
Abstract
Improvements in mental health literacy [1] at the community level have been shown to have positive effects on helping behaviours and to reduce both stigmatizing attitudes and social distancing of individuals with a mental health problem [2]. Poor mental health literacy on the other hand, is expected to create barriers to helping and help-seeking [3]. Further, there is some evidence that better literacy is associated with resilience in families affected by a mental health difficulty [4] and that more literate individuals have more positive attitudes to help-seeking [5].
Mood disorders in the perinatal period (pregnancy and the first 12 months postpartum) are highly prevalent [6], under-diagnosed, and, because of the presence of an infant or foetus, involve some unique considerations for identification, treatment and management [7–9]. In Australia no previous survey has focused specifically on community awareness, attitudes and knowledge in respect of depression in perinatal women (antenatal and postnatal depression). A number of initiatives have sought to raise community awareness of perinatal mood disorders (e.g. beyondblue: the national depression initiative), and the advent of the National Perinatal Depression Initiative (NPDI) [10] is likely to produce an increase in the identification of cases. This Federal initiative will offer a psychosocial assessment to every pregnant woman and every new mother in Australia, focused on the identification of depression, anxiety and related disorders [10]. Whether universal screening will have the desired effect of increasing the uptake of effective treatments remains to be seen. Nonetheless, the level of mental health literacy among women, their families and their support networks is likely to be a crucial factor in facilitating early recognition and appropriate help-seeking [11]. It is therefore timely and important to establish a benchmark of prevailing community knowledge, attitudes and beliefs about depression in the perinatal period.
Several previous population surveys [12–16] have assessed the mental health literacy of Australians in regard to common mental disorders. By allowing tracking of population level changes, especially in connection with awareness-raising initiatives, these have proved valuable in building a picture of what Australians know and think about mental health generally and about depression in particular. Whilst most people's specific knowledge of depression and its effective treatment is limited, the situation has improved within the last decade [13,17]. Men and women have been found to differ in their knowledge of and attitudes to mental health [15,18] as have different age groups [19]. Also, sizeable differences in knowledge and attitudes about appropriate treatments have been recorded between the general population and those with training in the mental health field [20]. Some similar patterns have emerged in the few existing studies of perinatal mental health literacy [11]. The present study, conducted by beyondblue, aimed to provide a national snapshot of literacy, advance our knowledge with respect to potential demographic variations, and to set the scene for monitoring future changes in the Australian population.
Methods
A 26-item survey (The Perinatal Depression Monitor) was designed to measure awareness, attitudes and knowledge concerning antenatal and postnatal depression and perinatal mental health more broadly. The survey was structured similarly to those used in two previous studies of depression literacy in Australia [12,17]. Items were developed from consultations between beyondblue project officers and health professionals and from feedback to beyondblue via education sessions and its website. Prior to being finalized, a draft was circulated for comment through BlueVoices, the consumer and carer arm of beyondblue, and to health professionals working in the field of perinatal mental health.
The target sample was randomly selected, in proportion to each State and Territory population, from the Sample Pages database which contains 6,000,000 Australian residential telephone numbers, updated monthly (see http://www.samplepages.com.au/). The survey was conducted by 34 interviewers following the ICC/ESOMAR international code of marketing and social research practice. Calls were made in the daytime (mainly weekends) and evenings from 4 November 2009 to 18 November 2009. Respondents were invited to take part in a survey about health issues before and after pregnancy, and were not told that its focus was depression or that it was being undertaken on behalf of beyondblue.
The survey commenced with the question ‘To begin with, what do you consider to be the major health problems which may be experienced during pregnancy?’ This was followed immediately by a similarly worded item concerning major health problems in the postnatal period. Next, respondents were asked ‘And thinking about mental health in particular, what do you consider to be the major mental health problems which may be experienced during pregnancy?’ This was followed by an equivalent question concerning mental health in the first postnatal year. For each of these items, up to four spontaneous responses were recorded from each participant, followed by further responses elicited by a probe question (‘Are there any other major health/mental health problems during pregnancy/in the first year?’).
Subsequent items in the survey focused on awareness of and attitudes to depression in the perinatal period, and on literacy about its prevalence, symptoms, causes and treatments. Next, respondents were asked to rate their agreement on a 4-point scale (from Strongly agree to Strongly disagree) with a number of statements designed to measure the prevalence of some specific attitudes to antenatal and postnatal depression. Demographic data were also collected including age, gender, parental status and whether respondents had training in the field of mental health. The survey concluded with the question ‘Have you heard of any organizations related to depression?’ followed by three prompting questions. These responses were coded as representing level of awareness of beyondblue: the national depression initiative, on a scale of High (beyondblue = unprompted first response) to None (no mention of beyondblue after three prompts).
Percentage responses on each item were calculated by applying survey weights according to gender, age and location (State, Territory and metropolitan versus regional locations) based on the Australian Bureau of Statistics 2001 Census (http://www.abs.gov.au/websitedbs). Differences in response frequencies between demographic groups were tested by χ2. Since the weighted sample size was large (n = 14 663) a more conservative alpha level of 0.001 was applied when assessing statistical significance (p < 0.001). Statistical computations were executed in SPSS version 16 and in PASSW 18.
