
Abstract
Stigma is often nominated as a central concern for people with mental disorders [1,2]. Stigmatizing attitudes may inhibit help seeking, may compound the experience of psychological distress and may also adversely affect personal relationships and the ability to achieve educational and vocational goals [3–5]. In spite of recent progress in the development of evidence-based treatments and increased public knowledge about mental disorders, many people report direct experiences of stigma and discrimination and it remains a significant issue [6,7].
Studies from a number of countries have examined stigmatizing attitudes towards people with mental disorders, including participants' beliefs about those with the disorders (known as personal or, alternatively, public stigma) [8,9], participants beliefs about the attitudes of others (perceived stigma) [10], or a desire for social distance [11]. In Australia, such studies include the 2003–2004 National Survey of Mental Health Literacy in the adult population, in which stigmatizing attitudes were examined towards a person described in one of four vignettes: depression, depression with suicidal thoughts, early schizophrenia and chronic schizophrenia [12]. Consistent with survey findings from other countries, the results showed that Australians were more likely to endorse stigmatizing statements about schizophrenia, particularly the items concerning dangerousness and unpredictability, a desire for social distance and the perception that the person would be discriminated against [13].
As such research has tended to focus on mental illness broadly, or specifically on depression and schizophrenia, relatively little is known about stigmatizing attitudes towards anxiety disorders, despite their high prevalence rates [14]. As evidence suggests that it is not appropriate to generalize stigmatizing attitudes about depression or schizophrenia to anxiety disorders, there is a need to explore specific attitudes to these disorders [15,16]. Moreover, stigma is a multidimensional construct, the various aspects of which may operate differently according to circumstances such as age, gender and culture [10,17,18]. There is a need to explore various aspects of stigma in relation to a range of mental disorders in order to better understand how to target stigma reduction interventions. The aim of the study was to carry out a national survey in order to assess stigmatizing attitudes towards depression, anxiety disorders and schizophrenia/psychosis.
Methods
The survey involved computer-assisted telephone interviews (CATI) with a national sample of 6019 members of the general community aged 15 +. The survey was carried out by the survey company Social Research Centre (Melbourne, Victoria). The sample was contacted by random-digit dialling of both landlines and mobile phones covering the whole country from January to May 2011. Further details of the methods are given in an accompanying paper [19].
Survey interview
The interview was based on a vignette of a person with a mental disorder. On a random basis, respondents were read one of six vignettes: depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and post-traumatic stress disorder (PTSD). Respondents were also randomly assigned to receive either male (‘John’) or female (‘Jenny’) versions of the vignette. All vignettes were written to satisfy the diagnostic criteria for either major depression or schizophrenia according to DSM-IV and ICD-10. The first four vignettes have been published previously [20] and the latter two, which were used for the first time, are given elsewhere [19].
After being presented with the vignette, respondents were asked what, if anything, they thought was wrong with the person described in the vignette and a series of questions about the likely helpfulness of a wide range of interventions, their health, knowledge of causes and risk factors and contact with people like those in the vignette. Data relating to these questions is reported elsewhere [19]. The focus of this paper is respondents' beliefs about the stigma and discrimination associated with mental disorders.
Personal and perceived stigma
Stigmatizing attitudes were assessed with two sets of statements, one assessing the respondent's personal attitudes towards the person described in the vignette (personal stigma) and the other assessing the respondent's beliefs about other people's attitudes towards the person in the vignette (perceived stigma) [9]. The personal stigma items were: (i) People with a problem like John/Jenny's could snap out of it if they wanted, (ii) A problem like John/Jenny's is a sign of personal weakness, (iii) John/Jenny's problem is not a real medical illness, (iv) People with a problem like John/Jenny's are dangerous, (v) It is best to avoid people with a problem like John/Jenny's so that you don't develop this problem, (vi) People with a problem like John/Jenny's are unpredictable, (vii) If I had a problem like John/Jenny's I would not tell anyone, (viii) I would not employ someone if I knew they had a problem like John/Jenny's, (ix) I would not vote for a politician if I knew they had suffered a problem like John/Jenny's.
