
Abstract
Objective:
To assess whether willingness to disclose experience of a mental disorder and treatment, and awareness of others’ experiences have changed over a 16-year period.
Methods:
In 2011, telephone interviews were carried out with 6019 Australians aged 15+. The survey interview used the same questions as those of the 1995 and 2003/4 national mental health literacy surveys, in which participants were presented with a case vignette describing either depression, depression with suicidal thoughts (2003/4 only), early schizophrenia or chronic schizophrenia (2003/4 only). Participants were asked whether they had a close friend or family member who had experienced a problem similar to that described in the vignette and whether the person received professional help. They were also asked whether they had experienced such a problem and whether they received professional help.
Results:
The numbers of those disclosing experiences of depression and early schizophrenia, and of having received professional help for depression, have increased since 1995. Awareness of a family member or close friend with experiences of depression and early schizophrenia also increased between these years, as did awareness that the person received professional help.
Conclusions:
The numbers of those disclosing experiences of and treatment for mental disorders has increased in the last 16 years. This is likely to be due to increased willingness to disclose rather than increased prevalence of disorders or increased rates of help-seeking.
Introduction
For many people, the decision to disclose a mental disorder is a complex one, whether this involves revealing a diagnostic label or the experience of psychiatric symptoms. As mental disorders largely fall into the category of ‘concealable stigmas’, stigmatised identities that are not readily apparent to others (Goffman, 1963), disclosure carries the risk of experiencing negative outcomes, such as social rejection and discrimination, that otherwise might have been avoided (Thornicroft et al., 2009; Wahl, 1999). Whether or not a person has had such negative experiences, anxiety about anticipated discrimination may lead to the decision to conceal stigmatising characteristics in order to avoid adverse outcomes (Lasalvia et al., 2013). In the case of mental disorders, the decision to disclose is further complicated by the fact that there may also be benefits of disclosure. For someone with a diagnosis, these may include increased social support and reduced feelings of isolation (Garcia and Crocker, 2008), while for someone with as yet undiagnosed symptoms, labelling the problem as a mental disorder facilitates help-seeking, treatment compliance and ultimately, relief from symptoms (Wright et al., 2011). A person making a decision may need to weigh up the risks and benefits of disclosure according to the context in which they find themselves, for example disclosing a diagnosis to a friend or family member is likely to involve different considerations to disclosure to an employer. Moreover, as stigmatising attitudes vary according to disorder, with people with schizophrenia generally seen as more dangerous and unpredictable, the nature of the diagnosis is also likely to impact on the decision to disclose (Silton et al., 2011; Yap et al., in press). Thus, issues around disclosure, both positive and negative, can play a key role in the degree to which a mental disorder impacts on a person’s life.
In recent decades, concern about the considerable burden of disease related to mental disorders has led to national and international efforts to address this (Kessler et al., 2009). In Australia, the first survey of ‘mental health literacy’ (defined as the ‘knowledge and beliefs about mental disorders which aid their recognition, management or prevention’ (Jorm et al., 1997)) revealed low levels of knowledge about mental disorders in the community. Since then, the National Mental Health Strategy, which has guided mental health reform in Australia since 1992, has become increasingly focused on stigma reduction, mental health promotion and mental illness prevention (Department of Health and Ageing, 2009). Such policies and programmes aim to facilitate early treatment-seeking by improving recognition of mental disorder signs and symptoms, knowledge of appropriate treatments and minimising the impact of stigma as a barrier to help-seeking. Stigma reduction interventions also seek to benefit those with diagnosed disorders by minimising the negative impacts of disclosure and maximising the positive aspects. Through improvements in mental health literacy and stigma reduction, it is possible that such interventions might have the effect of increasing the proportion of people willing to disclose their experience of mental disorders.
Subsequent Australian mental health literacy surveys (conducted in 2003/4 (Jorm et al., 2005b) and 2011 (Reavley and Jorm, 2011)) have revealed improvements in mental health literacy, particularly in recognition of signs and symptoms of depression and beliefs about the likely helpfulness of interventions, which have moved closer to those of health professionals (Reavley and Jorm, 2012a). While stigmatising attitudes were not assessed in the 1995 survey, analysis of changes between 2003/4 and 2011 suggest some reduction in the desire for social distance from those with mental disorders, although increases in beliefs about dangerousness and unpredictability were also seen (Reavley and Jorm, 2012b).