Results
A total of 1201 people responded to the survey (315 men; 886 women). Of 9260 telephone numbers in scope, 7417 declined participation and 642 were not contactable by the end of the survey period (busy, no answer, answerphone). The regional representation in the unweighted sample of respondents was: New South Wales, 408; Victoria, 300; Queensland, 222; Western Australia, 116; South Australia, 95; Tasmania and Territories, 60. Of the respondents, 740 (62%) lived within the major metropolitan areas (Sydney, Melbourne, Perth, Brisbane, Adelaide); 189 respondents were aged 18–34 years, 538 were aged 35–54 and 474 were aged 55 years or more; 1006 respondents (83.8%) identified themselves as parents; 263 (22%) of the respondents had achieved a degree as their highest educational qualification and a further 156 (13%) had a post-graduate qualification.
Awareness of depression in the perinatal period
In the weighted sample the most frequent spontaneous (un-probed) responses for major health problems during pregnancy were blood pressure (16.7%), diabetes/gestational diabetes (10.1%), and nausea/vomiting (7.1%). Unprobed mentions of mental health problems were comparatively rare in this context (3.7% of respondents cited anxiety, 3.3% cited depression and 0.8% cited unspecified mental health problems). In contrast, regarding the first year following birth, the frequency of issues cited first (i.e. first, unprobed responses only) as major health problems was headed by postnatal depression (24.8%), followed by unspecified depression (18.8%), and fatigue (10.4%). Of first responses alone, mentions of all mental health issues were cited by 49.9% of respondents to this item on general postnatal health. Awareness of beyondblue was positively associated with citing depression as a major postnatal health problem (ranging from 53.1% among those with a high awareness to 22% of those with no awareness of beyondblue: χ2 = 835, df = 3, p < 0.001).