The perceived stigma items covered the same statements but started with ‘Most other people believe that…’ Ratings of each were made on a 5-point Likert scale ranging from strongly agree to strongly disagree. For these analyses the agree and strongly agree categories were combined.
Social distance
Self-reported willingness to have contact with the person described in the vignette was measured using the 5-item scale developed by Link et al. [21]. The items rated the person's willingness to (i) move next door to John/Jenny, (ii) spend an evening socializing with John/Jenny, (iii) make friends with John/Jenny, (iv) work closely with John/Jenny on a job, (v) have John/Jenny marry into their family. Each item was rated on a 4-point scale ranging from definitely willing to definitely unwilling. For these analyses the definitely unwilling and probably unwilling categories were combined.
Perceived discrimination
Perceived discrimination was examined by asking if respondents thought the person in the vignette was likely to be discriminated against by others in the community. Possible responses were ‘yes’, ‘no’ and ‘I don't know’.
Statistical analysis
The data were analysed using percentage frequencies and 95% confidence intervals. A pre-weight was applied to adjust for the dual frame design and the respondent chance of selection. The achieved sample was close to the Australian national population in terms of geographic distribution; however, there was an under-representation of men and of younger adults, and an over-representation of university educated people and people with an English-speaking background. A population weight was used to adjust for these biases. Differences between percentage frequencies could be considered statistically significant if there is no overlap between the 95% confidence intervals for the relevant percentages. With n = 1000 per vignette, a percentage difference of 5% is always statistically significant at the p < 0.05 level.
Design-based chi-square analyses (or the F statistic in the case of continuous variables) were used to examine the differences in attitudes according to the gender of the person described in the vignette. All analyses were performed using Intercooled Stata 10 (StataCorp, TX).
Results
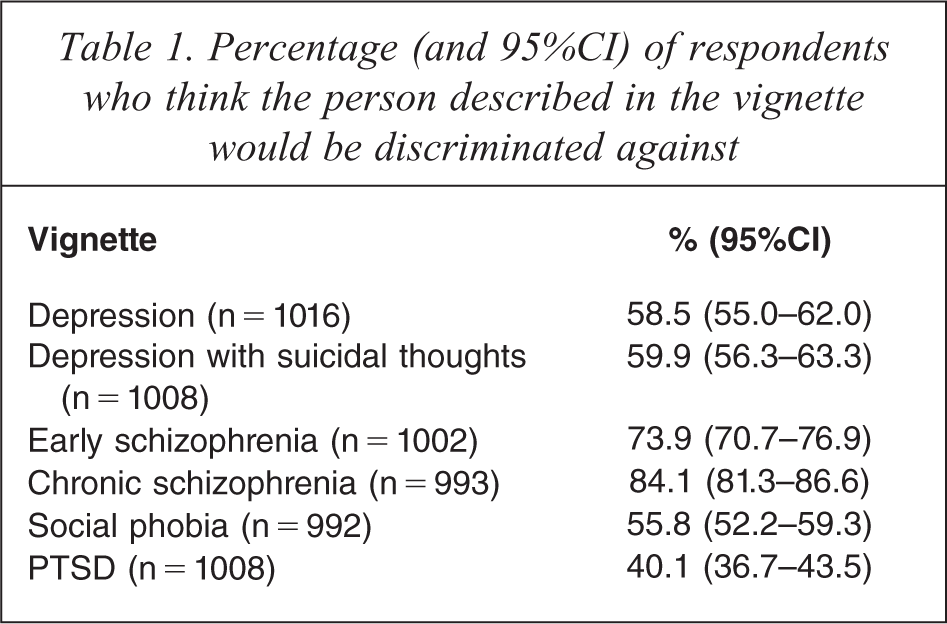
When asked if the person described in the vignette was likely to be discriminated against, between 40.1% (PTSD vignette) and 84.1% (chronic schizophrenia vignette) thought this was likely to be the case (see Table 1). When beliefs about discrimination were analysed according to the gender of the person described in the vignette, there were no significant differences.