The aim of the current study was to use data from these three surveys of mental health literacy to assess whether willingness to disclose experience of a mental disorder and treatment, and awareness of others’ experiences of mental disorders and treatments, have changed over a 16-year period.
Methods
The 1995 survey
The 1995 survey was carried out by the Australian Bureau of Statistics and the methods have been described by Jorm et al. (1997). Contact was made with 2531 households in both urban and rural areas. One person aged 18–75 years was randomly sampled per household and 2164 people (85%) agreed to participate.
The interview was based on a vignette of a person with depression or schizophrenia (chosen to present one high-prevalence and one low-prevalence disorder). Participants were randomly assigned to receive either vignette and were also assigned to receive either a male (‘John’) or female (‘Mary’) version of the vignette. Respondents were then asked what, if anything, they thought was wrong with the person. They were also asked whether they had a close friend or family member who had a problem like the person in the vignette and if so, whether they received professional help. They were also asked whether they had ever had a problem like the person in the vignette and if so, whether they received professional help. A further question focused on whether they had worked in a job involving treating or providing services to people with similar problems. They were also asked whether they thought the person described in the vignette would be discriminated against. Other questions covered beliefs about the helpfulness of a range of interventions, the likely outcome for the person in the vignette with and without appropriate professional help, and knowledge of causes and risk factors. These analyses are not reported here.
The 2003/4 survey
The methods of the 2003/4 survey, which was carried out by the company AC Nielsen and aimed to replicate the methodology of the earlier survey as closely as possible, have been previously described (Jorm et al., 2005b). Households were sampled from 250 census districts covering all states and territories and metropolitan and rural areas. To achieve a target sample of 4000 interviews with adults aged 18 years or over, visits were made to 28,947 households. The achieved sample was 3998 respondents and the response rate 34%.
In addition to the depression and schizophrenia vignettes used in the 1995 survey, the 2003/4 survey included two additional vignettes: depression with suicidal thoughts and chronic schizophrenia. It also incorporated all the questions of the earlier survey and some additional questions that are not used in the present analyses.
The 2011 survey
The methods of the 2011 survey, which involved computer-assisted telephone interviews (CATI) with 6019 respondents aged 15+, are reported elsewhere (Reavley and Jorm, 2011). The survey was carried out by the company The Social Research Centre, with the sample contacted by random-digit dialling of both landlines and mobile phones covering the whole country from January to May 2011. The response rate was 44%, defined as completed interviews (6019) out of sample members who could be contacted and were confirmed as in scope (13,636).
The survey interview was based on those used in the 1995 and 2003/4 surveys and also included two additional vignettes: social phobia and post-traumatic stress disorder. As these vignettes are not used in the present analyses they are not described here. For the depression and depression with suicidal thoughts vignettes, responses were coded as ‘correct’ if the person mentioned depression and ‘incorrect’ if they did not. For the early and chronic schizophrenia vignettes, responses were coded as ‘correct’ if the person mentioned psychosis or schizophrenia and ‘incorrect’ if they did not.
Statistical analyses
The data were initially analysed using per cent frequencies and 95% confidence intervals. The analyses used sample weights that took account of the number of in-scope persons in the household, telephone type (mobile or landline), age, gender and geographic location. Subsequently, logistic regression analyses were used to assess changes between survey years for the following four dependent variables: the likelihood of having a family member or friend with a problem similar to that described in the vignette; the likelihood of that person having received professional help; the likelihood of the respondent having a problem similar to that described in the vignette; and the likelihood of the respondent having received professional help. In order to control for variations in the sociodemographic characteristics of the survey populations in different years, these analyses included gender, age, level of education and country of birth as covariates.
Further logistic regression analyses were also carried out to assess the interactions between change in disclosure or exposure between survey years and the following sociodemographic characteristics: gender; age; country of birth; and level of education. Due to the large number of analyses carried out, only those reaching the p < 0.01 level were considered significant.
As the 1995 survey only included the depression and chronic schizophrenia vignettes, comparison over three time points was only possible for responses relating to these vignettes. The 2003/4 survey also included the depression with suicidal thoughts and chronic schizophrenia vignettes, thus for data relating to these vignettes, comparison over two time points was possible.
