
Abstract
Stigmatizing attitudes towards people with mental disorders are common in adolescents and can lead to negative feelings, stereotyping and discriminatory behaviours [1,2]. Moreover, it is likely that someone with a mental disorder will internalize the stigma, leading to lowered self-esteem and a sense of hopelessness [3]. Stigma is an issue of major concern to young people with mental disorders, not least due to the fact that adolescence is a time when relationships with peers assume great significance [1,4]. Several studies have shown that stigmatizing attitudes can act as barriers to help seeking, interfere with treatment and adversely affect quality of life, as they may contribute to feelings of abnormality, social disconnection and dependency on others [5–7].
Exploration of stigmatizing attitudes in young people is of critical importance due to indications that, despite adolescence being the period of peak onset of mental disorders, help-seeking rates remain lower than those in other age groups [8,9]. Some studies have examined young people's stigmatizing attitudes towards people with mental disorders, including beliefs about those with the disorders (known as personal or, alternatively, public stigma) [10,11], participants' beliefs about the attitudes of others (perceived stigma) [10,12], or a desire for social distance [13]. In Australia, such studies include the 2006 national survey of mental health literacy in young people, in which stigmatizing attitudes were examined towards a person described in one of four vignettes: depression, depression with alcohol misuse, social phobia and psychosis/schizophrenia [14]. Consistent with survey findings from other countries, the results showed that young Australians were more likely to endorse stigmatizing statements about psychosis/schizophrenia, particularly the items concerning dangerousness and unpredictability and a desire for social distance [15,16].
As with research on stigmatizing attitudes in adults, most research in young people has focused on mental illness broadly, or specifically on depression and psychosis/schizophrenia, and relatively little is known about young people's stigmatizing attitudes towards anxiety disorders, despite their high prevalence rates [9]. However, evidence suggests that stigmatizing attitudes vary according to type of mental illness and that there is a need to explore attitudes to different illnesses separately [14,17]. Moreover, stigma is a multidimensional construct, the various aspects of which may operate differently according to circumstances such as age, gender and culture [18–20]. There is general agreement that stigma in young people is not well understood and there is a need for further research [1,21,22]. An improved understanding of stigma at this critical time may help in the development of interventions to reduce stigma from peers and improve help seeking for those developing mental disorders. The aim of the study was to carry out a national survey of young people aged 12–25 years in order to examine stigmatizing attitudes towards those with depression, anxiety disorders and psychosis/schizophrenia.
Methods
The 2011 survey involved computer-assisted telephone interviews (CATI) with 3021 young people aged between 15 and 25. The survey was carried out by the survey company Social Research Centre. A ‘dual frame’ approach was used, with the sample contacted by random-digit dialling of both landlines and mobile phones. This approach was taken in order to minimize the potential bias of collecting data solely from households with a landline telephone connection, which may under-sample younger people, particularly young men [23]. In order to achieve a mobile/landline distribution representative of the Australian population, targets of at least 1200 mobile and 1800 landline interviews were set. Interviews were conducted between January and May 2011. Up to six calls were made to establish contact. The response rate was 47.9%, defined as completed interviews (3021) out of sample members who could be contacted and were confirmed as in scope (6306). Interviewers ascertained whether there were residents in the household within the age range and, if there were multiple, selected one for interview using the nearest birthday method. Oral consent was obtained from all respondents before commencing the interview. Respondents aged below 18 could only commence their interviews after their parents provided oral consent. This study was approved by the University of Melbourne Human Research Ethics Committee.
Survey interview
The survey interview was based on a vignette of a young person with a mental disorder. On a random basis, respondents were read one of six vignettes: depression, depression with suicidal thoughts, depression with alcohol misuse, social phobia, psychosis/schizophrenia and post-traumatic stress disorder (PTSD). Each vignette had two versions. The respondents aged 15–17 years were read a version of the vignette portraying a person aged 15 years, whereas those aged 18–25 years were read one portraying a person aged 21 years. The details of the vignettes were altered slightly to be age appropriate (e.g. reference to functioning at school versus in a course). The first five vignettes have been published previously [24] and the PTSD vignette, which was used for the first time, is given elsewhere [25].
After being presented with the vignette, respondents were asked what, if anything, they thought was wrong with the person described in the vignette and a series of questions about the likely helpfulness of a wide range of interventions, their beliefs and intentions about first aid, beliefs about prevention, exposure to mental disorders, the Kessler 6-item (K6) symptom questionnaire [26], exposure to campaigns and media items about mental health, and sociodemographic characteristics. Data relating to these latter questions is reported elsewhere [25]. The focus of this paper is on respondents' beliefs about the stigma and discrimination associated with mental disorders.