Percentage (and 95%CI) of respondents who think the person described in the vignette would be discriminated against
Personal stigma
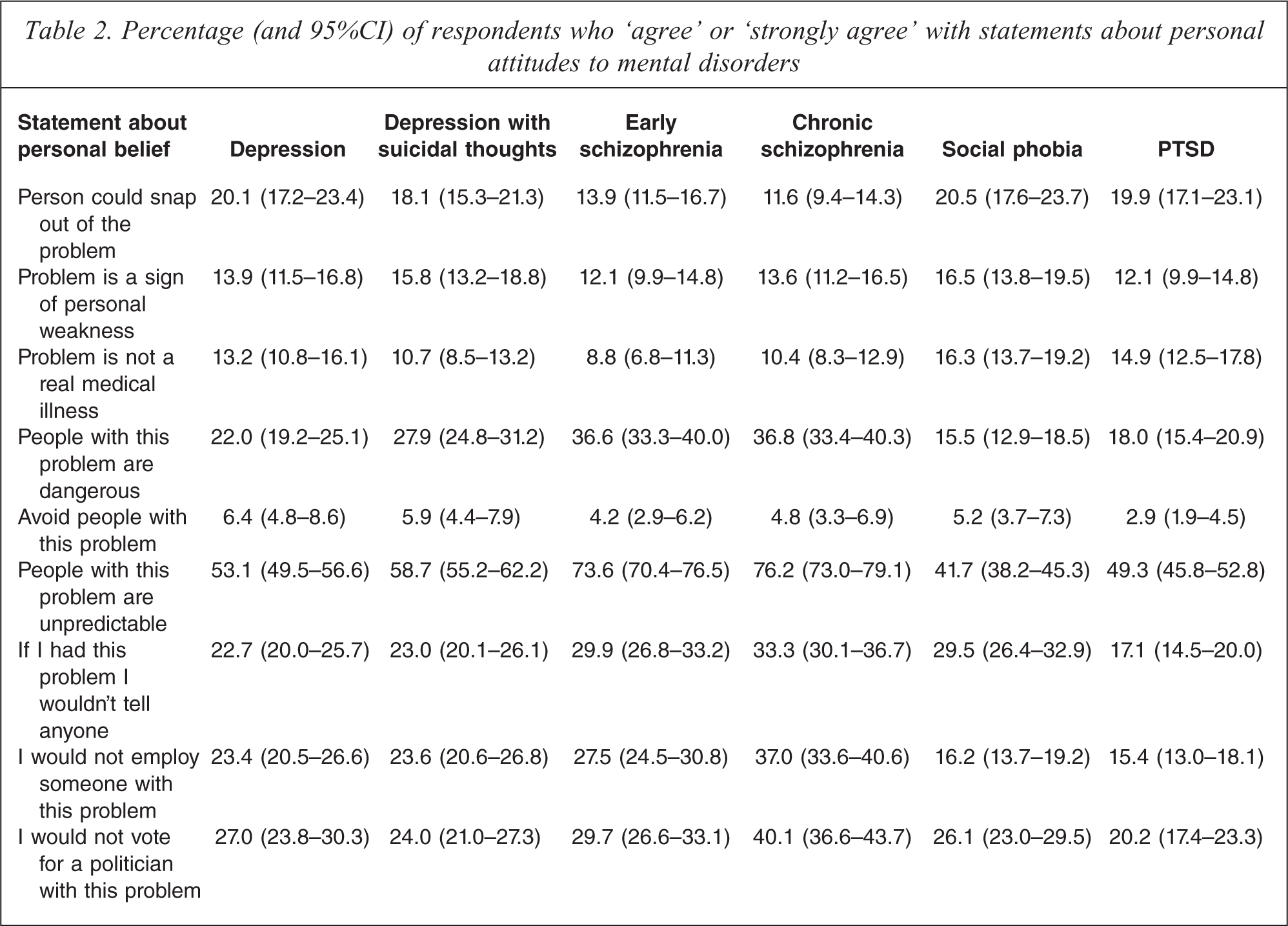
Respondents' personal agreement with statements reflecting attitudes to those with mental illness are given in Table 2, which shows that avoiding the person was the statement with which respondents were least likely to agree. This applied to all vignettes. ‘People with this problem are unpredictable’ was the statement with which respondents were most likely to agree. This was particularly notable for the schizophrenia vignettes with approximately 70% of people agreeing or strongly agreeing with the statement. Endorsement of personal stigma items relating to dangerousness, unpredictability, not employing someone with the problem and not voting for a politician with the problem was generally highest for the chronic schizophrenia vignette, while beliefs in the problem as a sign of personal weakness or ‘not a real medical illness’ were generally higher for social phobia than for other disorders. Willingness to disclose was highest for PTSD (17.1%) and lowest for chronic schizophrenia (33.3%).
