 3).
There was a significant interaction between the effects of AFO condition and contracture group for both peak knee extension angle in stance and peak knee flexion angle in swing (Table III). In the moderate contracture group, PS and Rigid AFOs reduced knee hyperextension during stance compared to the shoe condition (0.4 and 0.8 vs. −5.7°). Peak knee flexion in swing, however, was not affected by AFO condition. For the neutral group knee extension in stance was not affected by AFO condition. There was a significant effect of AFO condition on peak knee flexion in swing, however, for the neutral group (p = 0.017).
Peak ankle and knee motion - degrees (Standard Deviation) for the neutral ankle dorsiflexion and moderate plantar flexion contracture groups.
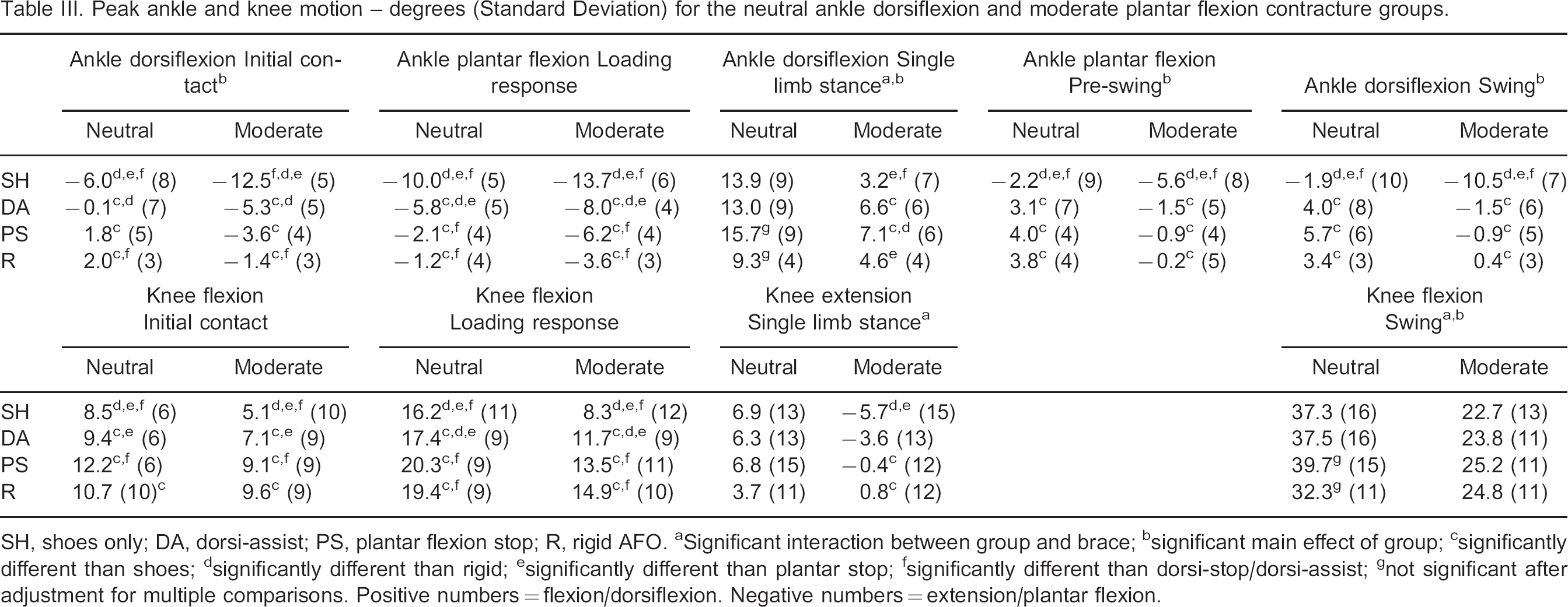
SH, shoes only; DA, dorsi-assist; PS, plantar flexion stop; R, rigid AFO.
