
Abstract
Approximately two thirds of those who meet the criteria for a mental disorder do not seek professional help, with those in the youngest age group the least likely to do so [1]. Among the factors impacting on help seeking is that of mental health literacy, which incorporates the ability to recognize specific disorders; knowledge of causes, risk factors, self-treatments and available professional help; as well as attitudes that promote recognition and appropriate help seeking [2]. Surveys in several countries have examined aspects of mental health literacy that affect whether an individual suffering from a mental disorder receives appropriate treatment [3–6]. In Australia, these include the national surveys of mental health literacy in the adult population that were carried out in 1995 and 2003–2004 [2,7].
It is generally agreed that recognition of a problem is the necessary first step to seeking help from an appropriate professional, with failure to recognize signs and symptoms as indicating a mental disorder likely to delay help seeking [8]. This is of importance as there is evidence that early recognition and treatment may improve long-term outcomes for those with mental disorders [9,10]. Moreover, the use of correct psychiatric labels may facilitate communication with health professionals, and it has been shown that GPs are more likely to detect a mental disorder if the patient conceptualizes their problem as such [11]. Beliefs about the helpfulness of interventions also impact on help seeking and treatment compliance. Surveys in several countries have shown that negative attitudes towards medications such as antipsychotics and antidepressants are common, while psychological and complementary therapies and self-help strategies tend to be viewed more positively [2,3,6,12]. Such beliefs can affect treatment outcomes. For example, it has been found that depressed patients who have negative attitudes towards antidepressants are less likely to be prescribed these medications, less likely to fill prescriptions and less likely to benefit overall [13].
Evidence of the relatively low levels of mental health literacy in members of the public has led to campaigns to improve this in a number of countries. Such campaigns have tended to focus on mental illness broadly, or specifically on depression [14–17]. Despite their relatively high prevalence, there has been very little focus on anxiety disorders [18]. The aim of the study was to carry out a national survey in order to assess recognition and beliefs about treatment and outcomes for affective disorders, anxiety disorders and schizophrenia/psychosis.
Methods
The survey involved computer-assisted telephone interviews (CATI) with a national sample of 6019 members of the general community aged 15 +. The survey was carried out by the survey company Social Research Centre. A ‘dual frame’ approach was used, with the sample contacted by random-digit dialling of both landlines and mobile phones. This approach was taken in order to minimize the potential bias of collecting data solely from households with a landline telephone connection. The landline-only approach may under-sample young people, particularly young men [19]. In order to achieve a mobile/landline distribution representative of the Australian population, targets of at least 1500 mobile and 4000 landline interviews were set. Interviews were conducted between January and April 2011.
Survey interview
The interview was based on a vignette of a person with a mental disorder. On a random basis, respondents were read one of six vignettes: depression, depression with suicidal thoughts, early schizophrenia, chronic schizophrenia, social phobia and post-traumatic stress disorder (PTSD). Respondents were also randomly assigned to receive either male (‘John’) or female (‘Jenny’) versions of the vignette. All vignettes were written to satisfy the diagnostic criteria for either major depression or schizophrenia according to DSM-IV and ICD-10. The first four vignettes have been published previously [7] and the latter two, which were used for the first time, are given here.
The social phobia vignette was as follows: John is a 30-year old who lives alone. Since moving to a new town last year he has become even more shy than usual and has made only one friend. He would really like to make more friends but is scared that he'll do or say something embarrassing when he's around others. Although John's work is OK he rarely says a word in meetings and becomes incredibly nervous, trembles, blushes and seems like he might vomit if he has to answer a question or speak in front of his workmates. John is quite talkative with his close relatives, but becomes quiet if anyone he doesn't know well is present. He never answers the phone and he refuses to attend social gatherings. He knows his fears are unreasonable but he can't seem to control them and this really upsets him.
The PTSD vignette was as follows: John is a 30-year-old who lives with his wife. Recently his sleep has been disturbed and he has been having vivid nightmares. He has been increasingly irritable, and can't understand why. He has also been jumpy, on edge and tending to avoid going out, even to see friends. Previously he had been highly sociable. These things started happening around two months ago. John owns a newsagent shop with his wife and has found work difficult since a man armed with a knife attempted to rob the cash register while he was working four months ago. He sees the intruder's face clearly in his nightmares. He refuses to talk about what happened and his wife says she feels that he is shutting her out.