Percentage (and 95%CI) of respondents who ‘agree’ or ‘strongly agree’ with statements about personal attitudes to mental disorders
When personal attitudes were analysed according to the gender of the person described in the vignette, for the depression vignette, men were more likely to be seen as dangerous (men: 25.7% (95%CI 21.7–30.3), women: 18.2% (95%CI 14.5–22.6), p = 0.013). This was also the case for the early schizophrenia vignette (men: 40.1% (95%CI 35.4–45.1), women: 33.2% (95%CI 28.7–38.0), p = 0.043). For the chronic schizophrenia vignette, men were more likely to be seen as best avoided (men: 7.0% (95%CI 4.5–10.8), women: 2.6% (95%CI 1.5–4.6), p = 0.006). For the social phobia vignette, men were more likely to be seen as best avoided (men: 7.1% (95%CI 4.6–10.8), women: 3.4% (95%CI 2.0–5.7), p = 0.029), unpredictable (men: 45.9% (95%CI 40.9–51.0), women: 37.6% (95%CI 32.8–42.7), p = 0.023) and not to be employed (men: 19.9% (95%CI 16.0–24.6), women: 12.7% (95%CI 9.7–16.4), p = 0.014). For the PTSD vignette, men were more likely to be seen as dangerous (men: 21.4% (95%CI 17.5–25.8), women: 14.8% (95%CI 11.4–18.9), p = 0.021) and unpredictable (men: 53.5% (95%CI 48.5–58.5), women: 45.2% (95%CI 40.3–50.2), p = 0.021).
Perceived stigma
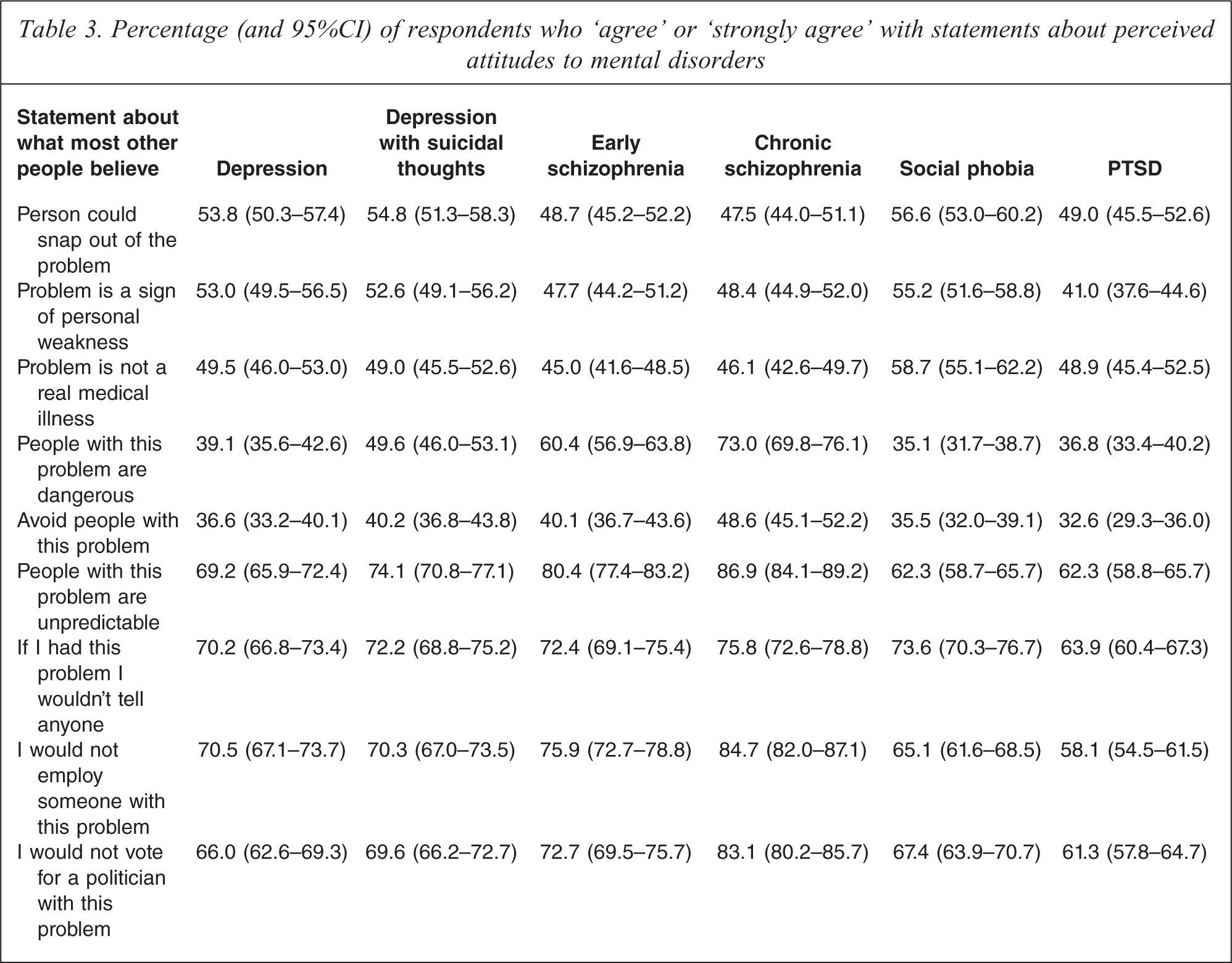
Respondents' personal agreement with statements reflecting perceived attitudes to those with mental illness are given in Table 3. Perceived stigma items received much higher rates of agreement than personal stigma items. For all vignettes, respondents were most likely to agree or strongly agree with the statements about other people's belief in unpredictability, the belief that most other people would not tell anyone and the belief that most other people would not employ someone with the problem. As with personal stigma, endorsement of perceived stigma items relating to dangerousness, unpredictability, not employing someone with the problem and not voting for a politician with the problem was generally highest for the chronic schizophrenia vignette, while beliefs in the problem as a sign of personal weakness or ‘not a real medical illness’ were generally highest for social phobia.