The 1995 survey only included adults aged between 18 and 74 years and to make the samples comparable, those aged 15–17 and 75+ from the 2003/4 and 2011 surveys were dropped from the analyses reported here. This left a total of 3603 respondents: 893 people who received the depression vignette, 903 who received the depression with suicidal thoughts vignette, 892 who received the early schizophrenia vignette and 915 who received the chronic schizophrenia vignette. All analyses were performed using Intercooled Stata 10 (StataCorp LP, Texas, USA).
Results
Survey year
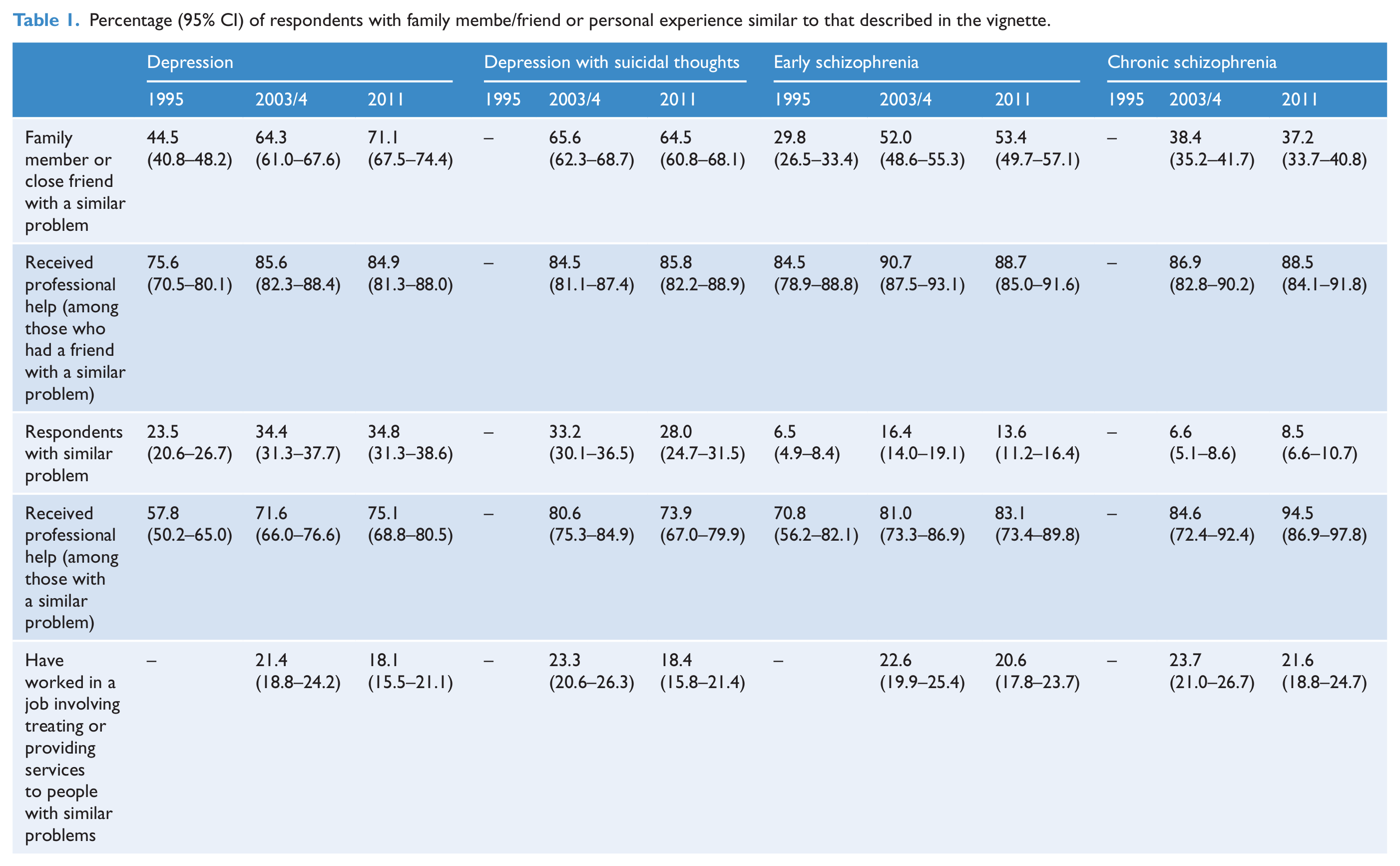
Table 1 gives the percentages of those in each year who reported a problem, or the receipt of professional help for a problem like those described in the vignettes. It also gives the percentages of those aware of a family member or close friend with a similar problem, as well as the percentages aware of a family member or close friend who received professional help. Logistic regression analyses showed that, between 1995 and 2003/4 and 1995 and 2011 there were significant increases in the proportions of respondents with a problem similar to that described in the depression and early schizophrenia vignettes (see Tables 2 and 3). Between 1995 and 2011 and between 2003/4 and 2011 there were significant increases in the numbers of respondents reporting having received professional help for a problem similar to that described in the depression vignette.