After being presented with the vignette, respondents were asked what, if anything, they thought was wrong with the person described in the vignette, how the person could best be helped, and a series of questions about the likely helpfulness of a wide range of interventions (rated as likely to be helpful, harmful or neither for the person described in the vignette). The interventions were: a typical GP or family doctor; a typical chemist (pharmacist); a counsellor; a social worker; a telephone counselling service such as Lifeline; a psychiatrist; a psychologist; help from close family; help from close friends; a naturopath or a herbalist; the clergy; a minister or priest; John/Jenny tried to deal with his/her problems on his/her own; vitamins and minerals; tonics or herbal medicines; pain relievers such as aspirin, codeine or Panadol; antidepressants; antibiotics; sleeping pills; antipsychotics; tranquillizers such as Valium; becoming physically more active, such as playing more sport, or doing a lot more walking or gardening; reading about people with similar problems and how they have dealt with them; getting out and about more; attending courses or relaxation, stress management, meditation or yoga; cutting out alcohol altogether; psychotherapy; hypnosis; being admitted to a psychiatric ward of a hospital; undergoing electro-convulsive therapy (ECT); having an occasional alcoholic drink to relax; going on a special diet or avoiding certain foods. The interview also included questions asking about the likely result for the person in the vignette with and without ‘the sort of professional help you think is most appropriate’. The response options were: full recovery with no further problems, full recovery but problems would probably reoccur, partial recovery, partial recovery but problems would probably reoccur, no improvement, get worse. Data relating to these questions is reported here.
Respondents were also asked questions about their health, knowledge of causes and risk factors, beliefs associated with stigma and discrimination and contact with people like those in the vignette. Data relating to these latter questions is reported elsewhere [20].
Coding of open-ended responses
Responses were coded based on the pre-coded categories similar to those used in previous surveys [2,21]. Responses to the question of what was wrong with the person in the vignette were depression, schizophrenia, mental illness, stress, nervous breakdown, psychological/mental emotional problem, has a problem, cancer, nothing, don't know. A content analysis of responses that did not fit these pre-coded categories led to post-coding of 35 other categories. Many of these were used to describe the social phobia or PTSD vignettes. They include anxiety/anxious, anxiety disorder, social anxiety/social phobia, shy, low self-confidence/low self-esteem, PTSD, fear/scared, trauma and stress. Responses were coded with a ‘yes’ or ‘no’ in each category, so that multiple categories were possible. For simplicity, the response categories reported here include those that were either the most accurate, or those nominated by more than 10% of the sample.
Responses to the question about how the person might best be helped were also based on categories from previous surveys and also included other responses nominated by more than 1% of those who received any particular vignette. These included: talk over the problem with friends or family, see a GP/doctor, see a psychiatrist, take medication, see a counsellor, John/Jenny must first recognize the problem, see a psychologist, see a specialist, get out more, talk to someone, beyondblue, be admitted to an institution, and join a club.
Statistical analysis
The data were analysed using per cent frequencies and 95% confidence intervals. A pre-weight was applied to adjust for the dual frame design and the respondent chance of selection. The achieved sample was close to the Australian national population in terms of geographic distribution, however, there was an under-representation of males and of younger adults, and an over-representation of university educated individuals and people with an English-speaking background. A population weight was used to adjust for these biases. All analyses were performed using Intercooled Stata 10 (StataCorp, College Station, TX).
Results
The response rate for the survey was 44%, defined as completed interviews (6019) out of sample members who could be contacted and were confirmed as in scope (13 636). Those who were in scope, but who fell into age or gender categories that were full, did not complete the interview. Overall, 4324 interviews were conducted on landlines and 1696 on mobiles. The numbers assigned to each vignette were: depression, n = 1016; depression with suicidal thoughts, n = 1008; early schizophrenia, n = 1002; chronic schizophrenia, n = 993; social phobia, n = 992; and PTSD, n = 1008. There were no significant differences between vignettes in regard to age, gender, marital status, level of education, country of birth and location.