When the survey went on to ask specifically about major mental health problems, those with professional training in mental health were more likely to spontaneously identify depression as a mental health problem in pregnancy (57% versus 38%: χ2 = 17.6, p < 0.001) and they also more frequently identified anxiety (35.2% versus 21.4% of those not trained; χ2 = 110.9, p < 0.001). With respect to mental health training, a similar pattern held for the postnatal period (data not shown). Table 1 gives frequencies of responses in respect of the postnatal period: responses regarding pregnancy were very similar with depression the most common answer followed by stress and anxiety. Older Australians (55 years and over) identified depression and stress as postnatal mental health problems significantly less than other age groups, identified lack of sleep significantly more frequently and were more likely to answer ‘don't know’ (Table 1). Awareness of the specific term ‘perinatal depression’ was 41%, but older Australians had a significantly better recognition of this term than other groups (51.2% versus 36.7% of younger Australians: χ2 = 262, p < 0.001).
Mental health problems in the postnatal period most frequently cited†
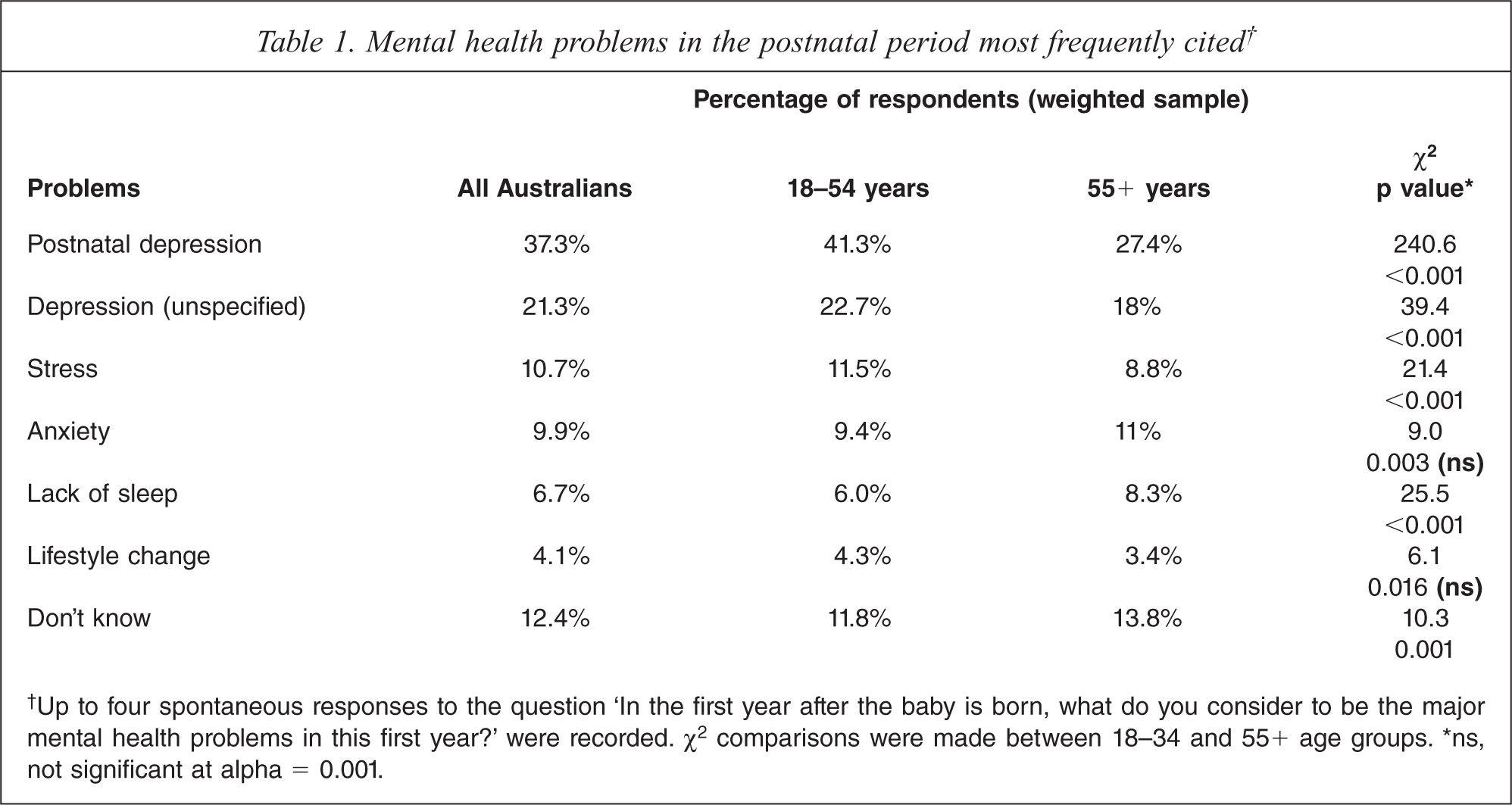
†Up to four spontaneous responses to the question ‘In the first year after the baby is born, what do you consider to be the major mental health problems in this first year?’ were recorded. χ2 comparisons were made between 18–34 and 55+ age groups. ∗ns, not significant at alpha = 0.001.