Percentage (and 95%CI) of respondents who ‘agree’ or ‘strongly agree’ with statements about perceived attitudes to mental disorders
When perceived attitudes were analysed according to the gender of the person described in the vignette, for the depression vignette, men were more likely to be seen as best avoided (men: 41.1% (95%CI 36.3–46.2), women: 32.0% (95%CI 27.5–36.9), p = 0.009) and not to be employed (men: 73.9% (95%CI 69.3–78.0), women: 67.1% (95%CI 62.0–71.8), p = 0.041). For the depression with suicidal thoughts vignette, men were more likely to be seen as dangerous (men: 54.5% (95%CI 49.5–59.4), women: 44.7% (95%CI 39.8–49.8), p = 0.007) and not to be voted for as a politician (men: 74.2% (95%CI 69.5–78.4), women: 65.1% (95%CI 60.2–69.6), p = 0.006). For the early schizophrenia vignette, men were more likely to be seen as dangerous (men: 64.1% (95%CI 59.1–68.7), women: 56.8% (95%CI 51.8–61.6), p = 0.038) and not to be employed (men: 79.4% (95%CI 75.1–83.1), women: 72.5% (95%CI 67.8–76.7), p = 0.024). For the social phobia vignette, men were less likely to be seen as being able to snap out of the problem (men: 53.0% (95%CI 47.8–58.0), women: 60.2% (95%CI 55.2–65.1), p = 0.046) and more likely to be seen dangerous (men: 41.4% (95%CI 36.4–46.5), women: 29.0% (95%CI 24.6–33.9), p = 0.001). For the PTSD vignette, men were more likely to be seen as dangerous (men: 44.0% (95%CI 39.1–49.0), women: 29.9% (95%CI 25.5–34.7), p = 0.001), best avoided (men: 36.0% (95%CI 31.3–41.0), women: 29.3% (95%CI 25.0–34.0), p = 0.048), unpredictable (men: 68.8% (95%CI 63.9–73.3), women: 56.1% (95%CI 51.1–60.9), p = 0.0003), not to be employed (men: 62.5% (95%CI 57.5–67.3), women: 53.8% (95%CI 48.8–58.7), p = 0.015) and not to be voted for as a politician (men: 66.0% (95%CI 61.0–70.6), women: 56.9% (95%CI 51.9–61.8), p = 0.0108).