Recognition of disorders
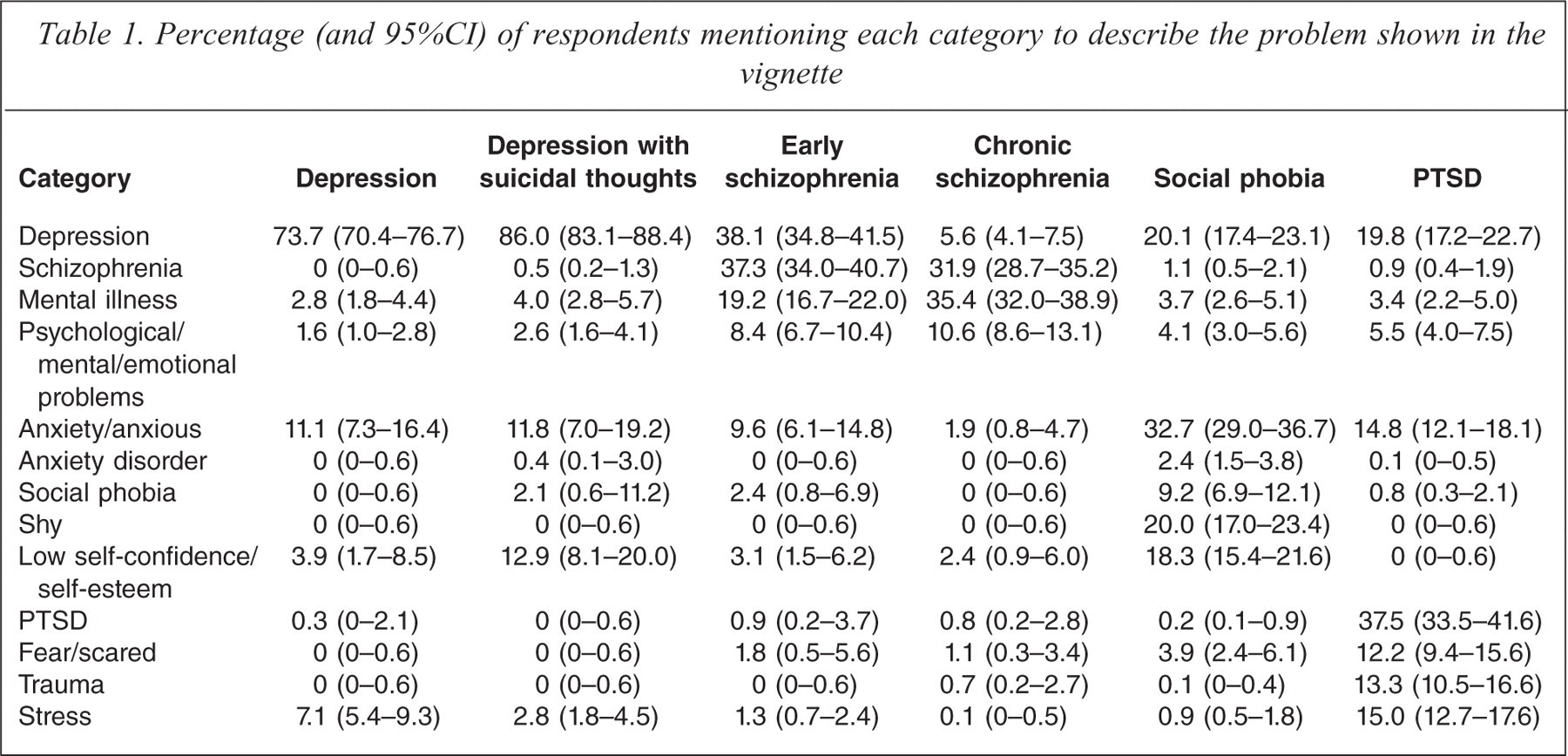
Table 1 shows the percentage of respondents mentioning the categories to describe the problems shown in the vignettes. ‘Depression’ was the term used most often to describe both the depression vignette and the depression with suicidal thoughts vignette. ‘Depression’ and ‘schizophrenia’ were the terms most often used for the early schizophrenia vignette, while ‘mental illness’ and ‘schizophrenia’ were the terms most commonly used for the chronic schizophrenia vignette. ‘Anxiety/anxious’, ‘depression’, ‘shy’ and ‘low self-confidence/self esteem’ were the terms most often used to describe the social phobia vignette. ‘PTSD’, ‘depression’, ‘stress’, ‘trauma’, ‘anxiety/anxious’ and ‘fear’ were the terms most often used to describe the PTSD vignette.