Percentage (95% CI) of respondents with family membe/friend or personal experience similar to that described in the vignette.
Summary of binary logistic regression analyses examining changes in exposure and disclosure for the depression vignettes.
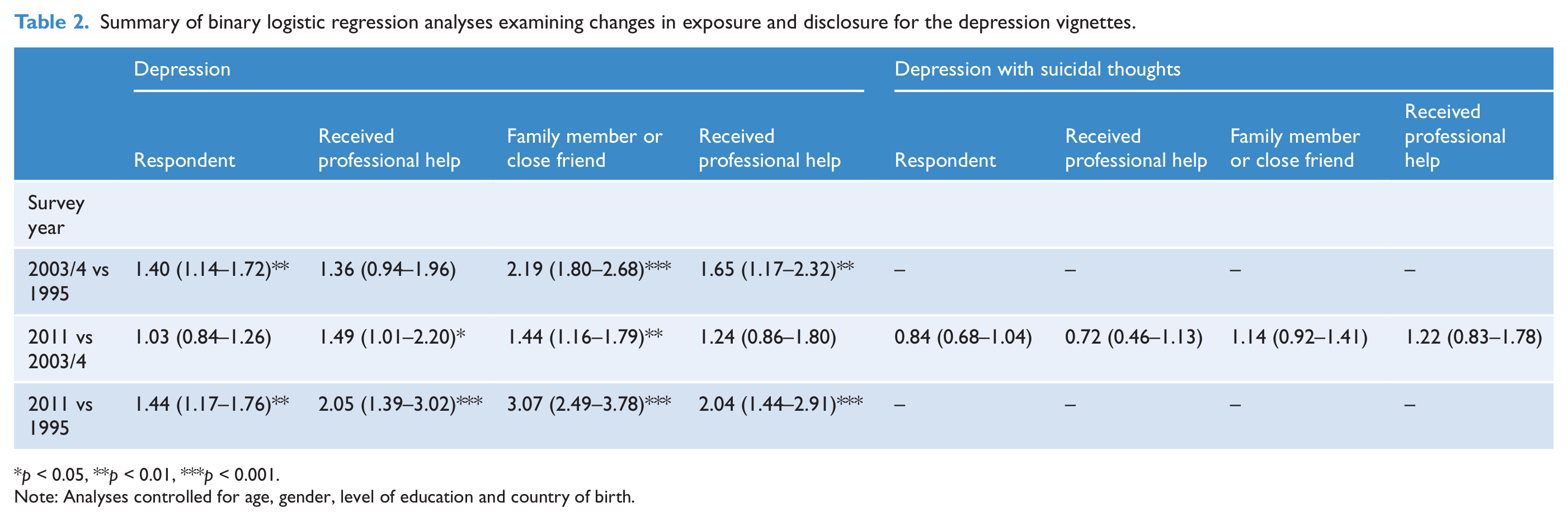
p < 0.05, **p < 0.01, ***p < 0.001.
Note: Analyses controlled for age, gender, level of education and country of birth.
Summary of binary logistic regression analyses examining changes in exposure and disclosure for the schizophrenia vignettes.