In general, Australians believed that the prevalence of depression in both pregnancy and the postnatal period was high. Of the respondents, 73% indicated that depression occurred in 15–50% of women during pregnancy, and 88% of respondents said it occurred in 15–50% of new mothers in the first postnatal year. Less than 10% of respondents answered ‘don't know’ to these two items, indicating that most Australian adults readily identify depression as a highly prevalent perinatal mood disorder.
Knowledge about depression in perinatal women
When asked ‘What are the signs and symptoms of postnatal depression?’ the most frequent responses (Table 2) included five which mapped closely to diagnostic criteria [21] for a major depressive episode (depressed mood, anhedonia, weight/appetite changes, insomnia/hypersomnia, fatigue). Overall, 33.7% of respondents nominated one of these, 14.1% mentioned two and 4.5% cited three or more diagnostic symptoms. Notably, the second most common response concerned women's feelings of bonding with their infant. Whilst both men and women cited this as a symptom, women did so significantly more frequently – a contrasting pattern that held across ten of the twelve most common responses (Table 2). Men mentioned externally identifiable manifestations of emotional state (anger, irritability, mood swings) significantly more frequently than women, and also identified internalized qualities of feelings (sadness, anxiety, feelings of not coping, tiredness, isolation) significantly less frequently.
Symptoms of postnatal depression cited by men and women
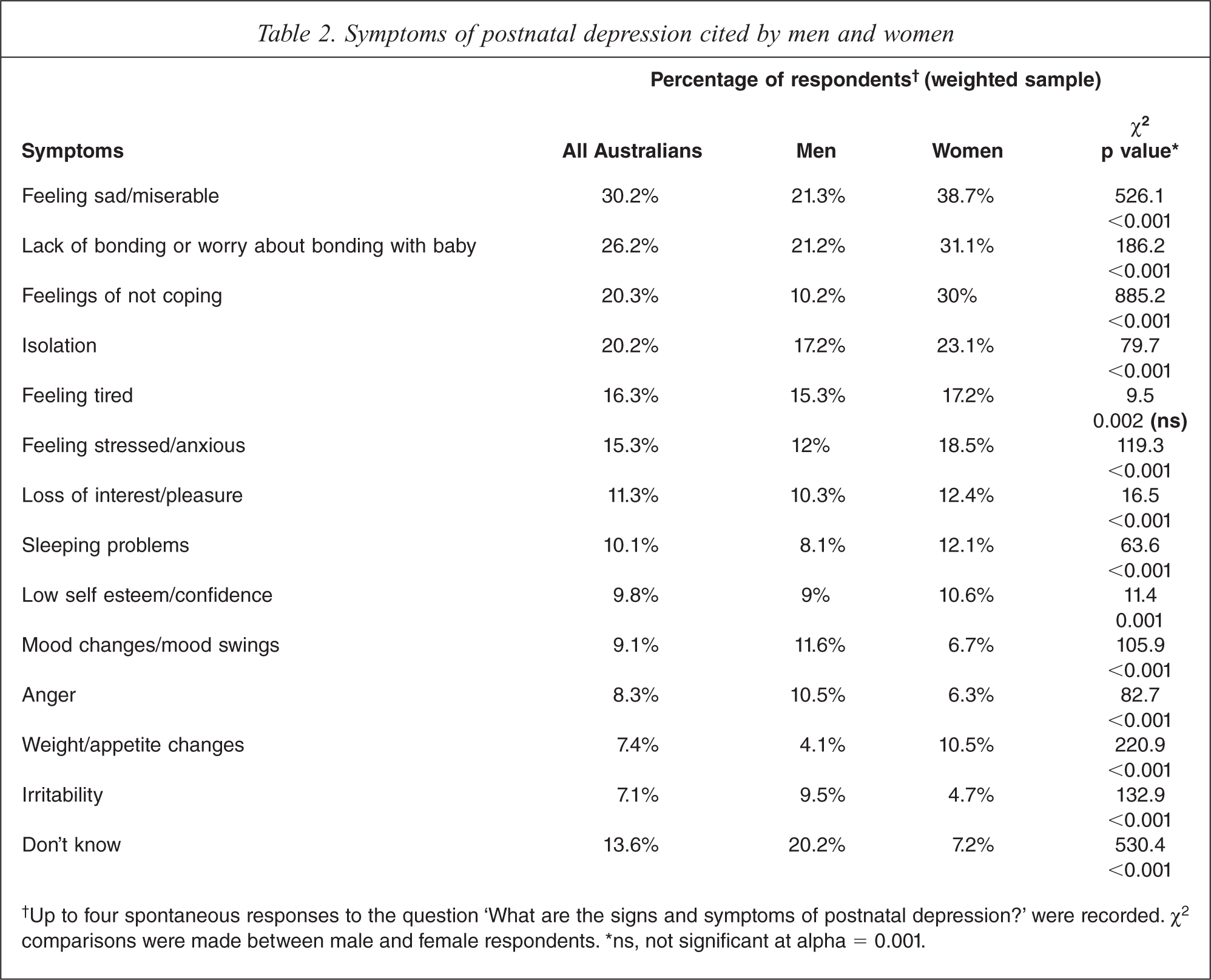
†Up to four spontaneous responses to the question ‘What are the signs and symptoms of postnatal depression?’ were recorded. χ2 comparisons were made between male and female respondents. ∗ns, not significant at alpha = 0.001.