Percentage (and 95%CI) of respondents mentioning each category to describe the problem shown in the vignette
Best method of help
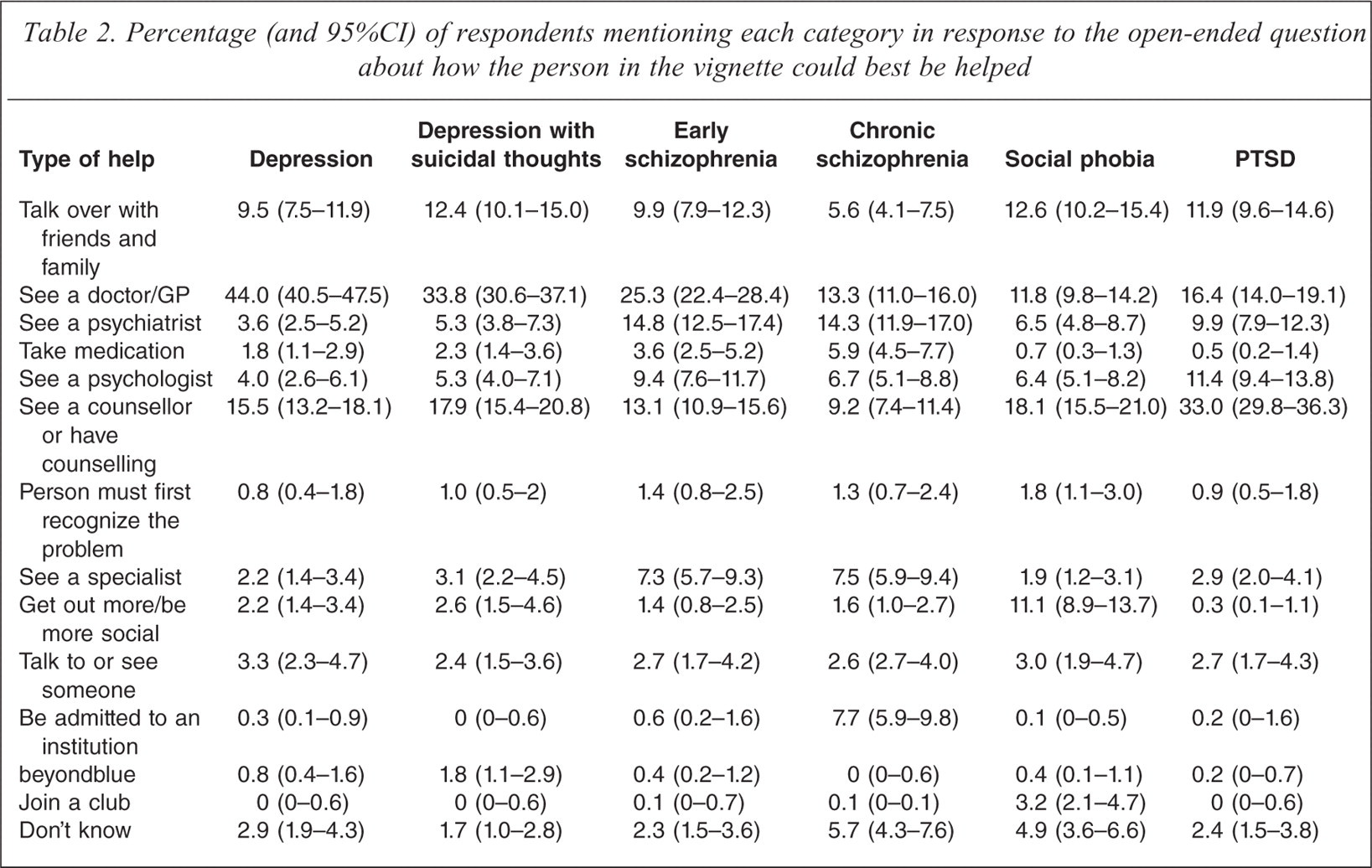
Table 2 shows the frequency of responses to the open-ended question about how the person in the vignette could best be helped. For the depression, depression with suicidal thoughts, and early schizophrenia vignettes, GPs were considered the most helpful. For the chronic schizophrenia vignette, GPs and psychiatrists were considered the most helpful. For social phobia, counselling and talking things over with family and friends were considered the most helpful, whereas for PTSD, counselling was considered the most helpful.