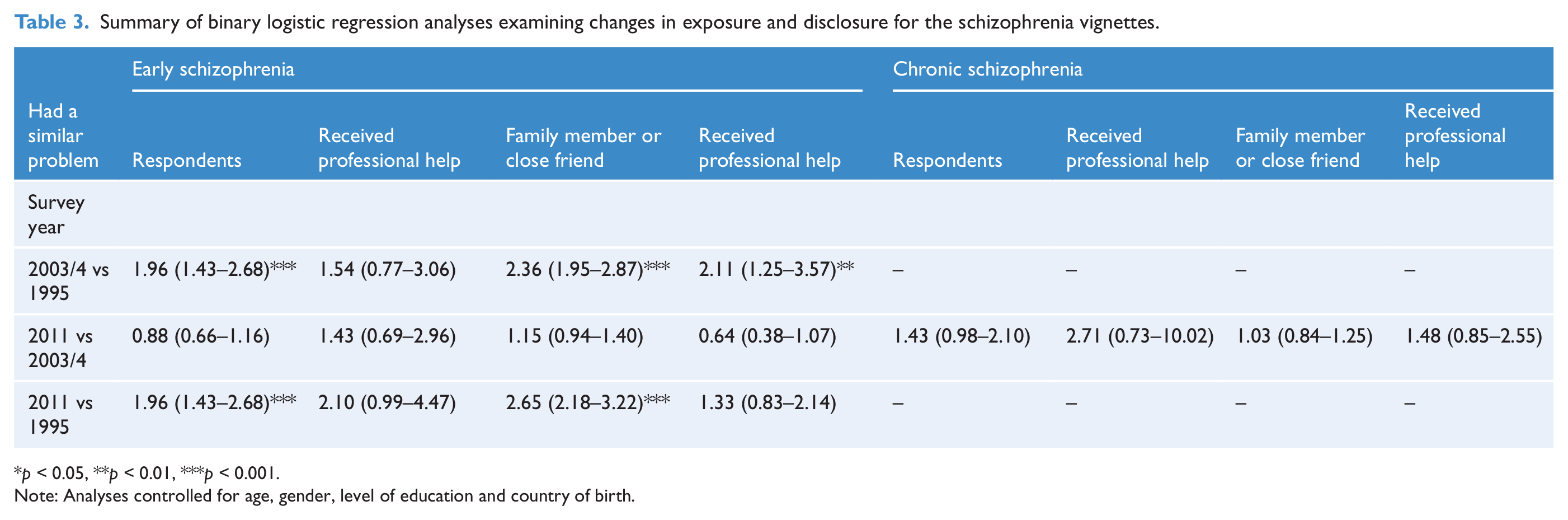
p < 0.05, **p < 0.01, ***p < 0.001.
Note: Analyses controlled for age, gender, level of education and country of birth.
Between 1995 and 2003/4 and 1995 and 2011 there were significant increases in the proportions of people with a family member or close friend with a problem similar to that described in the depression and early schizophrenia vignettes. For the depression vignette, significant increases between 2003/4 and 2011 were also seen. Between 1995 and 2003/4, significant increases in those reporting family members or friends receiving treatment for depression or early schizophrenia were seen. For the depression vignette, significant increases between 1995 and 2011 were also seen.
Subgroup analyses
Changes in awareness and disclosure largely occurred across all subgroups that were examined. Only the differences between subgroups that reached significance at the p < 0.01 level are reported here. For the depression vignette, between 2003/4 and 2011, the change in the number of female respondents reporting receiving professional help was greater than that for males (OR 3.50, 95% CI 1.66 to 7.39, p = 0.001). Between 2003/4 and 2011, the change in the number of respondents born overseas who reported a problem like that described in the depression with suicidal thoughts vignette was greater than that for those born in Australia (OR 2.08, 95% CI 1.30 to 3.32, p = 0.002).
Discussion
The results of the study revealed that the numbers of those disclosing experiences of depression and early schizophrenia, and of having received professional help for depression, have increased since 1995. Awareness of family members or close friends with experiences of depression and early schizophrenia also increased between these years, as did awareness that the person received professional help. The study also showed that, between 2003/4 and 2011, females were more likely than males to disclose experiencing a problem like that described in the depression vignette, and those born overseas were more likely than those born in Australia to disclose experiencing a problem like that described in the depression with suicidal thoughts vignette.