Personal and perceived stigma
Stigmatizing attitudes were assessed with two sets of statements, one assessing the respondent's personal attitudes towards the person described in the vignette (personal stigma) and the other assessing the respondent's beliefs about other people's attitudes towards the person in the vignette (perceived stigma). The items were adapted to be suitable for young people [14] based on a scale for adults [27,28]. The personal stigma items were: (i) People with a problem like (John/Jenny)'s could snap out of it if they wanted; (ii) A problem like (John/Jenny)'s is a sign of personal weakness; (iii) (John/Jenny)'s problem is not a real medical illness; (iv) People with a problem like (John/Jenny)'s are dangerous; (v) It is best to avoid people with a problem like (John/Jenny)'s so that you don't develop this problem; (vi) People with a problem like (John/Jenny)'s are unpredictable; (vii) If I had a problem like (John/Jenny)'s I would not tell anyone.
The perceived stigma items covered the same statements but started with ‘Most other people believe that…’ Ratings of each were made on a 5-point Likert scale ranging from ‘strongly agree’ to ‘strongly disagree’. For these analyses the ‘agree’ and ‘strongly agree’ categories were combined.
Social distance
Self-reported willingness to have contact with the person described in the vignette was measured by using a social distance scale suitable for young people [14] which was an adaptation of a scale developed by Link et al. for adults [29]. The items were rated the person's willingness to (i) go out with (John/Jenny) on the weekend; (ii) invite (John/Jenny) around to their house; (iii) go to (John/Jenny's) house; (iv) work closely with (John/Jenny) on a project; (v) develop a close friendship with (John/Jenny). Each item was rated on a 4-point scale ranging from definitely willing to definitely unwilling. For these analyses the ‘definitely unwilling’ and ‘probably unwilling’ categories were combined.