Significant interaction between group and brace
significant main effect of group
significantly different than shoes
significantly different than rigid
significantly different than plantar stop
significantly different than dorsi-stop/dorsi-assist
not significant after adjustment for multiple comparisons. Positive numbers = flexion/dorsiflexion. Negative numbers = extension/plantar flexion
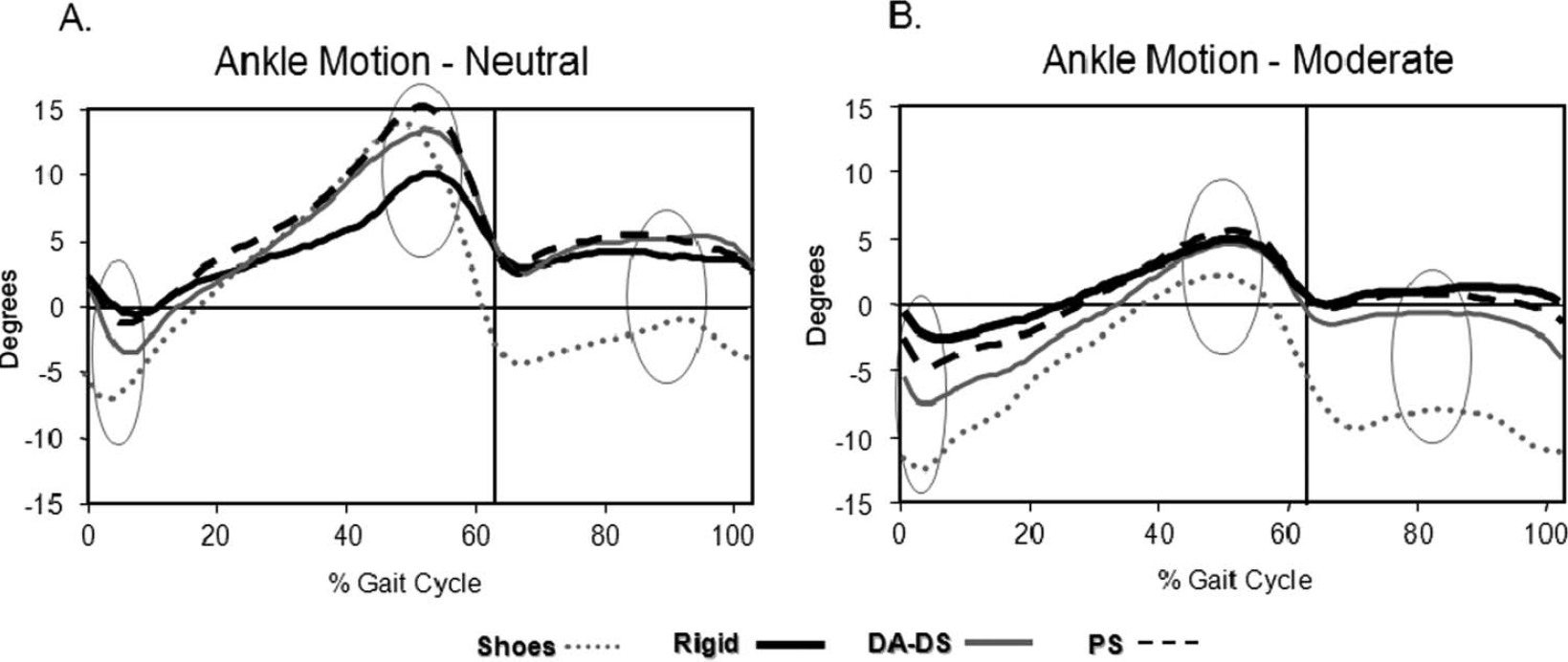
Mean ankle motion curves for the Neutral (A) and Moderate contracture (B) groups. Positive values = dorsiflexion and negative values = plantar flexion. Shoes only curves are depicted with grey dotted line, Rigid AFO curves in solid black line, DA-DS AFO curves in solid grey line, and PS AFO curves in dashed black line. The vertical lines indicate the end of stance and beginning of swing. Ankle dorsiflexion in mid swing, initial contact, and loading response was increased in all three AFOs compared to shoes only in both groups. Ankle dorsiflexion in terminal stance was greater in the PS AFO than in both shoes only and Rigid AFO in the moderate contracture group (B). For the neutral group ankle dorsiflexion in terminal stance was greater in the PS AFO than in the Rigid AFO (A).