There are several potential explanations for these findings. There could have been increases in the numbers of those experiencing symptoms and seeking professional help, in the ability to recognise symptoms or in the willingness to disclose experiences of symptoms of and treatments for these disorders. Turning first to the possibility that the numbers of those experiencing symptoms has increased, it seems unlikely that this is sufficient to account for the increases. Analysis of changes in the 4NS, a measure of psychological distress included in the 1995, 2003/4 and 2011 surveys, did not show significant increases (Jorm and Reavley, 2012). Moreover, these results are consistent with other studies covering similar time periods that show few changes in mental health (Goldney et al., 2010; Reavley et al., 2011). It also seems unlikely that large increases in the numbers of people seeking professional help between 1995 and 2003/4 account for these results. While there were some difficulties in comparing data from the 1997 and 2007 National Surveys of Mental Health and Wellbeing, Burgess et al. (2009) concluded that, while the pattern of service use changed, overall rates of service use by people with affective disorders did not change substantially between surveys.
Data from the three mental health literacy surveys show that the ability to accurately label the symptoms given in the vignettes as depression or schizophrenia has increased over 16 years, with the largest changes occurring between 1995 and 2003/4 (Reavley and Jorm, 2012a). Such improvements in mental health literacy have also been seen in other studies (Angermeyer and Matschinger, 2005a; Angermeyer et al., 2009, Goldney et al., 2005, 2009). Thus, it is possible that the improved ability to recognise symptoms partly explains the results of the current study, particularly as the question about knowledge of others’ experiences asked about close friends or family. However, a greater ability to identify symptoms would not explain the increases in the proportions of those disclosing professional help-seeking (in the absence of data suggesting that actual increases have occurred).
Thus, it seems likely that willingness to disclose experiences of mental disorders and help-seeking for such problems has increased over the last 16 years. The finding that not only were respondents more aware of problems in others, but were also willing to disclose their own experiences of symptoms and treatment point to the possible contribution of lower stigma around disclosure. As the stigma measures that were included in the 2003/4 and 2011 surveys were not included in the 1995 survey, it is not possible to assess changes in stigmatising attitudes over this time period. However, 2011 respondents were not significantly less likely to believe that people with depression or early schizophrenia would be discriminated against in 2011 than in 1995 (Reavley and Jorm, 2012b). The results of the current study also contrast with those of the study assessing changes in stigmatising attitudes over time, in that the proportion of people who would not tell anyone if they had a problem like the person in the depression vignette increased between 2003/4 and 2011 (Reavley and Jorm, 2012b). However, the relationship between stigma and disclosure is likely to be a complex one, with results of longitudinal surveys in several countries suggesting that while there have been improvements in some stigmatising attitudes, these depend on both the disorder and the aspect of stigma under consideration (Angermeyer and Matschinger, 2005b; Mehta et al., 2009; Reavley and Jorm, 2012b).
It is possible that increased likelihood of disclosure partly reflect the efforts of beyondblue: the national depression initiative, as results from previous surveys have shown changes in mental health literacy to be linked to these campaigns (Jorm et al., 2005a). The results of the current study suggest that, in recent years at least, they have been particularly effective in increasing the likelihood of disclosure in females and those born overseas. Such campaigns have tended to focus on education about and promotion of help-seeking for depression. While there have not been equivalent education campaigns focusing on early schizophrenia, it is possible that education about depression has led to greater knowledge about other types of mental illness. However, further research needs to explore issues around disclosure of mental disorders and the links to stigma. Such research could explore anticipated stigma as well as the outcomes of disclosure in various contexts, both positive and negative.
Evidence from such studies could provide much needed input into the design of anti-discrimination interventions, for example public education about human rights and the impact of discrimination on people with mental disorders; action from health services to help overcome anticipated discrimination as a barrier to help-seeking; and the incorporation into treatments of techniques to address disclosure and anticipated discrimination.
Limitations of the study include the differences in survey methodology between the surveys. The 2003/4 survey involved household interviews while the 2011 survey adopted CATI as an alternative because household surveys are much more expensive. Thus, when comparing the findings from 2011 with the earlier survey, some caution was required in interpreting any differences, as the change in method might have affected the results. Furthermore, the relatively low response rates of 34% and 44% for the first and second surveys respectively, although in line with other similar Australian surveys, may limit the generalisability of the results (Curtin et al., 2005).
Conclusions
The numbers of those disclosing experiences of and treatment for mental disorders has increased in the last 16 years, particularly between 1995 and 2003/4. This is likely to be due to increased willingness to disclose rather than increased prevalence of disorders or increased rates of help-seeking.
Footnotes
Funding
The study was funded by the Commonwealth Government Department of Health and Ageing. The authors receive salary support from the National Health and Medical Research Council.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.