Percentage (and 95%CI) of respondents mentioning each category in response to the open-ended question about how the person in the vignette could best be helped
Beliefs about specific interventions
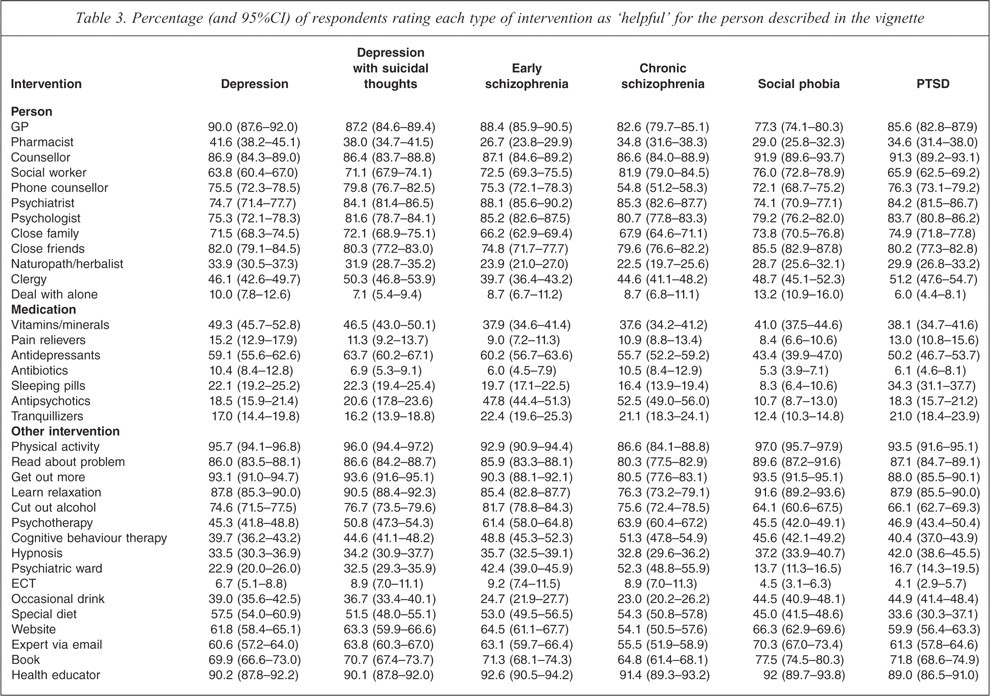
Table 3 shows respondents' ratings of the likely helpfulness of specific people and interventions, while Table 4 shows ratings of harmfulness. Among people who could help, GPs received the highest rating for the depression, depression with suicidal thoughts and early schizophrenia vignettes. For the other vignettes, counsellors received the highest rating. Among medications, antidepressants were considered the most helpful for all vignettes. Around 50% of survey respondents rated antipsychotics as likely to be helpful for both schizophrenia vignettes. Vitamins and minerals were also relatively highly rated compared to other medications with between 37.9% and 49.3% of respondents rating these as likely to be helpful. Among other interventions, the most highly rated interventions were physical activity, reading about the problem, ‘getting out more’, learning relaxation and seeing a health educator. This was the case for all vignettes.
Percentage (and 95%CI) of respondents rating each type of intervention as ‘helpful’ for the person described in the vignette
Percentage (and 95%CI) of respondents rating each type of intervention as ‘harmful’ for the person described in the vignette
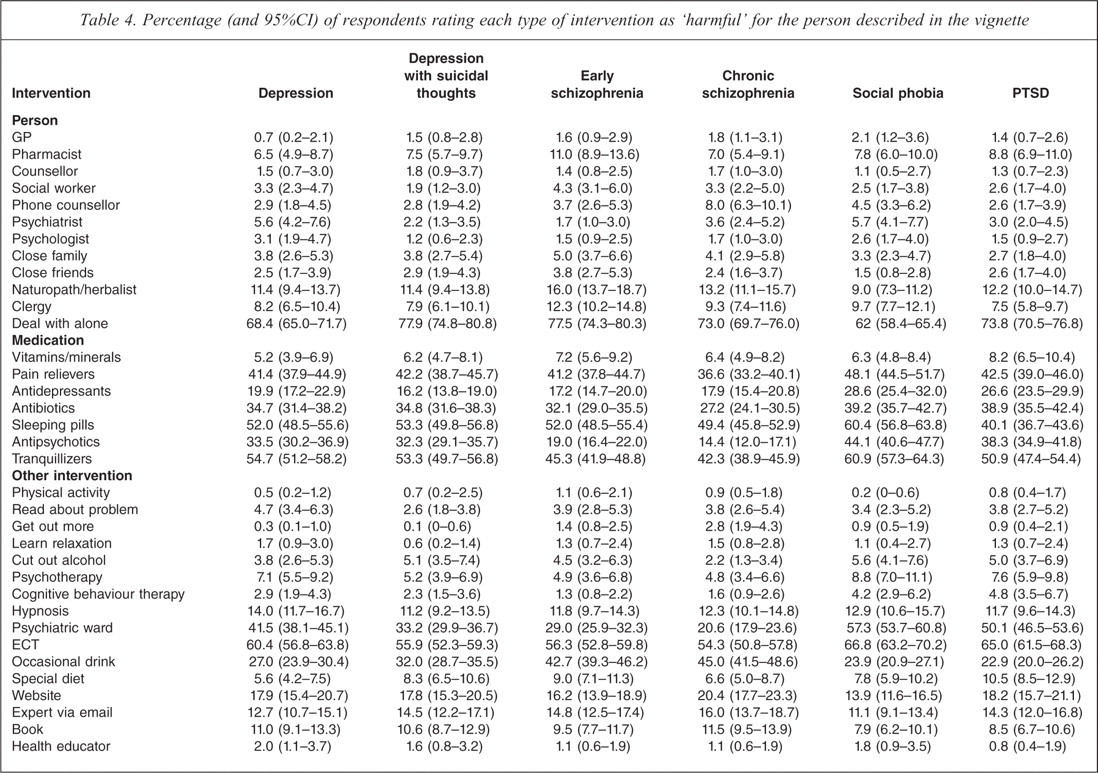
For all vignettes, dealing with the problem alone was considered the most likely to be harmful. Among medications, sleeping pills and tranquillizers were considered the most likely to be harmful across all vignettes, although pain relievers were considered more likely to be harmful than sleeping pills for PTSD. Among other interventions, ECT, being admitted to a psychiatric ward and having an occasional drink were rated the most harmful across all vignettes. In addition, more people thought it would be more helpful than harmful to have an occasional alcoholic drink to relax for the depression and anxiety disorder vignettes.