Table 3 lists the most commonly reported male and female beliefs about the causes of postnatal depression. Biological causes and a lack of preparedness for parenting were the most commonly held views among both men and women. Whilst the general pattern of responses to this question was similar for those who had training in the mental health field and those who had not, those with mental health training identified biological causes significantly more frequently (45.4% of responses from this group: χ2 = 52.8, p < 0.001). Other causes frequently cited included lack of support, not coping with infant's demands and stress.
Causes of postnatal depression most frequently cited†
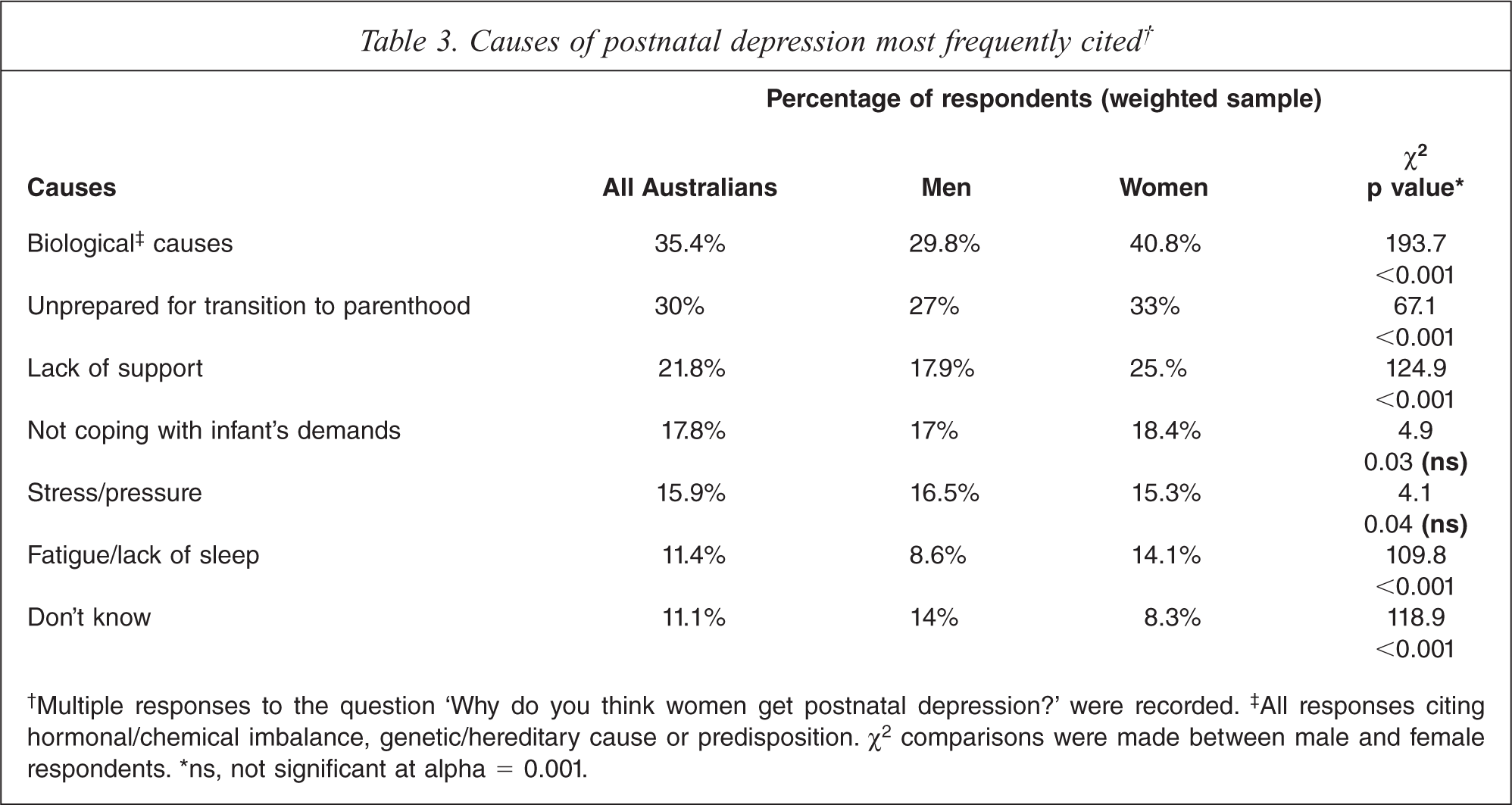
†Multiple responses to the question ‘Why do you think women get postnatal depression?’ were recorded.‡ All responses citing hormonal/chemical imbalance, genetic/hereditary cause or predisposition. χ2 comparisons were made between male and female respondents. ∗ns, not significant at alpha = 0.001.
The survey next asked ‘What types of treatment are most suitable for a woman with postnatal depression?’ Table 4 lists the most common spontaneous responses of male and female respondents. Non-pharmacological treatments, in total, were overwhelmingly more frequently cited than the use of antidepressant medication, with counselling the most commonly suggested ‘talk’ therapy. Further, among those citing antidepressants as a suitable treatment, women were significantly more likely to do so than men (Table 4).
Most suitable treatments for postnatal depression
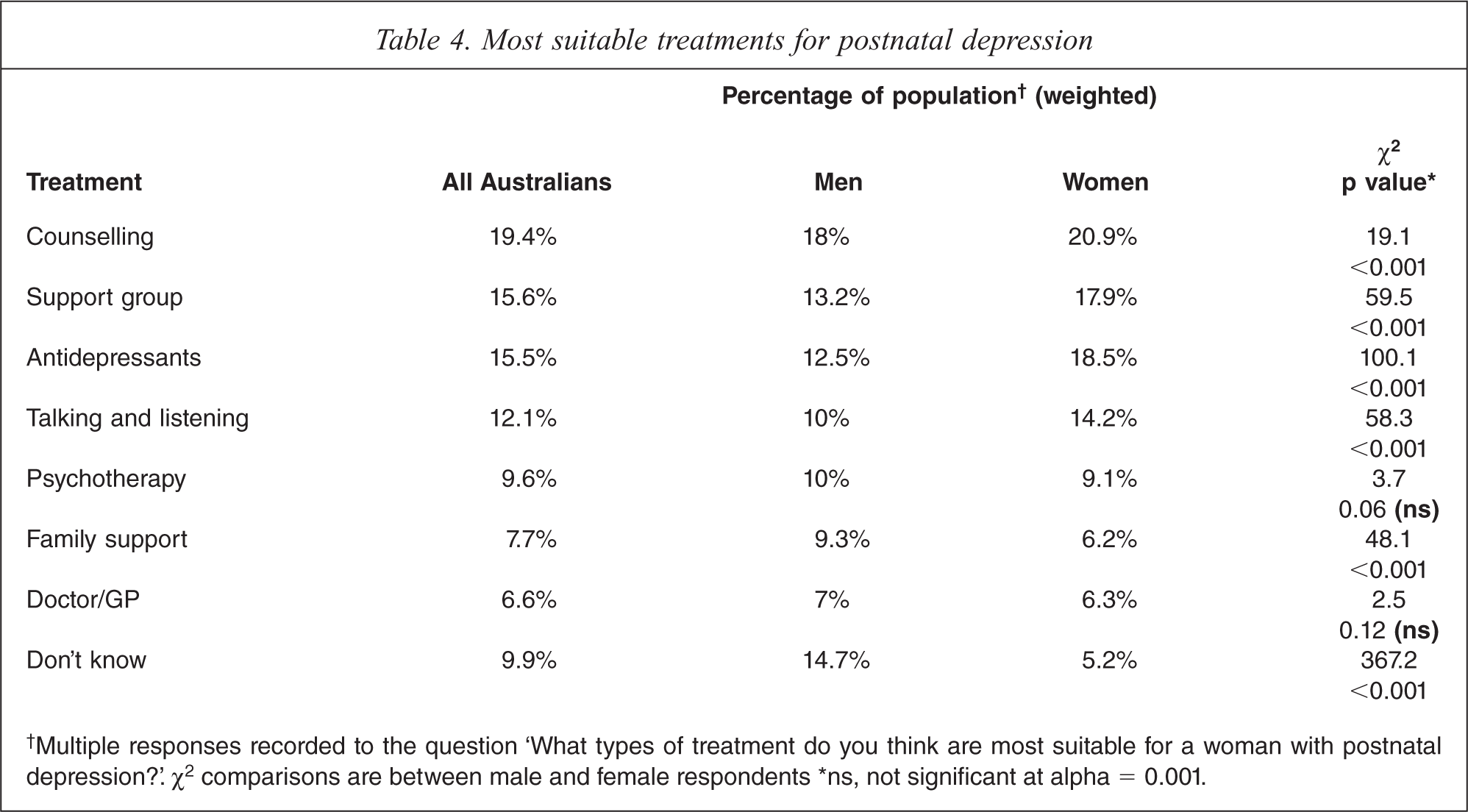
†Multiple responses recorded to the question ‘What types of treatment do you think are most suitable for a woman with postnatal depression?’. χ2 comparisons are between male and female respondents ∗ns, not significant at alpha = 0.001.