Statistical analysis
The data were analysed using percentage frequencies and 95% confidence intervals, using survey weights to give greater population representativeness. A pre-weight was applied to adjust for the dual frame design and the respondent chance of selection. The achieved sample was close to the Australian national population in terms of gender and geographic distribution; however, there was an under-representation of 22 to 25 year olds. A population weight was used to adjust for this bias. All analyses were performed using Intercooled Stata 10 (StataCorp, TX, USA).
Results
Overall, 1278 participants (47.6%) were contacted by mobile phone and 1743 (52.4%) by landline. The numbers assigned to each vignette were: depression, n = 506; depression with suicidal thoughts, n = 502; depression and substance abuse, n = 499, psychosis/schizophrenia, n = 501; social phobia, n = 507; and PTSD, n = 506.
Personal and perceived stigma
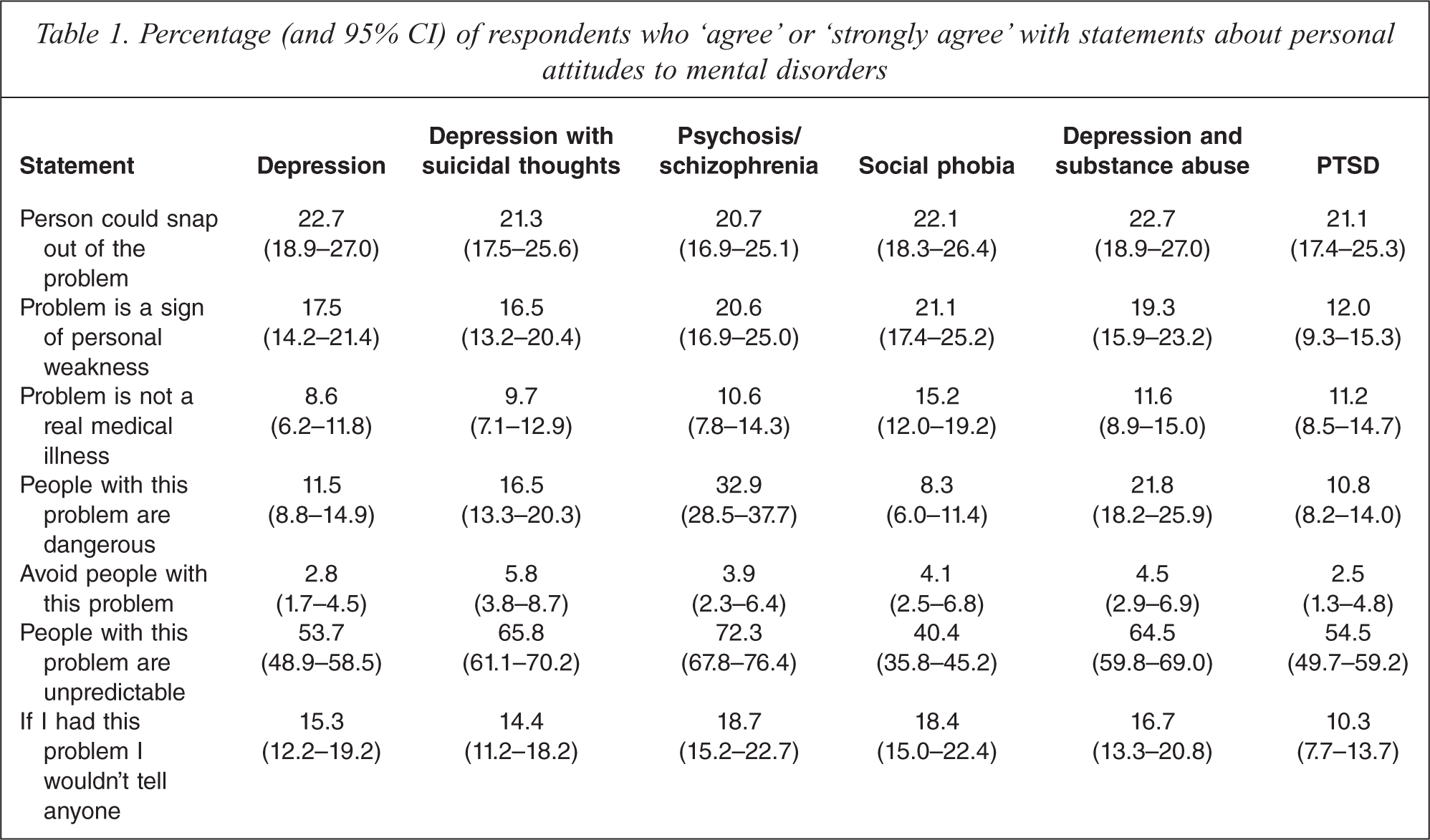
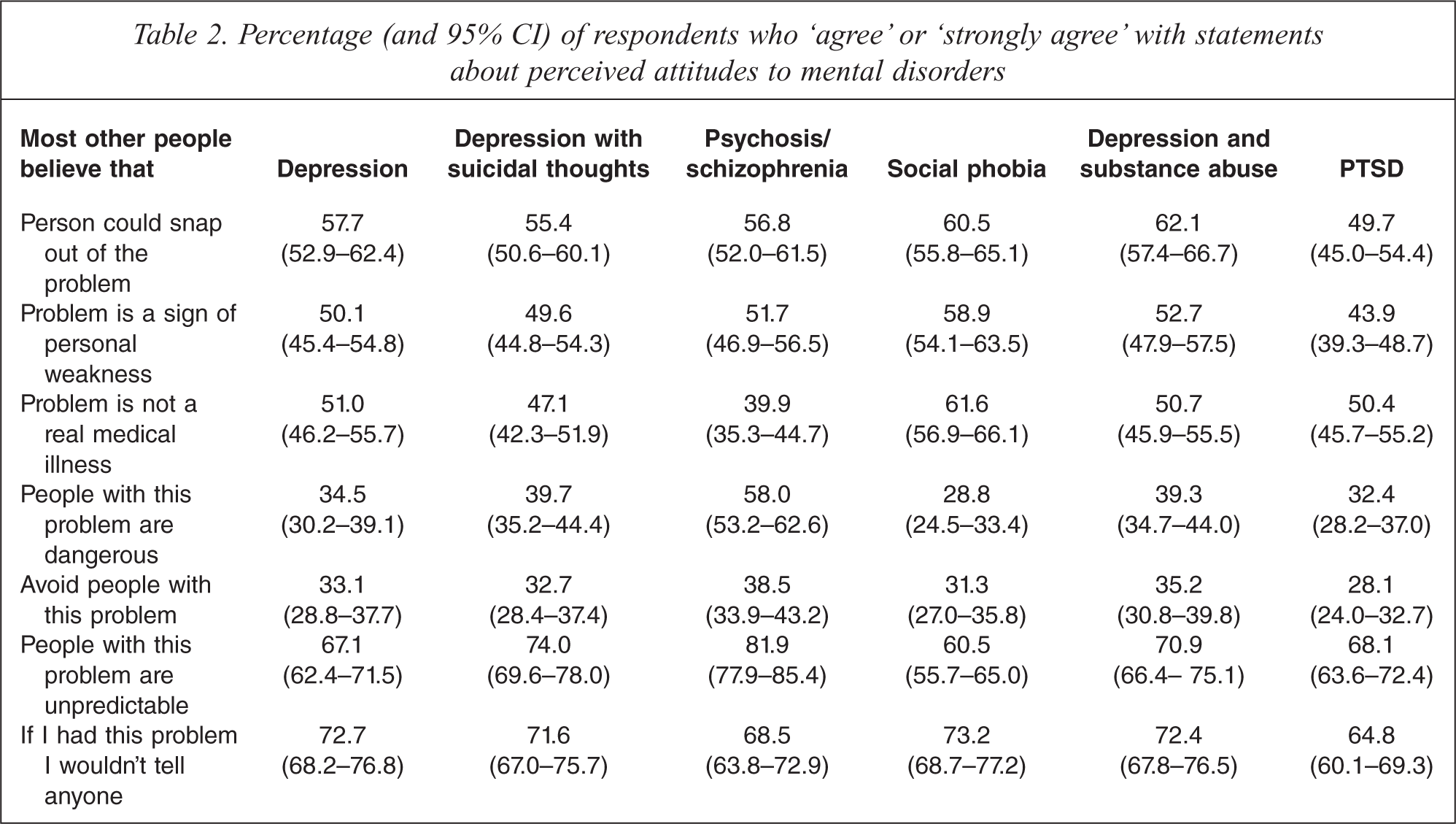
Respondents' agreement with statements reflecting attitudes to those with mental illness are given in Tables 1 and 2. Levels of agreement in Table 1 were given in response to the questions about the respondent's own beliefs (personal stigma), while those in Table 2 reflect the level of agreement with statements about what most other people believe (perceived stigma).
Percentage (and 95% CI) of respondents who ‘agree’ or ‘strongly agree’ with statements about personal attitudes to mental disorders