Beliefs about likely outcomes for those with mental disorders
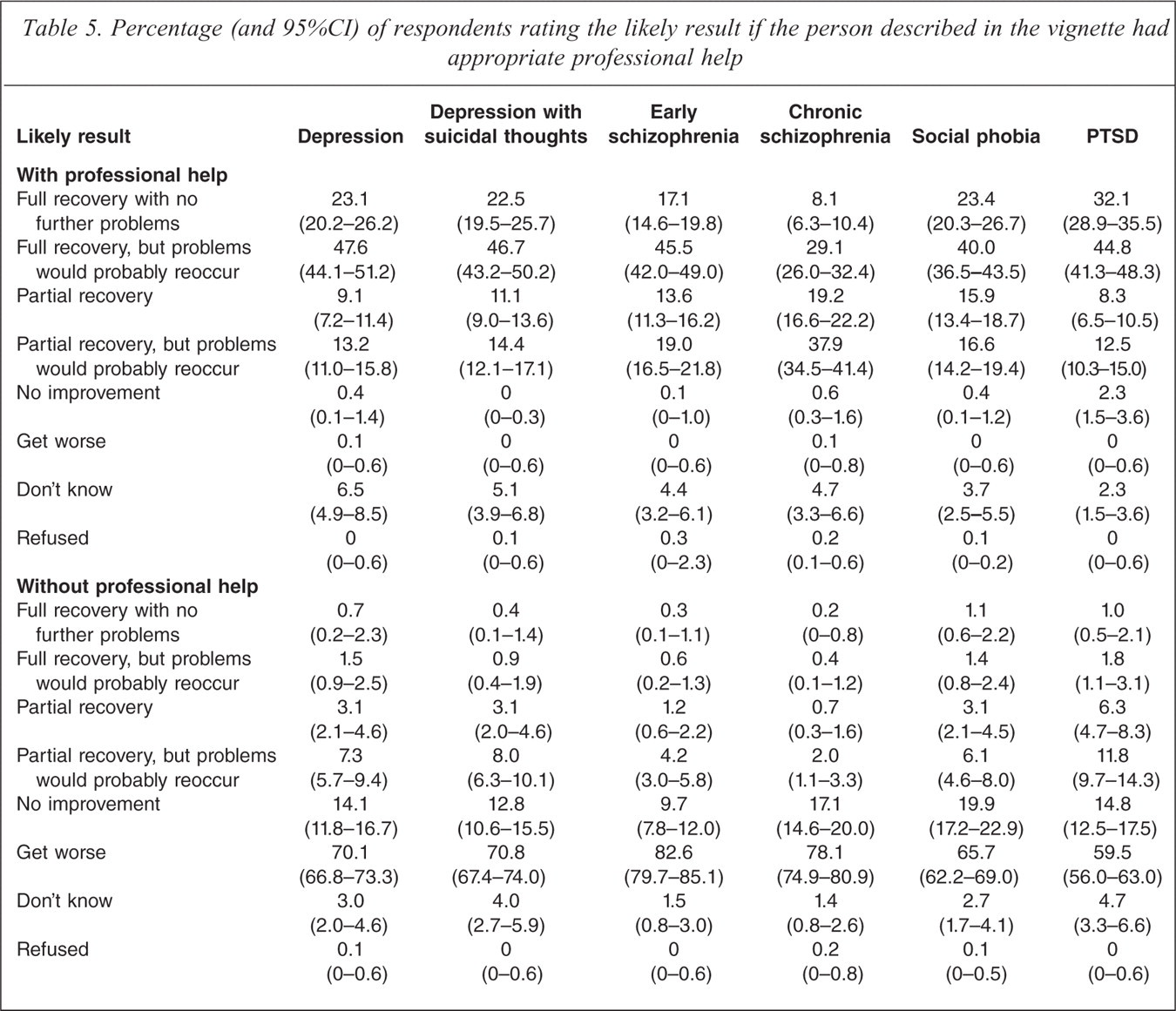
Table 5 shows respondents' views about the likely outcomes if the person described in the vignette did or did not have appropriate professional help. The majority of respondents considered that full recovery with problems reoccurring would be the most likely outcomes for all vignettes other than the chronic schizophrenia vignette, for which partial recovery with problems reoccurring was considered to be the most likely outcome. For all vignettes, getting worse was considered the most likely outcome if the person did not receive appropriate treatment.
Percentage (and 95%CI) of respondents rating the likely result if the person described in the vignette had appropriate professional help
Discussion
A 2011 survey of mental health literacy and stigma in 6019 Australians aged 15+ showed that rates of recognition of depression in a vignette were relatively high, with almost 75% of respondents using the correct label. Rates of recognition for the schizophrenia vignettes and PTSD were similar, with around one third of respondents using the correct labels. Only 9.2% of respondents were able to correctly label social phobia. When asked about the helpfulness of various people and interventions for the disorders described in the vignettes, respondents tended to give the highest ratings to GPs, counsellors, antidepressants, antipsychotics (for schizophrenia) and lifestyle interventions such as physical activity, relaxation and getting out more.
Recognition of the disorders in the vignettes
As far as the authors are aware, this is the first population survey to assess mental health literacy in relation to PTSD. This is of significance as relatively few studies have assessed mental health literacy in relation to anxiety disorders [22,23], despite the fact that anxiety disorders have higher prevalence than affective disorders, with 14.4% of the Australian population affected in any 12-month period, compared to 6.2% for affective disorders [18]. Of the anxiety disorders, PTSD is the most common, and social phobia the next most common, with 12-month prevalence rates of 6.4% and 4.7% respectively [18].