First responses to the next question ‘If you (your wife/partner) had postnatal depression, who would be your first choice to go to?’ (who would you recommend they go to first?) are summarized in Figure 1. Men were significantly more likely to nominate seeking help from a GP (χ2 = 200, p < 0.001) or an unspecified doctor (χ2 = 90, p < 0.001), while women were significantly more likely to indicate that support from friends and family would be their first preference as a source of help (χ2 = 842, p < 0.001). Results were very similar for the equivalent question on help-seeking in pregnancy (data not shown).
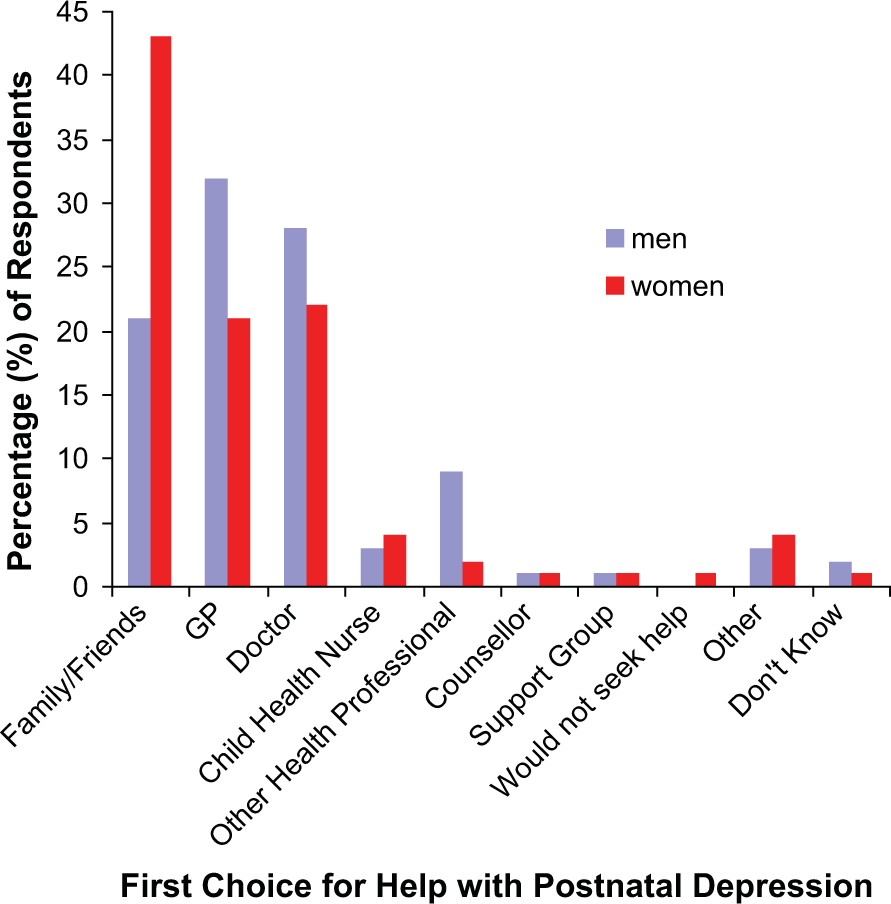
Male and female attitudes to help seeking. The frequencies of first responses to the question ‘If you (your wife/partner) had postnatal depression, who would be your first choice to go to?’ (who would you recommend they go to first?). Percentages for the weighted sample are plotted separately for men (black columns) and women (white columns).
For most of the items concerning symptoms, causes and treatments for postnatal depression, male respondents were significantly more likely to respond ‘don't know’
Attitudes and beliefs
Table 5 summarizes the extent of agreement with a number of statements regarding antenatal and postnatal depression. Attitudes to whether depression was ‘normal’ differed with respect to the antenatal and postnatal periods. However, the majority of responses connected with attitudes to depression and to expectations of women in a mothering role were clearly positive.