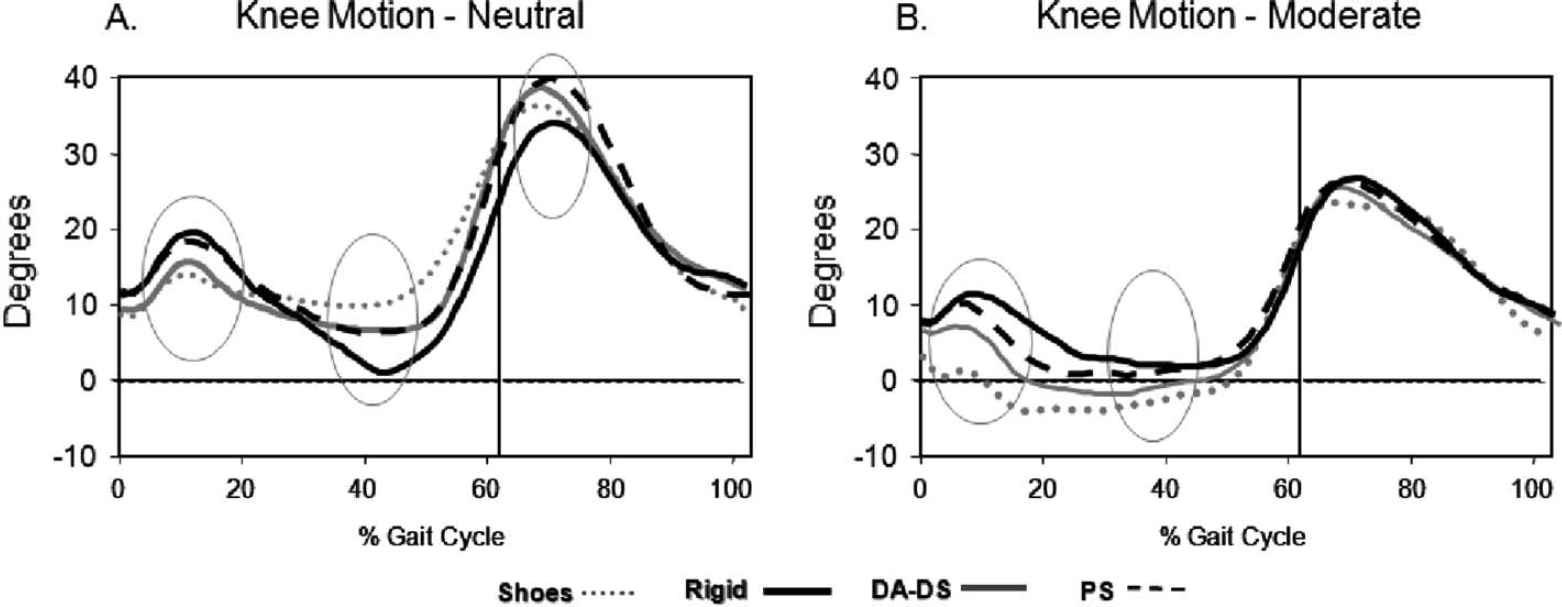
Mean external knee motion curves for the Neutral (A) and Moderate contracture (B) groups. Positive values = flexion and negative values = extension. Shoes only curves are depicted with grey dotted line, Rigid AFO curves in solid black line, DA-DS AFO curves in solid grey line, and PS AFO curves in dashed black line. The vertical lines indicate the end of stance and beginning of swing. Knee flexion flexion at initial contact and loading response was greatest in the Rigid and PS AFO, intermediate in the DA-DS AFO, and lowest in shoes only in both contracture groups. Knee extension in terminal stance was greater in shoes only than in both the PS AFO and Rigid AFO in the moderate contracture group (B). For the neutral dorsiflexion group knee flexion in swing was greater in the PS AFO than in the Rigid AFO (A).