Social distance
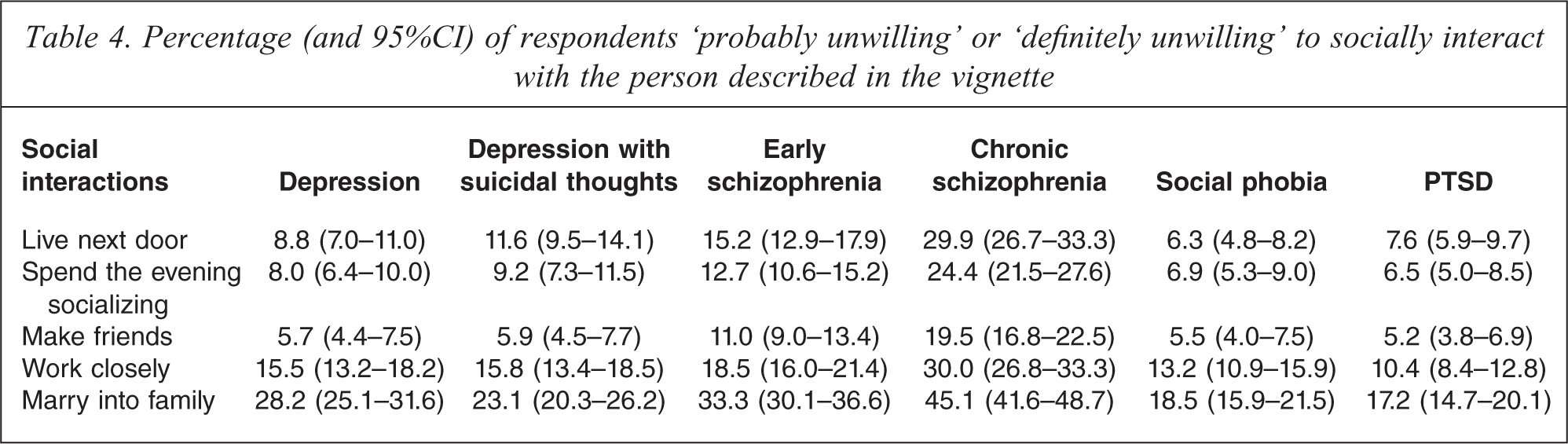
Table 4 shows the percentage of respondents who were either ‘probably unwilling’ or ‘definitely unwilling’ to interact socially with the person described in the vignette. For each vignette, respondents were most unwilling to work closely with or marry into the family of someone with a mental disorder, while a desire for social distance was least likely for ‘making friends’.