Some beliefs about perinatal women with depression
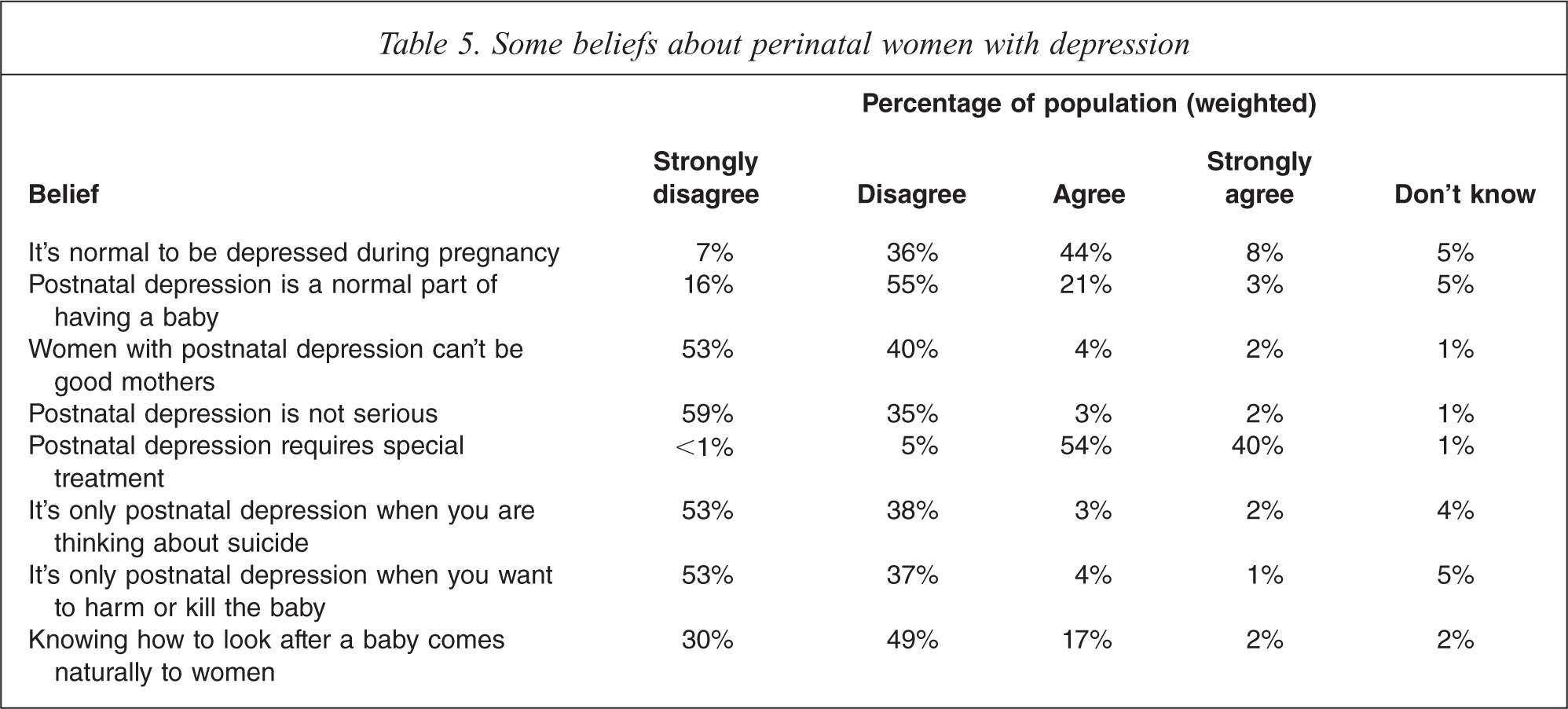
In total, 78% of respondents agreed that all women should be ‘checked for depression’ during pregnancy and 83% agreed that this should be done in the postnatal period (not tabled).
Discussion
As a general health issue, awareness of depression in the first postnatal year appears high (43.6% of spontaneous first responses). Thus, in comparison with our previous surveys, postnatal depression was better recognized than depression in general (1.3% of responses in previous work [17]). At the same time, levels of awareness showed a stark dichotomy between the antenatal and postnatal periods. Antenatal depression was rarely identified spontaneously as a general health issue (3.7%). Despite this, when asked specifically about mental health issues in pregnancy, depression was seen as a major problem. It may be somewhat concerning, however, that just over half of Australians viewed being depressed in pregnancy as ‘a normal part of having a baby’, as much evidence now points to the deleterious effects of prenatal maternal depression, anxiety and stress on infant development [22,23]. By contrast, the equivalent attitude to postnatal depression was a virtual mirror image, with most Australians disagreeing that depression is a normal part of being a new mother.