Peak knee flexion in swing was reduced in the Rigid AFO compared to the PS AFO (32.3 vs. 39.7°), but this did not reach statistical significance after adjustment for multiple comparisons.
Moments
Moments at the ankle were affected by AFO condition, but not by ankle mobility. For participants in both groups ankle plantar flexion moments at loading response were greater
in all three AFO conditions compared with shoes (Table IV, Figure 4). The greatest plantar flexion moment occurred in the Rigid AFO for both groups. At terminal stance the PS AFO resulted in a significantly greater DF moment than the Rigid AFO and shoe conditions for both groups.
At the knee the flexion moment in loading response was greater in the neutral group than in the moderate contracture group for all AFO conditions (Table IV, Figure 5). The Rigid AFO resulted in a significantly greater knee flexion moment in loading than the shoe condition for both contracture groups. There was a significant interaction between the effects of contracture group and AFO condition for the peak knee extension moment in stance. For the moderate contracture group only, the Rigid AFO resulted in a lower peak knee extension moment in stance than in both PS AFO and shoes only conditions (— 0.11 vs. −0.24 and −0.29 Nm/kgm).
Peak ankle and knee moments - Nm/kgm (Standard Deviation) for the neutral ankle dorsiflexion and moderate plantar flexion contracture groups.

SH, shoes only; DA, dorsi-assist; PS, plantar flexion stop; R, rigid AFO.
Significant interaction between group and brace
significant main effect of group
significantly different than shoes
significantly different than rigid
significantly different than plantar stop
significantly different than dorsi-stop/dorsi-assist. Positive numbers = flexion/dorsiflexion. Negative numbers = extension/plantar flexion.
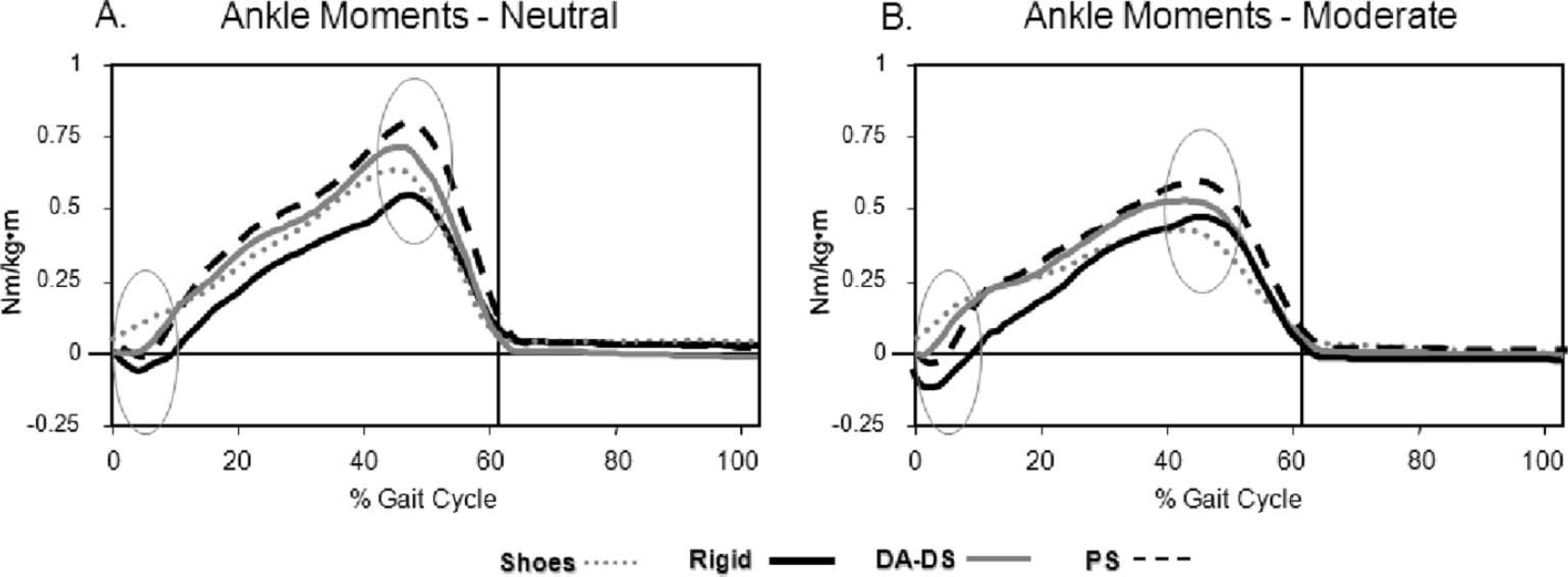