Percentage (and 95% CI) of respondents who ‘agree’ or ‘strongly agree’ with statements about perceived attitudes to mental disorders
For the personal stigma items, avoiding the person was the statement with which respondents were least likely to agree. This applied to all vignettes. ‘People with this problem are unpredictable’ was the statement with which respondents were most likely to agree. This was particularly notable for the psychosis/schizophrenia and depression with substance abuse vignettes. Beliefs in the problem as a sign of personal weakness or ‘not a real medical illness’ were generally higher for social phobia than for other disorders. Reluctance to disclose was greatest for the psychosis/schizophrenia or social phobia vignettes and least for the PTSD vignette.
Perceived stigma items received much higher rates of agreement than personal stigma items, although there were some differences in patterns. For example, in the case of perceived stigma, across all vignettes other than psychosis/schizophrenia, respondents were more likely to believe that the disorder was not a real mental illness than to believe that the person would be violent. In the case of personal stigma, they were more likely to believe in dangerousness for all vignettes other than social phobia and PTSD.
For all vignettes, a perception of other people's belief in unpredictability and the belief that most other people would not tell anyone were the statements with which respondents were most likely to agree or strongly agree. As with personal stigma, beliefs in the problem as a sign of personal weakness or ‘not a real medical illness’ were generally higher for social phobia than for other disorders.