Beliefs about rates of occurrence of depression in pregnancy and in the first postnatal year indicated that most Australians do not underestimate the period prevalence (i.e. the cumulative rate) of these problems. Indeed, if anything these rates were overestimated by the general public, and this may suggest a confusion with the much more common ‘baby blues’, which affects the majority of new mothers to some degree [24]. Whilst point prevalence (i.e. the rate at any one particular moment in time) is often cited as around 10%, the vast majority of Australians estimated that the prevalence of depression throughout the perinatal period was between 15% and 50%. Considering the occurrence of major and minor depressive disorders combined, this is within the confidence limits of available period prevalence estimates from meta-analyses of studies based on diagnostic interviews [6].
In common with previous findings on mental health literacy [19], older Australians were less aware of postnatal depression as a mental health problem and there could be a number of reasons for this. First, those aged 55 years and older may have gained much of their health literacy at a time when perinatal mood disorders were under-recognized and perhaps stigmatized. However, as pointed out by others [25] relatively little is yet known about how mental health literacy is accumulated by individuals.
Anxiety, which often exists comorbidly with depression in the perinatal period [26,27] was not well recognized as a mental health problem in its own right, or as a possible sign of maternal depression. Its recognition was also higher among those with mental health training. Although estimates vary considerably [28], anxiety disorders in the perinatal period may be more prevalent than depressive disorders [27], and antenatal anxiety has been found to be a risk factor for postnatal depression [29,30].
Several symptoms corresponding to diagnostic criteria for major depression were recognized by survey respondents: over 50% spontaneously mentioned at least one of these, although less than 20% correctly identified two or more. When citing symptoms, men and women tended toward mentions of external manifestations (e.g. irritability) and internalized qualities (e.g. sadness) of emotional state respectively. Interestingly, difficulties in mother–infant bonding were seen as a common symptom of postnatal depression (especially among women). This is supported by research findings that mother–infant relationships can be compromised during maternal depressive episodes and not readily redressed by treatment of, or remission from, depression [31].
In terms of the causes of postnatal depression, many Australians identified lack of support and stressful life events, which are well established risk factors. However, by far the most common perception about the cause of postnatal depression was that it is biological in nature, stemming from hormonal imbalances or from congenitally pre-existing characteristics of particular women (including genetic characteristics). Possibly, the pervasiveness of the biological explanation is in part due to confusion with ‘baby blues’. Next in order of frequency came the idea that postnatal depression is due to a lack of readiness for the transition to parenthood. It is interesting that neither of these two most common perceptions are among the major known risk factors for postnatal depression identified by research (antenatal depression, antenatal anxiety, major life events, lack of support, low partner support and previous depression history [32–35]). It is striking that these two perceptions were shared equally by those trained in the mental health field. It has been previously noted, in regard to mental health literacy in general, that the concordance of professional and public beliefs has increased in recent years in Australia [13]. On the basis of our results, it would appear that most beliefs about the causes of depression in perinatal women are closely similar among both mental health professionals and the general population.
Non-pharmacological treatments for depression in perinatal women were clearly seen as more suitable by the majority of respondents, but supports from a range of people were considered useful, e.g. family, friends, doctors, counsellors. This coincides somewhat with the latest clinical guidance [36] for the best-practice management of perinatal mood disorders, a major concern of both women and clinicians being the possible side-effects of medication on unborn and breast-feeding infants. It seems somewhat paradoxical then, that women cited medication as a suitable treatment for postnatal depression more frequently than men (a similar divergence of male and female attitudes on this issue has been reported previously [17]). Possibly, this difference simply reflects women's wider knowledge about available treatments for postnatal depression generally. Furthermore, there was an apparent discrepancy between what Australians nominated as the most suitable treatments, and the courses of action they nominated as their own first choice if affected personally. For example, counselling, medication and support groups were most commonly cited as suitable treatments (37% in total), with seeing a doctor and family support totalling just 5% and 6% of responses respectively. However, when the survey focused specifically on respondents own personal preference, contacting a doctor (52%) and seeking support from friends and family (32%) became the most common responses. Under these circumstances, only 2% said they would choose (or recommend) counselling or joining a support group. Possibly, this reflects a major difference in people's attitudes towards helping others with a mental health difficulty on the one hand, and towards personal help-seeking on the other.
Among Australian adults, awareness of depression in perinatal women is generally high, and prevailing community attitudes are largely positive, though there are particular areas where knowledge is at odds with the research evidence in the field. Negative myths and unhelpful stereotypes about depression and motherhood appear to have very little prominence. However, education and improved literacy about the causes and symptoms of depression, the prevalence of anxiety disorders, and the seriousness of antenatal depression in particular, are indicated. The majority of Australians, both men and women, appear to support universal screening for depression in the perinatal period. This concurs with previous surveys in both depressed and non-depressed perinatal women in Australia [37,38] and may suggest a positive community response to the NPDI. The effect of depression on mother–child relationships also appears to be a primary community concern.
The discrepancy in male and female literacy about perinatal depressive disorders, taken with the fact that poor support from a male partner is one of the greatest risk factors for postnatal depression that is amenable to change, suggests that there may be value in targeting the literacy of men, and new and expectant fathers in particular. Finally, encouraging positive attitudes towards personal help-seeking for effective treatments is likely to remain a worthwhile aim of future information and awareness campaigns.
Footnotes
Acknowledgements