Mean external ankle moment curves for the Neutral (A) and Moderate contracture (B) groups. Positive values = dorsiflexion and negative values = plantar flexion. Shoes only curves are depicted with grey dotted line, Rigid AFO curves in solid black line, DA-DS AFO curves in solid grey line, and PS AFO curves in dashed black line. The vertical lines indicate the end of stance and beginning of swing. Ankle plantar flexion moment in loading was greatest in the Rigid, intermediate in the PS and DA-DS AFOs, and lowest in shoes only in both contracture groups. Ankle dorsiflexion moment in terminal stance was greater in the PS AFO than in both shoes only and Rigid AFO in both groups.
EMG
There were no differences between the neutral and moderate contracture groups in EMG intensity of the three muscles studied. For both groups, walking in the PS orthosis produced greater soleus EMG activity compared to the DA-DS orthosis (48.0 vs. 30.4% max for the neutral group and 27.4 vs. 19.1% max for the moderate contracture group). Additionally, EMG intensity in AT was lower in the PS AFO compared to the shoes only and DA-DS conditions (8.5 vs. 14.2 and 14.5% max averaged across groups) (Table V). VI EMG intensity was not different between groups or AFO conditions.
Discussion
In this study, walking with an AFO had a minimal impact on self-selected gait speed compared to walking without an orthosis in individuals with hemiparesis after stroke. For
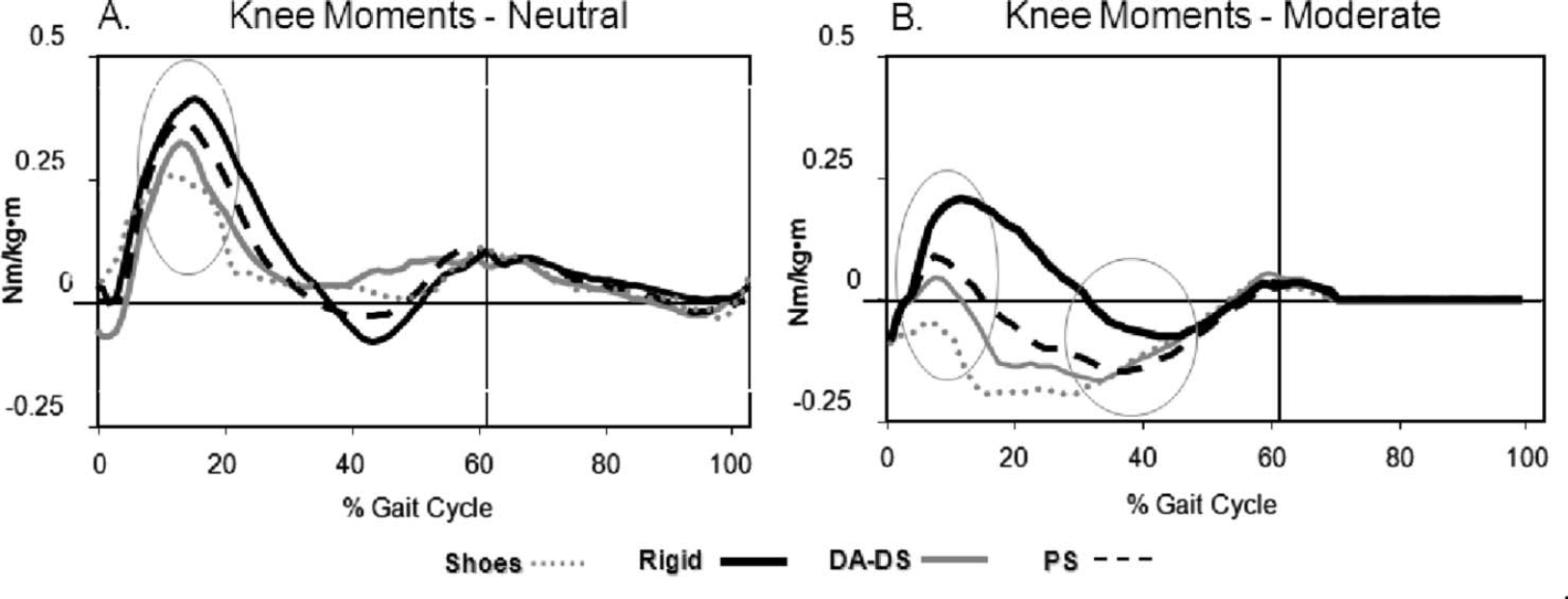
Mean external knee moment curves for the Neutral (A) and Moderate contracture (B) groups. Positive values = flexion and negative values = extension. Shoes only curves are depicted with grey dotted line, Rigid AFO curves in solid black line, DA-DS AFO curves in solid grey line, and PS AFO curves in dashed black line. The vertical lines indicate the end of stance and beginning of swing. Knee flexion moment in loading response was greater in the Rigid AFO than in shoes only in both groups. Knee extension moment in terminal stance was greater in shoes only and the PS AFO than in the Rigid AFO in the moderate contracture group only.
Mean electromyographic(EMG) activity for vastus intermedius (VI), soleus (SOL), and anterior tibialis (AT) muscles - % of max MMT (Standard Deviation) for the neutral ankle dorsiflexion and moderate plantar flexion contracture groups.