Social distance
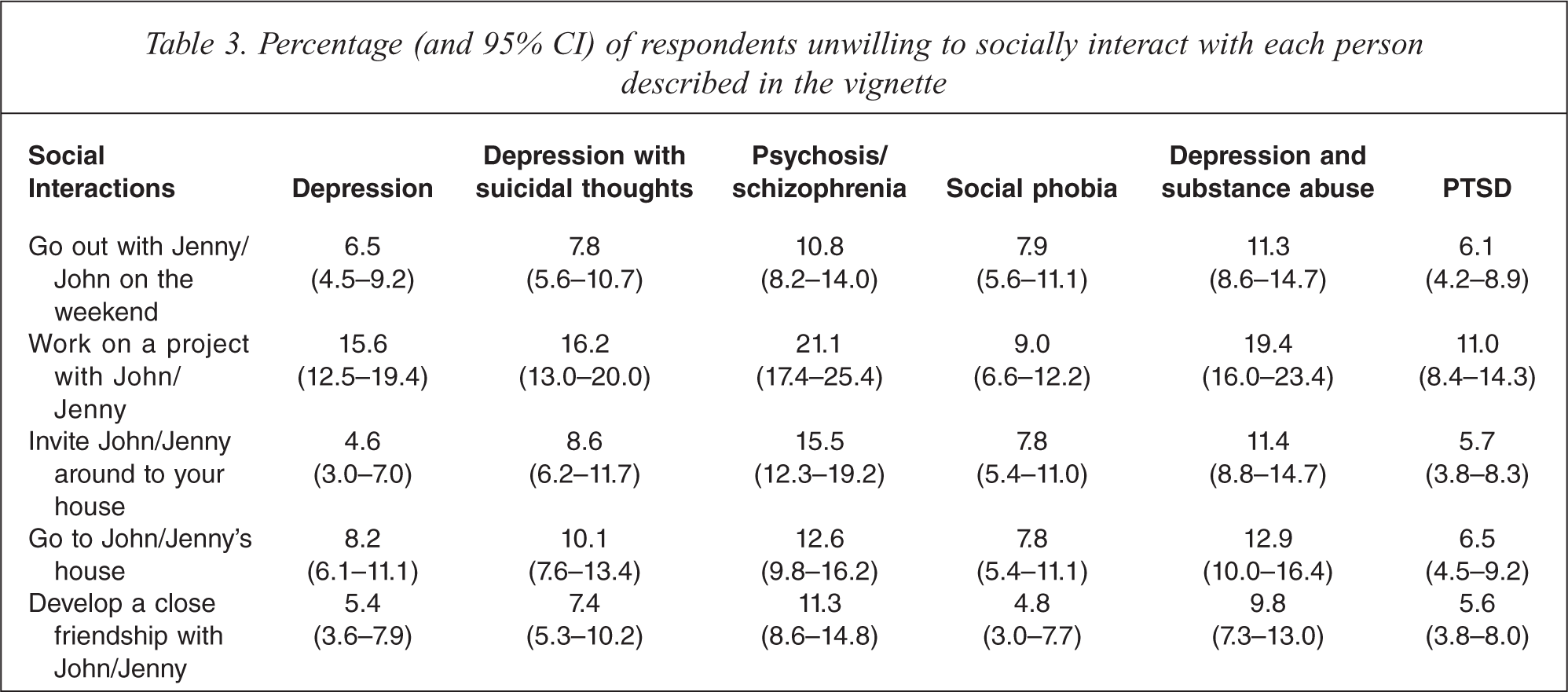
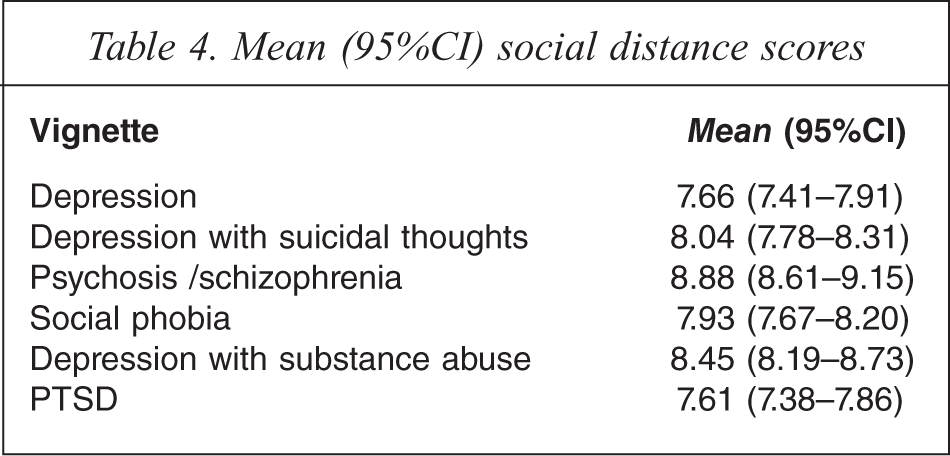
Table 3 shows the percentage of respondents who were either ‘probably unwilling’ or ‘definitely unwilling’ to interact socially with the person described in the vignette (social distance). For each vignette, respondents were most unwilling to work on a project with John or Jenny, while desire for social distance was generally lowest for developing a close friendship. Table 4 shows the total social distance scores for each vignette. Desire for social distance was greatest for the psychosis/schizophrenia vignette and lowest for the PTSD vignette.