Percentage (and 95%CI) of respondents ‘probably unwilling’ or ‘definitely unwilling’ to socially interact with the person described in the vignette
When desire for social distance was analysed according to the gender of the person described in the vignette, for the depression vignette, desire for men not to marry into the family was higher than for women (men: 32.2% (95%CI 27.7–37.1), women: 24.2% (95%CI 20.1–28.9), p = 0.032). For the depression with suicidal thoughts vignette, unwillingness to spend the evening socializing was higher for men (men: 11.4% (95%CI 8.5–15.0), women: 7.0% (95%CI 4.8–10.1), p = 0.003) as was desire not to have the person marry into the family (men: 28.5% (95%CI 24.3–33.2), women: 17.8% (95%CI 14.4–22.0), p = 0.0002). For the early schizophrenia vignette, desire for men not to marry into the family was higher (men: 38.1% (95%CI 33.4–43.0), women: 28.7% (95%CI 24.5–33.3), p = 0.015). This was also the case for the chronic schizophrenia vignette (men: 51.0% (95%CI 45.9–56.0), women: 39.2% (95%CI 34.4–44.2), p = 0.003) and the social phobia vignette (men: 22.3% (95%CI 18.3–26.9), women: 14.9% (95%CI 11.6–18.9), p = 0.004). For the PTSD vignette, the desire not to live next door to someone was higher for men (men: 10.2% (95%CI 7.5–13.6), women: 5.2% (95%CI 3.4–7.9), p = 0.023) as was desire for the person not to marry into the family (men: 23.3% (95%CI 19.3–27.8), women: 11.4% (95%CI 8.6–15.1), p = 0.0001).
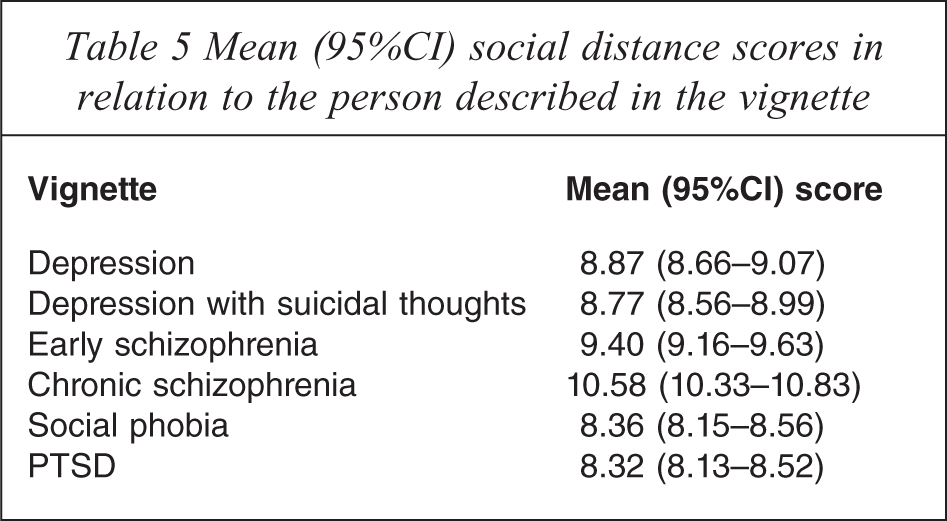
Table 5 gives the mean social distance scores. Desire for social distance was greatest for the chronic schizophrenia vignette and lowest for the social phobia and PTSD vignettes. Scores across the following vignettes were significantly greater for men: depression (men: 9.21 (95%CI 8.92–9.51), women: 8.51 (95%CI 8.23–8.80), p = 0.001), depression with suicidal thoughts (men: 9.11 (95%CI 8.81–9.43), women: 8.44 (95%CI 8.15–8.72), p = 0.002), chronic schizophrenia (men: 10.88 (95%CI 10.51–11.25), women: 10.27 (95%CI 9.93–10.62) p = 0.019) and PTSD (men: 8.74 (95%CI 8.21–8.81), women: 7.92 (95%CI 7.67–8.18) p = 0.000).
Mean (95%CI) social distance scores in relation to the person described in the vignette
Discussion
A 2011 survey of mental health literacy and stigma in 6019 Australians aged 15 + showed that perceptions of discrimination, social distance, dangerousness and unpredictability were generally highest for chronic schizophrenia, while beliefs in the problem as a sign of personal weakness or ‘not a real medical illness’ were generally higher for social phobia than for other disorders. For both personal and perceived stigma, across all vignettes, the statements with which respondents were most likely to agree or strongly agree involved beliefs about unpredictability, not telling anyone and not employing someone with the problem. Current findings are also in keeping with those of other studies that report higher levels of stigmatizing attitudes towards schizophrenia than those of other disorders [12,22,23].