SH, shoes only; DA, dorsi-assist; PS, plantar flexion stop; R, rigid AFO.
Significantly different than shoes
significantly different than plantar stop
significantly different than dorsi-stop/dorsi-assist. Positive numbers = flexion/dorsiflexion. Negative numbers = extension/plantar flexion.
Conclusion
An individual's passive range of ankle joint motion is an important consideration for selection of the most appropriate AFO design after stroke. Both rigid and articulating AFO designs improved ankle flexion in swing and initial contact regardless of passive ankle mobility, though only the PS AFO diminished AT activity. The restriction of plantar flexion in loading by both the PS and Rigid AFOs increased knee flexion motion, but only the Rigid orthosis increased the knee flexion moments. Consequently, individuals with quadriceps weakness may more easily tolerate an AFO with plantar flexion mobility in loading. Overall, the Rigid AFO impeded walking ability for participants with normal ankle range of motion. Both ankle dorsiflexion in stance and knee flexion in swing were restricted in the Rigid AFO and walking speed was reduced. The PS and Rigid AFOs corrected knee hyperextension in participants with a moderate ankle plantar flexion contracture. The PS AFO permitted the largest excursion of dorsiflexion in stance, but also elicited increased soleus EMG regardless of contracture status. This may be an important factor in level of daily activity and fatigue. The DA-DS AFO was intermediate in its effect on walking, providing some restraint of the tibia in
single limb support that encouraged tibial advancement while stabilizing the tibia in a position of moderate dorsiflexion. Future studies are needed to identify the impact of AFO design on endurance and daily activities.
Acknowledgements
The authors wish to acknowledge Leslie Schein, DPT, for her assistance with data analysis. This study was funded by the National Institute of Disability and Rehabilitation Research grant #H133G000004.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.