Percentage (and 95% CI) of respondents unwilling to socially interact with each person described in the vignette
Mean (95%CI) social distance scores
Discussion
This survey showed that, for all disorders, young people aged 15–25 years were most likely to agree with statements about unpredictability and least likely to agree that they would avoid someone with the problem. Perceptions of dangerousness and unpredictability and a desire for social distance were generally higher for psychosis/schizophrenia than for other disorders, while respondents were most likely to believe that social phobia was a sign of personal weakness and not a real medical illness. The belief that the person could snap out of the problem was also relatively highly endorsed with around 20% of respondents across all vignettes personally agreeing with this statement. In terms of social interactions, young people were most unwilling to work on a project with the person described in the vignette. Current findings are also in keeping with those of other studies of young people that report higher levels of stigmatizing attitudes towards psychosis/schizophrenia than those of other disorders [14–16,30].
Most previous studies of young people's stigmatizing attitudes towards mental illness have focused on depression or psychosis/schizophrenia. While the 2006 National Survey of Mental Health Literacy in young people [14] included a social phobia vignette, as far as the authors are aware, the current survey is the first population-level survey to assess young people's stigmatizing attitudes towards PTSD. This is of significance as relatively few studies have assessed young people's stigma in relation to anxiety disorders [14,15,30]. The inclusion of these anxiety disorder vignettes allowed for an exploration of how different aspects of stigma might vary according to disorder. Results of the current study showed that patterns of agreement with different statements varied according to disorder, highlighting the multidimensional nature of stigma. Beliefs in the problem as a sign of personal weakness or ‘not a real medical illness’ were generally higher for social phobia than for other disorders, while beliefs in dangerousness and unpredictability were notably higher for the psychosis/schizophrenia vignette. This may partly reflect that fact that social phobia is less often identified as a mental disorder and is therefore less likely to be associated with some types of stigmatizing attitudes [25,31]. While some respondents may have had personal experience of violence involving a person with schizophrenia, it is likely that this is rare and that media reports associating violence with schizophrenia contribute to perceptions of dangerousness [32,33].
Findings from the current study indicating that young people's stigmatizing attitudes towards PTSD are lower than those towards schizophrenia and similar to or lower than those towards depression are consistent with those of other smaller studies, including a study involving Croatian adolescents [30]. It is possible that attributing a disorder to an external cause, such as that described in the vignette, makes it less likely that it be seen as a character problem or source of shame.
Questionnaire items assessing perceived stigma received much higher endorsement than those assessing personal stigma, findings that replicate those of other studies in young people [10,14]. It is possible that the desire not be judged by the interviewer contributed to the differences. However, it is unlikely that social desirability effects are sufficient to explain the large differences, which may in fact be due to ‘pluralistic ignorance’, a phenomenon in which most people erroneously perceive that they have different attitudes to the majority. It is possible that increasing awareness of the issue of stigma in the community has contributed to the over-estimation of prevalence of stigmatizing beliefs. This is supported by reports of an increase in the belief that a person with depression would be discriminated against, particularly in those Australian states with greatest exposure to campaigns run by beyondblue: the national depression initiative [34]. Thus it is likely that stigma reduction campaigns that target young people should focus on bringing beliefs about public perceptions in line with personal beliefs, particularly those concerning non-disclosure or mental disorders as being due to weakness of character. Such an approach has been used in other areas, including the use of social norms interventions to curb problem drinking in university students [35].
Limitations
Survey limitations include the self-report nature of the data and the fact that responses may be affected by a social desirability bias. In addition, the original items in the scales were developed for use in evaluating depression stigma in adults, and they may not be optimal for assessing stigmatizing attitudes to other disorders. In this study, stigmatizing attitudes were assessed in relation to an unknown person described in a vignette, and it is unclear how young people's beliefs might differ in cases where the respondent knows someone with the disorder. Moreover, relatively little is known about how young people's attitudes translate into behaviour, although there is evidence that stigmatizing attitudes affect the first aid actions of young people towards those with mental disorders [36].
Conclusions
Results of a national survey of young people's stigmatizing attitudes towards those with depression, schizophrenia and anxiety disorders show that patterns of stigmatizing attitudes differ according to disorder, with notable differences between psychosis/schizophrenia and social phobia. It is therefore likely that anti-stigma interventions focusing on individual disorders rather than ‘mental illness’ in general will have a greater chance of success. While all interventions may need to address beliefs about unpredictability, those focusing on social phobia should address beliefs about weakness of character and those addressing more severe disorders may need to address perceptions of dangerousness. Interventions should also focus on bringing beliefs about public perceptions in line with personal beliefs, as the latter are much less stigmatizing.