Most previous studies of stigmatizing attitudes towards mental illness have focused on depression or schizophrenia. The inclusion of anxiety disorder vignettes allowed for an exploration of how different aspects of stigma might vary according to disorder. Results of the current study showed that patterns of agreement with different statements varied according to disorder, highlighting the multidimensional nature of stigma. Beliefs in the problem as a sign of personal weakness or ‘not a real medical illness’ were generally higher for social phobia than for other disorders, while beliefs in dangerousness and unpredictability were notably higher for the schizophrenia vignettes. This may partly reflect that fact that social phobia is less often identified as a mental disorder and is therefore less likely to be associated with some types of stigmatizing attitudes [19,24]. Because it would be rare for a respondent to have had personal experience of violence involving a person with schizophrenia, it is likely that media reports associating violence with schizophrenia contribute to perceptions of dangerousness [25,26].
As far as the authors are aware, the current survey is the first population-level survey to assess stigmatizing attitudes towards PTSD. This is of significance as relatively few studies have assessed stigma in relation to anxiety disorders [15,27,28]. Findings from the current study indicating lower levels of stigmatizing attitudes towards PTSD than to other mental disorders are consistent with those of other smaller studies, including a South African study assessing community attitudes to a range of mental disorders [28] and a study involving Croatian adolescents [27]. It is possible that attributing a disorder to an external cause, such as that described in the vignette, makes it less likely that it be seen as a character problem or source of shame.
As with previous studies of stigmatizing attitudes, questionnaire items assessing perceived stigma received much higher endorsement than those assessing personal stigma [9,12]. A social desirability effect may have contributed to this finding, although it is unlikely that a desire not be judged by an anonymous telephone interviewer fully explains the large differences. The discrepancy could be an example of what social psychologists have called ‘pluralistic ignorance’, where most people erroneously perceive that they have different attitudes to the majority. It is possible that increasing awareness of the issue of stigma in the community has contributed to the over-estimation of prevalence of stigmatizing beliefs. This is supported by reports of an increase in the belief that a person with depression would be discriminated against, particularly in those Australian states with greatest exposure to campaigns run by beyondblue: the national depression initiative [29]. These results suggest that stigma reduction campaigns should focus on bringing beliefs about public perceptions in line with personal beliefs. Such an approach has been used in other areas, including the use of social norms interventions to curb problem drinking [30].
When stigmatizing attitudes were compared according to whether the person described in the vignette was male or female, some significant differences emerged, with men generally more likely to be seen as dangerous. Desire for social distance was also generally significantly higher for men, possibly due to perceptions of dangerousness. This is consistent with other reported studies [31,32]. However, the differences in perceptions of dangerousness were less likely to be significant for more severe disorders, perhaps indicating that views of dangerousness of more severe disorders outweigh any perceptions of gender differences.
Limitations
Survey limitations include the self-report nature of the data and the fact that responses may be affected by a social desirability bias. In addition, the original items in the scales were developed for use in evaluating depression stigma and they may not be optimal for assessing stigmatizing attitudes to other disorders. In this study, stigmatizing attitudes were assessed in relation to an unknown person described in a vignette. It is unclear how such beliefs might differ in cases where the person with the disorder is known to the respondent. It is also not clear whether such attitudes translate into behaviour and there is a need for further research into the links between attitudes and behaviours towards people with mental disorders.
Conclusions
Results of a national survey of stigmatizing attitudes towards those with depression, schizophrenia and anxiety disorders show that patterns of stigmatizing attitudes differ according to disorder, with differences between schizophrenia and social phobia being particularly striking. This suggests that anti-stigma interventions are more likely to be successful if they focus on individual disorders rather than on ‘mental illness’ in general. Such interventions may need to focus on perceptions of social phobia as being due to weakness and address perceptions of dangerousness in those with more severe disorders. Such interventions should also focus on bringing beliefs about public perceptions in line with personal beliefs as the latter are much less stigmatizing.