It has been estimated that three quarters of Australian men and women have been exposed to at least one potentially traumatic event (PTE) during their lifetime [24]. PTEs include a range of major life stressors such as natural and technological disasters, combat exposure, rape, physical assault, child abuse, severe car crashes, and sudden death of a loved one. It is possible that the relatively high rates of recognition of PTSD compared to social phobia may be due to media coverage of PTSD in veterans returning from wars in Afghanistan and Iraq as well that following natural disasters such as cyclones, floods and bushfires. That the most commonly nominated source of help for PTSD was counselling may support this possibility, as psychological interventions are often promoted after traumatic events and may be discussed in media reports [25]. However, results from the current survey show that a considerable number of Australians do not recognize PTSD in a vignette, and while most people do not develop PTSD as a result of exposure to PTEs, the high numbers experiencing PTEs in the Australian population point to the need for education about signs, symptoms and appropriate treatments for the disorder.
Recognition of social phobia was notably lower than that for PTSD. For this vignette, respondents were much more likely to use terms such as anxious (32.7%), shy (20.2%) and low self-confidence (18.3%), revealing that they were much less likely to view the symptoms described in the vignette as indicating a mental disorder. While these results may also indicate low mental health literacy in regard to correct labels, rather than a lack of recognition of the symptoms as being due to a mental disorder, results from a study by Wright and colleagues [26] point to the importance of using the label ‘social phobia’ in predicting help seeking, particularly from health professionals.
While the correct use of the term ‘depression’ appears to be common, results from the 2011 survey suggest that its use may be over-generalized, as it was also commonly used to describe the other disorders in the vignettes. For the early schizophrenia vignette, very similar percentages of people used the terms ‘depression’ and ‘schizophrenia’ and those given the social phobia vignette were more likely to use the label ‘depression’ than ‘social phobia’, ‘shy’ and ‘low self-esteem/low self-confidence’. For PTSD, it was the second most common label after PTSD. While labelling a range of disorders as ‘depression’ may be helpful in prompting professional help seeking, these data point to the need to build on public knowledge of depression in order to differentiate its symptoms and treatments from other disorders, particularly anxiety disorders, which are less well recognized and generally perceived as having less need for treatment.
Beliefs about the helpfulness of interventions
The lower likelihood of recognizing social phobia as an anxiety disorder is also reflected in the data on respondents' beliefs about sources of help. Numbers of those recommending a GP as the best source of help were lowest for social phobia and rates of talking the problem over with family and friends were relatively high. In addition, respondents were least likely to receive professional help if they experienced a problem similar to that described in the social phobia vignette. The results of the current survey reflect the results of other studies suggesting a lower perceived need for help for anxiety disorders [27] and may explain the low rate of professional help seeking for anxiety disorders found in the 2007 Australian National Survey of Mental Health and Wellbeing [16]. In the 2011 survey, as in previous mental health literacy surveys, respondents gave higher ratings to counsellors than psychologists and psychiatrists (other than for the early schizophrenia vignette) [2,7]. This is despite the fact that psychologists and psychiatrists are nationally registered professions with scientifically based training, requirements for supervised professional practice and continuing professional education, while ‘counsellors’ are not a registered profession. This may reflect media reports of mental health treatments which often refer to recipients of ‘counselling’ rather than other psychological interventions [25]. However, there may be a need for further public education on the role and training of various professionals in order that consumers may make better informed decisions.
When asked about the helpfulness of various medications, antidepressants received the highest ratings for all disorders, with the highest rating of 63.7% for depression with suicidal thoughts. Around 50% of respondents rated antipsychotics as helpful for schizophrenia, rates which were notably higher than for other disorders. However, respondents gave higher helpfulness ratings to lifestyle interventions, such as physical activity, relaxation and getting out more, than those generally endorsed by health professionals, such as psychotherapy, cognitive behaviour therapy and admission to a psychiatric ward [28–30]. They were also more positive about generic counselling than the more evidence-based cognitive behaviour therapy (CBT). Such gaps between public and professional beliefs are of concern as they may limit adherence to recommended treatments. It was also notable that more people think it would be more helpful than harmful to have an occasional alcoholic drink to relax for the depression and anxiety disorder vignettes, pointing to the need for education about ways of coping with anxiety and depression that do not involve alcohol.
Websites as a source of help received lower ratings than reading about a problem, books or health educators, possibly due to concerns about the quality of information. This may be justified given the relatively poor quality of many mental health information websites [31].
Comparison with the results of earlier surveys of mental health literacy in the Australian public revealed improvements, particularly in recognition of depression in a vignette, beliefs about the helpfulness of GPs, psychiatrists and counsellors and beliefs in the helpfulness of medications, particularly antidepressants and antipsychotics. It is likely that improved recognition rates for depression partly reflect the efforts of beyondblue: the national depression initiative [32]. However, there is still potential for mental health literacy gains in the areas of recognition and treatment beliefs for all the mental disorders covered in this survey, particularly schizophrenia and anxiety disorders.
Beliefs about likely outcomes for those with mental disorders
When asked about possible outcomes for those described in the vignettes, respondents were more likely to believe in full recovery with problems reoccurring for those who received appropriate treatment for mental disorders. The exception to this was the chronic schizophrenia vignette for which partial recovery with problems reoccurring was the most common belief. Public beliefs about possible outcomes for those with mental disorders reflected a less optimistic view in 2011 than in the 1995 survey, with beliefs in full or partial recovery with relapse for depression and schizophrenia increasing and belief in full recovery decreasing. Beliefs in getting worse without appropriate treatment also increased. In this regard, the public have become more like mental health professionals, who were less optimistic about full recovery when surveyed in the late 1990s [33].
Conclusions
While beliefs about effective medications and interventions for mental disorders have moved closer to those of health professionals since surveys conducted in 1995 and 2003–2004, there is still potential for mental health literacy gains in the areas of recognition and treatment beliefs for mental disorders. This is particularly the case for schizophrenia and anxiety disorders, which are less well recognized and, in the case of social phobia, generally perceived as having less need for professional help.